
Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
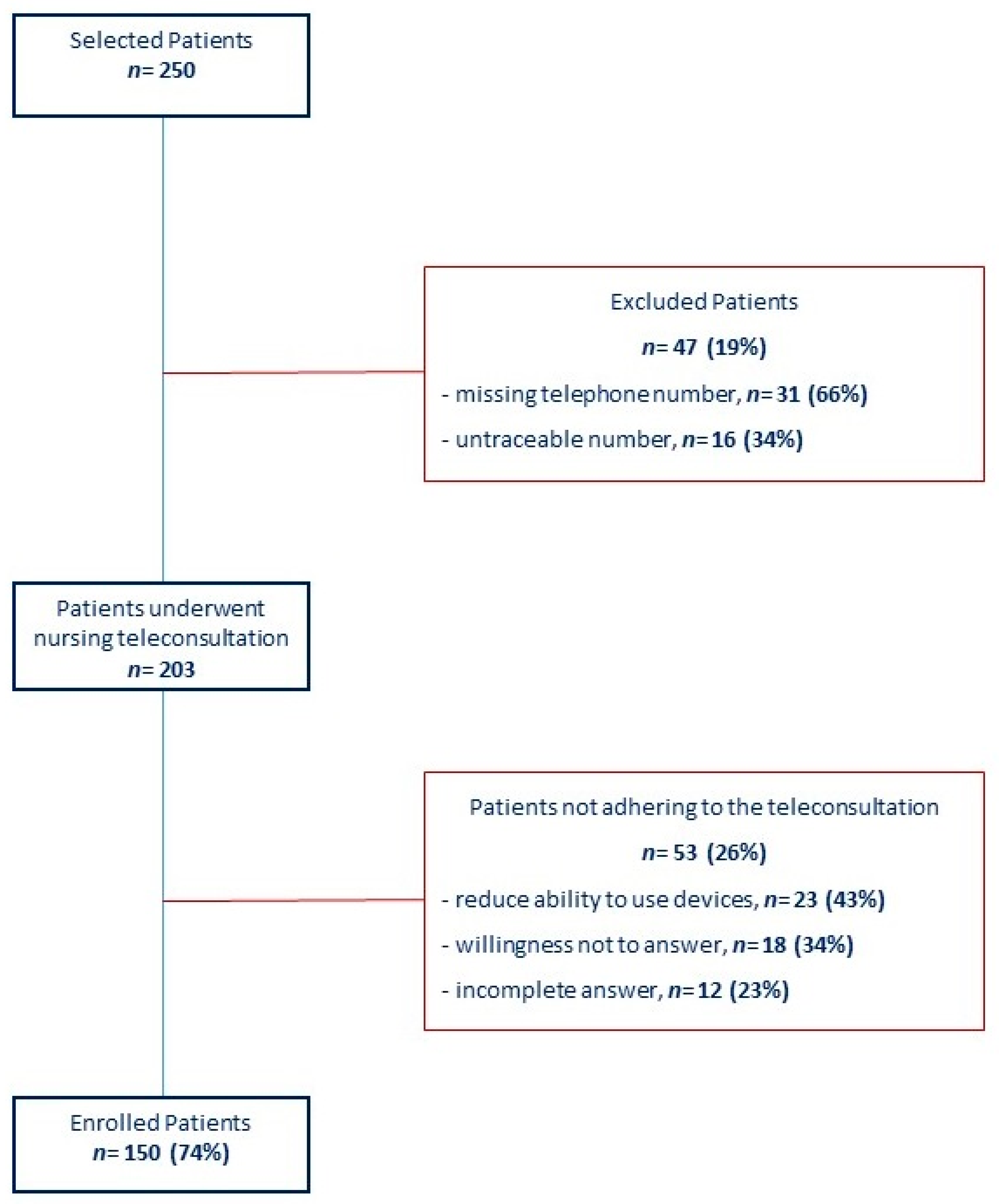
2.1. Study Design and Population
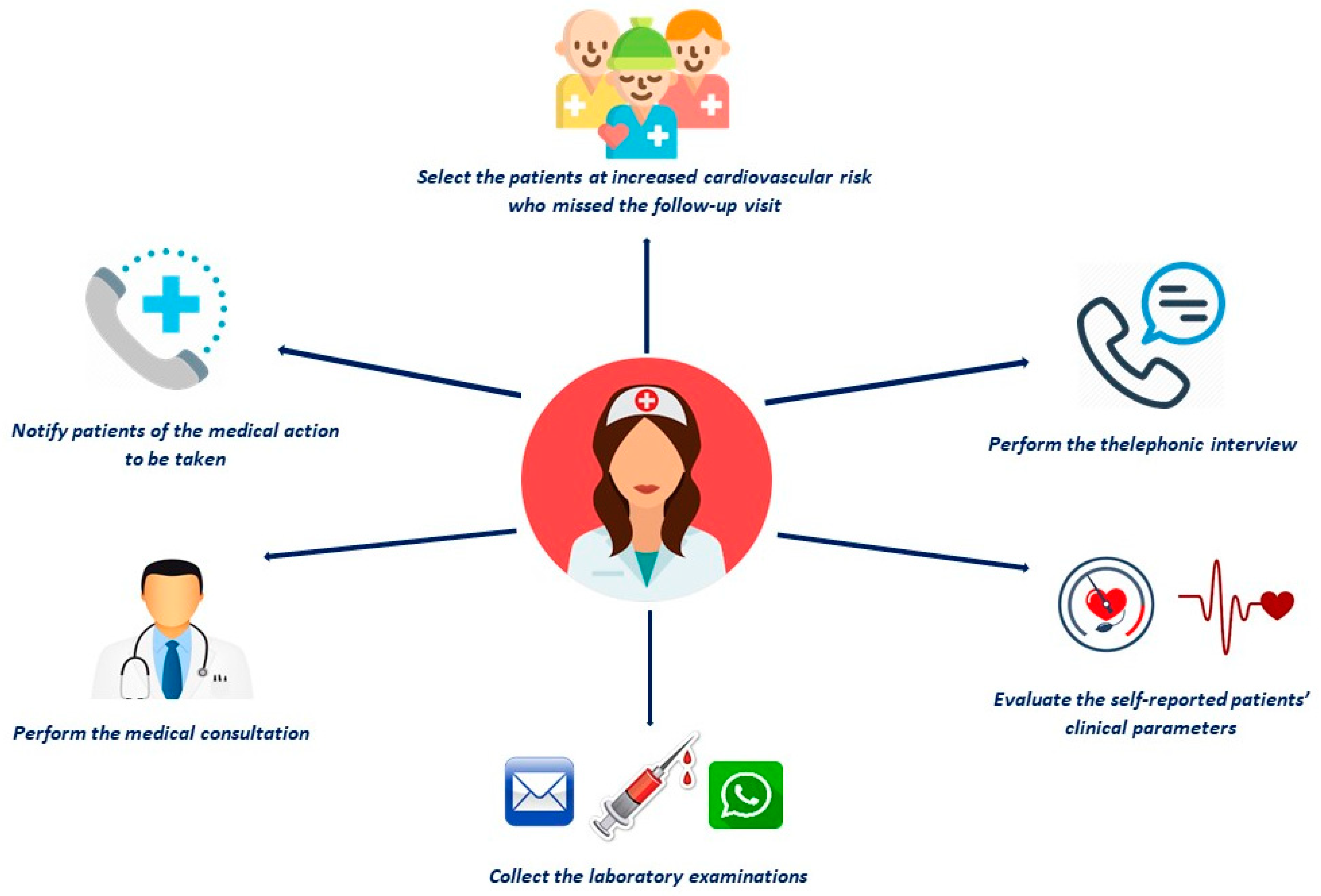
2.2. Nursing Teleconsultation
2.3. Outcomes
2.4. Statistical Analysis
2.5. Ethics Approval
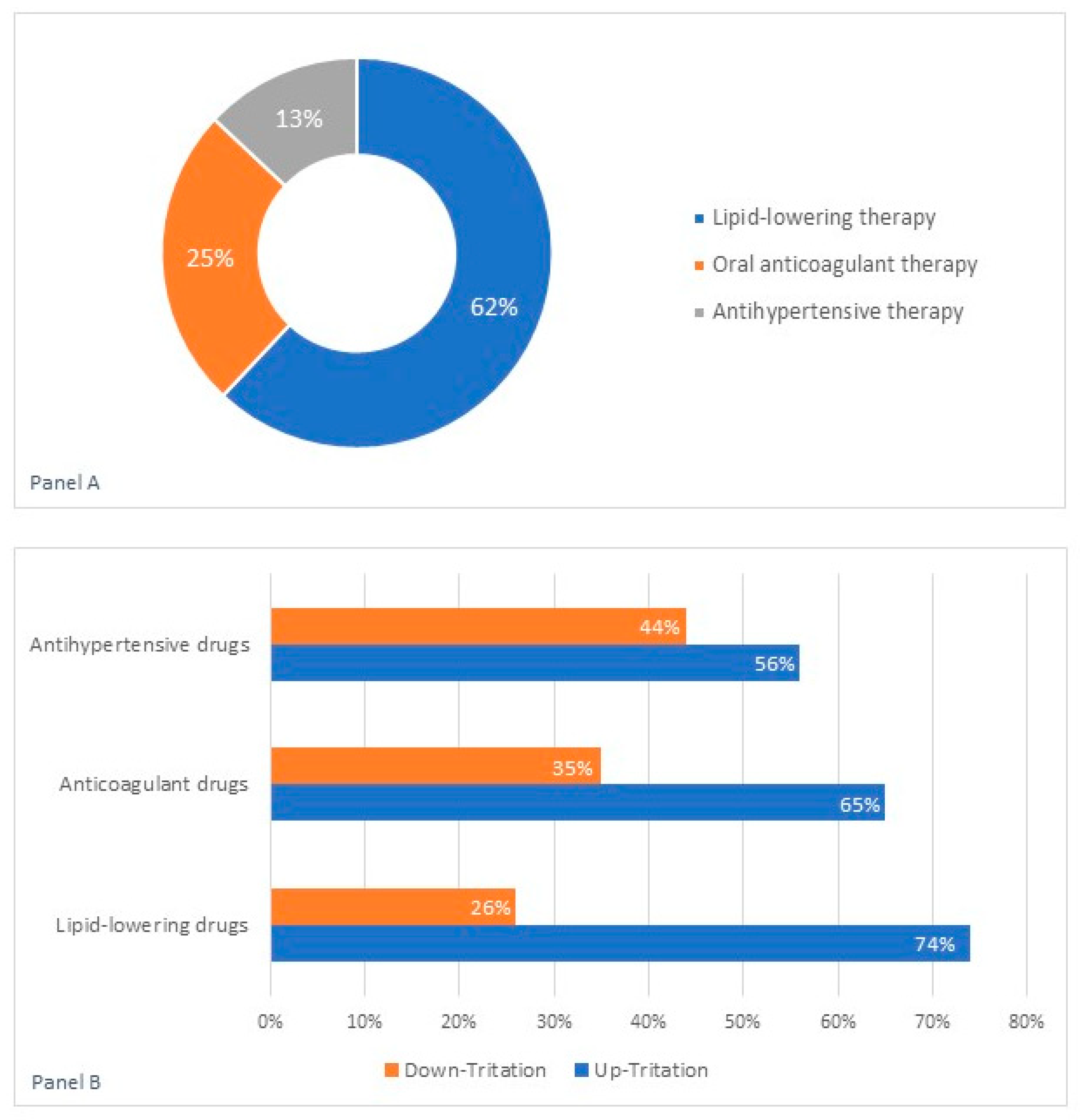
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef]
- Russo, V.; Bottino, R.; Carbone, A.; Rago, A.; Papa, A.A.; Golino, P.; Nigro, G. COVID-19 and Heart: From Clinical Features to Pharmacological Implications. J. Clin. Med. 2020, 9, 1944. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Piccinocchi, G.; Mandaliti, V.; Annunziata, S.; Cimmino, G.; Attena, E.; Moio, N.; Di Micco, P.; Severino, S.; Trotta, R.; et al. Cardiovascular Comorbidities and Pharmacological Treatments of COVID-19 Patients Not Requiring Hospitalization. Int. J. Environ. Res. Public Health 2020, 18, 102. [Google Scholar] [CrossRef]
- Civil Protection: Presidency of the Council of Ministers Department of Civil Protection. Available online: https://opendatadpc.maps.arcgis.com/apps/opsdashboard/index.html#/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 1 January 2021).
