
A Comparison of Germany and the United Kingdom Indicates That More SARS-CoV-2 Circulation and Less Restrictions in the Warm Season Might Reduce Overall COVID-19 Burden


Abstract
:1. Introduction
2. Methods
3. Results
3.1. Demography and Public Health
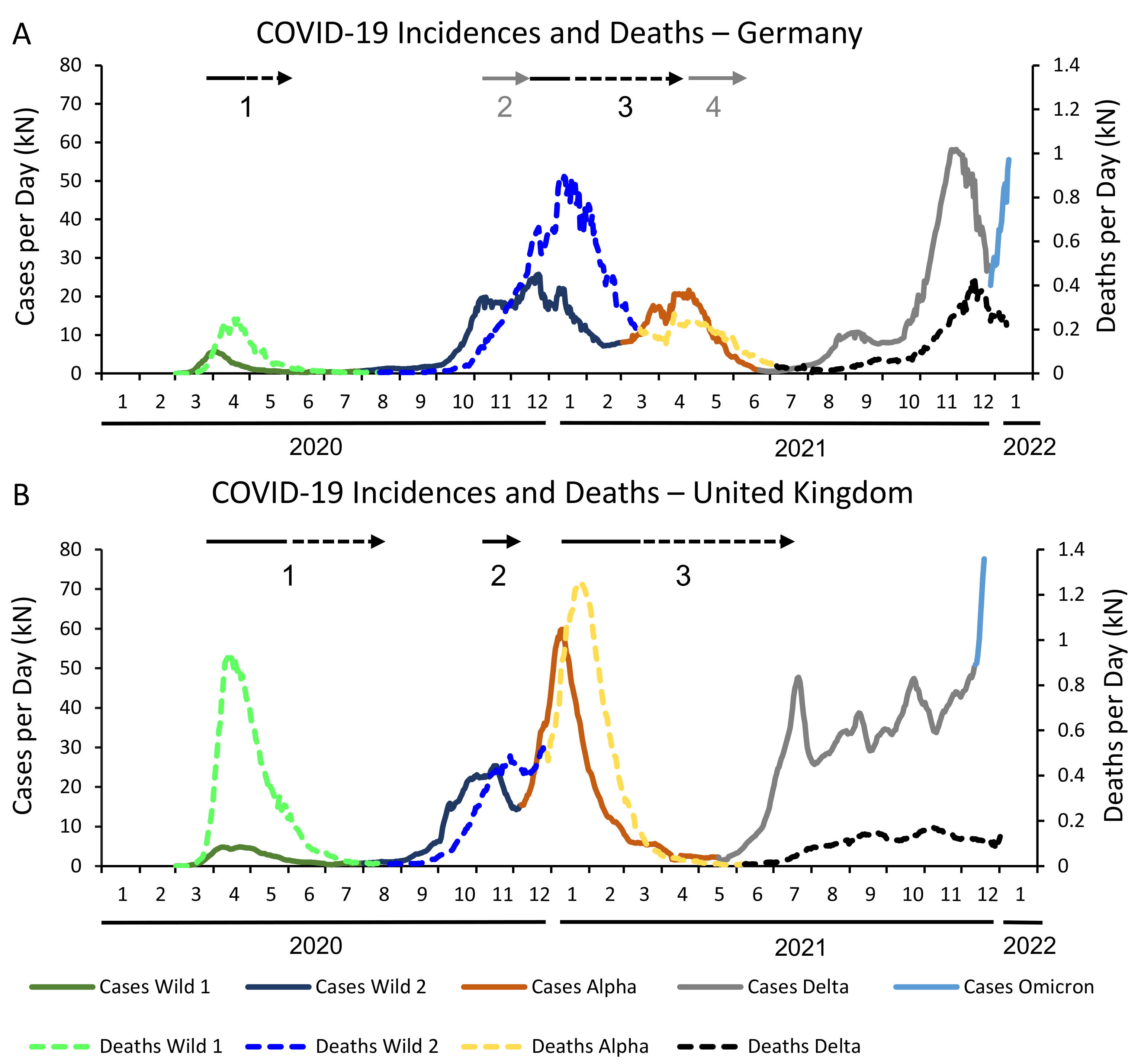
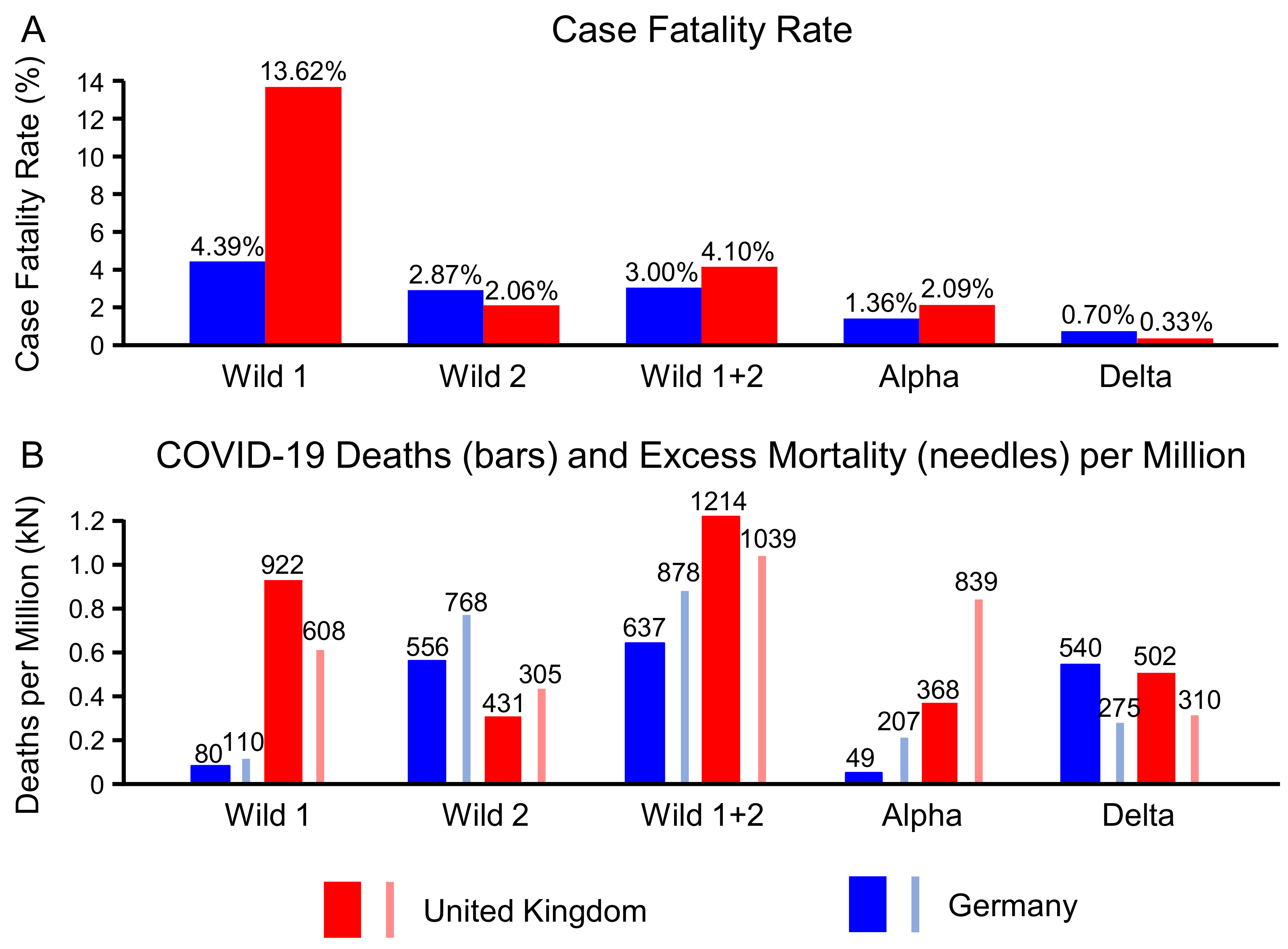
3.2. COVID-19 Incidences, Deaths, and Case Fatality Rates
3.3. Government Responses to COVID-19
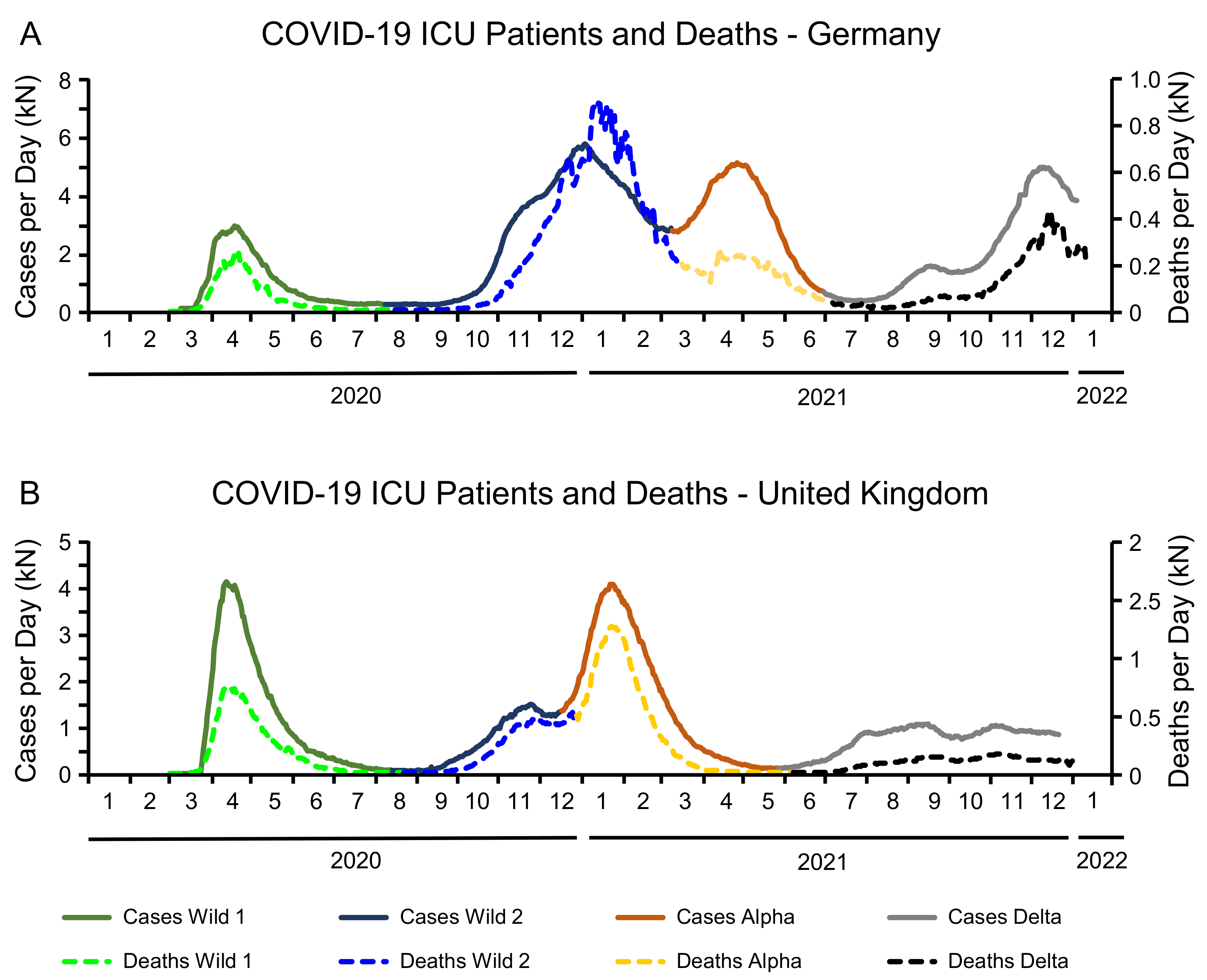
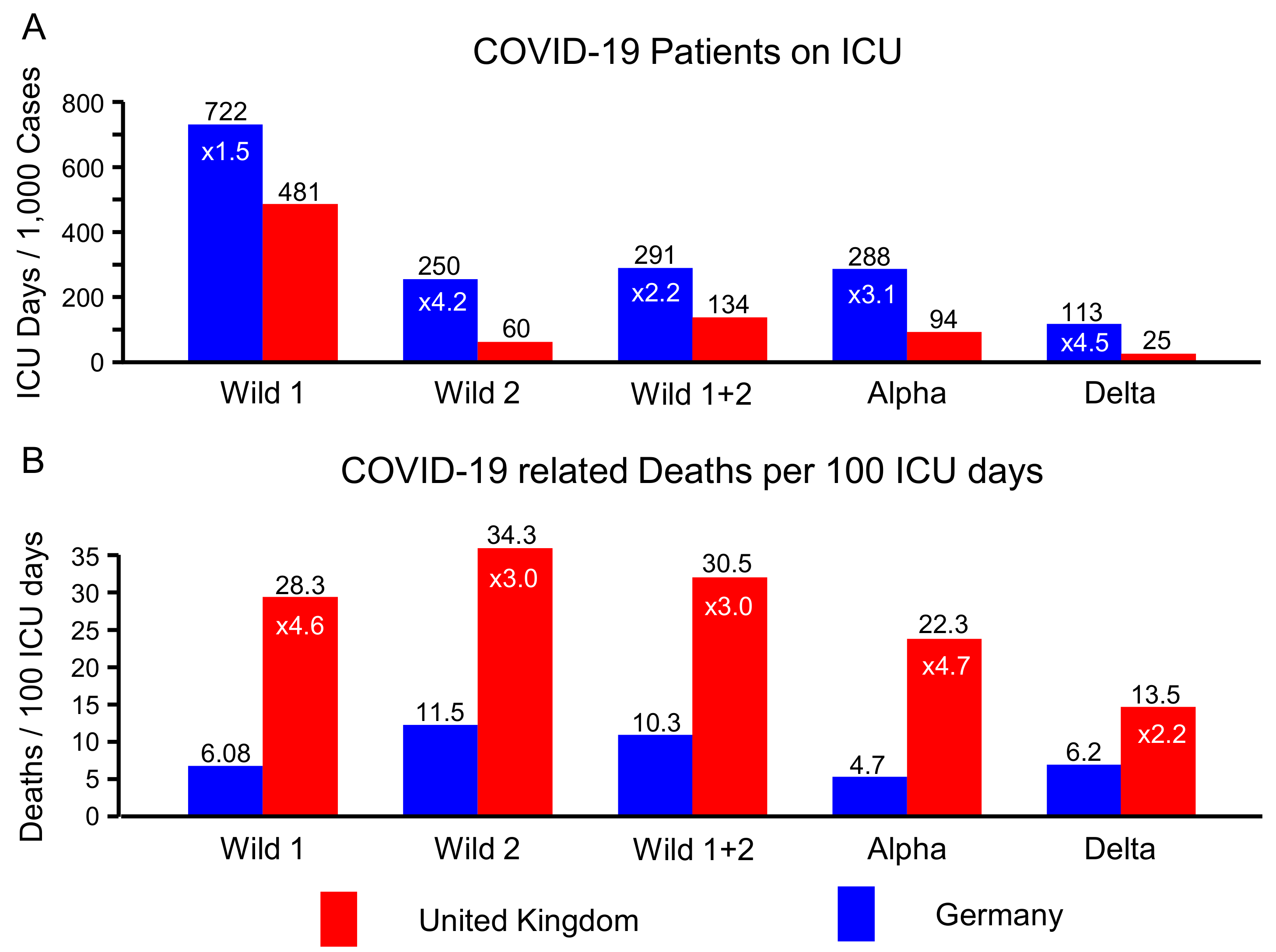
3.4. COVID-19 Related Patients in ICUs and Related Deaths
- Generally, the graph of the ICU patients and COVID-19 related deaths are highly correlated. Modeling the death curve as percentage of the ICU patients plus a constant shift for each wave individually yielded -values between and .
- Germany tends to have more patients on ICUs. This can be confirmed by the column “ICU sum” in Table 2.
- In both countries, the number of deaths per day reaches its absolute maximum in January 2021, independently of the variant. This peak is caused by the second wave of the wildtype in Germany, and by the Alpha variant in the UK.
- During the Delta period, ICU patients and deaths remained relatively constant in the UK, while both curves exhibited a steep increase in Germany.
3.5. Excess Mortality
4. Discussion
5. Conclusions
- Silent spread of SARS-CoV-2 induces immunity in affected individuals lowering extension and fatality of the following wave. The more individuals are silently affected the more pronounced the benefit.
- There is a strong seasonal association of SARS-CoV-2 epidemiology and fatality. The seasonal effect can outweigh other factors and lead to reduced efficiency of NPI.
- In the UK and in Germany, NPI in the warm season were counterproductive to achieve mild courses within the following wave.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 March 2022).
- ECDC. European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en (accessed on 13 March 2022).
