
Histopathological Lung Findings in COVID-19 B.1.617.2 SARS-CoV-2 Delta Variant

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Virology Analysis for SARS-CoV-2 Variant
2.3. Histopathology
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tao, K.; Tzou, P.L.; Nouhin, J.; Gupta, R.K.; de Oliveira, T.; Kosakovsky Pond, S.L.; Fera, D.; Shafer, R.W. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat. Rev. Genet. 2021, 22, 757–773. [Google Scholar] [CrossRef]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics Against Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar] [PubMed]
- World Health Organisation. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 24 August 2022).
- Fan, L.Q.; Hu, X.Y.; Chen, Y.Y.; Peng, X.L.; Fu, Y.H.; Zheng, Y.P.; Yu, J.M.; He, J.S. Biological significance of the genomic variation 325 and structural dynamics of SARS-CoV-2 B.1.617. Front. Microbiol. 2021, 12, 750725. [Google Scholar]
- Allen, H.; Vusirikala, A.; Flannagan, J.; Twohig, K.A.; Zaidi, A.; Chudasama, D.; Lamagni, T.; Groves, N.; Turner, C.; Rawlinson, C.; et al. COVID-19 Genomics UK (COG-UK Consortium). Household transmission of COVID-19 cases associated with SARS-CoV-2 delta variant (B.1.617.2): National case-control study. Lancet Reg. Health Eur. 2022, 12, 100252. [Google Scholar] [CrossRef]
- Kucharski, A.; Davies, N.; Eggo, R.; Funk, S. Modelling Importations and Local Transmission of B.1.617.2 in the UK. Report for SPI-M (updated), 12 May 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/988203/S1240_CMMID_COVID-19_Working_Group_Modelling_importations_and_local_transmission_of_B.1.617.2_in_the_UK__13_May_2021.pdf (accessed on 27 August 2022).
- Ong, S.W.X.; Chiew, C.J.; Ang, L.W.; Mak, T.M.; Cui, L.; Toh, M.P.H.S.; Lim, Y.D.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and Virological Features of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants of Concern: A Retrospective Cohort Study Comparing, B.1.1.7 (Alpha), B.1.351 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2022, 75, e1128–e1136. [Google Scholar] [CrossRef]
- Fisman, D.N.; Tuite, A.R. Progressive Increase in Virulence of Novel SARS-CoV-2 Variants in Ontario, Canada. CMAJ 2021, 193, E1619–E1625. [Google Scholar] [CrossRef] [PubMed]
- Arslan, M.; Xu, B.; Gamal El-Din, M. Transmission of SARS-CoV-2 via fecal-oral and aerosols-borne routes: Environmental dynamics and implications for wastewater management in underprivileged societies. Sci. Total Environ. 2020, 743, 140709. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Gattarello, S.; Steinberg, I.; Busana, M.; Palermo, P.; Lazzari, S.; Romitti, F.; Quintel, M.; Meissner, K.; Marini, J.; et al. COVID-19 pneumonia: Pathophysiology and management. Eur. Respir. Rev. 2021, 30, 210138. [Google Scholar] [CrossRef] [PubMed]
- Pandey, P.; Agarwal, S.; Rajkumar. Lung Pathology in COVID-19: A Systematic Review. Int. J. Appl. Basic Med. Res. 2020, 10, 226–233. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Muñoz Martin, A.J. Thrombosis and Coagulopathy in COVID-19. Curr. Probl. Cardiol. 2021, 46, 100742. [Google Scholar]
- Kuypers, F.A.; Rostad, C.A.; Anderson, E.J.; Chahroudi, A.; Jaggi, P.; Wrammert, J.; Mantus, G.; Basu, R.; Harris, F.; Hanberry, B.; et al. Secretory phospholipase A2 in SARS-CoV-2 infection and multisystem inflammatory syndrome in children (MIS-C). Exp. Biol. Med. 2021, 246, 2543–2552. [Google Scholar] [CrossRef]
- Snider, J.M.; You, J.K.; Wang, X.; Snider, A.J.; Hallmark, B.; Zec, M.M.; Seeds, M.C.; Sergeant, S.; Johnstone, L.; Wang, Q.; et al. Group IIA secreted phospholipase A2 is associated with the pathobiology leading to COVID-19 mortality. J. Clin. Investig. 2021, 131, e149236. [Google Scholar] [CrossRef] [PubMed]
- WHO. Infection Prevention and Control for the Safe Management of a Dead Body in the Context of COVID-19. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331538/WHO-COVID-19-lPC_DBMgmt-2020.1-eng.pdf (accessed on 20 December 2022).
