
Measuring COVID-19 Related Health Literacy in Healthcare Professionals—Psychometric Evaluation of the HL-COV-HP Instrument

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Measure
2.3. Analysis
2.3.1. Descriptive Measures
2.3.2. Exploratory Factor Analysis
2.3.3. Confirmatory Factor Analysis
2.3.4. Internal Consistency and Convergent Validity
3. Results
3.1. Sample Characteristics and Descriptive Results
3.2. Exploratory Factor Analysis
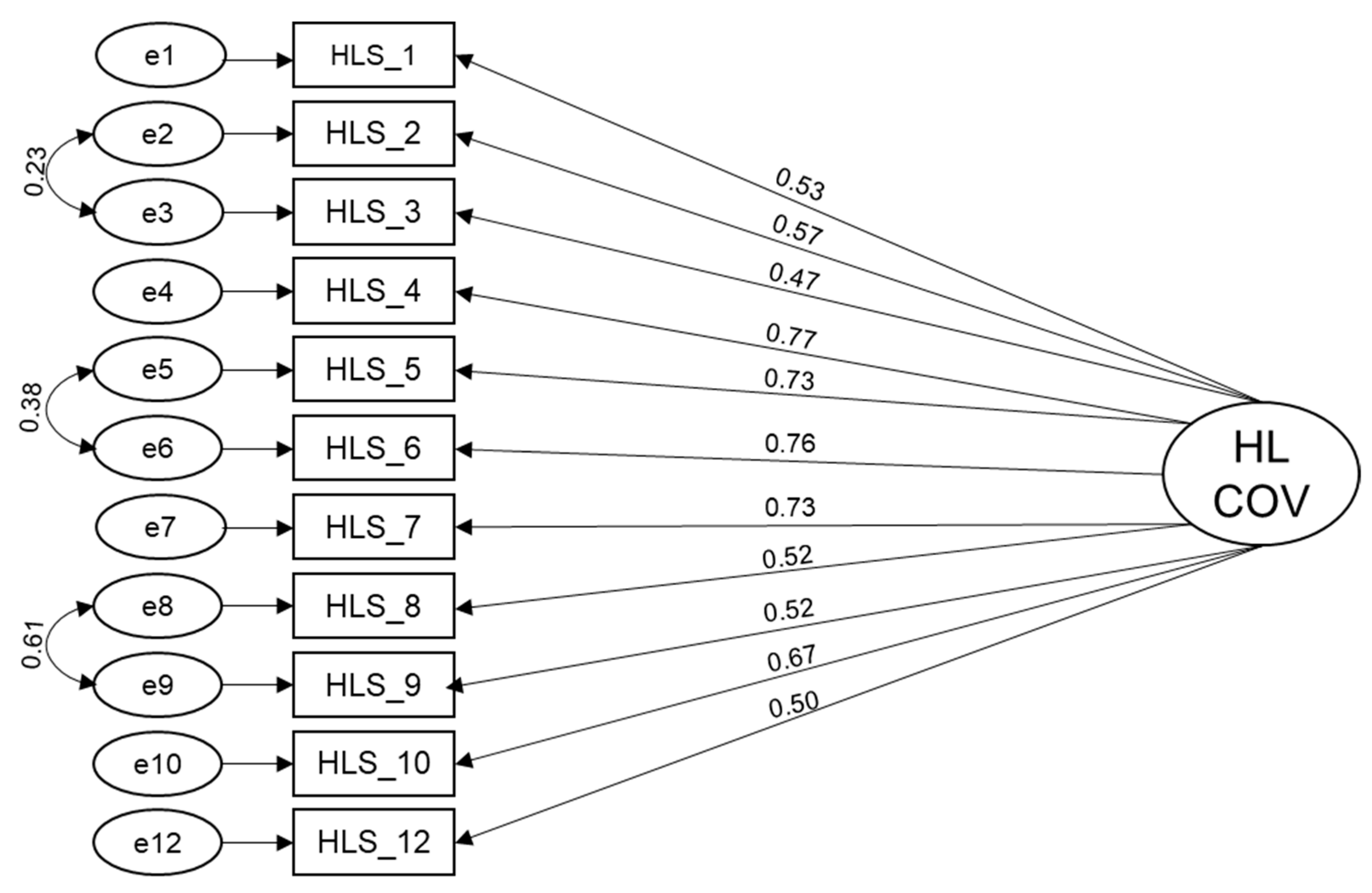
3.3. Confirmatory Factor Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sørensen, K.; van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squiers, L.; Peinado, S.; Berkman, N.; Boudewyns, V.; McCormack, L. The health literacy skills framework. J. Health Commun. 2012, 17 (Suppl. 3), 30–54. [Google Scholar] [CrossRef]
- COVID-HL Network. Health Literacy in Times of COVID-19. Available online: https://covid-hl.eu/ (accessed on 12 November 2021).
