Article Text

Abstract
SARS-CoV-2 has proven its versatility in host presentations; one such presentation is a hypercoagulable state causing large-vessel thrombosis. We report a case on a previously asymptomatic COVID-19-positive patient presenting with an acute ischaemic stroke and an incidental left internal carotid artery thrombus. The patient’s medical, social and family history and hypercoagulability screening excluded any other explanation for the left carotid thrombus or stroke, except for testing positive for the COVID-19. This case explores the known hypercoagulable state associated with COVID-19 and the effect of the virus on the host’s immune response. It also questions whether administration of recombinant tissue plasminogen activator (t-PA), according to the American Heart Association guidelines, following a negative head CT for haemorrhagic stroke is safe without prior extended imaging in this patient population. We recommend, in addition to obtaining a non-contrast CT scan of the brain, a CT angiogram or carotid duplex of the neck be obtained routinely in patients with COVID-19 exhibiting stroke symptoms before t-PA administration as the effects may be detrimental. This recommendation will likely prevent fragmentation and embolisation of an undetected carotid thrombus.
- COVID-19
- vascular surgery
- haematology (drugs and medicines)
- stroke
- haematology (incl blood transfusion)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The first reported case of SARS-CoV-2 in the USA occurred in January 2020 and shortly thereafter developed into a global pandemic. The novel virus is transmitted by respiratory droplets, human-to-human contact or contaminated objects and has a broad range of presentations.1
SARS-CoV-2 has been linked to thrombosis in both asymptomatic and symptomatic patients with COVID-19. The incidence of thrombotic events in patients infected with SARS-CoV-2 is as high as 79%.2 Within these events, arterial thrombosis ranked low in occurrences with approximately 3.7% of cases.3 Still, COVID-19 thrombotic events prove to be unpredictable in location and association with other medical conditions. The cause of venous and arterial thrombosis has been linked to an overwhelming innate immune response to SARS-COV-2 leading to systemic inflammation, coagulopathy and localised endotheliitis.
