
Humoral Immune Response following SARS-CoV-2 Vaccination in Liver Transplant Recipients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
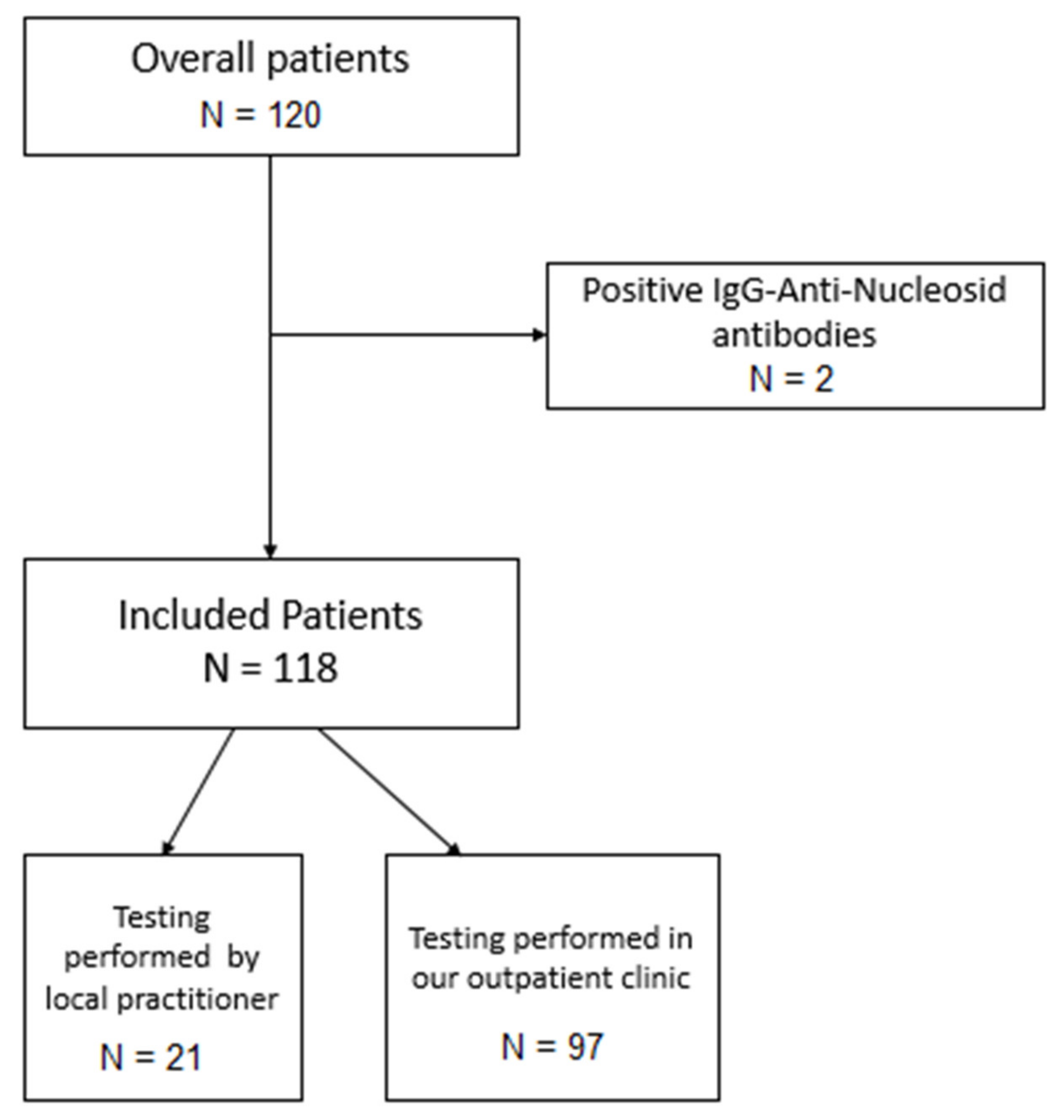
2.1. Patients, Inclusion and Exclusion Criteria
2.2. Antibody Assessment
2.3. Statistical Analysis
3. Results
3.1. Results from the Overall Cohort
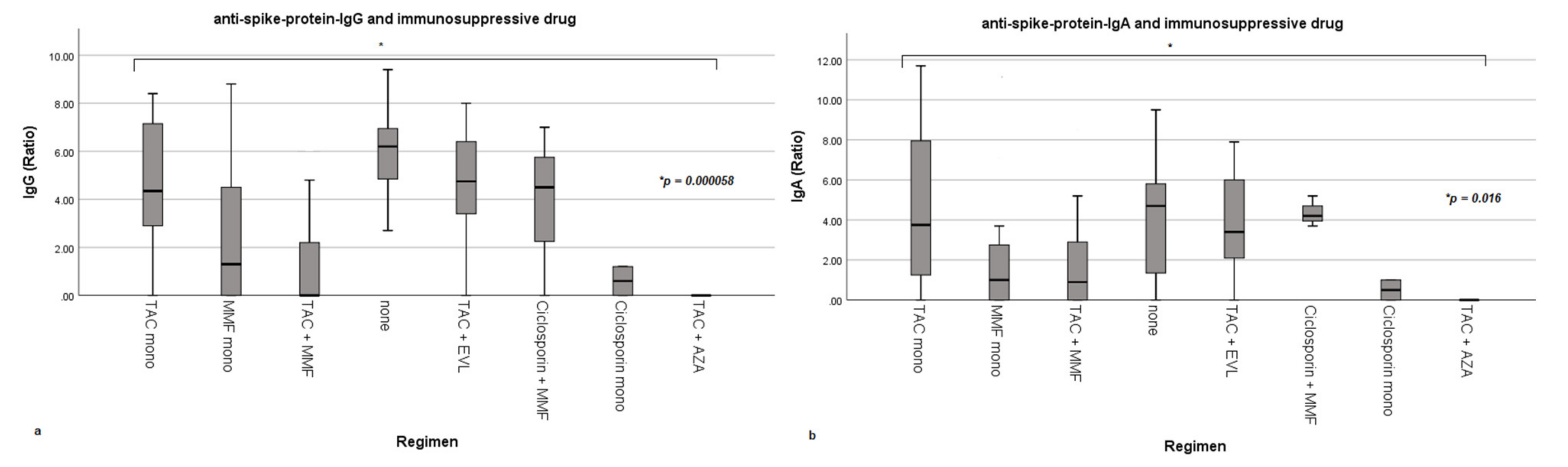
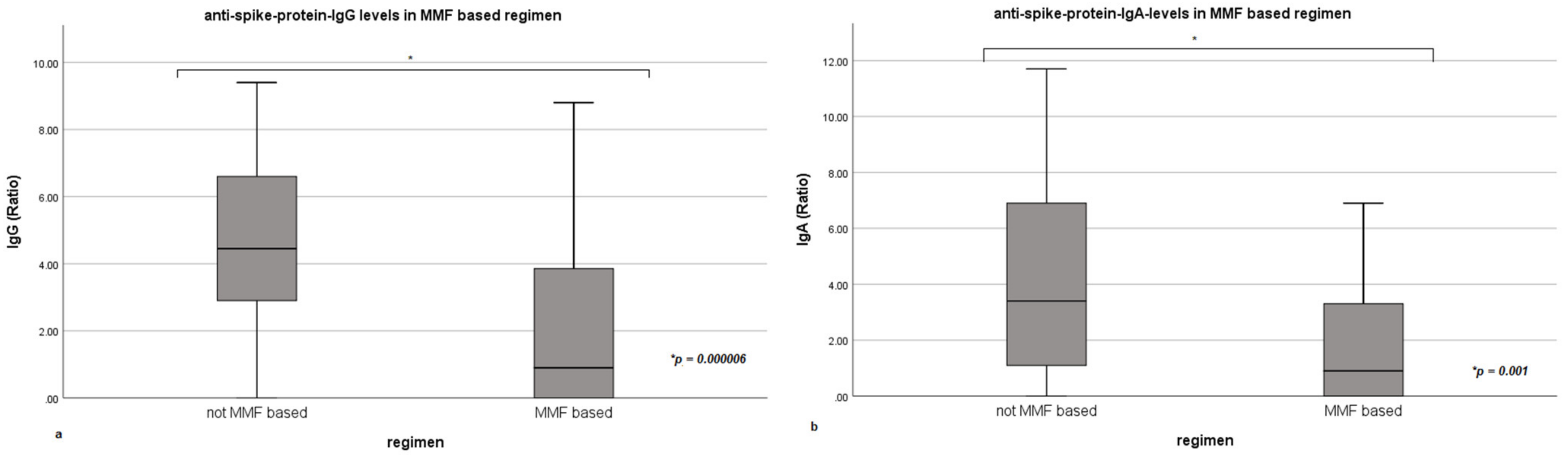
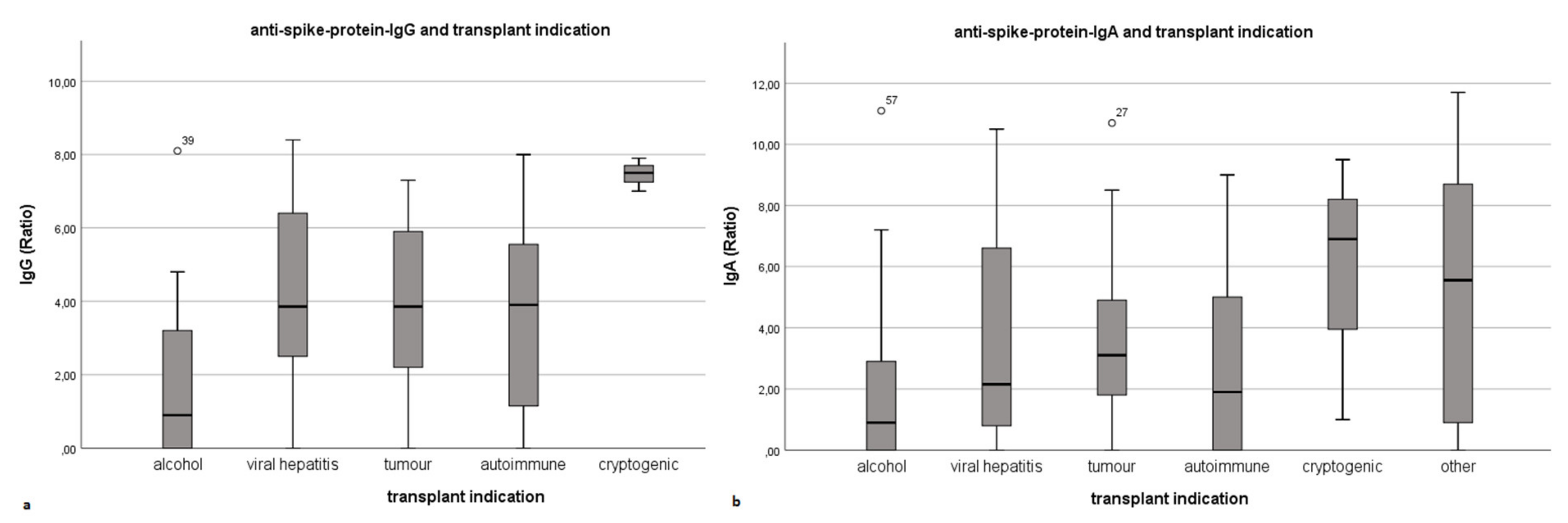
3.2. Anti-Spike-Protein-IgG- and IgA-Levels Corresponding Immunosupression and Underlying Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Cohort (N = 97) | IgG Positive (N = 75) | IgG Negative (N = 22) | p-Value | |
|---|---|---|---|---|
| Sex N (%) | 0.193 | |||
| Male | 59 (60.8) | 43 (57.3) | 16 (72.2) | |
| Female | 38 (39.2) | 32 (42.7) | 6 (27.3) | |
| Time since transplantation (years) | 0.244 | |||
| Mean | 13.5 | 14.0 | 12.0 | |
| Minimum | 0 | 0 | 0 | |
| Maximum | 32 | 32 | 30 | |
| Age at vaccination (years) | 0.425 | |||
| Mean | 65.7 | 65.0 | 68.1 | |
| Minimum | 31 | 31 | 42 | |
| Maximum | 84 | 84 | 82 | |
| Transplant indication N (%) | 0.046 | |||
| Alcohol-induced | 21 (21.6) | 11 (14.7) | 10 (45.5) | |
| Viral hepatitis | 22 (22.7) | 20 (26.7) | 2 (9.1) | |
| Tumour | 22 (22.7) | 17 (22.7) | 5 (22.7) | |
| Autoimmune | 16 (15.5) | 12 (16.0) | 3 (13.6) | |
| Cryptogenic | 3 (3.1) | 3 (4.0) | 0 (0) | |
| Other | 14 (14.4) | 12 (16.0) | 2 (9.1) | |
| Immunosuppression N (%) | 0.001 | |||
| Tacrolimus mono | 32 (33.0) | 30 (40) | 2 (9.1) | |
| MMF mono | 13 (13.4) | 9 (12.0) | 4 (18.2) | |
| Tacrolimus + MMF | 21 (21.6) | 10 (13.3) | 11 (50) | |
| Tacrolimus and Everolimus | 14 (14.4) | 12 (16.0) | 2 (9.1) | |
| Everolimus mono | 0 (0) | 0 (0) | 0 (0) | |
| Ciclosporin + MMF | 3 (3.1) | 2 (2.7) | 1 (4.5) | |
| Ciclosporin mono | 2 (2.1) | 1 (1.3) | 1 (4.5) | |
| None | 11 (11.3) | 11 (14.7) | 0 (0) | |
| Tacrolimus + Azathioprine | 1 (1) | 0 (0) | 1 (4.5) | |
