
Preferences for Indoor Environmental and Social Comfort of Outpatient Staff during the COVID-19 Pandemic, an Explanatory Study


Abstract
:1. Introduction
1.1. Background
1.2. Objective
2. Materials and Methods
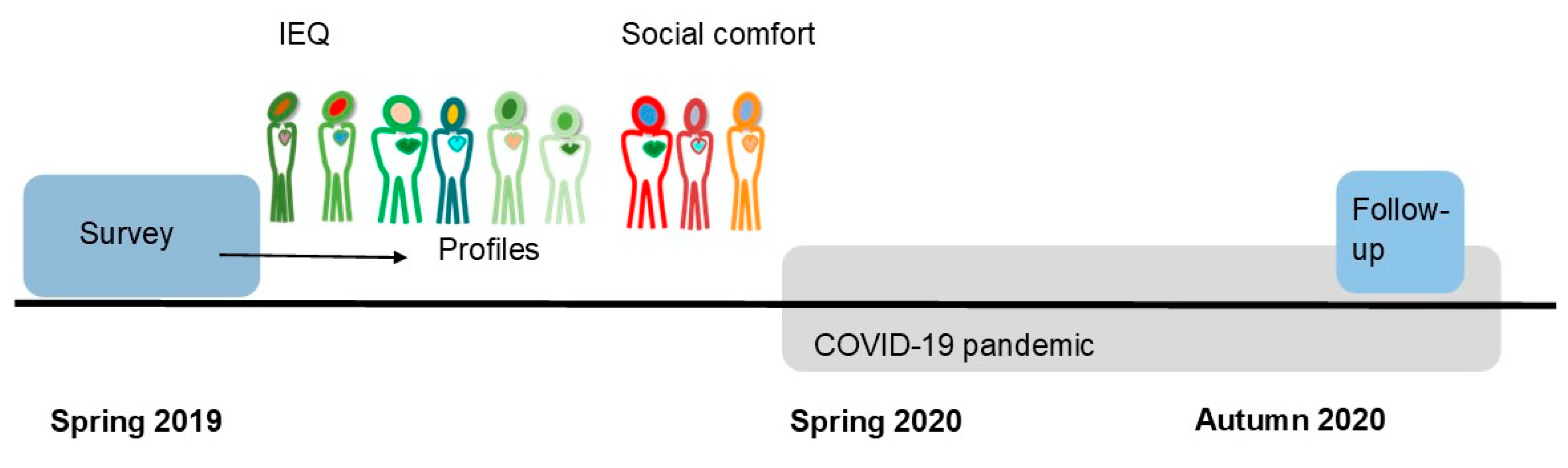
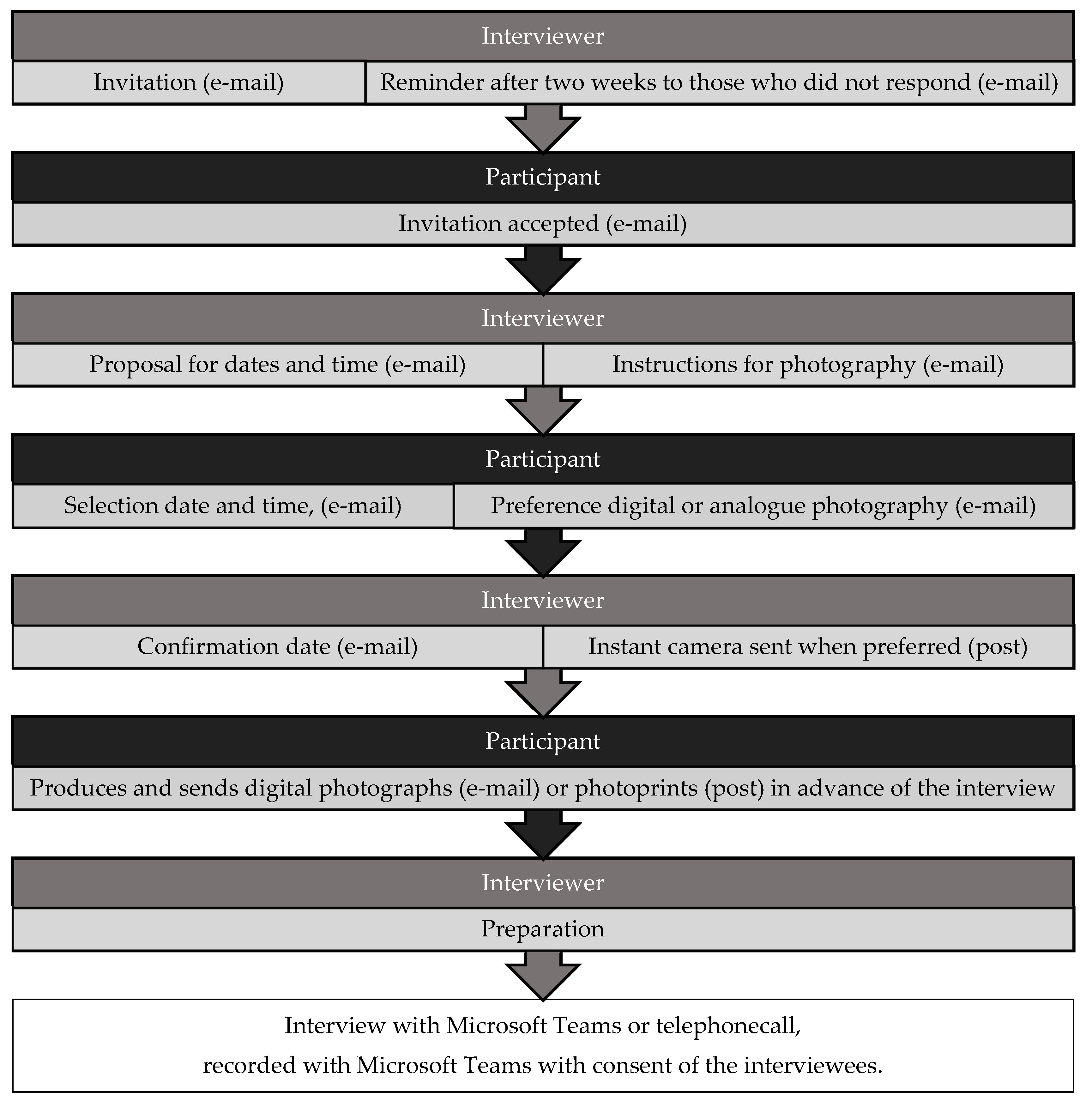
2.1. Study Design
2.2. Ethical Approval
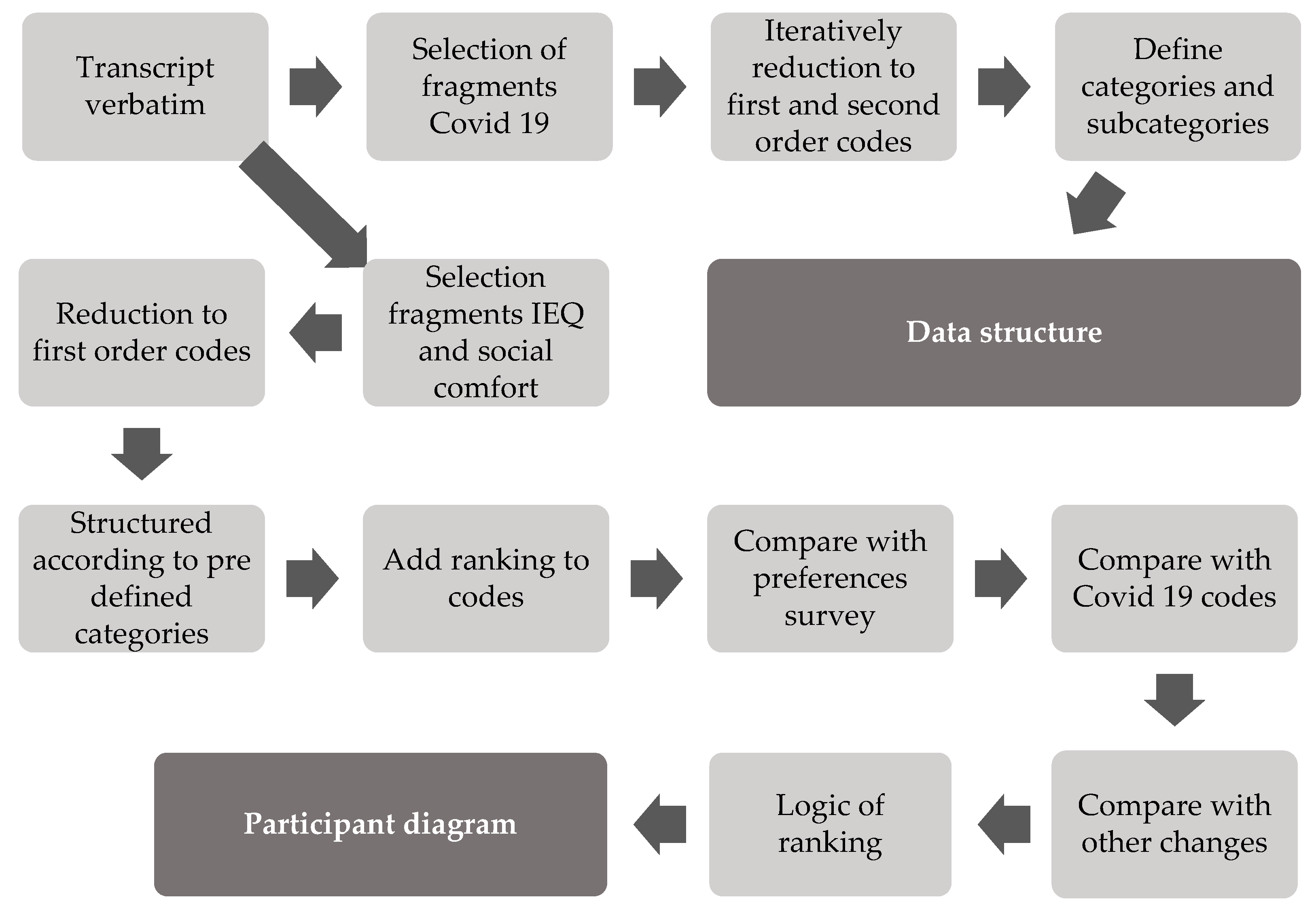
2.3. Data Analysis
3. Results
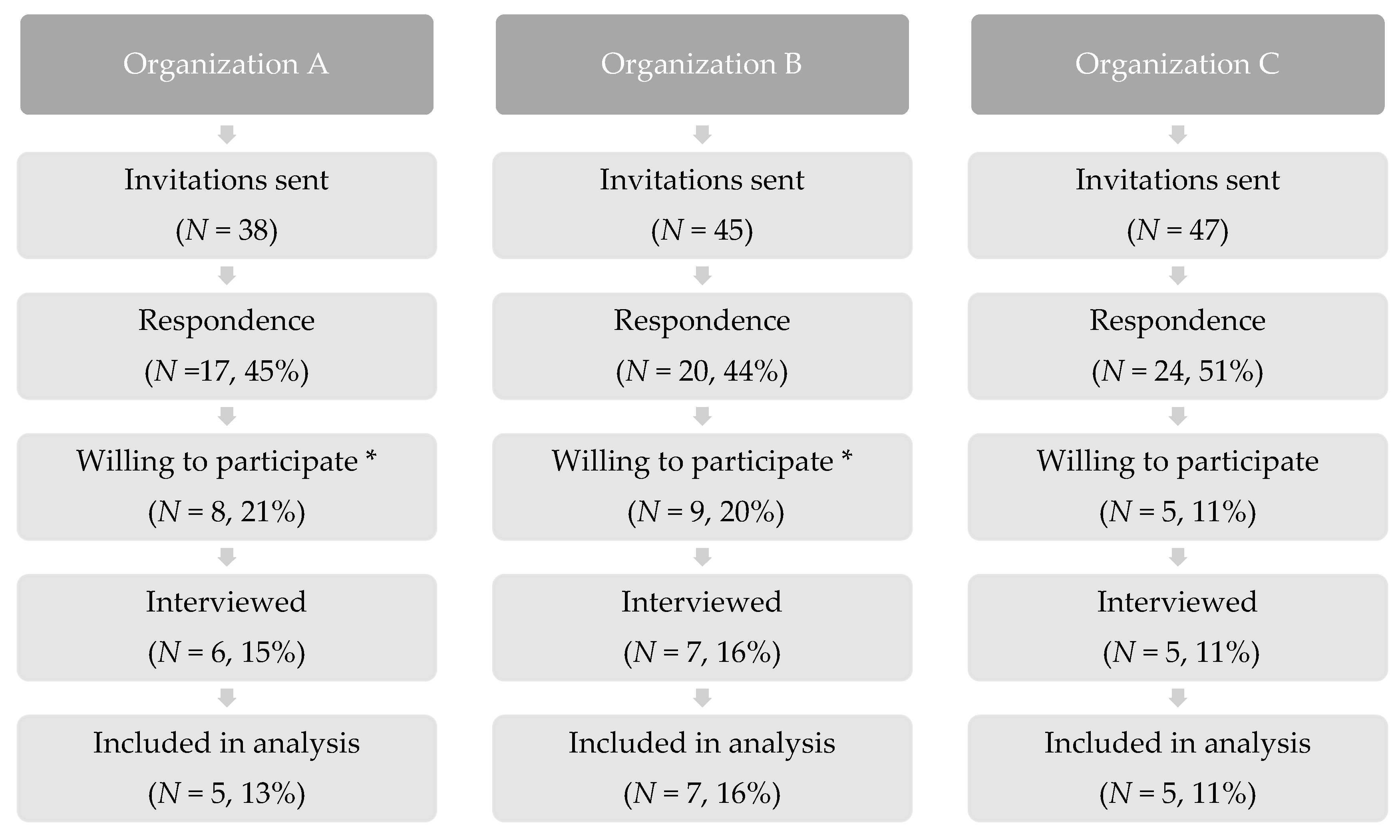
3.1. Participants
3.2. Changes Due to the Coronavirus Disease 2019 (COVID-19) Pandemic
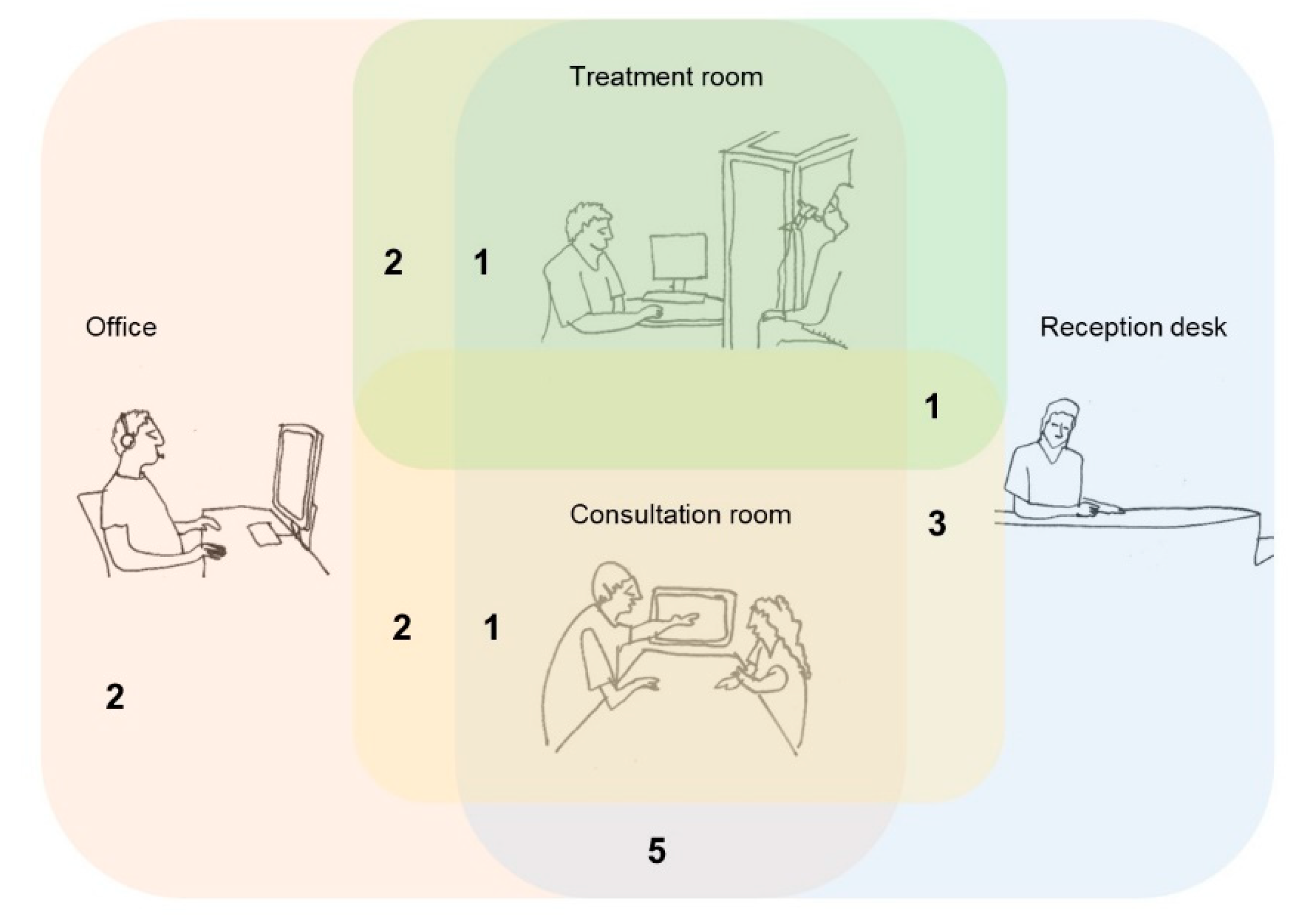
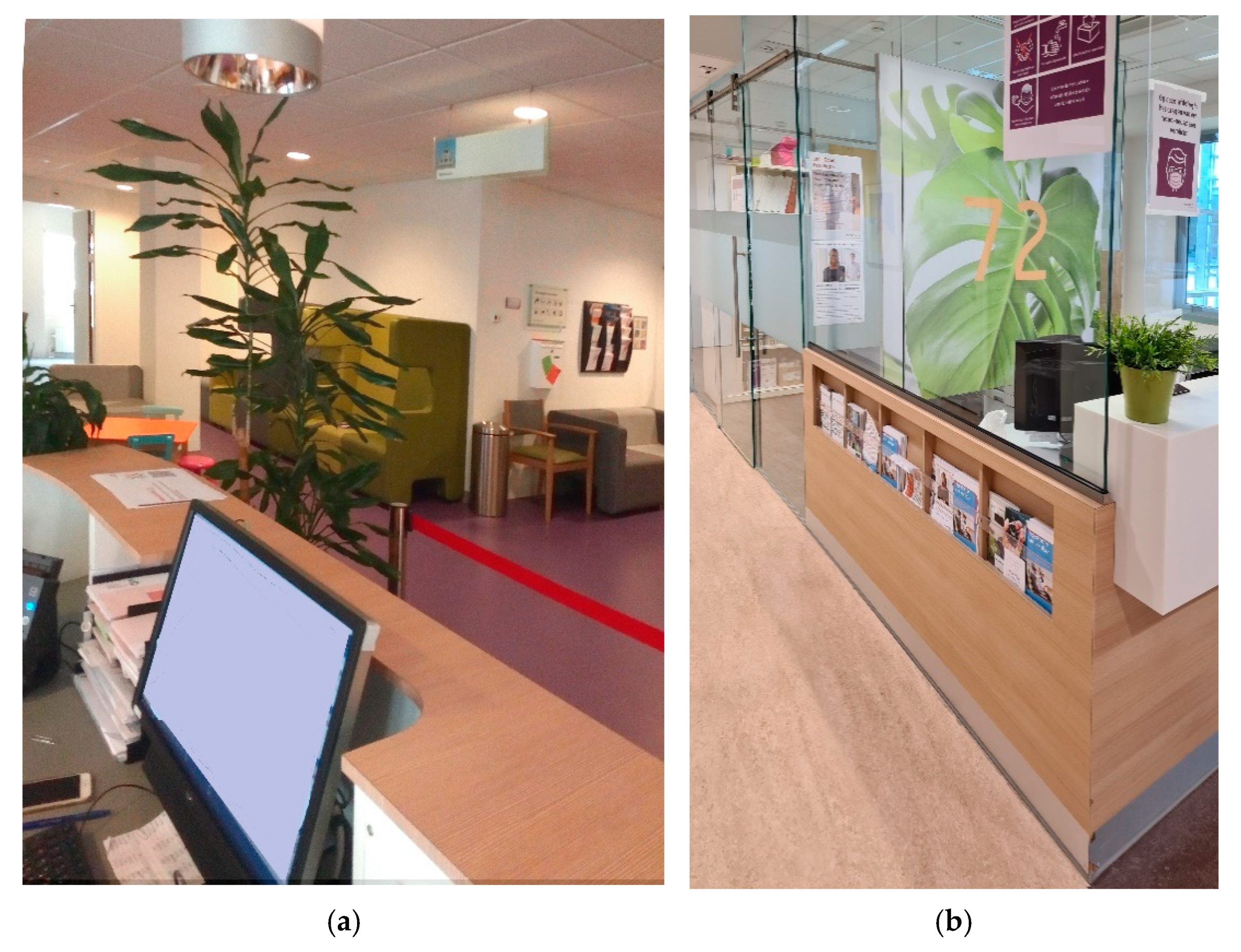
3.2.1. Context
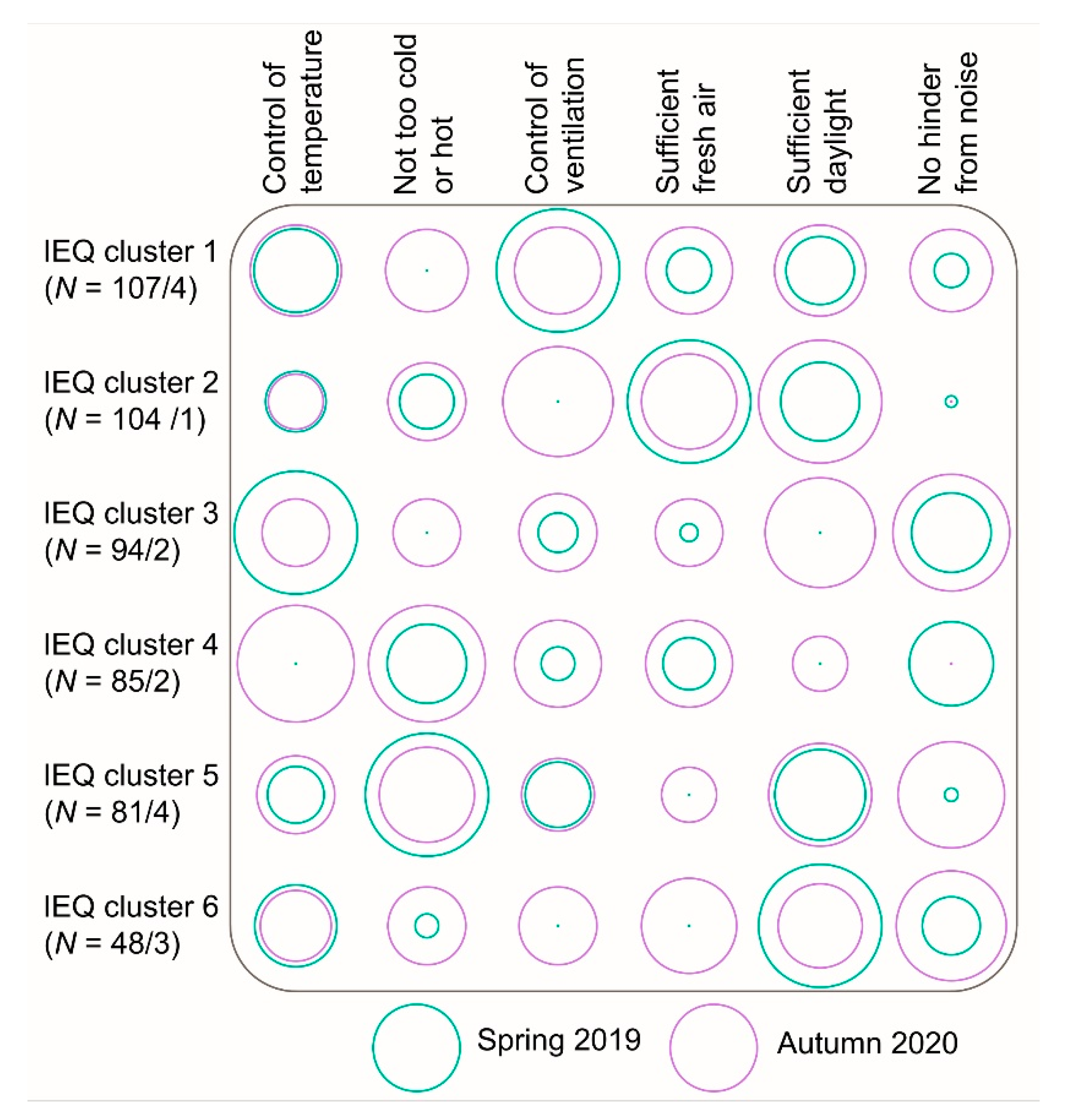
3.2.2. Indoor Environmental Quality
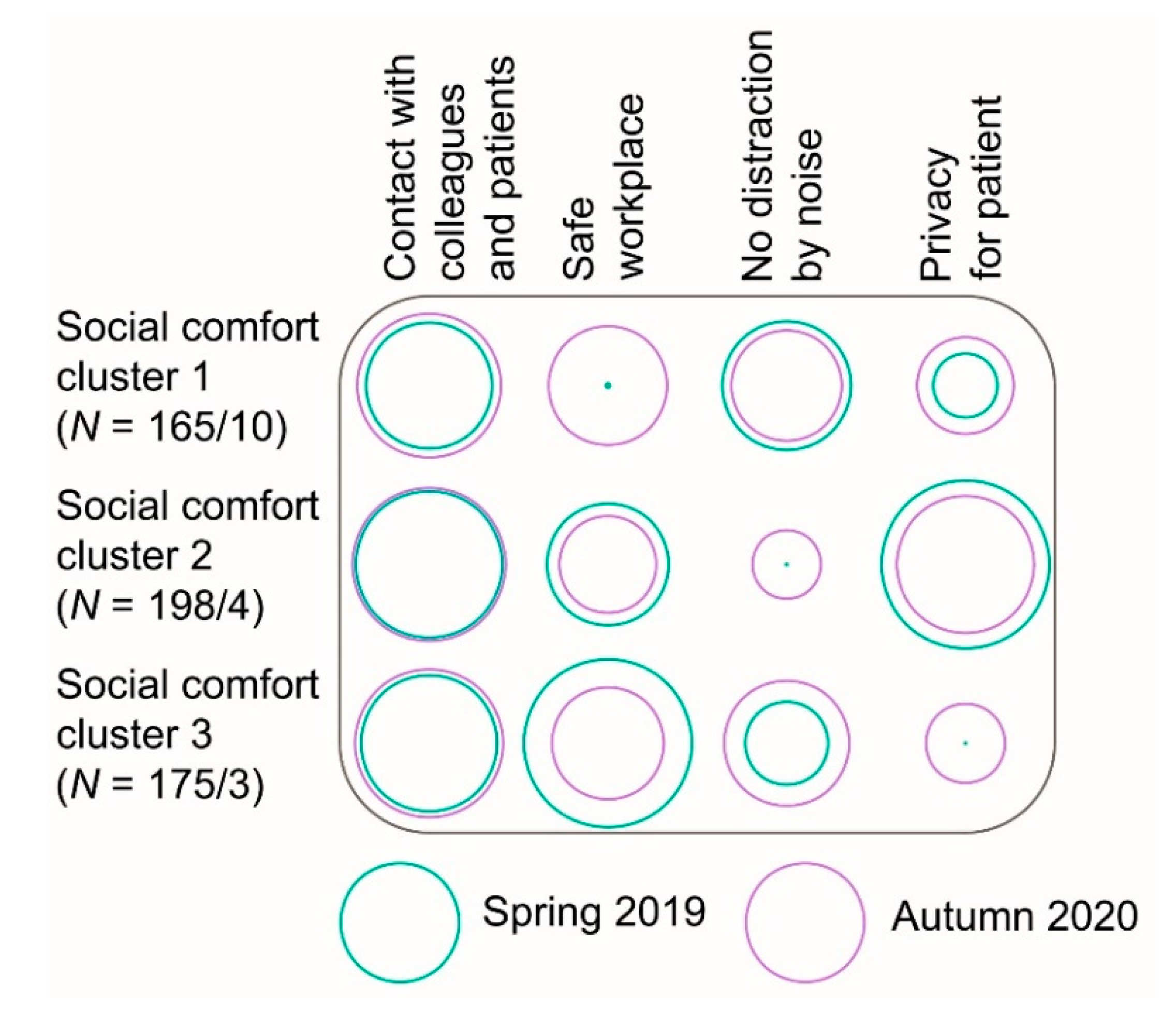
3.2.3. Social Comfort
4. Discussion
