
Behavioral and Disease-Related Characteristics of Patients with Acute Stroke during the Coronavirus Disease Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
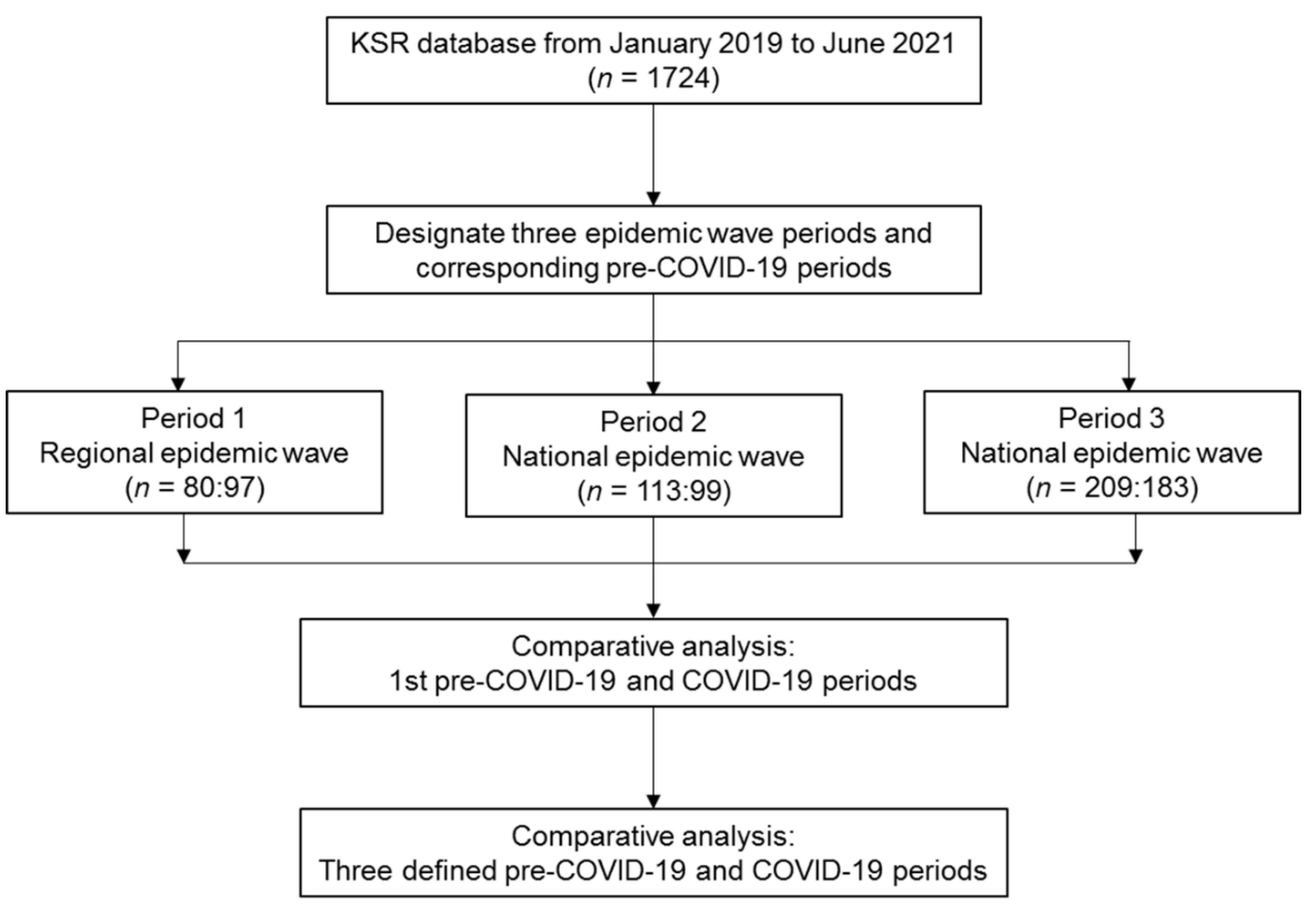
2.1. Participants, Data Source, and Ethics Statements
2.2. Study Design
2.3. Definitions of Variables
2.4. Statistical Analysis
3. Results
3.1. The Entire Pandemic Period (Periods 1, 2, and 3)
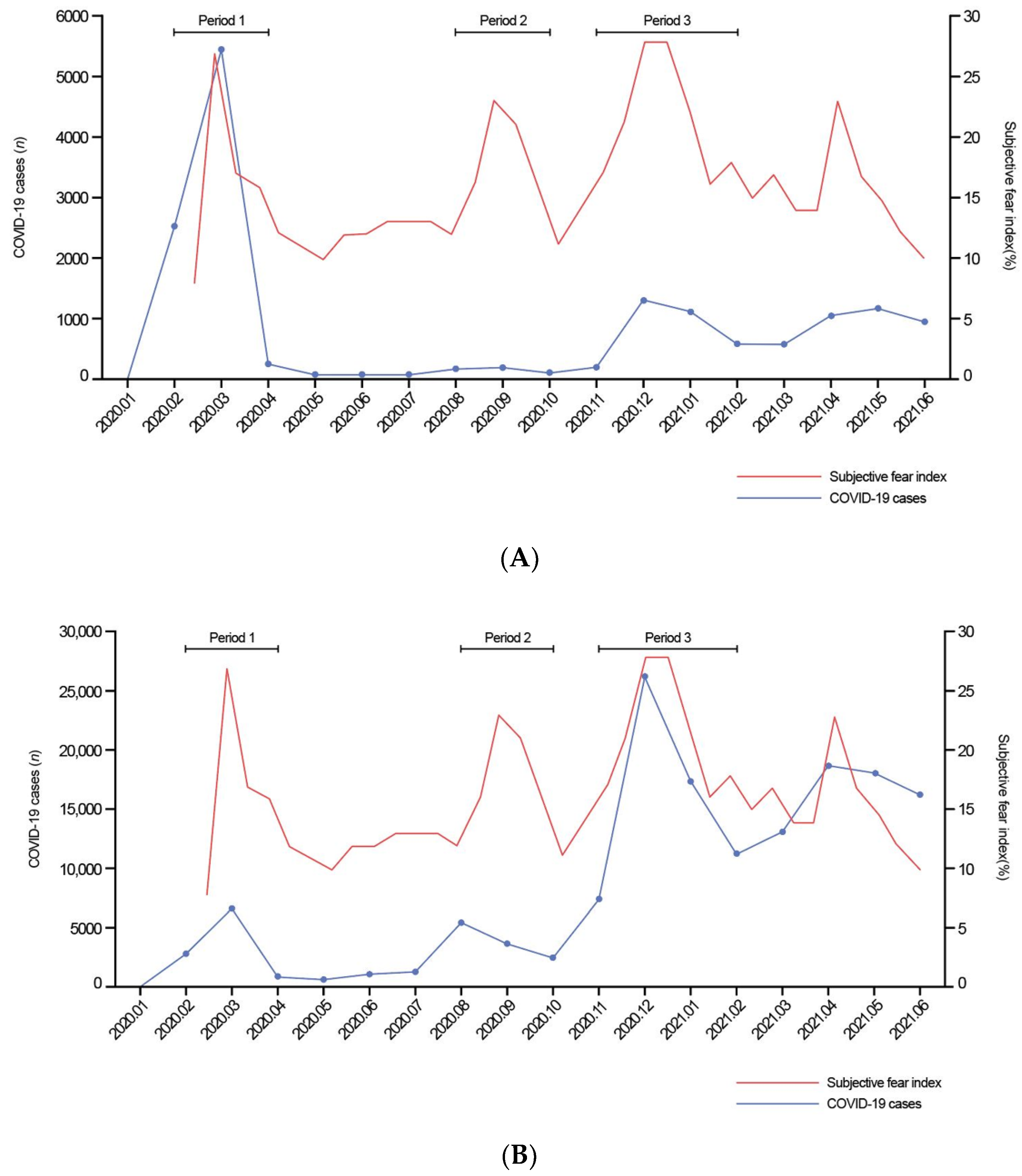
3.2. The Regional Outbreak (Period 1)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- Núñez, A.; Sreeganga, S.D.; Ramaprasad, A. Access to Healthcare during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2980. [Google Scholar] [CrossRef] [PubMed]
- Baracchini, C.; Pieroni, A.; Viaro, F.; Cianci, V.; Cattelan, A.M.; Tiberio, I.; Munari, M.; Causin, F. Acute stroke management pathway during Coronavirus-19 pandemic. Neurol. Sci. 2020, 41, 1003–1005. [Google Scholar] [CrossRef] [Green Version]
- Mai, D.T.; Phan, H.; Hoang, V.M.; Nguyen, T.D.; Phan, H.Q.; Vuong, X.T.; Dao, V.P. Treatment of stroke patients in the context of the COVID-19 pandemic: Lessons learnt from a major stroke center in Vietnam. J. Glob. Health 2021, 11, 03092. [Google Scholar] [CrossRef]
- Kansagra, A.P.; Goyal, M.S.; Hamilton, S.; Albers, G.W. Collateral Effect of Covid-19 on Stroke Evaluation in the United States. N. Engl. J. Med. 2020, 383, 400–401. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.S.; Brainin, M. COVID-19 and stroke—A global World Stroke Organization perspective. Int. J. Stroke 2020, 15, 361–364. [Google Scholar] [CrossRef]
- De Sousa, D.A.; Sandset, E.C.; Elkind, M.S.V. The Curious Case of the Missing Strokes During the COVID-19 Pandemic. Stroke 2020, 51, 1921–1923. [Google Scholar] [CrossRef]
- Samson, P.; Waingankar, N.; Shah, P.; Friedman, D.; Kavoussi, L.; Han, J. Predictors of genitourinary malignancy in patients with asymptomatic microscopic hematuria. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 10.e1–10.e6. [Google Scholar] [CrossRef]