- Okan, O.; Bollweg, T.M.; Berens, E.-M.; Hurrelmann, K.; Bauer, U.; Schaeffer, D. Coronavirus-Related Health Literacy: A Cross-Sectional Study in Adults during the COVID-19 Infodemic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 5503. [Google Scholar] [CrossRef]
- McCaffery, K.J.; Dodd, R.H.; Cvejic, E.; Ayrek, J.; Batcup, C.; Isautier, J.M.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; et al. Health literacy and disparities in COVID-19-related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pract. 2020, 30, e30342012. [Google Scholar] [CrossRef]
- Paakkari, L.; Okan, O. COVID-19: Health literacy is an underestimated problem. Lancet Public Health 2020, 5, e249–e250. [Google Scholar] [CrossRef]
- Abel, T.; McQueen, D. Critical health literacy and the COVID-19 crisis. Health Promot. Int. 2020, 35, 1612–1613. [Google Scholar] [CrossRef]
- Gautam, V.; Dileepan, S.; Rustagi, N.; Mittal, A.; Patel, M.; Shafi, S.; Thirunavukkarasu, P.; Raghav, P. Health literacy, preventive COVID 19 behaviour and adherence to chronic disease treatment during lockdown among patients registered at primary health facility in urban Jodhpur, Rajasthan. Diabetes Metab. Syndr. 2021, 15, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.J.; Santos, P. The Impact of Health Literacy on Knowledge and Attitudes towards Preventive Strategies against COVID-19: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5421. [Google Scholar] [CrossRef]
- Li, X.; Neter, E.; Dadaczynski, K.; Li, S.; Cui, G.; Kaminga, A.C.; Cheng, S.; Xu, H. Associations Between Health Literacy, eHealth Literacy, and COVID-19–Related Health Behaviors Among Chinese College Students: Cross-sectional Online Study. J. Med. Internet Res. 2021, 23, e25600. [Google Scholar] [CrossRef] [PubMed]
- Patil, U.; Kostareva, U.; Hadley, M.; Manganello, J.A.; Okan, O.; Dadaczynski, K.; Massey, P.M.; Agner, J.; Sentell, T. Health Literacy, Digital Health Literacy, and COVID-19 Pandemic Attitudes and Behaviors in U.S. College Students: Implications for Interventions. Int. J. Environ. Res. Public Health 2021, 18, 3301. [Google Scholar] [CrossRef]
- Hermans, L.; van den Broucke, S.; Gisle, L.; Demarest, S.; Charafeddine, R. Mental health, compliance with measures and health prospects during the COVID-19 epidemic: The role of health literacy. BMC Public Health 2021, 21, 1365. [Google Scholar] [CrossRef]
- Hong, K.J.; Park, N.L.; Heo, S.Y.; Jung, S.H.; Lee, Y.B.; Hwang, J.H. Effect of e-Health Literacy on COVID-19 Infection-Preventive Behaviors of Undergraduate Students Majoring in Healthcare. Healthcare 2021, 9, 573. [Google Scholar] [CrossRef]
- Niu, Z.; Qin, Z.; Hu, P.; Wang, T. Health Beliefs, Trust in Media Sources, Health Literacy, and Preventive Behaviors among High-Risk Chinese for COVID-19. Health Commun. 2021, 1–9. [Google Scholar] [CrossRef]
- Neter, E.; He, D.; Guo, Z.; Zhao, S.Z.; Guo, N.; Wu, Y.; Weng, X.; Wong, J.Y.-H.; Lam, T.H.; Wang, M.P. Socioeconomic Disparities in eHealth Literacy and Preventive Behaviors During the COVID-19 Pandemic in Hong Kong: Cross-sectional Study. J. Med. Internet Res. 2021, 23, e24577. [Google Scholar] [CrossRef]
- Montagni, I.; Ouazzani-Touhami, K.; Mebarki, A.; Texier, N.; Schück, S.; Tzourio, C. Acceptance of a Covid-19 vaccine is associated with ability to detect fake news and health literacy. J. Public Health Oxf. Engl. 2021. [Google Scholar] [CrossRef]