4.1. Explanation of the IEQ Clusters
4.2. Explanation of the Social Comfort Clusters
4.3. Changes of Preferences
4.4. IEQ in Relation to Changes Due to the COVID-19 Pandemic
4.5. Social Comfort in Relation to Changes Due to the COVID-19 Pandemic
4.6. Methodological Considerations
4.7. Limitations
4.8. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Subcategory | Second Order Codes |
|---|---|---|
| Organizational adaptations | Capacity care | Reduction capacity care during first wave of the pandemic (7) |
| Recent capacity care normal (4) | ||
| Capacity care not reduced during first wave (2) | ||
| Waiting list for patients after first wave (3) | ||
| Number of persons in hospital building | Number of workplaces reduced (4) | |
| Number of visitors reduced (4) | ||
| Number of patients reduced (3) | ||
| Working partly from home (5) | ||
| Spread staff among locations (2) | ||
| Adaptations work methods | Corona care | Determine corona policy (1) |
| Buddy corona care (2) | ||
| Perform corona tests in triage tent (2) | ||
| Digital care | Digital meeting (1) | |
| Digital consultation (4) | ||
| Prepare digital consultations (6) | ||
| Face-to-face care | Face-to-face consultation when urgent (3) | |
| Physical examination when urgent (3) | ||
| Decreased medical acts (2) | ||
| Adjusted workflow (2) | ||
| Increased disinfecting acts (2) | ||
| Physical adaptations | Room | Seating in waiting room reduced (3) |
| Stanchions in front of reception desk (5) | ||
| Amount of stuff reduced (1) | ||
| Location furniture adapted (3) | ||
| Splash guard installed (2) | ||