- Jeong, H.-Y.; Lee, E.-J.; Kang, M.K.; Nam, K.-W.; Bae, J.; Jeon, K.; Jung, K.-H.; Ko, S.-B.; Oh, M.S.; Lee, J.S.; et al. Changes in Stroke Patients’ Health-Seeking Behavior by COVID-19 Epidemic Regions: Data from the Korean Stroke Registry. Cerebrovasc. Dis. 2021, 51, 169–177. [Google Scholar] [CrossRef]
- Lee, J.Y.; Jo, M.-W.; Yoo, W.-S.; Kim, H.J.; Eun, S.J. Evidence of a Broken Healthcare Delivery System in Korea: Unnecessary Hospital Outpatient Utilization among Patients with a Single Chronic Disease Without Complications. J. Korean Med. Sci. 2014, 29, 1590–1596. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Kang, K.; Kang, J.; Koo, J.; Kim, D.-H.; Kim, B.J.; Kim, W.-J.; Kim, E.-G.; Kim, J.G.; Kim, J.-M.; et al. Executive Summary of Stroke Statistics in Korea 2018: A Report from the Epidemiology Research Council of the Korean Stroke Society. J. Stroke 2019, 21, 42–59. [Google Scholar] [CrossRef] [PubMed]
- Jasne, A.S.; Sucharew, H.; Alwell, K.; Moomaw, C.J.; Flaherty, M.L.; Adeoye, O.; Woo, D.; Mackey, J.; Ferioli, S.; Martini, S.; et al. Stroke Center Certification Is Associated with Improved Guideline Concordance. Am. J. Med. Qual. 2019, 34, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Kim, S.-E.; Park, H.-K.; Cho, Y.-J.; Kim, J.Y.; Lee, K.-J.; Park, J.-M.; Park, K.-Y.; Lee, K.B.; Lee, S.J.; et al. Routing to Endovascular Treatment of Ischemic Stroke in Korea: Recognition of Need for Process Improvement. J. Korean Med. Sci. 2020, 35, e347. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, S.G.; Kim, T.H.; Park, E.-C. Healthcare Spending and Performance of Specialty Hospitals: Nationwide Evidence from Colorectal-Anal Specialty Hospitals in South Korea. Yonsei Med. J. 2015, 56, 1721–1730. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Yoo, J.W.; Lee, S.G.; Kim, T.H.; Han, K.-T.; Park, E.-C. Governmental designation of spine specialty hospitals, their characteristics, performance and designation effects: A longitudinal study in Korea. BMJ Open 2014, 4, e006525. [Google Scholar] [CrossRef] [Green Version]