| MMF-based regimen | 35 (36.1) | 19 (25.3) | 16 (72.2) | 0.000047 |
References
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; A Blumberg, E.; Besharatian, B.D.; et al. Coronavirus Disease 2019 in Solid Organ Transplant: A Multicenter Cohort Study. Clin. Infect. Dis. 2020, 126, ciaa1097. [Google Scholar] [CrossRef]
- Dumortier, J.; Duvoux, C.; Roux, O.; Altieri, M.; Barraud, H.; Besch, C.; Caillard, S.; Coilly, A.; Conti, F.; Dharancy, S.; et al. Covid-19 in liver transplant recipients: The French SOT COVID registry. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101639. [Google Scholar] [CrossRef]
- Becchetti, C.; Zambelli, M.F.; Pasulo, L.; Donato, M.F.; Invernizzi, F.; Detry, O.; Dahlqvist, G.; Ciccarelli, O.; Morelli, M.C.; Fraga, M.; et al. COVID-19 in an international European liver transplant recipient cohort. Gut 2020, 69, 1832–1840. [Google Scholar] [CrossRef]
- Colmenero, J.; Rodríguez-Perálvarez, M.; Salcedo, M.; Arias-Milla, A.; Muñoz-Serrano, A.; Graus, J.; Nuño, J.; Gastaca, M.; Bustamante-Schneider, J.; Cachero, A.; et al. Epidemiological pattern, incidence, and outcomes of COVID-19 in liver transplant patients. J. Hepatol. 2021, 74, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Webb, G.J.; Marjot, T.; A Cook, J.; Aloman, C.; Armstrong, M.J.; Brenner, E.J.; Catana, M.-A.; Cargill, T.; Dhanasekaran, R.; García-Juárez, I.; et al. Outcomes following SARS-CoV-2 infection in liver transplant recipients: An international registry study. Lancet Gastroenterol. Hepatol. 2020, 5, 1008–1016. [Google Scholar] [CrossRef]
- Villanego, F.; Cazorla, J.M.; Vigara, L.A.; Garcia, T.; Trujillo, T.; Montiel, N.; Rodriquez-Iglesias, M.; Mazuecos, A. Protecting kidney transplant recipients against SARS-CoV-2 infection: A third dose of vaccine is necessary now. Am. J. Transpl. 2021. [Google Scholar] [CrossRef]