| Protective clothing | Use of facial mask | |
| Use of facial shield | ||
| Protective suit, glasses, and gloves (1) | ||
| Experience of changes | Work pressure | Increased work pressure (8) |
| Unchanged work pressure (4) | ||
| Increased work pressure during the first wave (4) | ||
| Suffering from Burn-out (1) | ||
| Stressed feelings (2) | ||
| Satisfaction with work | Adjusted to new work method (3) | |
| Annoyed by extra administration (4) | ||
| Worries about quality patientcare (3) | ||
| Worries about infection (4) | ||
| Satisfied with organization (1) | ||
| Unsafe feelings because of dirt and dust (1) | ||
| Social comfort | Social distancing difficult (6) | |
| Missing face-to-face contact (8) | ||
| Preferred to see facial expression (3) | ||
| Increased privacy (1) | ||
| Less annoyance by aggression (1) | ||
| Annoyance by aggression (4) | ||
| Indoor environment | Missing control of ventilation (4) | |
| Decreased intelligibility through facial mask or splashguard (3) | ||
| Preferred natural ventilation (3) | ||
| Decreased discussion about control of temperature (1) | ||
| Breathing difficulties through facemask (1) | ||
| Protective suit too hot (1) | ||
| Facial shield reflects light in screen (1) |
References
- Barker, R. 2030—The Future of Medicine, Avoiding a Medical Meltdown; Oxford University Press Inc.: New York, NY, USA, 2011; p. 118. ISBN 978-0-19-960066-3. [Google Scholar]
- CBS. Werknemers in de Zorg en Welzijn; Arbeidsomstandigheden. 2019. Available online: https://azwstatline.cbs.nl/#/AZW/nl/dataset/24069NED/table?ts=1578064277911 (accessed on 1 March 2020).
