
A One-Year Longitudinal Study: Changes in Depression and Anxiety in Frontline Emergency Department Healthcare Workers in the COVID-19 Pandemic

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
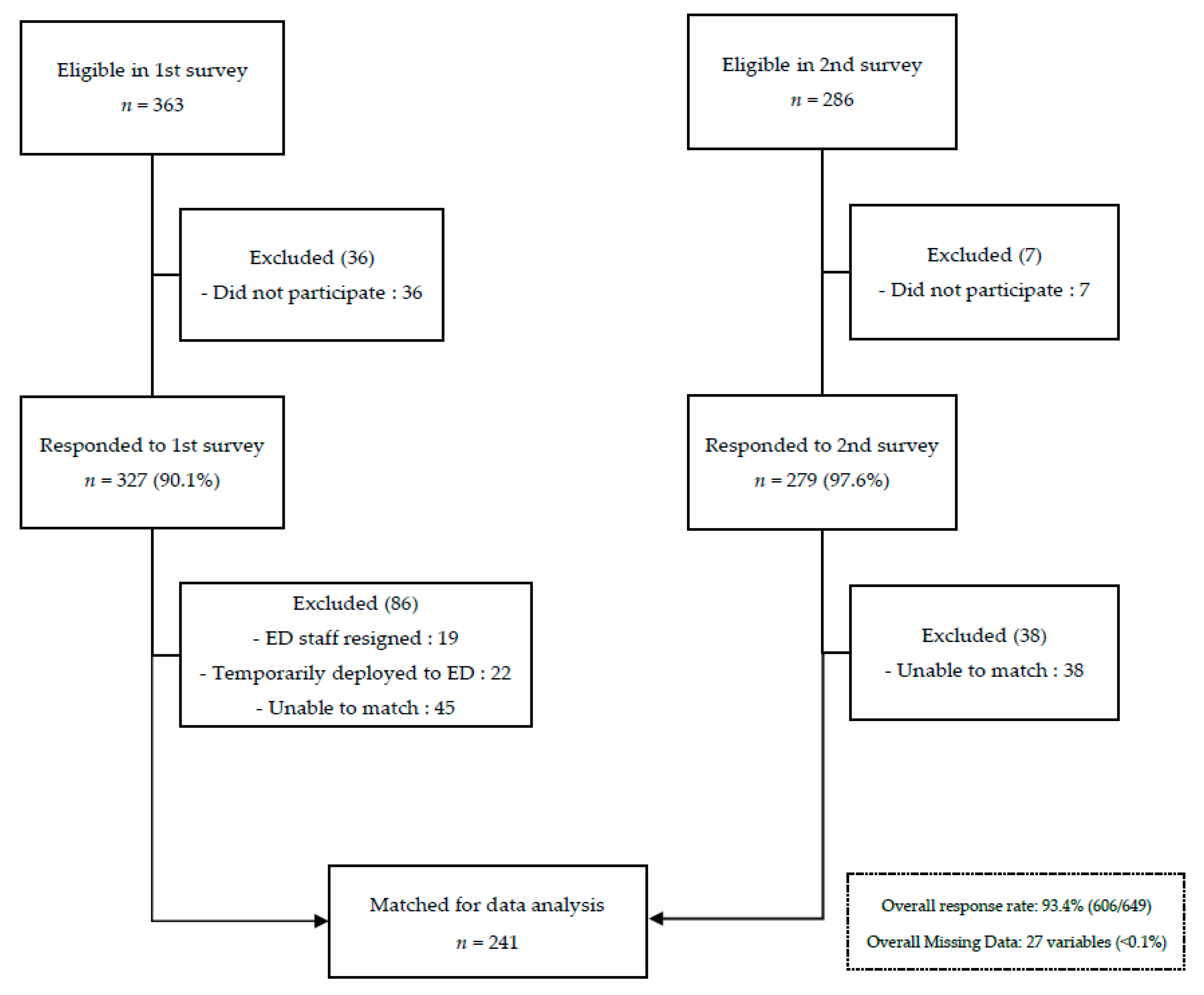
2.1. Study Design and Participants
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Sample
3.2. Mental Health Outcomes
3.2.1. Depression
3.2.2. Anxiety
4. Discussion
4.1. Overall Reduced Anxiety in HCWs
4.2. Increased Depression in Doctors
4.3. Increased Depression and Demographic Characteristics
4.4. Increased Depression and Concerns about Workload
4.5. COVID-19 Vaccination
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 June 20 | 408 cases. Final day of 8-week circuit breaker (national lock-down). |
| 2 June 20 | 544 cases. Phase 1: Compulsory to wear face masks in public areas, Pre-schools/schools/institutions to re-open in phases, People encouraged to work from home, Only allowed to visit parents/grandparents from a different household. |
| 9 June 20 | 218 cases. |
| 19 June 20 | 142 cases. Phase 2: Maximum groups of 5 with safe distancing of 1 metre in public areas, Reopening of park, sports facilities and cafes/restaurants. |
| 28 December 20 | 5 cases (0 local cases). Phase 3: Maximum groups of 8 allowed in public areas. |
| 11 January 21 | 22 cases (0 local cases). COVID-19 vaccine (Pfizer) offered to all HCWs in KTPH. |
| 10 March 21 | 10 cases (0 local cases). COVID-19 vaccination offered to residents 60 years old and above nationally. |
| 25 March 21 | 17 cases (0 local cases). COVID-19 vaccination offered to residents 45–59 years old nationally. |
| 29 April 21 | 35 cases (16 local cases—highest number over past 9 months). First COVID-19 cluster involving a hospital. N95s to be used even in clean areas in our hospital instead of surgical masks. |
| 4 May 21 | 17 cases (5 local cases). Affected hospital cluster was shut—all cases diverted to other hospitals including KTPH. |
| 5 May 21 | 16 cases (1 local case). All healthcare workers to be swabbed every 1–2 weeks. |
| 8 May 21 | 20 cases (7 local cases). Reduction of public groups from 8 to 5 people, Cessation of all indoors physical activities. |
| 14 May 21 | 52 cases (24 local cases). Emergence of multiple new clusters including a children tuition centre and another hospital. |
| 16 May 21 | 49 new cases (38 local cases). Social gatherings limited from 5 to 2 people, Defaulted to work from home, No dine-ins in public areas. |