- Aslam, S.; Adler, E.; Mekeel, K.; Little, S.J. Clinical effectiveness of COVID-19 vaccination in solid organ transplant recipients. Transpl. Infect. Dis. 2021, 23, e13705. [Google Scholar] [CrossRef] [PubMed]
- Malinis, M.; Cohen, E.; Azar, M.M. Effectiveness of SARS-CoV-2 vaccination in fully vaccinated solid organ transplant recipients. Arab. Archaeol. Epigr. 2021, 21, 2916–2918. [Google Scholar] [CrossRef]
- Serper, M.; Liu, C.; Blumberg, E.A.; Burdzy, A.E.; Veasey, S.; Halpern, S.; Lander, E.; Sigafus, M.R.; Bloom, R.D.; Dunn, T.B.; et al. A pragmatic outreach pilot to understand and overcome barriers to COVID-19 vaccination in abdominal organ transplant. Transpl. Infect. Dis. 2021, 23, e13722. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA 2021, 325, 1784. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Marion, O.; Del Bello, A.; Abravanel, F.; Couat, M.C.; Faguer, S.; Esposito, L.; Hebral, A.L.; Izopet, J.; Kamar, N. Safety and Immunogenicity of Anti–SARS-CoV-2 Messenger RNA Vaccines in Recipients of Solid Organ Transplants. Ann. Intern. Med. 2021, 174, 1336–1338. [Google Scholar] [CrossRef] [PubMed]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef]
- Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.; Sorge-Hädicke, B.; Eisenberger, U.; Gäckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 2021, 13, 756. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Arab. Archaeol. Epigr. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Georgery, H.; Devresse, A.; Yombi, J.-C.; Belkhir, L.; De Greef, J.; Darius, T.; Buemi, A.; Scohy, A.; Kabamba, B.; Goffin, E.; et al. Disappointing Immunization Rate After 2 Doses of the BNT162b2 Vaccine in a Belgian Cohort of Kidney Transplant Recipients. Transplantation 2021, 105, e283–e284. [Google Scholar] [CrossRef]
- Glatman-Freedman, A.; Bromberg, M.; Dichtiar, R.; Hershkovitz, Y.; Keinan-Boker, L. The BNT162b2 vaccine effectiveness against new COVID-19 cases and complications of breakthrough cases: A nation-wide retrospective longitudinal multiple cohort analysis using individualised data. EBioMedicine 2021, 72, 103574. [Google Scholar] [CrossRef]