- Shader, K.; Broome, M.E.; Broome, C.D.; West, M.E.; Nash, M. Factors Influencing Satisfaction and Anticipated Turnover for Nurses in an Academic Medical Center. JONA J. Nurs. Adm. 2001, 31, 210–216. [Google Scholar] [CrossRef]
- Grunfeld, E.; Whelan, T.J.; Zitzelsberger, L.; Willan, A.R.; Montesanto, B.; Evans, W.K. Cancer care workers in Ontario: Prev-alence of burnout, job stress and job satisfaction. Can. Med. Assoc. J. 2000, 163, 166–169. [Google Scholar]
- McVicar, A. Workplace stress in nursing: A literature review. J. Adv. Nurs. 2003, 44, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Vischer, J.C. The effects of the physical environment on job performance: Towards a theoretical model of workspace stress. Stress Health 2007, 23, 175–184. [Google Scholar] [CrossRef]
- Applebaum, D.; Fowler, S.; Fiedler, N.; Osinubi, O.; Robson, M. The Impact of Environmental Factors on Nursing Stress, Job Satisfaction, and Turnover Intention. JONA J. Nurs. Adm. 2010, 40, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alimoglu, M.K.; Donmez, L. Daylight exposure and the other predictors of burnout among nurses in a University Hospital. Int. J. Nurs. Stud. 2005, 42, 549–555. [Google Scholar] [CrossRef]
- Hashiguchi, N.; Hirakawa, M.; Tochihara, Y.; Kaji, Y.; Karaki, C. Thermal Environment and Subjective Responses of Patients and Staff in a Hospital during Winter. J. Physiol. Anthropol. Appl. Hum. Sci. 2005, 24, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Eijkelenboom, A.; Blok, G.A. Evaluation of design interventions for hospitality and privacy at inpatient wards. In Proceedings of the ARCH 2019, Trondheim, Norway, 12–14 June 2019; SINTEF Academic Press: Trondheim, Norway. [Google Scholar]
- Eijkelenboom, A.; Blok, G.A.; Bluyssen, P.M. Comfort and satisfaction of patients, visitors and staff with patient rooms at inpatient wards, a pilot study. In Proceedings of the CLIMA 2019, E3S Web Conference, Bucharest, Romania, 26–29 May 2019. [Google Scholar]
- Tähtinen, K.; Remes, J.; Karvala, K.; Salmi, K.; Lahtinen, M.; Reijula, K. Perceived indoor air quality and psychosocial work environment in office, school and health care environments in Finland. Int. J. Occup. Med. Environ. Health 2020, 33, 479–495. [Google Scholar] [CrossRef]
- Hellgren, U.-M.; Reijula, K. Indoor-air-related complaints and symptoms among hospital workers. SJWEH Suppl. 2006, 2, 47–49. [Google Scholar]
- Shin, J.-H. Toward a theory of environmental satisfaction and human comfort: A process-oriented and contextually sensitive theoretical framework. J. Environ. Psychol. 2016, 45, 11–21. [Google Scholar] [CrossRef]
- Cole, R.J.; Robinson, J.; Brown, Z.; O’Shea, M. Re-contextualizing the notion of comfort. Build. Res. Inf. 2008, 36, 323–336. [Google Scholar] [CrossRef]
- Willems, S.; Saelens, D.; Heylighen, A. Comfort requirements versus lived experience: Combining different research approaches to indoor environmental quality. Arch. Sci. Rev. 2020, 63, 316–324. [Google Scholar] [CrossRef]
- Donetto, S.; Penfold, C.; Anderson, J.; Robert, G.; Maben, J. Nursing work and sensory experiences of hospital design: A before and after qualitative study following a move to all-single room inpatient accommodation. Health Place 2017, 46, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Pattison, H.M.; E Robertson, C. The effect of ward design on the well-being of post-operative patients. J. Adv. Nurs. 1996, 23, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Dean, M.; Gill, R.; Barbour, J.B. “Let’s Sit Forward”: Investigating Interprofessional Communication, Collaboration, Professional Roles, and Physical Space at EmergiCare. Health Commun. 2016, 31, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Zimring, C. A Review of the Empirical Literature on the Relationships Between Indoor Environment and Stress in Health Care and Office Settings. Environ. Behav. 2008, 40, 151–190. [Google Scholar] [CrossRef]
- Eijkelenboom, A.; Bluyssen, P.M. Comfort and health of patients and staff, related to the physical environment of different departments in hospitals: A literature review. Intell. Build. Int. 2019. [Google Scholar] [CrossRef] [Green Version]
- Eijkelenboom, A.; Kim, D.H.; Bluyssen, P.M. First results of self-reported health and comfort of staff in outpatient areas of hospitals in the Netherlands. Build. Environ. 2020, 177, 106871. [Google Scholar] [CrossRef]
- Bluyssen, P.M. Towards an integrated analysis of the indoor environmental factors and its effects on occupants. Intell. Build. Int. 2019, 12, 199–207. [Google Scholar] [CrossRef]
- Tkaczynski, A. Segmentation Using Two-Step Cluster Analysis. In Segmentation in Social Marketing: Process, Methods and Ap-plication; Dietrich, T., Rundle-Thiele, S., Kubacki, K., Eds.; Springer: Singapore, 2017; pp. 109–125. ISBN 978-981-10-1835-0. [Google Scholar]
- Eijkelenboom, A.; Bluyssen, P.M. Profiling outpatient staff based on their self-reported comfort and preferences of indoor environmental quality and social comfort in six hospitals. Build. Environ. 2020, 184, 107220. [Google Scholar] [CrossRef]
- Mourshed, M.; Zhao, Y. Healthcare providers’ perception of design factors related to physical environments in hospitals. J. Environ. Psychol. 2012, 32, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Sadatsafavi, H.; Walewski, J.; Shepley, M.M. Factors influencing evaluation of patient areas, work spaces, and staff areas by healthcare professionals. Indoor Built Environ. 2015, 24, 439–456. [Google Scholar] [CrossRef]
- Karjalainen, S.; Koistinen, O. User problems with individual temperature control in offices. Build. Environ. 2007, 42, 2880–2887. [Google Scholar] [CrossRef]
- Healey, K.; Webster-Mannison, M. Exploring the influence of qualitative factors on the thermal comfort of office occupants. Arch. Sci. Rev. 2012, 55, 169–175. [Google Scholar] [CrossRef]
- Van Hoof, J.; Bennetts, H.; Hansen, A.; Kazak, J.K.; Soebarto, V. The Living Environment and Thermal Behaviours of Older South Australians: A Multi-Focus Group Study. Int. J. Environ. Res. Public Health 2019, 16, 935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eon, C.; Morrison, G.M.; Byrne, J. Unraveling everyday heating practices in residential homes. Energy Procedia 2017, 121, 198–205. [Google Scholar] [CrossRef]
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). 2019. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 21 March 2021).