| 19 May 21 | 38 cases (34 local cases). All institutions shut as COVID-19 affecting a high proportion of children. COVID-19 vaccination offered to residents 40–44 years old nationally. |
| 1st June 21 | 18 cases (15 local cases). Students ≥ 12 years old offered COVID-19 vaccination nationally. |
| 11 June 21 | 9 cases (3 local cases). Vaccination offered to residents 12–39 years old nationally. |
| 14 June 21 | 25 cases (19 local cases). Gatherings up to 5 people again, no dine-ins till 21 June 2021. |
| 16 June 21 | 24 cases (19 local cases). |
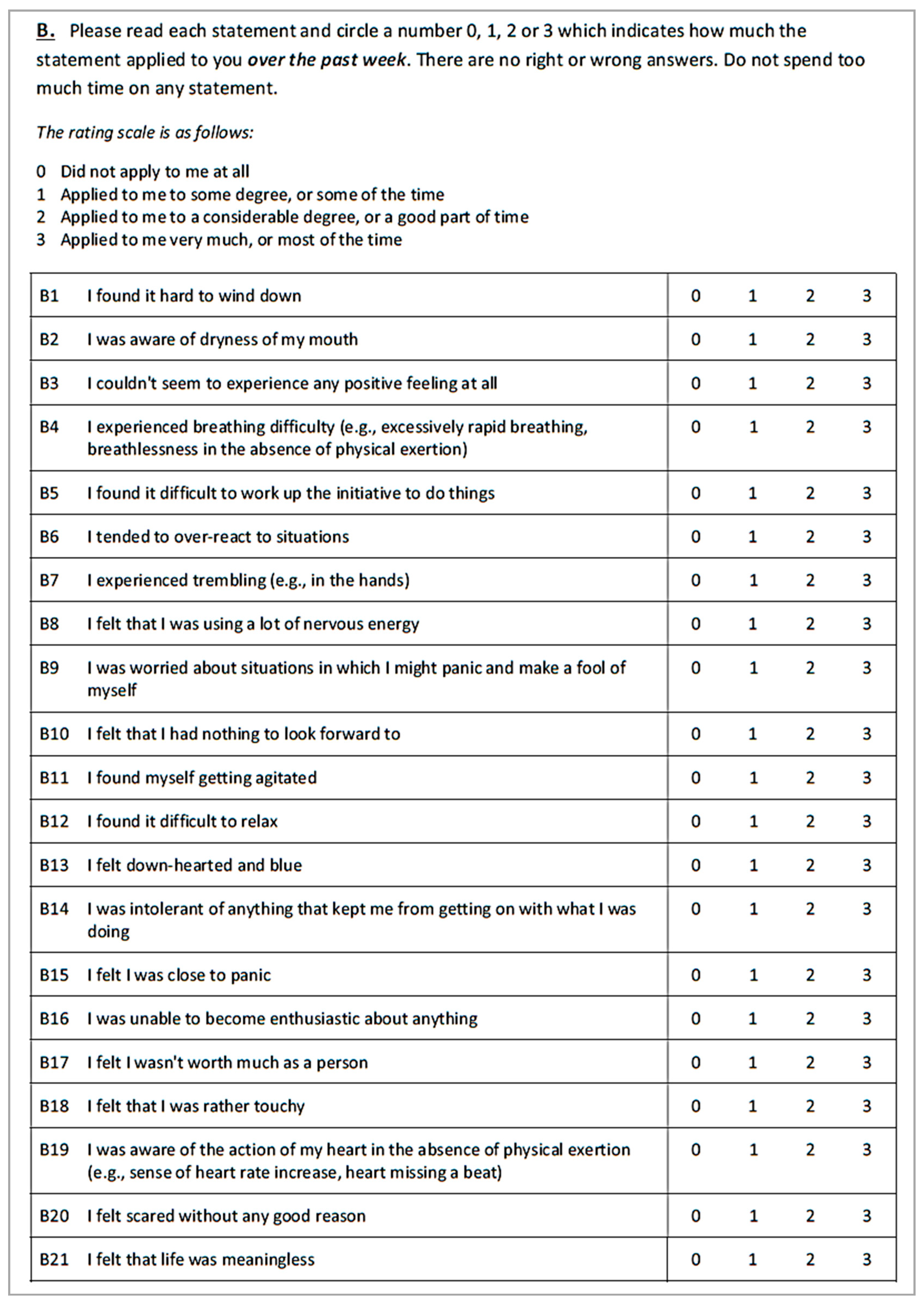
Appendix B





Appendix C

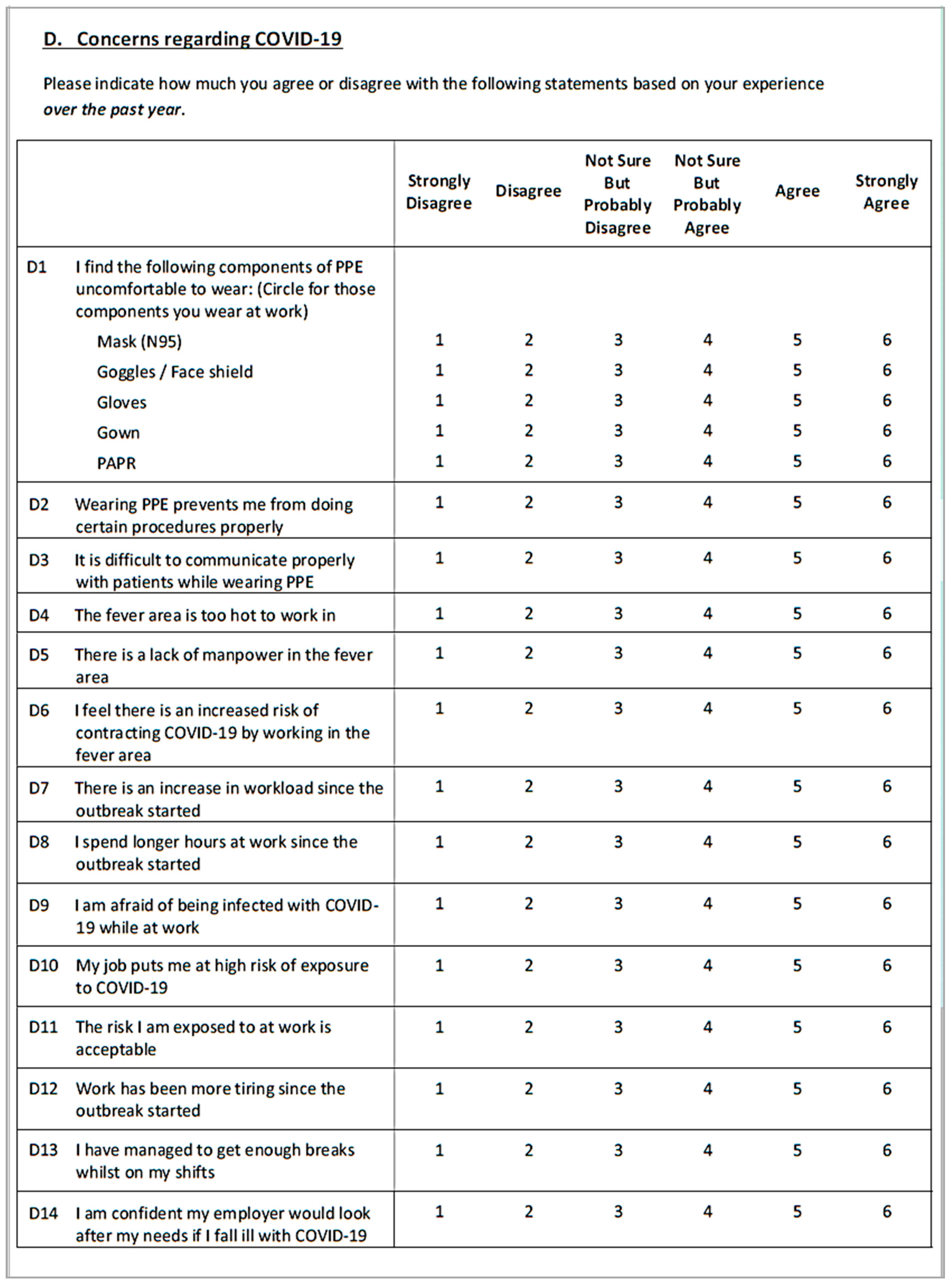
Appendix D
| Questions | Depression | Anxiety |
|---|---|---|
| p-Value | p-Value | |
| Workload (Higher odds of Depression) | ||
| D5: There is a lack of manpower in the fever area | 0.002 | |
| D7: There is an increase in workload since the outbreak started | 0.093 | |
| D8: I spend longer hours at work since the outbreak started | 0.010 | |
| D12: Work has been more tiring since the outbreak started | 0.167 | |
| Infection risk (Higher odds of Anxiety) | ||
| D6: I feel there is an increased risk of contracting COVID-19 by working in the fever area | 0.545 | |
| D9: I am afraid of being infected with COVID-19 while at work | 0.879 | |
| D10: My job puts me at high risk of exposure to COVID-19 | 0.389 | |
| D11: The risk I am exposed to at work is acceptable | 0.337 | |
| D18: People close to me are worried about getting infected by me | 0.657 | |
| D19: I am worried about infecting my loved once because of my job | 1.00 | |
| Workplace support (Lower odds of Depression) | ||
| D13: I have managed to get enough breaks whilst on my shifts | 0.074 | |
| D14: I am confident my employer would look after my needs if I fall ill withCOVID-19 | <0.001 | |
| D15: I am satisfied with the hospital response to the outbreak | 0.002 | |
| D16: I receive clear communication of outbreak directives from my superiors | 0.031 | |
| E1c: I get adequate support from my supervisors | <0.001 | |
| E1d: I get adequate support from my colleagues | 0.046 | |
| Social connectedness (Lower odds of Depression) | ||
| D21:I am frustrated about not being able to visit my family living abroad | 0.806 | |
| E1a: I get adequate support from my Family | 0.006 | |
| E1b: I get adequate support from my Friends | 0.022 | |
| E3: Being able to see my colleagues at work helps to decrease feelings of social isolation | 0.000 |