- Italy: Government of Italy Decree of the President of the Council of Ministers. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/09/20A01558/sg (accessed on 3 September 2020). (In Italian).
- Russo, V.; Pafundi, P.C.; Rapacciuolo, A.; D’Andrea, A.; De Devitiis, M.; Volpicelli, M.; Ruocco, A.; Nigro, G.; D’Onofrio, A. Arrhythmogenic syncope leading to cardiac rhythm management procedures during COVID-19 lockdown. Expert Rev. Med. Devices 2020, 17, 1207–1210. [Google Scholar] [CrossRef]
- Russo, V.; Pafundi, P.C.; Rapacciuolo, A.; de Divitiis, M.; Volpicelli, M.; Ruocco, A.; Rago, A.; Uran, C.; Nappi, F.; Attena, E.; et al. Cardiac pacing procedures during COVID-19 lockdown in Southern Italy: Insights from Campania Region. J. Cardiovasc. Med. 2021. Accepted in Press. [Google Scholar]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabro, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Barrios, V.; Cosín-Sales, J.; Bravo, M.; Escobar, C.; Gámez, J.M.; Huelmos, A.; Cortés, C.O.; Egocheaga, I.; García-Pinilla, J.M.; Jiménez-Candil, J.; et al. Telemedicine consultation for the clinical cardiologists in the era of COVID-19: Present and future. Consensus document of the Spanish Society of Cardiology. Rev. Española Cardiol. 2020, 73, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Report on the Health Status of the Country. 2011. Available online: http://www.rssp.salute.gov.it/rssp2011/documenti/RSSP_2011_Inglese_web.pdf (accessed on 1 January 2021).
- Centers for Disease Control and Prevention. Uses of Telehealth during COVID-19 in Low Resource Non-U.S. Settings. Available online: https://www.cdc.gov/coronavirus/2019-ncov/global-covid-19/telehealth-covid19-nonUS.html (accessed on 21 July 2020).
- Deldar, K.; Bahaadinbeigy, K.; Tara, S.M. Teleconsultation and Clinical Decision Making: A Systematic Review. Acta Inform. Med. 2016, 24, 286–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, V.; Nigro, G.; D’Onofrio, A. COVID-19 and cardiac implantable electronic device remote monitoring: Crocodile tears or new opportunity? Expert Rev. Med. Devices 2020, 17, 471–472. [Google Scholar] [CrossRef] [PubMed]
- Maines, M.; Zorzi, A.; Benetollo, P.P.; Guarrera, G.M.; Moz, M.; Manica, A.; Demattè, C.; Del Greco, M. Short-term outcome associated with remote evaluation (telecardiology) of patients with cardiovascular diseases during the COVID-19 pandemic. Int. J. Cardiol. Heart Vasc. 2020, 30, 100625. [Google Scholar] [CrossRef]
- Bruckert, E.; Parhofer, K.G.; Gonzalez-Juanatey, J.R.; Nordestgaard, B.; Arca, M.; Giovas, P.; Ray, K. Proportion of High-Risk/Very High-Risk Patients in Europe with Low-Density Lipoprotein Cholesterol at Target According to European Guidelines: A Systematic Review. Adv. Ther. 2020, 37, 1724–1736. [Google Scholar] [CrossRef] [Green Version]
- Vanuzzo, D. The epidemiological concept of residual risk. Intern. Emerg. Med. 2011, 6 (Suppl. 1), 45–51. [Google Scholar] [CrossRef]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef]