- Meintrup, D.; Nowak-Machen, M.; Borgmann, S. Nine Months of COVID-19 Pandemic in Europe: A Comparative Time Series Analysis of Cases and Fatalities in 35 Countries. Int. J. Environ. Res. Public Health 2021, 18, 6680. [Google Scholar] [CrossRef] [PubMed]
- Borgmann, S.; Meintrup, D.; Reimer, K.; Schels, H.; Nowak-Machen, M. Incidence and Death Rates from COVID-19 Are Not Always Coupled: An Analysis of Temporal Data on Local, Federal, and National Levels. Healthcare 2021, 9, 338. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, S.; Mishra, S.; Scott, J.; Ferguson, N.; Gandy, A.; Bhatt, S. Reply to: The effect of interventions on COVID-19. Nature 2020, 588, E29–E32. [Google Scholar] [CrossRef] [PubMed]
- The Guardian. How Did Britain Get Its Coronavirus Response So Wrong? 2020. Available online: https://www.theguardian.com/world/2020/apr/18/how-did-britain-get-its-response-to-coronavirus-so-wrong (accessed on 1 March 2022).
- Ong, S.W.X.; Chiew, C.J.; Ang, L.W.; Mak, T.M.; Cui, L.; Toh, M.P.H.S.; Lim, Y.D.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and virological features of SARS-CoV-2 variants of concern: A retrospective cohort study comparing B.1.1.7 (Alpha), B.1.315 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 1 March 2022).
- Dong, E.; Du, H. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Our World in Data. Github Repository. Available online: https://github.com/owid/covid-19-data/tree/master/public/data/ (accessed on 1 March 2022).
- Karlinsky, A.; Kobak, D. Tracking excess mortality across countries during the COVID-19 pandemic with the World Mortality Dataset. Elife 2021. [Google Scholar] [CrossRef]
- Eurostat. Weekly Death Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Weekly_death_statistics&stable (accessed on 8 June 2022).
- Shkolnikov, V.; Barbieri, M.; Wilmoth, J. The Human Mortality Database. Available online: https://www.mortality.org/ (accessed on 8 June 2022).
- Robert Koch-Institut. Berichte zu Virusvarianten von SARS-CoV-2 in Deutschland. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/DESH/Berichte-VOC-tab.html (accessed on 1 March 2022).
- UK Health Security Agency. Investigation of SARS-CoV-2 Variants: Technical Briefings. Available online: https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-technical-briefings (accessed on 1 March 2022).
- German Ministry of Health. Coronavirus-Pandemie (SARS-CoV-2): Chronik Bisheriger Maßnahmen und Ereignisse. Available online: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html (accessed on 1 March 2022).
- Institute for Government. Timeline of UK Government Coronavirus Lockdowns and Restrictions. Available online: https://www.instituteforgovernment.org.uk/charts/uk-government-coronavirus-lockdowns (accessed on 1 March 2022).
- Statista. Altersstruktur der Bevölkerung in Deutschland zum 31. Dezember 2020. Available online: https://de.statista.com/statistik/daten/studie/1351/umfrage/altersstruktur-der-bevoelkerung-deutschlands/ (accessed on 5 April 2022).
- Office for National Statistics. UK Population Pyramid Interactive. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/ukpopulationpyramidinteractive/2020-01-08 (accessed on 5 April 2022).
- Office for National Statistics. Healthcare Expenditure, UK Health Accounts Provisional Estimates: 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthcaresystem/bulletins/healthcareexpenditureukhealthaccountsprovisionalestimates/2020 (accessed on 5 April 2022).
- DeStatis - Statistisches Bundesamt. Gesundheitsausgaben. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Gesundheitsausgaben/_inhalt.html (accessed on 5 April 2022).
- Bauer, J.; Brüggmann, D.; Klingelhöfer, D.; Maier, W.; Schwettmann, L.; Weiss, D.J.; Groneberg, D.A. Access to intensive care in 14 European countries: A spatial analysis of intensive care need and capacity in the light of COVID-19. Intensive Care Med. 2020, 46, 2026–2034. [Google Scholar] [CrossRef]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef]
- Crisis24. UK: Authorities to Implement Three-Tier Lockdown System from October 14/Update 54. 2020. Available online: https://crisis24.garda.com/alerts/2020/10/uk-authorities-to-implement-three-tier-lockdown-system-from-october-14-update-54 (accessed on 1 March 2022).
- Age UK East London. England’s Roadmap Out of the Covid-19 Lockdown. Available online: https://www.ageuk.org.uk/eastlondon/our-services/covid-19-support/roadmap/ (accessed on 23 March 2022).