- Loo, R.K.; Lieberman, S.F.; Slezak, J.M.; Landa, H.M.; Mariani, A.J.; Nicolaisen, G.; Aspera, A.M.; Jacobsen, S. Stratifying Risk of Urinary Tract Malignant Tumors in Patients with Asymptomatic Microscopic Hematuria. Mayo Clin. Proc. 2013, 88, 129–138. [Google Scholar] [CrossRef]
- Perry, R.; Banaras, A.; Werring, D.J.; Simister, R. What has caused the fall in stroke admissions during the COVID-19 pandemic? J. Neurol. 2020, 267, 3457–3458. [Google Scholar] [CrossRef]
- Venketasubramanian, N.; Anderson, C.; Ay, H.; Aybek, S.; Brinjikji, W.; de Freitas, G.R.; Del Brutto, O.H.; Fassbender, K.; Fujimura, M.; Goldstein, L.B.; et al. Stroke Care during the COVID-19 Pandemic: International Expert Panel Review. Cerebrovasc. Dis. 2021, 50, 245–261. [Google Scholar] [CrossRef]
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef]
- Demczyszak, I.; Mazurek, J.; Marciniak, D.M.; Hap, K.; Kuciel, N.; Biernat, K.; Sutkowska, E. The Use of Medical and Non-Medical Services by Older Inpatients from Emergency vs. Chronic Departments, during the SARS-CoV-2 Pandemic in Poland. Healthcare 2021, 9, 1547. [Google Scholar] [CrossRef]
- Rudilosso, S.; Laredo, C.; Vera, V.; Vargas, M.; Renú, A.; Llull, L.; Obach, V.; Amaro, S.; Urra, X.; Torres, F.; et al. Acute Stroke Care Is at Risk in the Era of COVID-19: Experience at a comprehensive stroke center in Barcelona. Stroke 2020, 51, 1991–1995. [Google Scholar] [CrossRef] [PubMed]
- Miękisiak, G.; Pettersson, S.D.; Szarek, D.; Morasiewicz, P.; Fercho, J.; Adamski, S.; Kipiński, L.; Szmuda, T. Acute Stroke Care during COVID-19: National Data. Infect. Dis. Rep. 2022, 14, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, H.; Kung, D.; Fisher, M.; Shen, Y.; Liu, R. Impact of the COVID-19 Epidemic on Stroke Care and Potential Solutions. Stroke 2020, 51, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, C.; Ebert, A.; Huttner, H.B.; Puetz, V.; Kallmünzer, B.; Barlinn, K.; Haverkamp, C.; Harloff, A.; Brich, J.; Platten, M.; et al. Acute Stroke in Times of the COVID-19 Pandemic. Stroke 2020, 51, 2224–2227. [Google Scholar] [CrossRef] [PubMed]