- Centers for Disease Control and Prevention. Collection and Submission of Postmortem Specimens from Deceased Persons with Known or Suspected COVID-19, 2020 (Interim Guidance). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html (accessed on 20 December 2022).
- National Institute for Public Health from Romania. Available online: https://www.cnscbt.ro/index.php/info-medical/2047-metodologia-de-supraveghere-a-covid-19-actualizare-23-10-2020-1/file (accessed on 20 December 2022).
- Quick, J.; Loman, N. hCoV-2019/nCoV-2019 version 3 Amplicon Set. ARTIC Consortium. 2020. Available online: https://artic.network/resources/ncov/ncov-amplicon-v3.pdf (accessed on 31 January 2022).
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Mlcochova, P.; Kemp, S.A.; Dhar, M.S.; Papa, G.; Meng, B.; Ferreira, I.A.T.M.; Datir, R.; Collier, D.A.; Albecka, A.; Singh, S.; et al. SARS-CoV-2 B.1.617.2 Delta variant replication and immune evasion. Nature 2021, 599, 114–119. [Google Scholar] [CrossRef]
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Aghayari Sheikh Neshin, S.; Khatami, A.; Turner, D.L.; Djalalinia, S.; Mousavi, S.A.; Mardani-Fard, H.A.; et al. Effectiveness of COVID-19 Vaccines against Delta (B.1.617.2) Variant: A Systematic Review and Meta-Analysis of Clinical Studies. Vaccines 2021, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Harder, T.; Külper-Schiek, W.; Reda, S.; Treskova-Schwarzbach, M.; Koch, J.; Vygen-Bonnet, S.; Wichmann, O. Effectiveness of COVID-19 vaccines against SARS-CoV-2 infection with the Delta (B.1.617.2) variant: Second interim results of a living systematic review and meta-analysis, 1 January to 25 August 2021. Eurosurveillance 2021, 26, 2100920. [Google Scholar] [CrossRef] [PubMed]