We present a case on a previously healthy female patient with COVID-19 presenting with stroke symptoms and requiring surgical intervention after an incidental finding of a left carotid artery thrombosis, despite receiving thrombolytic therapy. This case questions the current stroke imaging protocols4 and the need for additional imaging when patients present to the emergency department with stroke symptoms and are positive for COVID-19.
Case presentation
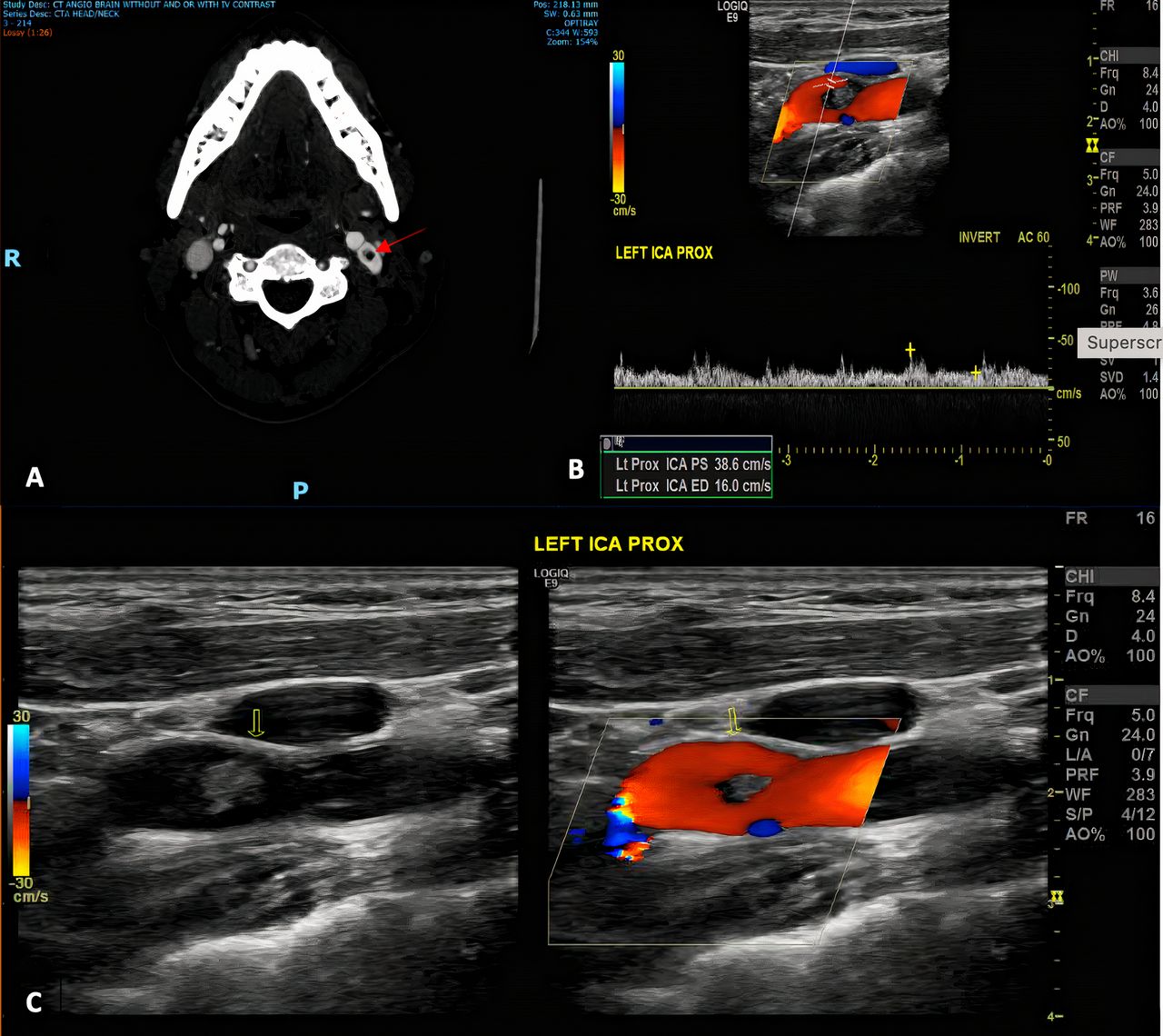
A 43-year-old woman with no significant medical, surgical or smoking history presented to the emergency department with 1-hour right-sided upper extremity weakness, slurred speech and difficulty with word finding. She reported having a headache for the past 3 days and tested positive for COVID-19 3 weeks prior. The patient was isolated in a quarantine room in the emergency department and proper COVID-19 precautions were taken by examiners, such as wearing N-95 respirator masks, goggles and gowns. On examination in the emergency room, her vitals were as follows: heart rate 65 beats/min, blood pressure (BP) 120/73 mm Hg, respiration rate 20 breaths/min and oxygen saturation 100%. Initial head CT showed no haemorrhage or stroke; however, a succeeding MRI brain following admission confirmed acute infarcts. Tissue plasminogen activator (t-PA) was administered within 30 min of arrival as she presented within 4-hour window of symptom onset. She was subsequently admitted to the intensive care unit (ICU) in an isolation room. After t-PA administration, a CT angiogram of the neck (figures 1A and 2) showed a left internal carotid artery filling defect consistent with a thrombus. A reverse transcriptase (RT)-PCR detected SARS-CoV-2, confirming the patient’s positive COVID-19 status.

(A) CT angiogram showing left ICA thrombus lodged just beyond the common carotid bifurcation. Red arrow shows an absence of contrast within the centre of the left ICA and contrast around the thrombus, showing the thrombus as free-floating within the vessel lumen. (B) Carotid duplex spectral analysis demonstrating diminished flow in the ICA. (C) Colour Doppler and B-mode grayscale showing free-floating thrombus and its location in the vessel is marked by the yellow arrows in both views. ICA, internal carotid artery.