- Turhan, Z.; Dilcen, H.Y.; Dolu, İ. The mediating role of health literacy on the relationship between health care system distrust and vaccine hesitancy during COVID-19 pandemic. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Schug, C.; Erim, Y.; Geiser, F.; Hiebel, N.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Steudte-Schmiedgen, S.; Borho, A.; et al. Bereitschaft zur COVID-19-Impfung unter Beschäftigten im Gesundheitswesen in Deutschland: Befragungsergebnisse aus dem Netzwerk Universitätsmedizin (NUM), November 2020 bis Januar 2021. Bundesgesundheitsblatt Gesundh. Gesundh. 2021. [Google Scholar] [CrossRef]
- Greer, M.L.; Sample, S.; Jensen, H.K.; McBain, S.; Lipschitz, R.; Sexton, K.W. COVID-19 Is Connected with Lower Health Literacy in Rural Areas. Stud. Health Technol. Inform. 2021, 281, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Zlotnick, C.; Dryjanska, L.; Suckerman, S. Health literacy, resilience and perceived stress of migrants in Israel during the COVID-19 pandemic. Psychol. Health 2021, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Amoah, P.A.; Leung, A.Y.M.; Parial, L.L.; Poon, A.C.Y.; Tong, H.H.-Y.; Ng, W.-I.; Li, X.; Wong, E.M.L.; Kor, P.P.K.; Molassiotis, A. Digital Health Literacy and Health-Related Well-Being Amid the COVID-19 Pandemic: The Role of Socioeconomic Status among University Students in Hong Kong and Macao. Asia Pac. J. Public Health 2021, 33, 10105395211012230. [Google Scholar] [CrossRef]
- Neter, E.; Dominguez-Rodriguez, A.; Flemming, D.; Fiordelli, M.; An, L.; Bacon, E.; Hawley, S.; Yang, P.; Russell, D.; Huffman, S.; et al. Relationship Between Coronavirus-Related eHealth Literacy and COVID-19 Knowledge, Attitudes, and Practices among US Adults: Web-Based Survey Study. J. Med. Internet Res. 2021, 23, e25042. [Google Scholar] [CrossRef]
- Bray, L.; Carter, B.; Blake, L.; Saron, H.; Kirton, J.A.; Robichaud, F.; Avila, M.; Ford, K.; Nafria, B.; Forsner, M.; et al. “People play it down and tell me it can’t kill people, but I know people are dying each day”. Children’s health literacy relating to a global pandemic (COVID-19); an international cross sectional study. PLoS ONE 2021, 16, e0246405. [Google Scholar] [CrossRef]
- Almohammed, O.A.; Aldwihi, L.A.; Alragas, A.M.; Almoteer, A.I.; Gopalakrishnan, S.; Alqahtani, N.M. Knowledge, Attitude, and Practices Associated With COVID-19 Among Healthcare Workers in Hospitals: A Cross-Sectional Study in Saudi Arabia. Front. Public Health 2021, 9, 643053. [Google Scholar] [CrossRef] [PubMed]
- Albahri, A.H.; Alnaqbi, S.A.; Alnaqbi, S.A.; Alshaali, A.O.; Shahdoor, S.M. Knowledge, Attitude, and Practice Regarding COVID-19 among Healthcare Workers in Primary Healthcare Centers in Dubai: A Cross-Sectional Survey, 2020. Front. Public Health 2021, 9, 617679. [Google Scholar] [CrossRef] [PubMed]
- Maurya, V.K.; Upadhyay, V.; Dubey, P.; Shukla, S.; Chaturvedi, A. Assessment of front-line healthcare workers’ Knowledge, Attitude and Practice after several months of COVID-19 pandemic. J. Healthc. Qual. Res. 2021. [Google Scholar] [CrossRef]
- Elgibaly, O.; Daef, E.; Elghazally, S.A.; Hassan, H.M.; ElsaidTash, R.M.; Bahgat, S.M.; ELantouny, N.G.; Zarzour, A.A.; Othman, M.M.A.; El-Sokkary, R.H. Knowledge, perception, and confidence of healthcare workers about COVID-19 preventive measures during the first wave of the pandemic: A cross-sectional study from Egypt. Germs 2021, 11, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Mahanta, P.; Deka, H.; Sarma, B.; Konwar, R.; Thakuria, K.D.; Kalita, D.; Singh, S.G.; Eshori, L. Knowledge, Attitude, Practice and Preparedness toward COVID-19 Pandemic among Healthcare Workers in Designated COVID Hospitals of a North-Eastern State of India. Hosp. Top. 2021, 1–10. [Google Scholar] [CrossRef]
