
Resilience of Medication Adherence Practices in Response to Life Changes: Learning from Qualitative Data Obtained during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Data Analysis
2.3. Ethical Considerations
3. Results
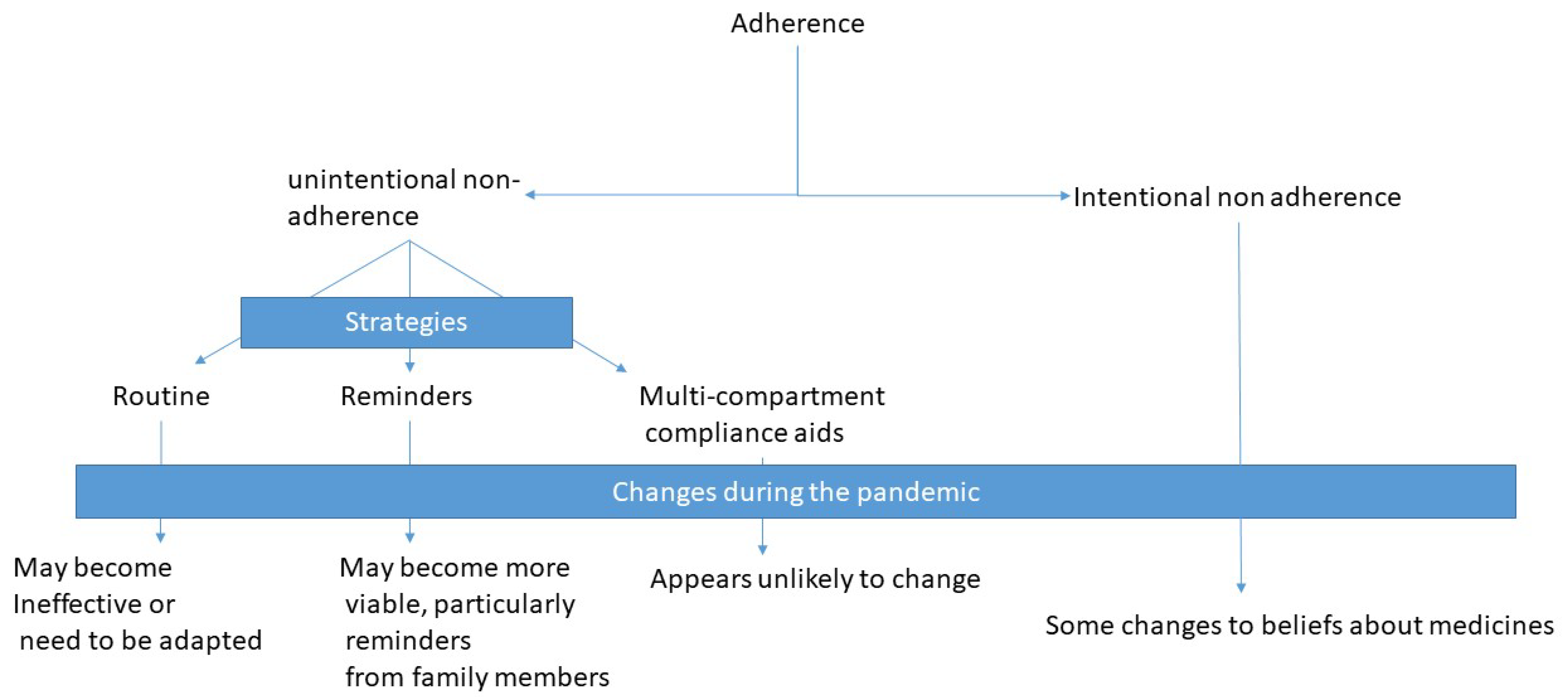
3.1. Resilience of Strategies Used to Reduce Unintentional Nonadherence
3.1.1. Routine
“Before I did have a sort of routine because I had to take it twice a day. So, I’d like try and wake up in the morning and then I was told to take it like 12 h after so then I’d try to take it just before I went to bed but because of the pandemic I’ve been waking up and going to bed later so I keep forgetting if I’ve taken them, or if I’ve taken them too closely, or have taken them too far apart.”(Participant 33).
“Doesn’t affect me at all. I just take my metformin three times a day with my meal.”(Participant 7).
“I take my tablets after I brush my teeth essentially first thing on a morning So if I haven’t brushed my teeth, I am pretty sure that I haven’t taken my tablets either, sometimes can’t remember whether I have taken my tablets when I have brushed my teeth but that’s another story.”(Participant 25).
“I know what I’m taking at a certain time of day because they’re close to where I make a cup of tea.”(Participant 11).
“I had to take a statin at night, before I go to sleep, and so actually instead of leaving that box of pills with all the others, I actually put it up in my bedroom and so it was there and I didn’t forget it.”(Participant 35).
“I guess I store my medications differently now. So, instead of having them all in one space because I would usually try and get up and take the medication and go to bed and take the medication, but because I keep forgetting, I changed the location. So, I’ve got a couple by my bed for when I wake up and then the living room for when I want to go to bed so to try and remember before I go up to bed. I think it kind of helps me remember if I’ve taken it or not. Because they don’t have the days or anything, I get mixed up if I’ve taken them or not and I think because they’re in different locations, I can tell if I’ve taken them-ish.”(Participant 33).
3.1.2. Reminders
“I actually tried to make sure by putting alarm on my phone now.”(Participant 22).
“I probably could set reminders on my phone given that it’s already inundated with the emails and WhatsApps and those sorts of things about Coronavirus, I can’t really have another thing on there as well. There wasn’t the mental space for that.”(Participant 3).