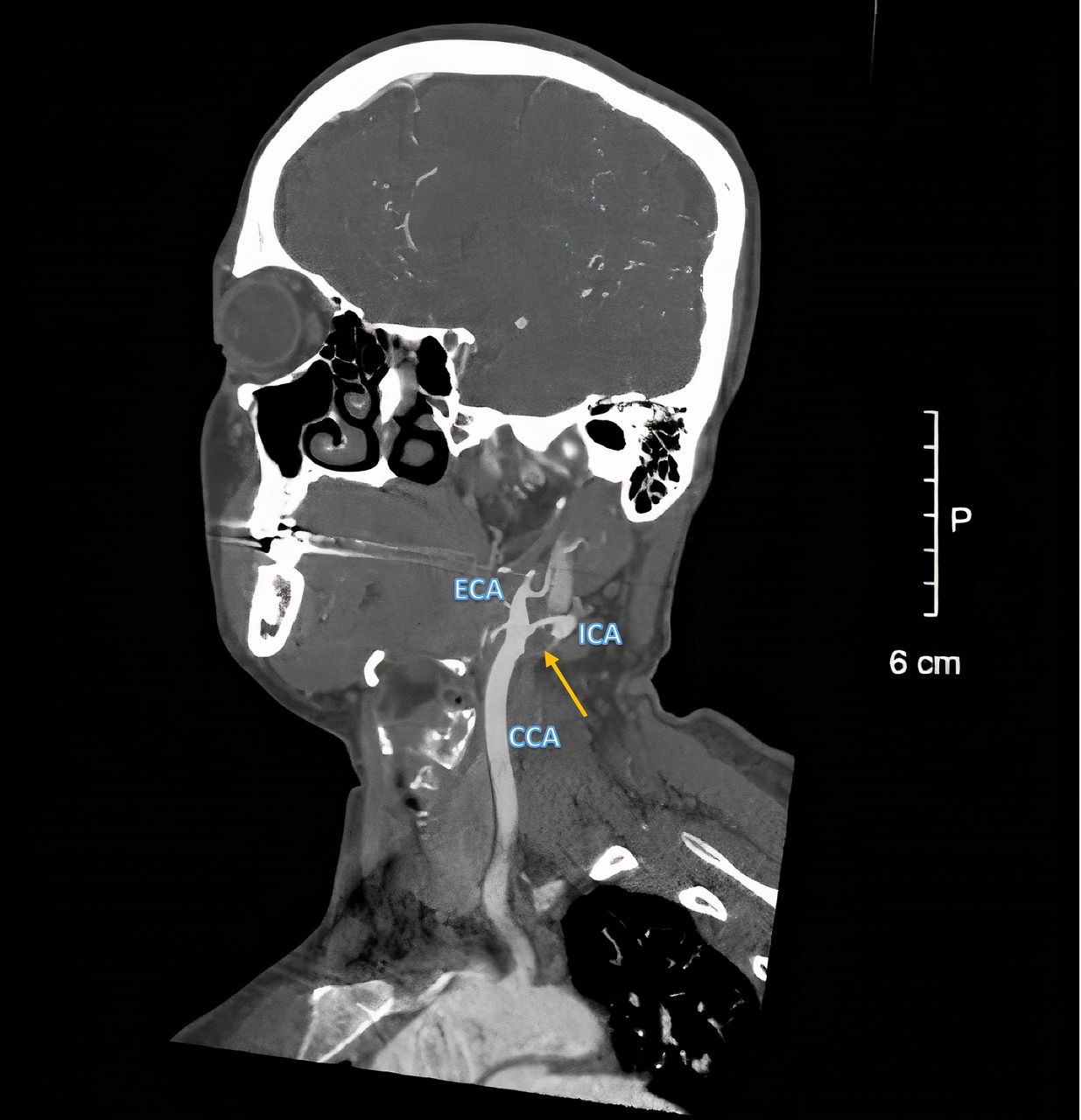
Sagittal CT of the neck showing the branches of the patient’s left CCA into the ICA and ECA. A yellow arrow identifies the thrombus within the patient’s ICA (Figure Courtesy of Dr. Tzivya Weiss, Staten Island University Hospital, Radiology). CCA, common carotid artery; ECA, external carotid artery; ICA, internal carotid artery.