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.; Sham, P.C.; Chua, S.E.; Wong, J.G. Immediate and Sustained Psychological Impact of an Emerging Infectious Disease Outbreak on Health Care Workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Belfroid, E.; van Steenbergen, J.; Timen, A.; Ellerbroek, P.; Huis, A.; Hulscher, M. Preparedness and the importance of meeting the needs of healthcare workers: A qualitative study on Ebola. J. Hosp. Infect. 2018, 98, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Khan, F.A.; Napolean, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Aalto, L.; Lappalainen, S.; Salonen, H.; Reijula, K. Usability evaluation (IEQ survey) in hospital buildings. Int. J. Work. Health Manag. 2017, 10, 265–282. [Google Scholar] [CrossRef]
- Amaratunga, D.; Baldry, D.; Sarshar, M.; Newton, R. Quantitative and qualitative research in the built environment: Application of “mixed” research approach. Work. Study 2002, 51, 17–31. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design Qualitative, Quantitative, And Mixed Methods Approaches, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2014; ISBN 978-4129-6556-9. [Google Scholar]
- Johnson, R.B.; Onwuegbuzie, A. Mixed Methods Research: A Research Paradigm Whose Time Has Come. Educ. Res. 2004, 33, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP. 2018. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 1 October 2020).
- Wilhoit, E.D. Photo and Video Methods in Organizational and Managerial Communication Research. Manag. Commun. Q. 2017, 31, 447–466. [Google Scholar] [CrossRef]
- Van Hoof, J.; Verbeek, H.; Janssen, B.M.; Eijkelenboom, A.; Molony, S.L.; Felix, E.; Nieboer, K.A.; Zwerts-Verhelst, E.L.M.; Sijstermans, J.J.W.M.; Wouters, E.J.M. A three perspective study of the sense of home of nursing home residents: The views of residents, care professionals and relatives. BMC Geriatr. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annemans, M.; Van Audenhove, C.; Vermolen, H.; Heylighen, A. Hospital Reality from a Lying Perspective: Exploring a Sensory Research Approach. In Designing Inclusive Systems; Langdon, P., Clarkson, J., Robinson, P., Lazar, J., Heylighen, A., Eds.; Springer: London, UK, 2012; pp. 3–12. [Google Scholar] [CrossRef]
- Barriball, K.L.; While, A. Collecting data using a semi-structured interview: A discussion paper. J. Adv. Nurs. 1994, 19, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Kallio, H.; Pietilä, A.-M.; Johnson, M.; Kangasniemi, M. Systematic methodological review: Developing a framework for a qualitative semi-structured interview guide. J. Adv. Nurs. 2016, 72, 2954–2965. [Google Scholar] [CrossRef]
- Gioia, D.A.; Corley, K.G.; Hamilton, A.L. Seeking Qualitative Rigor in Inductive Research: Notes on the Gioia Methodology. Organizational Research. Organ. Res. Methods 2013, 16, 15–31. [Google Scholar] [CrossRef]
- Eldh, A.C.; Årestedt, L.; Berterö, C. Quotations in Qualitative Studies: Reflections on Constituents, Custom, and Purpose. Int. J. Qual. Methods 2020, 19. [Google Scholar] [CrossRef]
- Anderson, C. Presenting and Evaluating Qualitative Research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.M.; Jackson, J.M. Qualitative Data Analysis: Challenges and Dilemmas Related to Theory and Method. Am. J. Occup. Ther. 2003, 57, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amir, O.; Levav, J. Choice Construction versus Preference Construction: The Instability of Preferences Learned in Context. J. Mark. Res. 2008, 45, 145–158. [Google Scholar] [CrossRef]
- Zajonc, R.B.; Markus, H. Affective and Cognitive Factors in Preferences. J. Consum. Res. 1982, 9, 123–131. [Google Scholar] [CrossRef]
- Tversky, A.; Simonson, I. Context-Dependent Preferences. Manag. Sci. 1993, 39, 1179–1189. [Google Scholar] [CrossRef]
- Sharot, T.; De Martino, B.; Dolan, R.J. How Choice Reveals and Shapes Expected Hedonic Outcome. J. Neurosci. 2009, 29, 3760–3765. [Google Scholar] [CrossRef]
- Hoeffler, S.; Ariely, D. Constructing Stable Preferences: A Look into Dimensions of Experience and Their Impact on Preference Stability. J. Consum. Psychol. 1999, 8, 113–139. [Google Scholar] [CrossRef]
- Mroczek, J.; Mikitarian, G.; Vieira, E.K.; Rotarius, T. Hospital Design and Staff Perceptions. Health Care Manag. 2005, 24, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Bahnfleth, W.; Bluyssen, P.; Buonanno, G.; Jimenez, J.; Kurnitski, J.; Li, Y.; Miller, S.; Sekhar, C.; Morawska, L.; et al. Dismantling myths on the airborne transmission of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J. Hosp. Infect. 2021, 110, 89–96. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, H.; Chen, Y.; He, J.; Chen, L.; Liu, Y.; Hu, X.; Li, A.; Liu, S.; Zhang, P.; et al. Clinical Data on Hospital Environmental Hygiene Monitoring and Medical Staff Protection during the Coronavirus Disease 2019 Outbreak. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef]
- Rashid, M. Hospital Design and Face to Face Interaction among Clinicians: A Theoretical Model. HERD Health Environ. Res. Des. J. 2009, 2, 62–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaney, G.; Jacob, S.; Iedema, R.; Winters, M.; Barton, M. Comparison of face-to-face and videoconferenced multidisciplinary clinical meetings. Australas. Radiol. 2004, 48, 487–492. [Google Scholar] [CrossRef]
- Crawford, A.; Serhal, E. Digital Health Equity and COVID-19: The Innovation Curve Cannot Reinforce the Social Gradient of Health. J. Med. Internet Res. 2020, 22, e19361. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of Telehealth During the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- Romanick-Schmiedl, S.; Raghu, G. Telemedicine—Maintaining quality during times of transition. Nat. Rev. Dis. Prim. 2020, 6, 45. [Google Scholar] [CrossRef]