- Thuluvath, P.J.; Robarts, P.; Chauhan, M. Analysis of antibody responses after COVID-19 vaccination in liver transplant recipients and those with chronic liver diseases. J. Hepatol. 2021, 75, 1434–1439. [Google Scholar] [CrossRef]
- Dumortier, J. Liver injury after mRNA-based SARS-CoV-2 vaccination in a liver transplant recipient. Clin. Res. Hepatol. Gastroenterol. 2021, 46, 101743. [Google Scholar] [CrossRef]
- Grupper, A.; Katchman, E.; Ben-Yehoyada, M.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Shashar, M.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Kidney transplant recipients vaccinated before transplantation maintain superior humoral response to SARS-CoV-2 vaccine. Clin. Transplant. 2021, e14478. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. New Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Del Bello, A.; Abravanel, F.; Marion, O.; Couat, C.; Esposito, L.; Lavayssière, L.; Izopet, J.; Kamar, N. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am. J. Transpl. 2021. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, J.; Vrij, C.; Vermeersch, P.; Van Elslande, J.; Vets, S.; Lagrou, K.; Vos, R.; van Cleemput, J.; Jochmans, I.; Monbaliu, D.; et al. Liver and/or Kidney Transplantation After SARS-CoV-2 Infection. Transplantation 2021. [Google Scholar] [CrossRef]
- Sterlin, D.; Mathian, A.; Miyara, M.; Mohr, A.; Anna, F.; Claër, L.; Quentric, P.; Fadlallah, J.; Devilliers, H.; Ghillani, P.; et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci. Transl. Med. 2021, 13, 577. [Google Scholar] [CrossRef]
- Wisnewski, A.V.; Luna, J.C.; Redlich, C.A. Human IgG and IgA responses to COVID-19 mRNA vaccines. PLoS ONE 2021, 16, e0249499. [Google Scholar] [CrossRef]