On hospital day 2, the patient’s vitals remained stable and her symptoms improved with a decreasing National Institute of Health (NIH) Stroke Scale from 4, on initial presentation, to 1. As a follow-up to the CT angiogram of the neck results, a carotid duplex was performed and demonstrated a persistent free-floating internal carotid artery thrombus and diminished flow beyond (figure 1B,C). There was an associated arterial wall thickening around the thrombus, however, the clot did not appear to be adherent to the arterial wall. Although there was no thrombus in the right internal carotid artery, there was a mild 20%–39% stenosis present based on the Consensus Criteria published in 2003.5
Investigations
The patient had a thorough hypercoagulability work-up consisting of antiphospholipid antibody, hyperhomocysteinaemia, activated pro-C resistance, factor 5 Leiden, prothrombin mutation, antithrombin 3 deficiency, protein C and S deficiency, and abnormal fibrinogen and plasminogen, with all being negative. She also had a normal lipid panel, haemoglobin A1c, thyroid-stimulating hormone, urinalysis, urine toxicology screen, echocardiogram with bubble study and venous and arterial duplexes of her bilateral lower extremities. Finally, the patient denied any personal or familial history of hypercoagulability.
Treatment
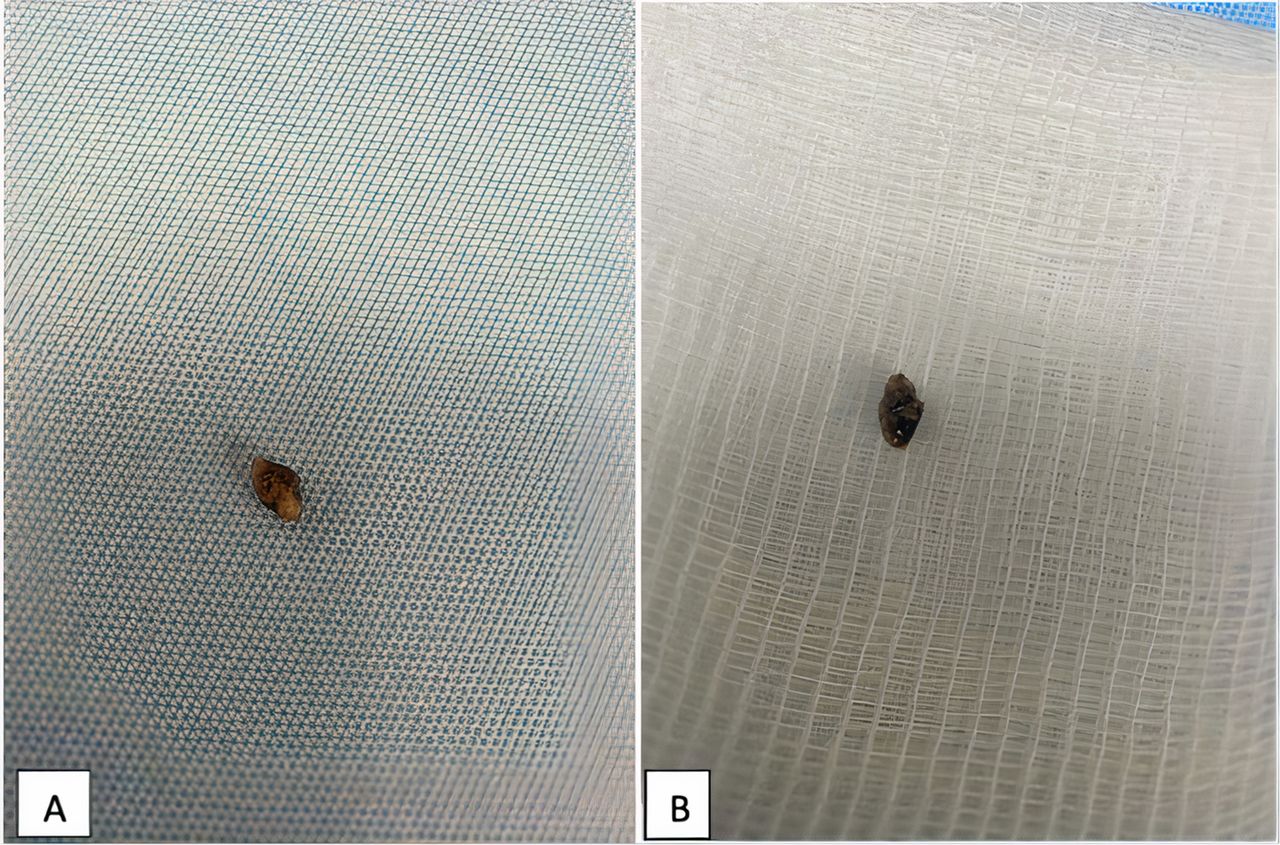
As the patient tested positive for COVID-19 3 weeks prior and had fully recovered from her viral-like respiratory symptoms at the time of admission, the treatment team opted against starting corticosteroids. To address the carotid artery thrombus, she was taken to the operating room by the vascular surgery team for a thrombectomy under general anaesthesia with an intraoperative neuromonitoring done via median nerve somatosensory evoked potentials and electroencephalogram. A standard longitudinal skin incision was made along the medial aspect of the sternocleidomastoid muscle and deepened until the carotid artery was visualised, similar to exposure of the carotid artery during a traditional carotid endarterectomy. Instead of manipulating or circumferentially dissecting the common carotid artery first, we instead secured the internal carotid artery with silastic