- Nahidi, S.; Sotomayor-Castillo, C.; Li, C.; Currey, J.; Elliott, R.; Shaban, R.Z. Australian critical care nurses’ knowledge, preparedness, and experiences of managing SARS-COV-2 and COVID-19 pandemic. Aust. Crit. Care 2021. [Google Scholar] [CrossRef]
- Bhandari, S.; Sharma, M.; Shrestha, G.S. Knowledge of COVID-19 among Health Care Workers at a Tertiary Care Hospital of Nepal: A Descriptive Cross-sectional Study. J. Nepal Med Assoc. 2020, 58, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Anuar, A.; Ang, W.C.; Musadad, N.M.A.; Wahab, S.N.A.; Sukor, N.A.; Warijo, O. Knowledge, attitude and practice towards COVID-19 and perceived challenges of working during the Movement Control Order: A quantitative analysis among healthcare workers in a Malaysian northwestern state. Curr. Med. Res. Opin. 2021, 1–19. [Google Scholar] [CrossRef]
- Imasuen, H.; Nzomiwu, C.L. The Knowledge of COVID-19 among Health Care Workers in a Nigerian Urban Community and their Willingness to Manage COVID-19 Patients. West. Afr. J. Med. 2021, 38, 859–865. [Google Scholar] [PubMed]
- Zaitoon, H.; Sharkansky, L.; Ganaim, L.; Chistyakov, I.; Srugo, I.; Bamberger, E. Evaluation of Israeli healthcare workers knowledge and attitudes toward the COVID-19 vaccine. Public Health Nurs. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yesse, M.; Muze, M.; Kedir, S.; Argaw, B.; Dengo, M.; Nesre, T.; Hamdalla, F.; Saliha, A.; Mussa, T.; Kasim, I.; et al. Assessment of knowledge, attitude and practice toward COVID-19 and associated factors among health care workers in Silte Zone, Southern Ethiopia. PLoS ONE 2021, 16, e0257058. [Google Scholar] [CrossRef]
- Iheanacho, T.; Stefanovics, E.; Okoro, U.G.; Anyaehie, U.E.; Njoku, P.O.; Adimekwe, A.I.; Ibediro, K.; Stefanovics, G.A.; Haeny, A.; Jackson, A.; et al. Assessing knowledge, attitude, practice and training related to COVID-19: A cross-sectional survey of frontline healthcare workers in Nigeria. BMJ Open 2021, 11, e050138. [Google Scholar] [CrossRef] [PubMed]
- Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef]
- Matterne, U.; Egger, N.; Tempes, J.; Tischer, C.; Lander, J.; Dierks, M.-L.; Bitzer, E.-M.; Apfelbacher, C. Health literacy in the general population in the context of epidemic or pandemic coronavirus outbreak situations: Rapid scoping review. Patient Educ. Couns. 2021, 104, 223–234. [Google Scholar] [CrossRef]
- Schug, C.; Morawa, E.; Geiser, F.; Hiebel, N.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Steudte-Schmiedgen, S.; Borho, A.; et al. Social Support and Optimism as Protective Factors for Mental Health among 7765 Healthcare Workers in Germany during the COVID-19 Pandemic: Results of the VOICE Study. Int. J. Environ. Res. Public Health 2021, 18, 3827. [Google Scholar] [CrossRef]
- Morawa, E.; Schug, C.; Geiser, F.; Beschoner, P.; Jerg-Bretzke, L.; Albus, C.; Weidner, K.; Hiebel, N.; Borho, A.; Erim, Y. Psychosocial burden and working conditions during the COVID-19 pandemic in Germany: The VOICE survey among 3678 health care workers in hospitals. J. Psychosom. Res. 2021, 144, 110415. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- Pelikan, J.M.; Ganahl, K.; van den Broucke, S.; Sørensen, K. Measuring health literacy in Europe: Introducing the European Health Literacy Survey Questionnaire (HLS-EU-Q). In International Handbook of Health Literacy; Okan, O., Bauer, U., Levin-Zamir, D., Pinheiro, P., Sørensen, K., Eds.; Policy Press: Bristol, UK, 2019; pp. 115–138. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE: Los Angeles, CA, USA; London, UK; New Delhi, India; Singapore; Washington, DC, USA; Melbourne, Australia, 2018; ISBN 978-1-52641-952-1. [Google Scholar]