Appendix E
| Excluded in 2020 (n = 86) | Included in 2020 (n = 241) | p-Value | |
|---|---|---|---|
| Depression | |||
| Yes (n,%) | 29 (33.7) | 61 (25.3) | 0.134 |
| No (n,%) | 57 (66.3) | 180 (74.7) | |
| Median (IQR) | 3 (1–6) | 2 (0–5) | 0.026 |
| Mean ± SD | 4.05 ± 3.89 | 3.05 ± 3.50 | - |
| Anxiety | |||
| Yes (n,%) | 38 (44.2) | 74 (30.7) | 0.024 |
| No (n,%) | 48 (55.8) | 167 (69.3) | |
| Median (IQR) | 3 (1–6) | 2 (0–4) | 0.038 |
| Mean ± SD | 3.71 ± 3.49 | 2.86 ± 3.18 | - |
References
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the psychological impact of COVID-19 among healthcare workers: A meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Muller, R.A.; Stensland, R.S.; van de Velde, R.S. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 1, 113441. [Google Scholar] [CrossRef]
- Cai, Z.; Cui, Q.; Liu, Z.; Li, J.; Gong, X.; Liu, J.; Wan, Z.; Yuan, X.; Li, X.; Chen, C.; et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J. Psychiatr. Res. 2020, 131, 132–137. [Google Scholar] [CrossRef]
- Chew, Q.H.; Chia, F.L.; Ng, W.K.; Lee, W.C.; Tan, P.L.; Wong, C.S.; Puah, S.H.; Shelat, V.G.; Seah, E.J.; Huey, C.W.; et al. Perceived Stress, Stigma, Traumatic Stress Levels and Coping Responses amongst Residents in Training across Multiple Specialties during COVID-19 Pandemic—A Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 6572. [Google Scholar] [CrossRef]
- Kwong, A.S.; Pearson, R.M.; Adams, M.J.; Northstone, K.; Tilling, K.; Smith, D.; Fawns-Ritchie, C.; Bould, H.; Warne, N.; Zammit, S.; et al. Mental health during the COVID-19 pandemic in two longitudinal UK population cohorts. Br. J. Psychiatry 2020, 218, 334–343. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences of the Coronavirus 2020 Pandemic (COVID-19) in Spain. A longitudinal study. Front. Psychiatry 2020, 11, 1256. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Ding, H.; Zhang, Y.; Zhang, B.; Guo, Y.; Cheung, T.; Hall, B.J.; Shi, T.; Xiang, Y.T.; Tang, Y. Prevalence of poor psychiatric status and sleep quality among frontline healthcare workers during and after the COVID-19 outbreak: A longitudinal study. Transl. Psychiatry 2021, 11, 223. [Google Scholar] [CrossRef]
- Van Steenkiste, E.; Schoofs, J.; Gilis, S.; Messiaen, P. Mental health impact of COVID-19 in frontline healthcare workers in a Belgian Tertiary care hospital: A prospective longitudinal study. Acta Clin. Belg. 2021, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, E.; Pullman, S.; Cotea, C.; Nasveld, P. Effects of deployment on health behaviours in military forces: A review of longitudinal studies. J. Mil. Veterans Health 2013, 21, 14–23. [Google Scholar]