vessel loops to avoid clot embolisation to the brain. Following control of the external, common and superior thyroid vessels and administration of weight-based intravenous heparin, the proximal internal carotid artery was incised longitudinally and the non-adherent thromboembolus was carefully extracted (figure 3) before extending the arteriotomy inferiorly along the common carotid artery. The artery appeared relatively healthy with trace fatty streaks at the bifurcation and no haemodynamically significant plaques. Given its diameter and location, we opted to reapproximate the edges of the carotid artery with a bovine pericardial patch. Arterial flow was confirmed with an intraoperative hand-held Doppler.

{kind=link}
{kind=link}
{kind=link}
Fully intact thrombus, front (A) and back (B), extracted from the left carotid artery. Thrombus consists of a fragment of dark red to tan white soft tissue measuring 0.5 cm×0.3 cm×0.2 cm. The cut surface is dark red and smooth.
Post operation, the patient was managed in the ICU with frequent neurological examinations and strict BP control, requiring intravenous hydralazine 5 mg once to maintain her systolic BP of <150 mm Hg. She was started on oral anticoagulation 6 hours post operation with apixaban (Bristol-Myers-Squibb, New Jersey, USA) 5 mg oral every 12 hours and aspirin oral 81 mg daily. Her pain was managed with oral tylenol (paracetamol) tablets 650 mg oral every 6 hours and oxycodone oral 5 mg every 6 hours, both as needed. The patient was discharged to home 2 days later neurologically intact with only mild right focal residual deficits.
Outcome and follow-up
After discharge, the patient followed up 2 weeks later as an outpatient with her vascular surgeon. The neck incisions were healing well. Her right-sided stroke symptoms had resolved and the right-hand strength and fine motor had improved to baseline. The patient’s apixaban and aspirin were continued.
One month from discharge, the patient had a repeat bilateral carotid artery duplex. The right carotid artery showed <20%–39% stenosis on duplex; the left carotid endarterectomy site was patent with no evidence of restenosis. The patient was then cleared to return to her normal daily routine and work.