- da Silva, C.G.L.; Santana, J.R.P.; Pinheiro, L.F.G.; de Sousa, G.O.; Galvão, L.M.A.; Gomes, K.G.S.; Medeiros, K.A.; Diniz, L.A.; de Oliveira, Í.G.P.; Felix, E.B.G.; et al. Anatomopathological Aspects and Clinical Correlation of COVID-19: A Systematic Review. Adv. Exp. Med. Biol. 2021, 1353, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Barton, L.M.; Duval, E.J.; Stroberg, E.; Ghosh, S.; Mukhopadhyay, S. COVID-19 Autopsies, Oklahoma, USA. Am. J. Clin. Pathol. 2020, 153, 725–733, Erratum in Am. J. Clin. Pathol. 2020, 153, 852. [Google Scholar] [CrossRef] [Green Version]
- Iida, S.; Arashiro, T.; Suzuki, T. Insights into Pathology and Pathogenesis of Coronavirus Disease 2019 from a Histopathological and Immunological Perspective. JMA J. 2021, 4, 179–186. [Google Scholar] [CrossRef]
- Konopka, K.E.; Nguyen, T.; Jentzen, J.M.; Rayes, O.; Schmidt, C.J.; Wilson, A.M.; Farver, C.F.; Myers, J.L. Diffuse alveolar damage (DAD) resulting from coronavirus disease 2019 Infection is Morphologically Indistinguishable from Other Causes of DAD. Histopathology 2020, 77, 570–578. [Google Scholar] [CrossRef]
- Bussani, R.; Schneider, E.; Zentilin, L.; Collesi, C.; Ali, H.; Braga, L.; Volpe, M.C.; Colliva, A.; Zanconati, F.; Berlot, G.; et al. Persistence of viral RNA, pneumocyte syncytia and thrombosis are hallmarks of advanced COVID-19 pathology. EBioMedicine 2020, 61, 103104. [Google Scholar] [CrossRef]
- Bösmüller, H.; Matter, M.; Fend, F.; Tzankov, A. The pulmonary pathology of COVID-19. Virchows Arch. 2021, 478, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Hikmet, F.; Méar, L.; Edvinsson, Å.; Micke, P.; Uhlén, M.; Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol. Syst. Biol. 2020, 16, e9610. [Google Scholar] [CrossRef] [PubMed]