- Hair, J.F.; Babin, B.J.; Anderson, R.E.; Black, W.C. Multivariate Data Analysis, 7th Pearson New International ed.; Pearson: Harlow, UK, 2014; ISBN 978-1-292-02190-4. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39. [Google Scholar] [CrossRef]
- Ansmann, L.; Hower, K.I.; Wirtz, M.A.; Kowalski, C.; Ernstmann, N.; McKee, L.; Pfaff, H. Measuring social capital of healthcare organizations reported by employees for creating positive workplaces—Validation of the SOCAPO-E instrument. BMC Health Serv. Res. 2020, 20, 272. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Hoebel, J. Gesundheitskompetenz von Erwachsenen in Deutschland: Ergebnisse der Studie “Gesundheit in Deutschland aktuell” (GEDA). Bundesgesundheitsblatt Gesundh. Gesundh. 2015, 58, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Farmanova, E.; Bonneville, L.; Bouchard, L. Organizational Health Literacy: Review of Theories, Frameworks, Guides, and Implementation Issues. Inquiry 2018, 55, 46958018757848. [Google Scholar] [CrossRef] [Green Version]
- Zanobini, P.; Lorini, C.; Baldasseroni, A.; Dellisanti, C.; Bonaccorsi, G. A Scoping Review on How to Make Hospitals health Literate Healthcare Organizations. Int. J. Environ. Res. Public Health 2020, 17, 1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bremer, D.; Klockmann, I.; Jaß, L.; Härter, M.; von dem Knesebeck, O.; Lüdecke, D. Which criteria characterize a health literate health care organization?—A scoping review on organizational health literacy. BMC Health Serv. Res. 2021, 21, 664. [Google Scholar] [CrossRef] [PubMed]
- Brach, C.; Keller, L.M.D.; Hernandez, C.; Baur, R.; Parker, B.; Dreyer, P.; Schyve, A.J.; Lemerise, D.; Schillinger, D. Ten Attributes of Health Literate Health Care Organizations; NAM Perspectives Discussion Paper: Washington, DC, USA, 2012. [Google Scholar]


{kind=link}
| Frequency (n) | Percentage (%) | |
|---|---|---|
| Sex | ||
| Male | 266 | 27.6 |
| Female | 697 | 72.2 |
| Diverse | 2 | 0.2 |
| Age | ||
| 18−30 years | 162 | 16.8 |
| 31−40 years | 199 | 20.6 |
| 41−50 years | 191 | 19.8 |
| 51−60 years | 324 | 33.6 |
| >60 years | 89 | 9.2 |
| Occupation | ||
| Physician | 222 | 23.0 |
| Nurse | 274 | 28.4 |
| Medical-technical staff | 88 | 9.1 |
| Psychologist | 21 | 2.2 |
| Spiritual care worker | 146 | 15.1 |
| Employees in administration in direct contact with patients | 47 | 4.9 |
| Other | 167 | 17.3 |
| Previous infection with SARS-CoV2 | ||
| Yes | 14 | 1.5 |
| No | 488 | 50.6 |
| I do not know | 463 | 48.0 |
| Item | M | SD | Md | S | Min | Max | ri | Pi | |
|---|---|---|---|---|---|---|---|---|---|
| How easy/difficult is it for you… | |||||||||
| 1. | to find information about COVID-19? | 1.38 | 0.545 | 1.00 | 1.109 | 1 | 4 | 0.477 | 12.8 |
| 2. | to find out where to get professional help if you have COVID-19 yourself? | 1.62 | 0.702 | 2.00 | 0.890 | 1 | 4 | 0.538 | 20.8 |
| 3. | to find information on behaviors that are good for your mental wellbeing during the COVID-19 pandemic? | 2.07 | 0.818 | 2.00 | 0.385 | 1 | 4 | 0.464 | 35.6 |
| 4. | to understand information on how to protect yourself against COVID-19? | 1.46 | 0.623 | 1.00 | 1.232 | 1 | 4 | 0.675 | 15.3 |