- Dillinger, J.-G.; Aleil, B.; Cheggour, S.; Benhamou, Y.; Béjot, Y.; Marechaux, S.; Delluc, A.; Bertoletti, L.; Lellouche, N. Dosing issues with non-vitamin K antagonist oral anticoagulants for the treatment of non-valvular atrial fibrillation: Why we should not underdose our patients. Arch. Cardiovasc. Dis. 2018, 111, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Rago, A.; Proietti, R.; Di Meo, F.; Papa, A.A.; Calabrò, P.; D’Onofrio, A.; Nigro, G.; Alturki, A. Efficacy and safety of the target-specific oral anticoagulants for stroke prevention in atrial fibrillation: The real-life evidence. Ther. Adv. Drug Saf. 2017, 8, 67–75. [Google Scholar] [CrossRef]
- Russo, V.; Attena, E.; Di Maio, M.; Carbone, A.; Parisi, V.; Rago, A.; Grieco, F.V.; Buonauro, A.; Golino, P.; Nigro, G. Non--vitamin K vs vitamin K oral anticoagulants in patients aged > 80 year with atrial fibrillation and low body weight. Eur. J. Clin. Investig. 2020, 50. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Attena, E.; Di Maio, M.; Mazzone, C.; Carbone, A.; Parisi, V.; Rago, A.; D’Onofrio, A.; Golino, P.; Nigro, G. Clinical profile of direct oral anticoagulants versus vitamin K anticoagulants in octogenarians with atrial fibrillation: A multicentre propensity score matched real-world cohort study. J. Thromb. Thrombolysis 2020, 49, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Bottino, R.; Rago, A.; Di Micco, P.; Onofrio, A.D.; Liccardo, B.; Golino, P.; Nigro, G.; Russo, V. Atrial Fibrillation and Malignancy: The Clinical Performance of Non–Vitamin K Oral Anticoagulants—A Systematic Review. Semin. Thromb. Hemost. 2019, 45, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Attena, E.; Mazzone, C.; Esposito, F.; Parisi, V.; Bancone, C.; Rago, A.; Nigro, G.; Sangiuolo, R.; Onofrio, A.D.; Russo, V. Nonvitamin K Antagonist Oral Anticoagulants Use in Patients with Atrial Fibrillation and Bioprosthetic Heart Valves/Prior Surgical Valve Repair: A Multicenter Clinical Practice Experience. Semin. Thromb. Hemost. 2018, 44, 364–369. [Google Scholar] [CrossRef]
- Russo, V.; Attena, E.; Rago, A.; Melillo, E.; Di Micco, P.; Papa, A.A.; Napolitano, G.; D’Onofrio, A.; Golino, P.; Nigro, G. Clinical Outcome of Edoxaban vs. Vitamin K Antagonists in Patients with Atrial Fibrillation and Diabetes Mellitus: Results from a Multicenter, Propensity-Matched, Real-World Cohort Study. J. Clin. Med. 2020, 9, 1621. [Google Scholar] [CrossRef]
- Russo, V.; Carbone, A.; Attena, E.; Rago, A.; Mazzone, C.; Proietti, R.; Parisi, V.; Scotti, A.; Nigro, G.; Golino, P.; et al. Clinical Benefit of Direct Oral Anticoagulants Versus Vitamin K Antagonists in Patients with Atrial Fibrillation and Bioprosthetic Heart Valves. Clin. Ther. 2019, 41, 2549–2557. [Google Scholar] [CrossRef]
- Russo, V.; Attena, E.; Mazzone, C.; Melillo, E.; Rago, A.; Galasso, G.; Riegler, L.; Parisi, V.; Rotunno, R.; Nigro, G.; et al. Real-life Performance of Edoxaban in Elderly Patients With Atrial Fibrillation: A Multicenter Propensity Score-Matched Cohort Study. Clin. Ther. 2019, 41, 1598–1604. [Google Scholar] [CrossRef] [PubMed]