- Rao, A.K.; Th’ng, F.; Mak, C.C.M.; Neo, H.N.; Ubeynarayana, C.U.; Kumar, R.K.N.; Mao, D.R.H. Factors associated with Mental Health Outcomes in Emergency Department Healthcare Workers on the frontlines of the COVID-19 Pandemic. Singap. Med. J. Date Cit. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Verdolini, N.; Amoretti, S.; Montejo, L.; García-Rizo, C.; Hogg, B.; Mezquida, G.; Rabelo-da-Ponte, F.D.; Vallespir, C.; Radua, J.; Martinez-Aran, A.; et al. Resilience and mental health during the COVID-19 pandemic. J. Affect. Disord. 2021, 283, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995; ISBN 7334-1423-7330. [Google Scholar]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Sasaki, N.; Asaoka, H.; Kuroda, R.; Tsuno, K.; Imamura, K.; Kawakami, N. Sustained poor mental health among healthcare workers in COVID-19 pandemic: A longitudinal analysis of the four-wave panel survey over 8 months in Japan. J. Occup. Health 2021, 63, e12227. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Huang, D.; Huang, H.; Zhang, J.; Guo, L.; Liu, Y.; Ma, H.; Geng, Q. The psychological impact of COVID-19 pandemic on medical staff in Guangdong, China: A cross-sectional study. Psychol. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Ji, Y.J.; Duan, X.Z.; Li, W.G.; Sun, Z.Q.; Song, X.A.; Meng, Y.H.; Tang, H.M.; Chu, F.; Niu, X.X.; et al. Prevalence of psychological symptoms among Ebola survivors and healthcare workers during the 2014-2015 Ebola outbreak in Sierra Leone: A cross-sectional study. Oncotarget 2017, 8, 12784. [Google Scholar] [CrossRef] [Green Version]
- Mokhtari, R.; Moayedi, S.; Golitaleb, M. COVID-19 pandemic and health anxiety among nurses of intensive care units. Int. J. Ment. Health Nurs. 2020, 29, 1275. [Google Scholar] [CrossRef]
- Batra, K.; Sharma, M.; Batra, R.; Singh, T.P.; Schvaneveldt, N. Assessing the psychological impact of COVID-19 among college students: An evidence of 15 countries. Healthcare 2021, 9, 222. [Google Scholar] [CrossRef]
- Xu, J.; Xu, Q.H.; Wang, C.M.; Wang, J. Psychological status of surgical staff during the COVID-19 outbreak. Psychiatry Res. 2020, 288, 112955. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Liao, Z.; Huang, H.; Jiang, B.; Zhang, X.; Wang, Y.; Zhao, M. Comparison of the indicators of psychological stress in the population of Hubei province and non-endemic provinces in China during two weeks during the coronavirus disease 2019 (COVID-19) outbreak in February 2020. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e923767-1. [Google Scholar]