3.1.3. Multicompartment Compliance Aids and Calendar Packs
“I use a dosette box and otherwise I’m okay with taking my medication.”(Participant 50).
“Like the dosette box, we started to try (to put the tablets) in the compartments, it kind of didn’t work.”(Participant 36).
3.1.4. No Specific Strategy
“No, because I just take them as I normally take them, pandemic or not.”(Participant 45).
“You could say, in fact, that if I didn’t have to go out ever again, I would probably never forget to take my medicine.”(Participant 5).
3.2. Changes to Intentional Nonadherence during the Pandemic
“Well, the thought of getting COVID, well, it really concentrated my mind and I made sure I didn’t miss any nebulisers, took my tablets by the clock and I sort, well, if I’m going to get this wretched disease, I want my chest to be in as good a condition as it can be and maybe the medication that I’m taking might actually help.”(Participant 43).
“You start these medications with a good idea of what the risks are and suddenly that’s taken [away] and you’re not sure how to weigh that up anymore. If I’m not supposed to go out ever again until COVID is definitely gone … that means that the risk/benefit balance has completely then fallen apart and then it becomes, is it worth taking them anymore, [if] that’s the level of restriction they can have on my quality of life. So it’s quite a profound, I suppose, effect if you think about it.”(Participant 3).
4. Discussion
4.1. Implications for Practice
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, F.; Mamtani, R.; Scott, F.I.; Goldberg, D.S.; Haynes, K.; Lewis, J.D. Increasing use of prescription drugs in the United Kingdom. Pharm. Drug Saf. 2016, 25, 628–636. [Google Scholar] [CrossRef] [Green Version]
- National Institution on Clinical Excellence. Medicines Adherence: Involving Patients in Decisions about Prescribed Medicines and Supporting Adherence. Available online: https://www.nice.org.uk/guidance/cg76/chapter/Introduction (accessed on 18 December 2020).
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Available online: https://www.who.int/chp/knowledge/publications/adherence_report/en/ (accessed on 18 December 2020).
- Mickelson, R.S.; Holden, R.J. Medication adherence: Staying within the boundaries of safety. Ergonomics 2018, 61, 82–103. [Google Scholar] [CrossRef]
- Horne, R.; Chapman, S.C.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: A meta-analytic review of the Necessity-Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Matthes, J.; Albus, C. Improving adherence with medication: A selective literature review based on the example of hypertension treatment. Dtsch. Arztebl. Int. 2014, 111, 41–47. [Google Scholar] [PubMed] [Green Version]
- Furniss, D.; Barber, N.; Lyons, I.; Eliasson, L.; Blandford, A. Unintentional non-adherence: Can a spoon full of resilience help the medicine go down? BMJ Qual. Saf. 2014, 23, 95–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frech, S.; Guthoff, R.F.; Gamael, A.; Helbig, C.; Diener, A.; Ritzke, M.; Wollny, A.; Altiner, A. Patterns and Facilitators for the Promotion of Glaucoma Medication Adherence—A Qualitative Study. Healthcare 2021, 9, 426. [Google Scholar] [CrossRef] [PubMed]
- Garfield, S.; Wheeler, C.; Boucher, C.; Etkind, M.; Lloyd, J.; Norton, J.; Ogunleye, D.; Taylor, A.; Williams, M.; Grimes, T.; et al. Franklin, Medicines management at home during the COVID-19 pandemic: A qualitative study exploring the UK patient/carer perspective. Int. J. Pharm. Pract. 2021. [Google Scholar] [CrossRef] [PubMed]
- Department of Health & Social Care and Public Health England. Guidance on Shielding and Protecting People Who Are Clinically Extremely Vulnerable from COVID-19. Available online: https://www.gov.uk/government/publications/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19/ (accessed on 20 December 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Musiimenta, A.; Atukunda, E.C.; Tumuhimbise, W.; Haberer, J.E. Resilience after withdrawing a technology-based medication adherence support intervention from people living with HIV in rural Uganda. AIDS Care 2018, 30, S89. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Distribution |
|---|---|
| Gender | 16 males 34 females |
| Age | Mean age: 68 (range 26–93) |
| Ethnic group | 43 white 7 other ethnicities |
| Urban versus rural location | 43 urban 1 semi-rural 6 rural |
| Number of medicines | Range 1–17 |
| Living arrangements | 40 living with others 10 living alone |
| Dominant role in assisting other family member with medicines | 9 yes 41 no |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, M.; Wheeler, C.; Franklin, B.D.; Begum, R.; Garfield, S. Resilience of Medication Adherence Practices in Response to Life Changes: Learning from Qualitative Data Obtained during the COVID-19 Pandemic. Healthcare 2021, 9, 1048. https://doi.org/10.3390/healthcare9081048
Ahmed M, Wheeler C, Franklin BD, Begum R, Garfield S. Resilience of Medication Adherence Practices in Response to Life Changes: Learning from Qualitative Data Obtained during the COVID-19 Pandemic. Healthcare. 2021; 9(8):1048. https://doi.org/10.3390/healthcare9081048
Chicago/Turabian StyleAhmed, Mushfique, Carly Wheeler, Bryony Dean Franklin, Rabia Begum, and Sara Garfield. 2021. "Resilience of Medication Adherence Practices in Response to Life Changes: Learning from Qualitative Data Obtained during the COVID-19 Pandemic" Healthcare 9, no. 8: 1048. https://doi.org/10.3390/healthcare9081048