- Ruether, D.F.; Schaub, G.M.; Duengelhoef, P.M.; Haag, F.; Brehm, T.T.; Fathi, A.; Wehmeyer, M.; Jahnke-Triankowski, J.; Mayer, L.; Hoffmann, A.; et al. SARS-CoV2-specific Humoral and T-cell Immune Response After Second Vaccination in Liver Cirrhosis and Transplant Patients. Clin. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef]
- Westhoff, T.H.; Seibert, F.S.; Anft, M.; Blazquez-Navarro, A.; Skrzypczyk, S.; Zgoura, P.; Meister, T.L.; Pfaender, S.; Stumpf, J.; Hugo, C.; et al. A third vaccine dose substantially improves humoral and cellular SARS-CoV-2 immunity in renal transplant recipients with primary humoral nonresponse. Kidney Int. 2021, 100, 1135–1136. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D. Humoral and cellular immune response and safety of two-dose SARS-CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transpl. 2021, 21, 3980–3989. [Google Scholar] [CrossRef] [PubMed]
- Sattler, A.; Schrezenmeier, E.; Weber, U.A.; Potekhin, A.; Bachmann, F.; Straub-Hohenbleicher, H.; Budde, K.; Storz, E.; Proß, V.; Bergmann, Y.; et al. Impaired humoral and cellular immunity after SARS-CoV-2 BNT162b2 (tozinameran) prime-boost vaccination in kidney transplant recipients. J. Clin. Investig. 2021, 131, e150175. [Google Scholar] [CrossRef] [PubMed]
- Lakota, K.; Perdan-Pirkmajer, K.; Hočevar, A.; Sodin-Semrl, S.; Rotar, Ž.; Čučnik, S.; Žigon, P. COVID-19 in Association with Development, Course, and Treatment of Systemic Autoimmune Rheumatic Diseases. Front. Immunol. 2021, 11, 611318. [Google Scholar] [CrossRef]




| Overall Cohort (N = 118) | IgG Positive (N = 92) | IgG Negative (N = 26) | p-Value | |
|---|---|---|---|---|
| Sex N (%) | 0.109 | |||
| Male | 75 (63.6) | 55 (59.8) | 20 (76.9) | |
| Female | 43 (36.4) | 37 (40.2) | 6 (23.1) | |
| Time since transplantation (years) | 0.186 | |||
| Mean | 14.4 | 14.8 | 12.9 | |
| Minimum | 0 | 0 | 0 | |
| Maximum | 37 | 32 | 37 | |
| Age at vaccination (years) | 0.232 | |||
| Mean | 66.1 | 65.1 | 69.4 | |
| Minimum | 28.0 | 28 | 42 | |
| Maximum | 89 | 84 | 89 | |