- Ruggieri, S.; Ingoglia, S.; Bonfanti, R.C.; Coco, G.L. The role of online social comparison as a protective factor for psychological wellbeing: A longitudinal study during the COVID-19 quarantine. Personal. Individ. Differ. 2021, 171, 110486. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Liu, D.; Baumeister, R.F.; Veilleux, J.C.; Chen, C.; Liu, W.; Yue, Y.; Zhang, S. Risk factors associated with mental illness in hospital discharged patients infected with COVID-19 in Wuhan, China. Psychiatry Res. 2020, 292, 113297. [Google Scholar] [CrossRef]
- Pappa, S.; Sakkas, N.; Sakka, E. A Year in Review: Sleep Dysfunction and Psychological Distress in Healthcare Workers during the COVID-19 Pandemic. Sleep Med. 2021. [Google Scholar] [CrossRef]
- Fteropoulli, T.; Kalavana, T.V.; Yiallourou, A.; Karaiskakis, M.; Koliou Mazeri, M.; Vryonides, S.; Hadjioannou, A.; Nikolopoulos, G.K. Beyond the physical risk: Psychosocial impact and coping in healthcare professionals during the COVID-19 pandemic. J. Clin. Nurs. 2021. [Google Scholar] [CrossRef] [PubMed]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.A.; Ellis, L.; Polson, R.; O’Malley, C.M. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: Implications for supporting psychological well-being. BMC Public Health 2021, 21, 104. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M.; et al. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PLoS ONE 2020, 15, e0238217. [Google Scholar]
- Schaufeli, W.B.; Greenglass, E.R. Introduction to special issue on burnout and health. Psychol. Health 2001, 16, 501–510. [Google Scholar] [CrossRef]
- Duarte, I.; Teixeira, A.; Castro, L.; Marina, S.; Ribeiro, C.; Jácome, C.; Martins, V.; Ribeiro-Vaz, I.; Pinheiro, H.C.; Silva, A.R.; et al. Burnout among Portuguese healthcare workers during the COVID-19 pandemic. BMC Public Health 2020, 20, 1885. [Google Scholar] [CrossRef]
- Ahola, K.; Hakanen, J.; Perhoniemi, R.; Mutanen, P. Relationship between burnout and depressive symptoms: A study using the person-centred approach. Burn. Res. 2014, 1, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Okoli, C.T.; He, H.; Feng, F.; Li, J.; Zhuang, L.; Lin, M. Factors associated with compassion satisfaction, burnout, and secondary traumatic stress among Chinese nurses in tertiary hospitals: A cross-sectional study. Int. J. Nurs. Stud. 2020, 102, 103472. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef]