- Jonigk, D.; Golpon, H.; Bockmeyer, C.L.; Maegel, L.; Hoeper, M.M.; Gottlieb, J.; Nickel, N.; Hussein, K.; Maus, U.; Lehmann, U.; et al. Plexiform lesions in pulmonary arterial hypertension composition, architecture, and microenvironment. Am. J. Pathol. 2011, 179, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Revercomb, L.; Hanmandlu, A.; Wareing, N.; Akkanti, B.; Karmouty-Quintana, H. Mechanisms of Pulmonary Hypertension in Acute Respiratory Distress Syndrome (ARDS). Front. Mol. Biosci. 2021, 7, 624093. [Google Scholar] [CrossRef] [PubMed]
- Price, L.C.; McAuley, D.F.; Marino, P.S.; Finney, S.J.; Griffiths, M.J.; Wort, S.J. Pathophysiology of pulmonary hypertension in acute lung injury. Am. J. Physiol. Lung Cell. Mol. Physiol. 2012, 302, L803–L815. [Google Scholar] [CrossRef] [Green Version]
- Moloney, E.D.; Evans, T.W. Pathophysiology and pharmacological treatment of pulmonary hypertension in acute respiratory distress syndrome. Eur. Respir. J. 2003, 21, 720–727. [Google Scholar] [CrossRef] [Green Version]
- Pagnesi, M.; Baldetti, L.; Beneduce, A.; Calvo, F.; Gramegna, M.; Pazzanese, V.; Ingallina, G.; Napolano, A.; Finazzi, R.; Ruggeri, A.; et al. Pulmonary hypertension and right ventricular involvement in hospitalised patients with COVID-19. Heart 2020, 106, 1324–1331. [Google Scholar] [CrossRef]
- Eroume, À.; Egom, E.; Shiwani, H.A.; Nouthe, B. From acute SARS-CoV-2 infection to pulmonary hypertension. Front. Physiol. 2022, 13, 1023758. [Google Scholar] [CrossRef]
- Abe, K.; Toba, M.; Alzoubi, A.; Ito, M.; Fagan, K.A.; Cool, C.D.; Voelkel, N.F.; McMurtry, I.F.; Oka, M. Formation of plexiform lesions in experimental severe pulmonary arterial hypertension. Circulation 2010, 121, 2747–2754. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.H.B. Plexiform Lesions in Pulmonary Arterial Hypertension: Are We Getting Closer to Manage with More Patience and Rigor? Arq. Bras. Cardiol. 2020, 115, 491–492. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. of Case, Sex, Age | Medical Institution of the Patients | Sampling of Lung Tissue | SARS-CoV-2 Variant/ GISAID | Histopathology Result | Immunohistochemistry Result |
|---|---|---|---|---|---|
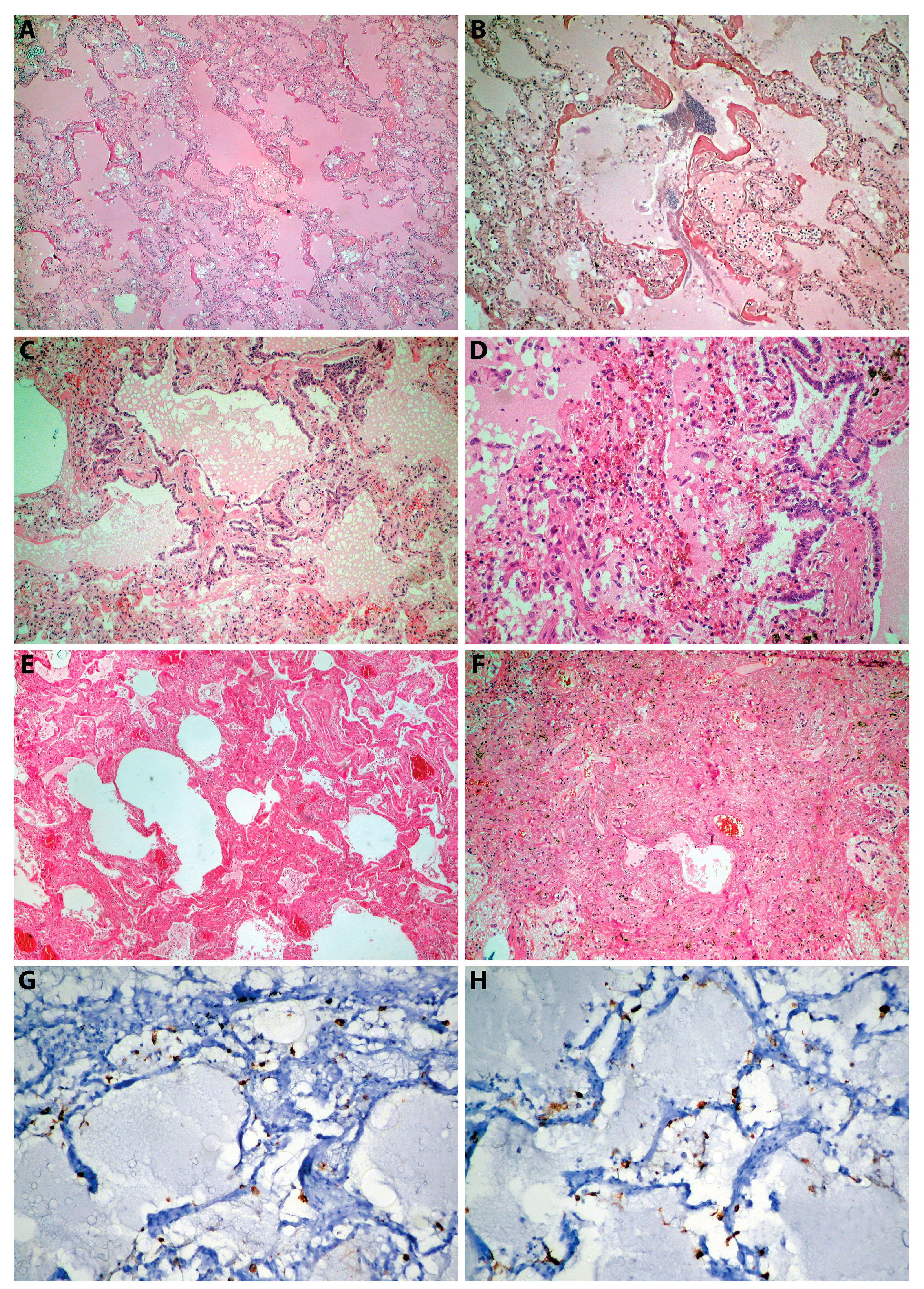
| 1, M, 61 | Department of Pathology, County Emergency Hospital Deva | Postmortem biopsy | B.1.617.2/ EPI_ISL_5241180 | Acute pulmonary edema (Figure 2A), DAD 1 | Negative |
| 2, M, 66 | Department of Pathology, County Emergency Hospital Deva | Postmortem biopsy | B.1.617.2/ EPI_ISL_5858608 | Acute pulmonary edema, DAD 1 (Figure 2B) | Positive proteins of SARS-CoV-2 in alveolocytes (Figure 2G–H) |
| 3, M, 83 | Department of Pathology, County Emergency Hospital Deva | Postmortem biopsy | B.1.617.2/ EPI_ISL_5858607 | DAD 3 (Figure 2E) | Positive proteins of SARS-CoV-2 in alveolocytes |
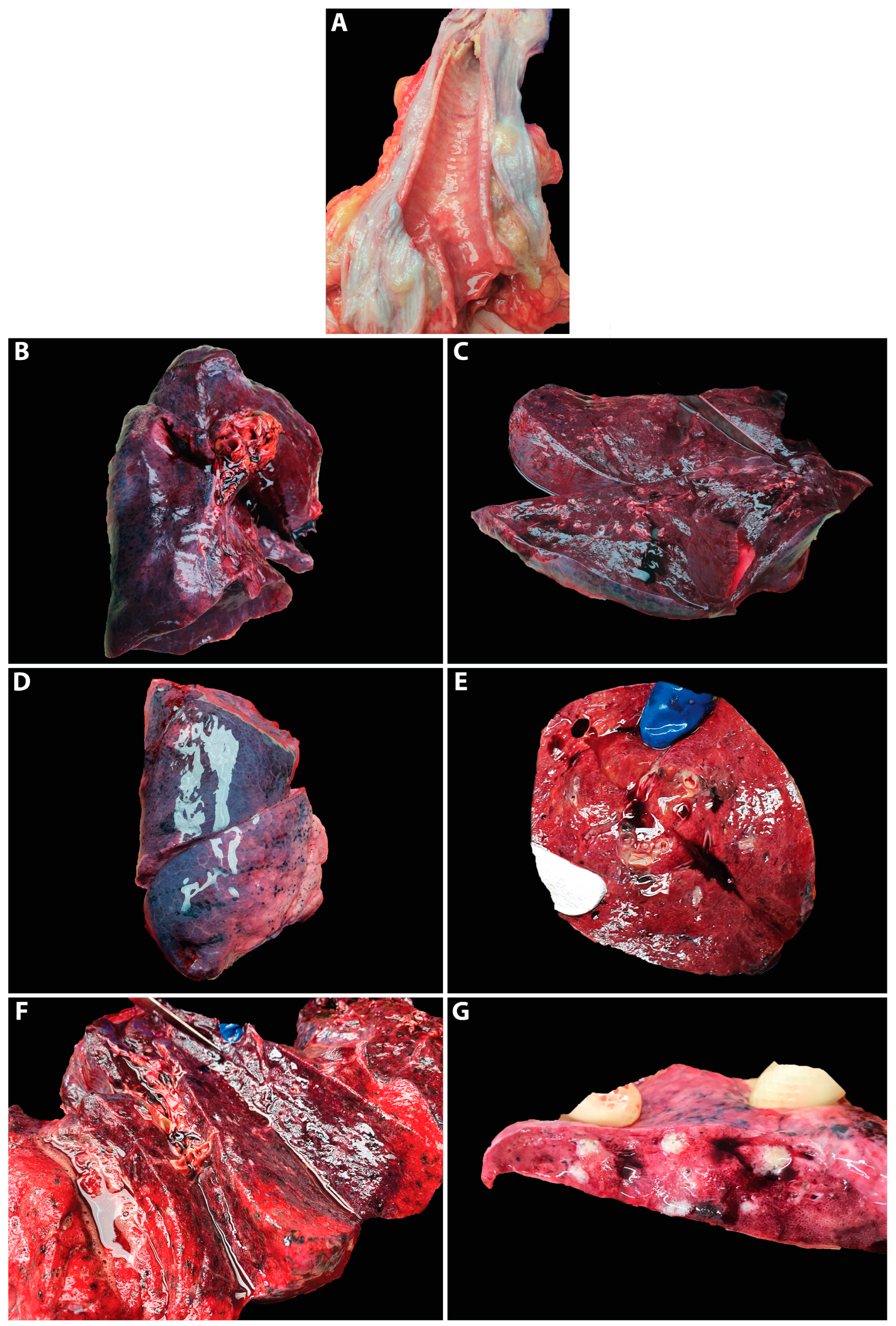
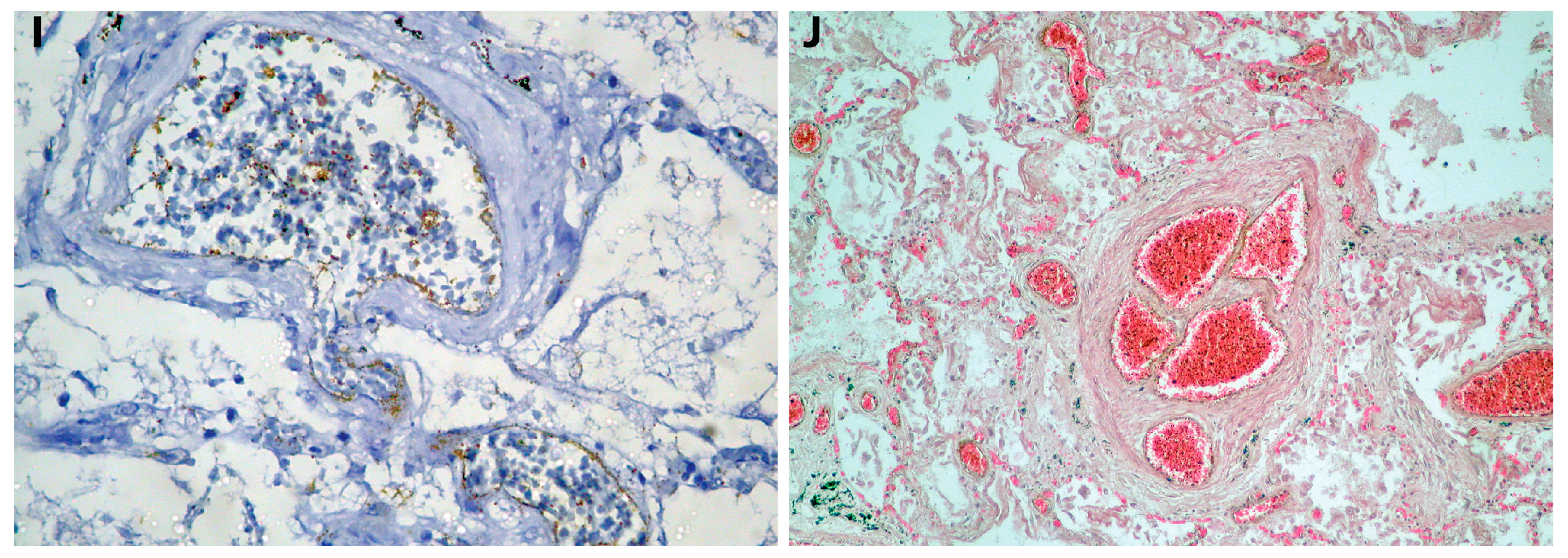
| 4, F, 69 | Department of Pathology, County Emergency Hospital Deva | Autopsy (Figure 1D–E) | B.1.617.2/ Positive for screening (L452R) | Acute pulmonary edema, DAD 1, focal DAD 2 (Figure 2C–D), multifocal organizing pneumonia, pulmonary microthrombosis, plexogenic lesion (Figure 2J) | Positive proteins of SARS-CoV-2 in endothelial cells (endothelithis COVID-19) (Figure 2I) |
| 5, M, 63 | Department of Pathology, County Emergency Hospital Deva | Postmortem biopsy | B.1.617.2/ EPI_ISL_15764977 | Acute pulmonary edema, DAD 1, focal DAD 2 | Positive proteins of SARS-CoV-2 in alveolocytes |
| 6, F, 70 | Department of Pathology, County Emergency Hospital Deva | Postmortem biopsy | B.1.617.2/EPI_ISL_15764981 | Acute pulmonary edema, DAD 1 | Negative |