| Transplant indication N (%) | 0.006 | |||
| Alcohol-induced | 25 (21.1) | 13 (14.1) | 12 (46.2) | |
| Viral hepatitis | 28 (23.7) | 26 (28.3) | 2 (7.7) | |
| Tumor | 26 (22) | 19 (20.7) | 7 (26.9) | |
| Autoimmune | 18 (15.3) | 15 (16.3) | 3 (11.5) | |
| Cryptogenic | 4 (3.4) | 4 (4.3) | 0 (0) | |
| Other | 17 (14.4) | 15 (16.3) | 2 (7.7) | |
| Immunosuppression N (%) | 0.000270 | |||
| Tacrolimus mono | 42 (35.6) | 40 (43.5) | 2 (7.7) | |
| MMF mono | 16 (13.6) | 10 (10.5) | 6 (23.1) | |
| Tacrolimus + MMF | 24 (20.3) | 12 (13) | 12 (46.2) | |
| Tacrolimus and Everolimus | 15 (12.7) | 12 (13) | 3 (11.5) | |
| Everolimus mono | 1 (0.8) | 1 (1.1) | 0 (0.0) | |
| Ciclosporin + MMF | 3 (2.5) | 2 (2.2) | 1 (3.8) | |
| Ciclosporin mono | 2 (1.7) | 1 (1.1) | 1 (3.8) | |
| None | 14 (11.9) | 14 (15.2) | 0 (0) | |
| Tacrolimus + Azathioprin | 1 (0.8) | 0 (0) | 1 (3.8) | |
| MMF-based regimen | 40 (33.9) | 21 (22.8) | 19 (73.1) | 0.000002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timmermann, L.; Globke, B.; Lurje, G.; Schmelzle, M.; Schöning, W.; Öllinger, R.; Pratschke, J.; Eberspächer, B.; Drosten, C.; Hofmann, J.; et al. Humoral Immune Response following SARS-CoV-2 Vaccination in Liver Transplant Recipients. Vaccines 2021, 9, 1422. https://doi.org/10.3390/vaccines9121422
Timmermann L, Globke B, Lurje G, Schmelzle M, Schöning W, Öllinger R, Pratschke J, Eberspächer B, Drosten C, Hofmann J, et al. Humoral Immune Response following SARS-CoV-2 Vaccination in Liver Transplant Recipients. Vaccines. 2021; 9(12):1422. https://doi.org/10.3390/vaccines9121422
Chicago/Turabian StyleTimmermann, Lea, Brigitta Globke, Georg Lurje, Moritz Schmelzle, Wenzel Schöning, Robert Öllinger, Johann Pratschke, Bettina Eberspächer, Christian Drosten, Jörg Hofmann, and et al. 2021. "Humoral Immune Response following SARS-CoV-2 Vaccination in Liver Transplant Recipients" Vaccines 9, no. 12: 1422. https://doi.org/10.3390/vaccines9121422