- Nanda, A. The Straits Time. More Doctors in Singapore Face Burnout, Anxiety amid the Pandemic. Available online: https://www.straitstimes.com/life/more-doctors-in-singapore-face-burnout-anxiety-amid-the-pandemic (accessed on 5 August 2021).
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2021, 75, 224–231. [Google Scholar]
- Rossi, R.; Jannini, T.B.; Socci, V.; Pacitti, F.; Lorenzo, G.D. Stressful life events and resilience during the COVID-19 lockdown measures in Italy: Association with mental health outcomes and age. Front. Psychiatry 2021, 12, 236. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Özaslan, A. Worry, severity, controllability, and preventive behaviours of COVID-19 and their associations with mental health of Turkish healthcare workers working at a pandemic hospital. Int. J. Ment. Health Addict. 2021, 3, 1–5. [Google Scholar]
- Pan, X.; Xiao, Y.; Ren, D.; Xu, Z.M.; Zhang, Q.; Yang, L.Y.; Liu, F.; Hao, Y.S.; Zhao, F.; Bai, Y.H. Prevalence of mental health problems and associated risk factors among military healthcare workers in specialized COVID-19 hospitals in Wuhan, China: A cross-sectional survey. Asia-Pac. Psychiatry 2020, 21, e12427. [Google Scholar] [CrossRef]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Mo, Y.; Deng, L.; Zhang, L.; Lang, Q.; Liao, C.; Wang, N.; Qin, M.; Huang, H. Work stress among Chinese nurses to support Wuhan in fighting against COVID-19 epidemic. J. Nurs. Manag. 2020, 28, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.M.; Green, J. Factor structure of the depression anxiety stress Scale-21 (DASS-21): Unidimensionality of the Arabic version among Egyptian drug users. Subst. Abus. Treat. Prev. Policy 2019, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Alkhamees, A.A.; Hori, H.; Kim, Y.; Kunugi, H. The Depression Anxiety Stress Scale 21: Development and Validation of the Depression Anxiety Stress Scale 8-Item in Psychiatric Patients and the General Public for Easier Mental Health Measurement in a Post COVID-19 World. Int. J. Environ. Res. Public Health 2021, 18, 10142. [Google Scholar] [CrossRef]
- Updates on Singapore’s COVID-19 Situation. Ministry of Health Singapore. Available online: https://www.moh.gov.sg/covid-19 (accessed on 1 July 2021).