| 7, F, 64 | Department of Pathology, County Emergency Hospital Deva | Postmortem biopsy | B.1.617.2/Positive for screening (L452R) | DAD 2 | Positive proteins of SARS-CoV-2 in alveolocytes |
| 8, F, 71 | Institute of Legal Medicine Cluj-Napoca | Autopsy (Figure 1A–C) | B.1.617.2/ EPI_ISL_15764979 | Acute pulmonary edema, areas of alveolar collapse, DAD 2 | Negative |
| 9, M, 77 | Institute of Legal Medicine Cluj-Napoca | Autopsy (Figure 1G) | B.1.617.2/ EPI_ISL_15764978 | Bronchopneumonia, alveolar proteinosis | Negative |
| 10, M, 40 | Institute of Legal Medicine Cluj-Napoca | Autopsy | B.1.617.2/EPI_ISL_15764980 | Acute pulmonary edema, DAD 3 (Figure 2F), alveolar collapse | Positive proteins of SARS-CoV-2 in alveolocytes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeican, I.I.; Inișca, P.; Gheban, D.; Anton, V.; Lazăr, M.; Vică, M.L.; Mironescu, D.; Rebeleanu, C.; Crivii, C.B.; Aluaș, M.; et al. Histopathological Lung Findings in COVID-19 B.1.617.2 SARS-CoV-2 Delta Variant. J. Pers. Med. 2023, 13, 279. https://doi.org/10.3390/jpm13020279
Jeican II, Inișca P, Gheban D, Anton V, Lazăr M, Vică ML, Mironescu D, Rebeleanu C, Crivii CB, Aluaș M, et al. Histopathological Lung Findings in COVID-19 B.1.617.2 SARS-CoV-2 Delta Variant. Journal of Personalized Medicine. 2023; 13(2):279. https://doi.org/10.3390/jpm13020279
Chicago/Turabian StyleJeican, Ionuț Isaia, Patricia Inișca, Dan Gheban, Vlad Anton, Mihaela Lazăr, Mihaela Laura Vică, Daniela Mironescu, Codrin Rebeleanu, Carmen Bianca Crivii, Maria Aluaș, and et al. 2023. "Histopathological Lung Findings in COVID-19 B.1.617.2 SARS-CoV-2 Delta Variant" Journal of Personalized Medicine 13, no. 2: 279. https://doi.org/10.3390/jpm13020279