- Sobolewski, P.; Szczuchniak, W.; Grzesiak-Witek, D.; Wilczyński, J.; Paciura, K.; Antecki, M.; Frańczak-Prochowski, T.; Kos, M.; Kozera, G. Stroke Care During the First and the Second Waves of the COVID-19 Pandemic in a Community Hospital. Front. Neurol. 2021, 12, 655434. [Google Scholar] [CrossRef] [PubMed]
- Dula, A.N.; Brown, G.G.; Aggarwal, A.; Clark, K.L. Decrease in Stroke Diagnoses During the COVID-19 Pandemic: Where Did All Our Stroke Patients Go? JMIR Aging 2020, 3, e21608. [Google Scholar] [CrossRef]
- White, T.G.; Martinez, G.; Wang, J.; Gribko, M.; Boltyenkov, A.; Arora, R.; Katz, J.M.; Woo, H.H.; Sanelli, P.C. Impact of the COVID-19 Pandemic on Acute Ischemic Stroke Presentation, Treatment, and Outcomes. Stroke Res. Treat. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Liu, S.-A.; Wu, C.-L.; Chou, I.-J.; Wang, P.-C.; Hsu, C.-L.; Chen, C.-P. The Impacts of COVID-19 on Healthcare Quality in Tertiary Medical Centers—A Retrospective Study on Data from Taiwan Clinical Performance Indicators System. Int. J. Environ. Res. Public Health 2022, 19, 2278. [Google Scholar] [CrossRef]
- Rubin, M.A.; Bonnie, R.J.; Epstein, L.; Hemphill, C.; Kirschen, M.; Lewis, A.; Suarez, J.I. AAN position statement. Neurology 2020, 95, 167–172. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pre-COVID-19 (n = 402) | COVID-19 (n = 379) | p Value | |
|---|---|---|---|
| Acute stroke cases, n (Monthly) | 60.0 (42.0–73.0) | 53.0 (49.0–56.0) | 0.547 |
| The ratio of acute stroke admission a, % | 5.3 (4.0–6.8) | 5.6 (4.8–6.3) | 0.578 |
| Age, years | 68.0 (58.0–77.0) | 68.0 (59.0–79.0) | 0.319 |
| Male, n (%) | 230 (57.2) | 225 (59.4) | 0.591 |
| Previous mRS, n (%) | 0.193 | ||
| 0 | 376 (93.5) | 362 (95.5) | |
| 1 | 17 (4.2) | 9 (2.4) | |
| 2 | 7 (1.7) | 5 (1.3) | |
| 3 | 2 (0.5) | 0 (0.0) | |
| 4 | 0 (0.0) | 2 (0.5) | |
| 5 | 0 (0.0) | 1 (0.3) | |
| Clear onset type, n (%) | 330 (82.1) | 298 (78.6) | 0.259 |
| Time-to-arrival, hours | |||
| Onset-to-arrival (n = 330:298) | 12.4 (2.1–50.0) | 12.4 (2.3–37.3) | 0.797 |