| Characteristics | June 2020 | June 2021 | p-Value |
|---|---|---|---|
| Gender (n,%) | |||
| Female | 173 (71.8) | 173 (71.8) | - |
| Male | 68 (28.2) | 68 (28.2) | |
| Ethnicity (n,%) | |||
| Chinese | 93 (38.6) | 93 (38.6) | - |
| Malay | 25 (10.3) | 25 (10.3) | |
| Indian | 34 (14.1) | 34 (14.1) | |
| Filipino | 77 (32.0) | 77 (32.0) | |
| Others | 12 (5.0) | 12 (5.0) | |
| Age group in years (n,%) | |||
| 21–30 | 104 (43.2) | 86 (35.7) | 0.573 |
| 31–40 | 100 (41.5) | 113 (46.9) | |
| 41–50 | 28 (11.6) | 32 (13.3) | |
| 51–60 | 6 (2.5) | 6 (2.5) | |
| >60 | 3 (1.2) | 4 (1.7) | |
| Marital status (n,%) | |||
| Single | 126 (52.3) | 115 (47.7) | 0.605 |
| Married | 113 (46.9) | 122 (50.6) | |
| Separated/Divorced | 1 (0.4) | 3 (1.2) | |
| Widowed | 1 (0.4) | 1 (0.4) | |
| Occupation (n,%) | |||
| Doctors: Senior doctors | 22 (9.1) | 22 (9.1) | - |
| Junior doctors | 36 (14.9) | 36 (14.9) | |
| Nursing staff: Nurses | 172 (71.4) | 172 (71.4) | |
| Healthcare assistants | 11 (4.6) | 11 (4.6) | |
| Past medical history (n,%) | |||
| Yes | 10 (4.2) | 13 (5.4) | 0.522 |
| No | 231 (95.9) | 228 (94.6) | |
| Living with young children (<12 years old) (n,%) | |||
| Yes | 36 (14.9) | 49 (20.3) | 0.120 |
| No | 205 (85.1) | 192 (79.7) | |
| Living with elderly (>65 years old) (n,%) | |||
| Yes | 34 (14.1) | 41 (17.0) | 0.379 |
| No | 207 (85.9) | 200 (83.0) | |
| Lives alone (n,%) | |||
| Yes | 35 (14.5) | 41 (17.0) | 0.453 |
| No | 206 (85.5) | 200 (83.0) | |
| Practices a religion (n,%) | |||
| Yes | 181 (75.1) | 182 (75.5) | 0.916 |
| No | 60 (24.9) | 59 (24.5) | |
| Has family or close friend with COVID-19 (n,%) | |||
| Yes | 20 (8.3) | 39 (16.2) | 0.008 |
| No | 221 (91.7) | 202 (83.8) | |
| COVID-19 vaccinated (1 or 2 doses) (n,%) | |||
| Yes | - | 220 (91.3) | - |
| No | - | 21 (8.7) | |
| Concerns about infection risk (Mean ± SD) | 4.18 ± 0.80 | 3.92 ± 0.85 | 0.000 |
| Concerns about working environment (Mean ± SD) | 4.14 ± 0.84 | 3.94 ± 0.99 | 0.003 |
| Concerns about workload (Mean ± SD) | 4.06 ± 0.98 | 4.37 ± 0.92 | 0.000 |
| Social connectedness (Mean ± SD) | 4.55 ± 0.65 | 4.40 ± 0.69 | 0.002 |
| Workplace support (Mean ± SD) | 4.83 ± 0.67 | 4.63 ± 0.72 | 0.000 |
| Depression in 2020 (n) | Depression in 2021 (n,%) | |||||
| Normal | Mild | Moderate | Severe | Extremely Severe | Total in 2020 | |
| Normal | 149 (82.3) | 14 (7.8) | 16 (8.9) | 0 | 1 (0.6) | 180 |
| Positive for Depression | ||||||
| Mild | 15 (55.6) | 6 (22.2) | 3 (11.1) | 0 | 3 (11.1) | 27 |
| Moderate | 7 (29.2) | 6 (24.0) | 6 (24.0) | 3 (12.5) | 2 (8.3) | 24 |
| Severe | 0 | 0 | 2 (40.0) | 0 | 3 (60.0) | 5 |
| Extremely severe | 1 (20.0) | 2 (40.0) | 1 (20.0) | 0 | 1 (20.0) | 5 |
| Total in 2021 | 172 (71.4) | 28 (11.6) | 28 (11.6) | 3 (1.2) | 10 (4.1) | 241 |
| Anxiety in 2020 (n) | Anxiety in 2021 (n,%) | |||||
| Normal | Mild | Moderate | Severe | Extremely Severe | Total in 2020 | |
| Normal | 144 (86.2) | 9 (5.4) | 12 (7.2) | 0 | 2 (1.2) | 167 |
| Positive for Anxiety | ||||||
| Mild | 16 (66.7) | 1 (4.2) | 5 (20.8) | 1 (4.2) | 1 (4.2) | 24 |
| Moderate | 11 (37.9) | 3 (10.3) | 11 (37.9) | 4 (13.8) | 0 | 29 |
| Severe | 4 (40.0) | 0 | 3 (30.0) | 1 (10.0) | 2 (20.0) | 10 |