- Prime Minister’s Office. Vaccination Programme Accelerated as Step 4 is Paused. Available online: https://www.gov.uk/government/news/vaccination-programme-accelerated-as-step-4-is-paused (accessed on 1 April 2022).
- HM Government. COVID-19 Response: Autumn and Winter Plan 2021. 2020. Available online: https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021 (accessed on 1 March 2022).
- Wikipedia. COVID-19-Pandemie in Deutschland. 2021. Available online: https://de.wikipedia.org/wiki/COVID-19-Pandemie_in_Deutschland (accessed on 1 March 2022).
- O’Connor, M. Covid: England Ending Isolation Laws and Mass Free Testing. Available online: https://www.bbc.com/news/uk-60467183 (accessed on 1 March 2022).
- Leung, K.; Wu, J.T.; Liu, D.; Leung, G.M. First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: A modelling impact assessment. Lancet 2020, 395, 1382–1393. [Google Scholar] [CrossRef]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Sun, J.; Shi, Z.; Xu, H. Non-pharmaceutical interventions used for COVID-19 had a major impact on reducing influenza in China in 2020. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Eikenberry, S.E.; Mancuso, M.; Iboi, E.; Phan, T.; Eikenberry, K.; Kuang, Y.; Kostelich, E.; Gumel, A.B. To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the COVID-19 pandemic. Infect. Dis. Model. 2020, 5, 293–308. [Google Scholar] [CrossRef]
- Brännström, A.; Sjödin, H.; Rocklöv, J. A Method for Estimating the Number of Infections From the Reported Number of Deaths. Front. Public Health 2021, 9, 648545. [Google Scholar] [CrossRef]
- Bicher, M.; Rippinger, C.; Schneckenreither, G.; Weibrecht, N.; Urach, C.; Zechmeister, M.; Brunmeir, D.; Huf, W.; Popper, N. Model based estimation of the SARS-CoV-2 immunization level in austria and consequences for herd immunity effects. Sci. Rep. 2022, 12, 2872. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 1 March 2022).
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. The Concept of Classical Herd Immunity May Not Apply to COVID-19. J. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Kuhbandner, C.; Homburg, S. Commentary: Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Front. Med. 2020, 7, 580361. [Google Scholar] [CrossRef]
- Mendez-Brito, A.; El Bcheraoui, C.; Pozo-Martin, F. Systematic review of empirical studies comparing the effectiveness of non-pharmaceutical interventions against COVID-19. J. Infect. 2021, 83, 281–293. [Google Scholar] [CrossRef]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef]
- Stokes, J.; Turner, A.J.; Anselmi, L.; Morciano, M.; Hone, T. The relative effects of non-pharmaceutical interventions on wave one Covid-19 mortality: Natural experiment in 130 countries. BMC Public Health 2022, 22, 1113. [Google Scholar] [CrossRef]
- Tsou, H.H.; Kuo, S.C.; Lin, Y.H.; Hsiung, C.A.; Chiou, H.Y.; Chen, W.J.; Wu, S.I.; Sytwu, H.K.; Chen, P.C.; Wu, M.H.; et al. A comprehensive evaluation of COVID-19 policies and outcomes in 50 countries and territories. Sci. Rep. 2022, 12, 8802. [Google Scholar] [CrossRef]
- Novakovic, A.; Marshall, A.H. The CP-ABM approach for modelling COVID-19 infection dynamics and quantifying the effects of non-pharmaceutical interventions. Pattern Recognit 2022, 130, 108790. [Google Scholar] [CrossRef]
- Vickers, D.M.; Baral, S.; Mishra, S.; Kwong, J.C.; Sundaram, M.; Katz, A.; Calzavara, A.; Maheu-Giroux, M.; Buckeridge, D.L.; Williamson, T. Stringency of containment and closures on the growth of SARS-CoV-2 in Canada prior to accelerated vaccine roll-out. Int. J. Infect. Dis. 2022, 118, 73–82. [Google Scholar] [CrossRef]
- Mader, S.; Rüttenauer, T. The Effects of Non-pharmaceutical Interventions on COVID-19 Mortality: A Generalized Synthetic Control Approach Across 169 Countries. Front. Public Health 2022, 10, 820642. [Google Scholar] [CrossRef]
- Chin, V.; Ioannidis, J.P.A.; Tanner, M.A.; Cripps, S. Effect estimates of COVID-19 non-pharmaceutical interventions are non-robust and highly model-dependent. J. Clin. Epidemiol. 2021, 136, 96–132. [Google Scholar] [CrossRef]
- Allen, D.W. Covid-19 Lockdown Cost/Benefits: A Critical Assessment of the Literature. Int. J. Econ. Bus. 2022, 29, 1–32. [Google Scholar] [CrossRef]
- Kratzer, S.; Pfadenhauer, L.M.; Biallas, R.L.; Featherstone, R.; Klinger, C.; Movsisyan, A.; Rabe, J.E.; Stadelmaier, J.; Rehfuess, E.; Wabnitz, K.; et al. Unintended consequences of measures implemented in the school setting to contain the COVID-19 pandemic: A scoping review. Cochrane Database Syst. Rev. 2022, 6, CD015397. [Google Scholar]
- Smolyak, A.; Bonaccorsi, G.; Flori, A.; Pammolli, F.; Havlin, S. Effects of mobility restrictions during COVID19 in Italy. Sci. Rep. 2021, 11, 21783. [Google Scholar] [CrossRef] [PubMed]
- Great Barrington Declaration. Available online: https://gbdeclaration.org/ (accessed on 8 June 2022).