| 5. | to understand information about possible treatment for COVID-19? | 1.77 | 0.775 | 2.00 | 0.778 | 1 | 4 | 0.668 | 25.6 |
| 6. | to understand Information about the risk factors associated with severe COVID-19? | 1.73 | 0.780 | 2.00 | 0.835 | 1 | 4 | 0.688 | 24.2 |
| 7. | to assess which of your everyday habits increase the risk of suffering from COVID-19 yourself? | 1.60 | 0.690 | 1.00 | 0.974 | 1 | 4 | 0.642 | 20.1 |
| 8. | to assess whether the information about COVID-19 in the media can be trusted? | 2.43 | 0.859 | 2.00 | 0.012 | 1 | 4 | 0.582 | 47.7 |
| 9. | to assess whether information about COVID-19 from scientific sources is reliable? | 2.38 | 0.821 | 2.00 | 0.033 | 1 | 4 | 0.578 | 46.1 |
| 10. | to use the information available to you to decide how to behave in the event of being infected with COVID-19 yourself? | 1.83 | 0.727 | 2.00 | 0.562 | 1 | 4 | 0.643 | 27.7 |
| 11. | to decide based on information from the media how you can protect yourself against COVID-19? | 2.05 | 0.818 | 2.00 | 0.500 | 1 | 4 | 0.573 | 35.0 |
| 12. | to decide based on information from your employer how you can protect yourself against COVID-19? | 2.01 | 0.874 | 2.00 | 0.585 | 1 | 4 | 0.490 | 33.7 |
| Item | Factor Loading | |
|---|---|---|
| 1. | Find information about COVID-19 | 0.563 |
| 2. | Find out where to receive professional help when falling ill with COVID-19 | 0.620 |
| 3. | Find information on behaviors which are good for the psychological well-being during the COVID-19 pandemic | 0.543 |
| 4. | Understand information about how to protect myself from COVID-19 | 0.758 |
| 5. | Understand information about a potential treatment of COVD-19 | 0.757 |
| 6. | Understand information about risk factors for a severe course of COVID-19 | 0.774 |
| 7. | Assess which daily routines increase the risk to fall ill with COVID-19 | 0.730 |
| 8. | Assess whether information about COVID-19 is reliable on the media | 0.649 |
| 9. | Assess whether information about COVID-19 is reliable from scientific sources | 0.644 |
| 10. | Decide based on present information how to behave when falling ill with COVID-19 | 0.718 |
| 11. | Decide based on information from media how to protect myself from COVID-19 | 0.644 |
| 12. | Decide based on information from employer how to protect myself from COVID-19 | 0.567 |
| % of explained variance | 44.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiltrop, K.; Hiebel, N.; Geiser, F.; Kriegsmann-Rabe, M.; Gambashidze, N.; Morawa, E.; Erim, Y.; Weidner, K.; Albus, C.; Ernstmann, N. Measuring COVID-19 Related Health Literacy in Healthcare Professionals—Psychometric Evaluation of the HL-COV-HP Instrument. Int. J. Environ. Res. Public Health 2021, 18, 11959. https://doi.org/10.3390/ijerph182211959
Hiltrop K, Hiebel N, Geiser F, Kriegsmann-Rabe M, Gambashidze N, Morawa E, Erim Y, Weidner K, Albus C, Ernstmann N. Measuring COVID-19 Related Health Literacy in Healthcare Professionals—Psychometric Evaluation of the HL-COV-HP Instrument. International Journal of Environmental Research and Public Health. 2021; 18(22):11959. https://doi.org/10.3390/ijerph182211959
Chicago/Turabian StyleHiltrop, Kati, Nina Hiebel, Franziska Geiser, Milena Kriegsmann-Rabe, Nikoloz Gambashidze, Eva Morawa, Yesim Erim, Kerstin Weidner, Christian Albus, and Nicole Ernstmann. 2021. "Measuring COVID-19 Related Health Literacy in Healthcare Professionals—Psychometric Evaluation of the HL-COV-HP Instrument" International Journal of Environmental Research and Public Health 18, no. 22: 11959. https://doi.org/10.3390/ijerph182211959