| LNT-to-arrival (n = 72:81) | 14.3 (8.3–25.7) | 14.6 (8.6–22.9) | 0.808 |
| Admission route, n (%) | 0.991 | ||
| Outpatient | 51 (12.7) | 49 (12.9) | |
| Emergency department | 348 (86.6) | 327 (86.3) | |
| In-hospital | 3 (0.7) | 3 (0.8) | |
| Stroke type, n (%) | 0.856 | ||
| Ischemic | 297 (73.9) | 275 (72.6) | |
| Hemorrhagic | 83 (20.6) | 80 (21.1) | |
| Transient ischemic attack | 22 (5.5) | 24 (6.3) | |
| Initial NIHSS | 2.0 (1.0–5.0) | 2.0 (1.0–6.0) | 0.222 |
| Vascular risk factor, n (%) | |||
| Previous CVA | 54 (13.4) | 53 (14.0) | 0.905 |
| Coronary heart disease | 28 (7.0) | 44 (11.6) | 0.034 |
| Hypertension | 237 (59.0) | 237 (62.5) | 0.342 |
| Diabetes | 107 (26.6) | 100 (26.4) | >0.999 |
| Dyslipidemia | 227 (56.5) | 253 (66.8) | 0.004 |
| Atrial fibrillation | 46 (11.4) | 56 (14.8) | 0.202 |
| Current smoker | 102 (25.4) | 110 (29.0) | 0.286 |
| Length of stay, days | 8.5 (5.4–17.5) | 11.1 (6.5–21.9) | 0.003 |
| Discharge NIHSS | 1.0 (0.0–3.0) | 1.0 (0.0–4.0) | 0.104 |
| Expired, n (%) | 12 (3.0) | 18 (4.7) | 0.264 |
| Pre-COVID-19 (n = 297) | COVID-19 (n = 275) | p Value | |
|---|---|---|---|
| Subtype, n (%) | 0.037 | ||
| LAA | 126 (42.4) | 109 (39.6) | |
| SVO | 118 (39.7) | 100 (36.4) | |
| CE | 22 (7.4) | 41 (14.9) | |
| Other determined | 4 (1.3) | 7 (2.5) | |
| Undetermined | 27 (9.1) | 18 (6.5) | |
| Acute treatments, n (%) | 0.278 | ||
| None | 261 (87.9) | 175 (63.6) | |
| IV | 7 (2.4) | 5 (1.8) | |
| IA | 23 (7.7) | 17 (6.2) | |
| IV and IA | 6 (2.0) | 13 (4.7) | |
| Time to IV/IA, minutes | |||
| Door-to-IV (n = 13:18) | 44.0 (35.0–53.0) | 43.0 (36.5–53.5) | 0.836 |
| Door-to-IA (n = 27 a:29) | 76.0 (55.0–120.0) | 85.0 (64.75–105.0) | 0.883 |
| 1st pre-COVID-19 (n = 80) | 1st COVID-19 (n = 97) | p Value | |
|---|---|---|---|
| Age, years | 65.0 (56.0–76.0) | 67.0 (60.0–79.0) | 0.288 |
| Male, n (%) | 42 (52.5) | 55 (56.7) | 0.684 |
| Previous mRS, n (%) | 0.435 | ||
| 0 | 73 (91.2) | 92 (94.8) | |
| 1 | 3 (3.8) | 2 (2.1) | |
| 2 | 2 (2.5) | 2 (2.1) | |
| 3 | 2 (2.5) | 0 (0.0) | |
| 4 | 0 (0.0) | 1 (1.0) | |
| 5 | 0 (0.0) | 0 (0.0) | |