| Extremely severe | 1 (10.0) | 1 (10.0) | 1 (10.0) | 2 (20.0) | 5 (50.0) | 10 |
| Total in 2021 | 176 (73.0) | 14 (5.8) | 32 (13.3) | 8 (3.3) | 10 (4.1) | 241 |
| MHOs | June 2020 Mean (± SD) | June 2021 Mean (± SD) | June 2020 Median (IQR) | June 2021 Median (IQR) | p-Value * |
|---|---|---|---|---|---|
| All HCWs (n = 241) | |||||
| Depression | 3.05 ± 3.50 | 3.45 ± 3.91 | 2 (0–5) | 2 (0–5) | 0.181 |
| Anxiety | 2.85 ± 3.19 | 2.54 ± 3.11 | 2 (0–4) | 2 (0–4) | 0.045 |
| Doctors (n = 58) | |||||
| Depression | 2.71 ± 4.18 | 3.60 ± 4.50 | 1 (0–3) | 3 (0–5) | 0.018 |
| Anxiety | 2.02 ± 3.0 | 1.78 ± 2.59 | 1 (0–3) | 1 (0–3) | 0.259 |
| Nursing Staff (n = 183) | |||||
| Depression | 3.16 ± 3.27 | 3.40 ± 3.72 | 2 (1–5) | 2 (0–5) | 0.815 |
| Anxiety | 3.12 ± 3.18 | 2.79 ± 3.23 | 2 (1–4) | 2 (0–4) | 0.086 |
| Depression | Anxiety | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age group (Ref: <31 years) | ||||
| 31–40 years | 1.6 (0.5–4.8) | 0.419 | 0.5 (0.2–1.6) | 0.245 |
| 41 years and above | 7.9 (1.1–55.6) | 0.039 | 1.6 (0.3–9.6) | 0.631 |
| Female | 1.0 (0.3–3.2) | 0.970 | 2.3 (0.7–7.6) | 0.178 |
| Ethnicity (Ref: Chinese) | ||||
| Filipino | 0.7 (0.2–2.6) | 0.617 | 0.5 (0.1–1.7) | 0.258 |
| Others | 0.8 (0.2–2.4) | 0.664 | 1.3 (0.4–4.1) | 0.703 |
| Married | 0.4 (0.1–1.1) | 0.084 | 1.6 (0.6–4.1) | 0.374 |
| Occupation (Ref: Physician) | ||||
| Nursing staff | 1.0 (0.3–3.9) | 0.998 | 1.4 (0.3–5.5) | 0.664 |
| Number of years in occupation | 0.9 (0.8–1.0) | 0.019 | 1.0 (0.9–1.1) | 0.382 |
| Living with elderly (Ref: No) | 6.3 (1.8–21.8) | 0.004 | 7.9 (2.3–27.2) | 0.001 |
| Living with young children (Ref: No) | 0.7 (0.2–2.6) | 0.601 | 0.1 (0–0.6) | 0.006 |
| Coping Strategies_Religion (Ref: No) | 0.8 (0.2–2.8) | 0.753 | 2.7 (0.7–10.3) | 0.138 |
| Concerns about infection risk | 1.2 (0.7–2.1) | 0.485 | 1.8 (1.03–3.0) | 0.039 |
| Concerns about workload | 2.0 (1.2–3.4) | 0.008 | 1.4 (0.9–2.4) | 0.155 |
| Concerns about working environment | 1.6 (0.9–2.7) | 0.058 | 1.5 (0.9–2.4) | 0.107 |
| Perceptions about workplace support | 0.5 (0.2–0.9) | 0.037 | 1.0 (0.5–2) | 0.934 |
| Perceptions about social connectedness | 0.3 (0.1–0.6) | 0.001 | 0.6 (0.3–1.2) | 0.173 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Th’ng, F.; Rao, K.A.; Ge, L.; Mao, D.; Neo, H.N.; Molina, J.A.D.; Seow, E. A One-Year Longitudinal Study: Changes in Depression and Anxiety in Frontline Emergency Department Healthcare Workers in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11228. https://doi.org/10.3390/ijerph182111228
Th’ng F, Rao KA, Ge L, Mao D, Neo HN, Molina JAD, Seow E. A One-Year Longitudinal Study: Changes in Depression and Anxiety in Frontline Emergency Department Healthcare Workers in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(21):11228. https://doi.org/10.3390/ijerph182111228
Chicago/Turabian StyleTh’ng, Francesca, Kailing Adriel Rao, Lixia Ge, Desmond Mao, Hwee Nah Neo, Joseph Antonio De Molina, and Eillyne Seow. 2021. "A One-Year Longitudinal Study: Changes in Depression and Anxiety in Frontline Emergency Department Healthcare Workers in the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 21: 11228. https://doi.org/10.3390/ijerph182111228