- Rosen, C.B.; Joffe, S.; Kelz, R.R. COVID-19 Moves Medicine into a Virtual Space: A Paradigm Shift from Touch to Talk to Establish Trust. Ann. Surg. 2020, 272, e159–e160. [Google Scholar] [CrossRef]
- Kim, J.; de Dear, R. Nonlinear relationships between individual IEQ factors and overall workspace satisfaction. Build. Environ. 2011, 49, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Harzing, A.-W.; Baldueza, J.; Barner-Rasmussen, W.; Barzantny, C.; Canabal, A.; Davila, A.; Espejo, A.; Ferreira, R.; Giroud, A.; Koester, K.; et al. Rating versus ranking: What is the best way to reduce response and language bias in cross-national research? Int. Bus. Rev. 2009, 18, 417–432. [Google Scholar] [CrossRef] [Green Version]
- Yannakakis, G.N.; Martínez, H.P. Ratings are Overrated! Front. ICT 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- Derks, M.; Mishra, A.; Loomans, M.; Kort, H. Understanding thermal comfort perception of nurses in a hospital ward work environment. Build. Environ. 2018, 140, 119–127. [Google Scholar] [CrossRef]
- Lembo, M.; Vedetta, C.; Moscato, U.; del Gaudio, M. Thermal discomfort in healthcare workers during the COVID-19 pandemic. Med. Lavoro 2021, 112, 123–129. [Google Scholar] [CrossRef]
- Awada, M.; Becerik-Gerber, B.; Hoque, S.; O’Neill, Z.; Pedrielli, G.; Wen, J.; Wu, T. Ten questions concerning occupant health in buildings during normal operations and extreme events including the COVID-19 pandemic. Build. Environ. 2021, 188, 107480. [Google Scholar] [CrossRef]
- Jain, N.; Burman, E.; Stamp, S.; Shrubsole, C.; Bunn, R.; Oberman, T.; Barrett, E.; Aletta, F.; Kang, J.; Raynham, P.; et al. Building Performance Evaluation of a New Hospital Building in the UK: Balancing Indoor Environmental Quality and Energy Performance. Atmosphere 2021, 12, 115. [Google Scholar] [CrossRef]
- Lupo, R.; Lezzi, A.; Conte, L.; Santoro, P.; Carvello, M.; Artioli, G.; Calabrò, A.; Caldararo, C.; Botti, S.; Carriero, M.C. Work environment and related burnout levels: Survey among healthcare workers in two hospitals of Southern Italy: Work environment and related burnout levels among healthcare workers. Acta Biomed. 2021, 92 (Suppl. 2), e2021009. [Google Scholar] [CrossRef]
- Shreffler, J.; Huecker, M.; Petrey, J. The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West. J. Emerg. Med. 2020, 21, 1059–1066. [Google Scholar] [CrossRef]
- Karanikola, P.; Andrea, V.; Tampakis, S.; Tsolakidou, A. Indoor and Outdoor Design in Healthcare Environments: The Employees’ Views in the General University Hospital of Alexandroupolis, Greece. Environments 2020, 7, 61. [Google Scholar] [CrossRef]








| Main Topic | Subtopics | Shared Documents |
|---|---|---|
| Introduction | ||
| Work-related aspects | Room, room type, number of persons in room, function, job tasks, department, location | |
| Changes due to the pandemic | Activities, work pressure, physical changes, other | |
| Preferences IEQ | Thermal, ventilation, lighting, noise | Photographs |
| Preferences social comfort | Contact, safety, privacy, distraction | Photographs |
| Ranking preferences | Order of importance Logic to distinguish preferences | List of ranking IEQ and social comfort |
| Other issues related to comfort | ||
| Closing |
| Most Important Aspect | 2020 | Same Preference in 2019 | |
|---|---|---|---|
| N | N | ||
| Indoor Environmental Quality (IEQ) IEQ | Sufficient fresh air | 1 | 1 |
| Control of ventilation | 2 | 2 | |
| Not too cold or hot | 3 | 2 * | |
| Control of temperature | 1 | 1 | |
| Sufficient daylight | 5 | 1 | |
| No annoyance by noise | 5 | 2 | |
| Total IEQ | 17 | 9 | |
| Social comfort | Sufficient contact | 7 | 7 |
| No distraction by noise | 3 | 2 | |
| Privacy for patients | 4 | 1 | |
| Safe workplace | 3 | 0 | |
| Total Social comfort | 17 | 10 |
| Category | Subcategory | Example |
|---|---|---|
| Organizational adaptations | Capacity | Reduction capacity during first wave of the pandemic |
| Number of persons in hospital building | Working partly from home | |
| Adaptations work methods | Corona care | Perform corona tests in triage tent |
| Digital care | Prepare digital consultations | |
| Face-to-face care | Physical examination when urgent | |
| Physical adaptations | Room | Stanchions in front of reception desk |
| Protective clothing | Use of facial mask | |
| Personal experiences | Work-pressure | Increased work pressure |
| Satisfaction with work | Annoyed by extra administration | |
| Indoor Environmental Quality (IEQ) | Missing control of ventilation | |
| Social comfort | Missing face-to-face contact |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eijkelenboom, A.; Ortiz, M.A.; Bluyssen, P.M. Preferences for Indoor Environmental and Social Comfort of Outpatient Staff during the COVID-19 Pandemic, an Explanatory Study. Int. J. Environ. Res. Public Health 2021, 18, 7353. https://doi.org/10.3390/ijerph18147353
Eijkelenboom A, Ortiz MA, Bluyssen PM. Preferences for Indoor Environmental and Social Comfort of Outpatient Staff during the COVID-19 Pandemic, an Explanatory Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7353. https://doi.org/10.3390/ijerph18147353
Chicago/Turabian StyleEijkelenboom, AnneMarie, Marco A. Ortiz, and Philomena M. Bluyssen. 2021. "Preferences for Indoor Environmental and Social Comfort of Outpatient Staff during the COVID-19 Pandemic, an Explanatory Study" International Journal of Environmental Research and Public Health 18, no. 14: 7353. https://doi.org/10.3390/ijerph18147353