- Alturki, A.; Maj, J.B.; Marafi, M.; Donato, F.; Vescovo, G.; Russo, V.; Proietti, R. The Role of Cardiovascular and Metabolic Comorbidities in the Link between Atrial Fibrillation and Cognitive Impairment: An Appraisal of Current Scientific Evidence. Medicina 2019, 55, 767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proietti, R.; Alturki, A.; Vio, R.; Licchelli, L.; Rivezzi, F.; Marafi, M.; Russo, V.; Potpara, T.S.; Kalman, J.M.; De Villers-Sidani, E.; et al. The association between atrial fibrillation and Alzheimer’s disease: Fact or fallacy? A systematic review and meta-analysis. J. Cardiovasc. Med. 2020, 21, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Weir, M.R.; Kreutz, R. Influence of Renal Function on the Pharmacokinetics, Pharmacodynamics, Efficacy, and Safety of Non–Vitamin K Antagonist Oral Anticoagulants. Mayo Clin. Proc. 2018, 93, 1503–1519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [Green Version]
- Stock, J. Targeting LDL cholesterol: Early treatment is key to population health. Atherosclerosis 2020, 300, 37–38. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall Population n: 150 | Intervention Group n: 69 | Target Group n: 81 | p Value |
|---|---|---|---|---|
| Age (mean ± SD) | 67 ± 10 | 66 ± 3 | 67 ± 10.4 | 0.89 |
| Male. n (%) | 102 (68) | 47 (68) | 55 (68) | 0.99 |
| Female. n (%) | 48 (32) | 63 (91) | 65 (80) | 0.06 |
| Smokers. n (%) | 23 (15) | 12 (17) | 11 (14) | 0.5 |
| Hypertension. n (%) | 128 (85) | 15 (22) | 10 (12) | 0.13 |
| Obesity. n (%) | 25 (17) | 67 (97) | 52 (64) | 0.0001 |
| Dyslipidemia. n (%) | 119 (79) | 18 (26) | 17 (21) | 0.5 |
| Diabetes mellitus. n (%) | 33 (22) | 52 (75) | 39 (48) | 0.0008 |
| CAD. n (%) | 91(61) | 17(25) | 16 (20) | 0.5 |
| Very high CV risk. n (%) | 92 (61) | 53(77) | 39 (48) | 0.0003 |
| COPD. n (%) | 35 (23) | 14 (20) | 20 (25) | 0.51 |
| AF. n (%) | 34 (23) | 3.18 (1.41) | 3.04 (1.52) | 0.77 |
| CHA2DS2VASc (mean ± SD) | 3.10 (1.5) | 2.3 (0.1) | 2 (0.96) | 0.28 |
| HASBLED (mean ± SD) | 2.05 (1.18) | 19 (27) | 18 (22) | 0.51 |
| Valvular Heart Diseases. n (%) | 37 (25) | 58 (84) | 65 (80) | 0.57 |
| Lipid-lowering therapy. n (%) | 123(82) | 32 (46) | 19 (23) | 0.10 |
| Anticoagulant therapy. n (%) | 51 (34) | 38 (55) | 41 (51) | 0.72 |
| Antihypertensive therapy. n (%) | 79 (52) | 38 (55) | 41 (51) | 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, V.; Cassini, R.; Caso, V.; Donno, C.; Laezza, A.; Naddei, M.; Fiorelli, A.; Golino, P.; Nigro, G. Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2087. https://doi.org/10.3390/ijerph18042087
Russo V, Cassini R, Caso V, Donno C, Laezza A, Naddei M, Fiorelli A, Golino P, Nigro G. Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(4):2087. https://doi.org/10.3390/ijerph18042087
Chicago/Turabian StyleRusso, Vincenzo, Roberta Cassini, Valentina Caso, Chiara Donno, Annunziata Laezza, Maria Naddei, Alfonso Fiorelli, Paolo Golino, and Gerardo Nigro. 2021. "Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 4: 2087. https://doi.org/10.3390/ijerph18042087