| Clear onset type, n (%) | 65 (81.2) | 81 (83.5) | 0.846 |
| Time-to-arrival, hours | |||
| Onset-to-arrival (n = 65:81) | 10.7 (2.3–27.0) | 15.5 (3.2–36.1) | 0.308 |
| LNT-to-arrival (n = 15:16) | 22.1 (8.9–35.9) | 15.3 (10.3–33.2) | 0.953 |
| Admission route, n (%) | 0.003 | ||
| Outpatient | 4 (5.0) | 21 (21.6) | |
| Emergency department | 76 (95.0) | 76 (78.4) | |
| In-hospital | 0 (0.0) | 0 (0.0) | |
| Stroke type, n (%) | 0.061 | ||
| Ischemic | 58 (72.5) | 80 (82.5) | |
| Hemorrhagic | 21 (26.2) | 13 (13.4) | |
| Transient ischemic attack | 1 (1.2) | 4 (4.1) | |
| Initial NIHSS | 2.0 (1.0–4.0) | 2.0 (0.0–5.0) | 0.710 |
| Vascular risk factor, n (%) | |||
| Previous CVA | 11 (13.8) | 17 (17.5) | 0.633 |
| Coronary heart disease | 8 (10.0) | 7 (7.2) | 0.696 |
| Hypertension | 49 (61.2) | 57 (58.8) | 0.856 |
| Diabetes | 25 (31.2) | 23 (23.7) | 0.341 |
| Dyslipidemia | 27 (33.8) | 74 (76.3) | <0.001 |
| Atrial fibrillation | 5 (6.2) | 10 (10.3) | 0.488 |
| Current smoker | 17 (21.2) | 29 (29.9) | 0.257 |
| Length of stay, days | 11.3 (6.6–23.1) | 9.2 (5.8–17.6) | 0.460 |
| Discharge NIHSS | 1.0 (0.0–3.0) | 1.0 (0.0–3.0) | 0.580 |
| Expired, n (%) | 4 (5.0) | 4 (4.1) | >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.; Jeong, E.; Lee, S.Y.; Kim, M.; Hong, D.Y.; Kwon, H.D.; Kim, M.-C. Behavioral and Disease-Related Characteristics of Patients with Acute Stroke during the Coronavirus Disease Pandemic. Healthcare 2022, 10, 604. https://doi.org/10.3390/healthcare10040604
Park D, Jeong E, Lee SY, Kim M, Hong DY, Kwon HD, Kim M-C. Behavioral and Disease-Related Characteristics of Patients with Acute Stroke during the Coronavirus Disease Pandemic. Healthcare. 2022; 10(4):604. https://doi.org/10.3390/healthcare10040604
Chicago/Turabian StylePark, Dougho, Eunhwan Jeong, Su Yun Lee, Mansu Kim, Dae Young Hong, Heum Dai Kwon, and Mun-Chul Kim. 2022. "Behavioral and Disease-Related Characteristics of Patients with Acute Stroke during the Coronavirus Disease Pandemic" Healthcare 10, no. 4: 604. https://doi.org/10.3390/healthcare10040604