- Flynn, D.; Moloney, E.; Bhattarai, N.; Scott, J.; Breckons, M.; Avery, L.; Moy, N. COVID-19 pandemic in the United Kingdom. Health Policy Technol. 2020, 9, 673–691. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut. Falldefinition Coronavirus Disease 2019 (COVID-19) (SARS-CoV-2), Stand: 23.12.2020. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Falldefinition.html (accessed on 8 June 2022).
- Our World in Data. Germany: What Is the Daily Number of Confirmed Cases? Available online: https://ourworldindata.org/coronavirus/country/germany#what-is-the-daily-number-of-confirmed-cases (accessed on 8 June 2022).
- Our World in Data. United Kingdom: Daily Confirmed Cases: How Do They Compare to Other Countries? Available online: https://ourworldindata.org/coronavirus/country/united-kingdom#what-is-the-daily-number-of-confirmed-cases (accessed on 8 June 2022).
- Linschoten, M.; Uijl, A.; Schut, A.; Jakob, C.E.M.; Romão, L.R.; Bell, R.M.; McFarlane, E.; Stecher, M.; Zondag, A.G.M.; van Iperen, E.P.A.; et al. Clinical presentation, disease course, and outcome of COVID-19 in hospitalized patients with and without pre-existing cardiac disease: A cohort study across 18 countries. Eur. Heart J. 2022, 43, 1104–1120. [Google Scholar]
- Cremer, S.; Pilgram, L.; Berkowitsch, A.; Stecher, M.; Rieg, S.; Shumliakivska, M.; Bojkova, D.; Wagner, J.U.G.; Aslan, G.S.; Spinner, C.; et al. Angiotensin II receptor blocker intake associates with reduced markers of inflammatory activation and decreased mortality in patients with cardiovascular comorbidities and COVID-19 disease. PLoS ONE 2021, 16, e0258684. [Google Scholar] [CrossRef]
- Meintrup, D.; Borgmann, S.; Seidl, K.; Stecher, M.; Jakob, C.E.M.; Pilgram, L.; Spinner, C.D.; Rieg, S.; Isberner, N.; Hower, M.; et al. Specific Risk Factors for Fatal Outcome in Critically Ill COVID-19 Patients: Results from a European Multicenter Study. J. Clin. Med. 2021, 10, 3855. [Google Scholar] [CrossRef]
- Cremer, S.; Jakob, C.; Berkowitsch, A.; Borgmann, S.; Pilgram, L.; Tometten, L.; Classen, A.; Wille, K.; Weidlich, S.; Gruener, B.; et al. Elevated markers of thrombo-inflammatory activation predict outcome in patients with cardiovascular comorbidities and COVID-19 disease: Insights from the LEOSS registry. Clin. Res. Cardiol. 2021, 110, 1029–1040. [Google Scholar] [CrossRef]
- Robert Koch-Institut. Meldeformular Meldepflichtige Krankheit Gemäß §6. July 2021. Available online: https://www.rki.de/DE/Content/Infekt/IfSG/Meldeboegen/Arztmeldungen/arztmeldung_vorschlag_des_rki_pdf (accessed on 8 June 2022).
- Keith Willett. COVID-19 Patient Notification System (CPNS). April 2020. Available online: https://www.england.nhs.uk/coronavirus/documents/covid-19-patient-notification-system-cpns/#data-capture (accessed on 8 June 2022).
- Armstrong, D. The COVID-19 pandemic and cause of death. Sociol. Health Illn. 2021, 43, 1614–1626. [Google Scholar] [CrossRef]
- Our World in Data. A Pandemic Primer on Excess Mortality Statistics and Their Comparability Across Countries. Available online: https://ourworldindata.org/covid-excess-mortality (accessed on 8 June 2022).
- Levitt, M.; Zonta, F.; Ioannidis, J.P. Comparison of pandemic excess mortality in 2020–2021 across different empirical calculations. medRxiv 2022. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Germany | UK | |
|---|---|---|
| Population Parameters | ||
| Population (million) | 83.1 | 68.2 |
| Median Age (years) | 46.6 | 40.8 |
| Percentage over 65 years | 21.5% | 18.5% |
| Mean Life Expectancy (years) | 81.3 | 81.3 |
| Public Health Costs | ||
| Total (billion): | €411 | €320 (269 Pound) |
| Costs per person: | €5298 | €4735 (3944 Pound) |
| Percentage of GDP: | 13.1% | 12.8% |
| Hospital beds | ||
| Total: | 486,700 | 141,000 |
| Beds per 1000 people: | 5.8 | 2.1 |
| ICU beds | ||
| Total: | 25,000 | 4500 |
| ICU Beds per 100,000 people: | 29.8 | 6.6 |
| Germany | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mutation/Wave | Period | Deaths | Cases | CFR | Deaths per Million | ICU sum | ICU per 1000 cases | Deaths per 100 ICU days |
| Wild 1 | 1 March 2020–31 July 2020 | 9230 | 210,320 | 4.39% | 110 | 151,841 | 722.0 | 6.1 |
| Wild 2 | 1 August 2020–1 March 2021 | 64,471 | 2,245,170 | 2.87% | 768 | 562,090 | 250.4 | 11.5 |
| Wild 1 + 2 | 1 March 2020–1 March 2021 | 73,701 | 2,455,490 | 3.00% | 878 | 713,931 | 290.7 | 10.3 |
| Alpha | 2 March 2021–21 June 2021 | 17,367 | 1,275,050 | 1.36% | 207 | 367,562 | 288.3 | 4.7 |
| Delta | 22 June 2021–27 December 2021 | 23,059 | 3,297,779 | 0.70% | 275 | 373,685 | 113.3 | 6.2 |
| UK | ||||||||
| Mutation/Wave | Period | Deaths | Cases | CFR | Deaths per Million | ICU sum | ICU per 1000 cases | Deaths per 100 ICU days |
| Wild 1 | 1 March 2020–31 July 2020 | 41,491 | 304,732 | 13.62% | 608 | 146,616 | 481.1 | 28.3 |
| Wild 2 | 1 August 2020–6 December 2020 | 29,369 | 1,422,961 | 2.06% | 431 | 85,719 | 60.2 | 34.3 |
| Wild 1 + 2 | 1 March 2020–6 December 2020 | 70,860 | 1,727,693 | 4.10% | 1039 | 232,335 | 134.5 | 30.5 |
| Alpha | 7 December 2020–16 May 2021 | 57243 | 2,738,835 | 2.09% | 839 | 256,737 | 93.7 | 22.3 |
| Delta | 17 May 2021–11 December 2021 | 21,128 | 6,362,960 | 0.33% | 310 | 156,161 | 24.5 | 13.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meintrup, D.; Nowak-Machen, M.; Borgmann, S. A Comparison of Germany and the United Kingdom Indicates That More SARS-CoV-2 Circulation and Less Restrictions in the Warm Season Might Reduce Overall COVID-19 Burden. Life 2022, 12, 953. https://doi.org/10.3390/life12070953
Meintrup D, Nowak-Machen M, Borgmann S. A Comparison of Germany and the United Kingdom Indicates That More SARS-CoV-2 Circulation and Less Restrictions in the Warm Season Might Reduce Overall COVID-19 Burden. Life. 2022; 12(7):953. https://doi.org/10.3390/life12070953
Chicago/Turabian StyleMeintrup, David, Martina Nowak-Machen, and Stefan Borgmann. 2022. "A Comparison of Germany and the United Kingdom Indicates That More SARS-CoV-2 Circulation and Less Restrictions in the Warm Season Might Reduce Overall COVID-19 Burden" Life 12, no. 7: 953. https://doi.org/10.3390/life12070953