Discussion
The normal function of the endothelium includes regulation of vascular tone, permeability, cell adhesion and anticoagulation. The hypercoagulability of COVID-19 stems from both the exaggerated host’s immune response to the virus as well as direct endothelial damage caused by viral invasion of these cells.6 Infected patients were found to have increased expression of ACE-2 receptors and transmembrane serine protease-2 (TMPRSS2), both expressed on the endothelium and required for viral entry. SARS-CoV-2 binding of ACE-2 receptors and TMPRSS2 indirectly promotes platelet activation and aggregation; in addition, endothelial cells lose their normal anti-inflammatory and anticoagulatory properties, promoting thrombosis.7 8
Our patient had no risk factors for stroke, besides testing positive for the coronavirus 3 weeks prior. She had no personal or family history of hypercoagulability. A complete hypercoagulable lab work-up was unremarkable, except for an elevated D-dimer of 246 ng/mL, which is common in patients with COVID-19. She is a non-smoker with a normal body mass index and cholesterol level and denied taking oral contraceptive pills. She has no history of deep vein thrombosis, pulmonary embolism or renal disease. The patient had a normal echocardiographic bubble study, largely excluding a venous embolism as the cause.
Current imaging guidelines for early management of patients who had an acute stroke include obtaining a CT head without contrast to determine whether the stroke is ischaemic or haemorrhagic. For ischaemic strokes, t-PA is administered to patients presenting 3–4.5 hours from symptoms onset.6 The goal of t-PA administration is to break down the smaller intracerebral clots causing ischaemia, thereby re-establishing cerebral blood flow in a timely manner.9 However, in patients with large-vessel thromboses, t-PA can theoretically break down larger clots into smaller fragments by converting plasminogen into plasmin, a potent enzyme, which subsequently degrades fibrin into fibrin degradation products.9 These fragments can then freely embolise to the brain causing further infarcts. Interestingly, our patient did receive t-PA as per the NIH guidelines,9 10 but it did not dissolve the thrombus. The inability of t-PA to break down the thrombus may be explained by the composition of the thrombus, which should be explored in future research.
The pandemic has altered the way we approach patients presenting with COVID-19 acute cerebral ischaemic symptoms; this includes the timing of operative management in atherosclerotic cerebrovascular disease, imaging modalities used, type of and duration of best medical management.11 Fortunately, our patient did not present with downstream lesions after t-PA administration. However, one small series by Wang et al12 described the use of mechanical thrombectomy for five patients presenting with either or both anterior and posterior circulation thrombotic occlusions. The series had technical success but there was a high rate of distal embolisation attributed to clot fragility and extent of clot burden, with a majority of poorer patient outcomes.
We encourage exploring new treatment algorithms for patients with COVID-19 with stroke-like symptoms. Based on our experience with this case, we strongly recommend obtaining and reviewing a CT angiogram of the neck and great vessels, in addition to the CT brain, prior to t-PA administration. Although t-PA did not dissolve the large-vessel clot in our patient, we encourage clinicians to use t-PA cautiously in this patient population without proper imaging of the great vessels, because of the observed hypercoagulability of COVID-19 in unpredictable locations, observed clot fragility and high rates of distal embolisation with mechanical thrombectomy.
Patient’s perspective
In late 27 December 2020, I was diagnosed with COVID-19 and spent 3 weeks quarantined until all symptoms were gone. During the 3 weeks, I exhibited typical viral symptoms such as fever, chills, malaise and cough. Notably, I did have a couple of days of chest tightness when my oxygen saturation dropped to 90% for about 10 s, but recovered and responded well to my albuterol inhaler.
In mid-January 2021, all symptoms were completely gone and I came out of quarantine doing my normal daily activities. A couple of days later, I woke up around 7 am with slurred speech and weakness in my right arm. I am a 43-year-old woman with no medical history, no family history significant for strokes, no prior medications, including no prior use of birth control. The only time I was a patient in a hospital was to give birth by vaginal delivery with no complications for the births of my three daughters. I have a very active lifestyle, exercising at least 4 times a week with weights and running.
As a prior physician assistant (PA), although all signs were leading to a diagnosis of stroke, I did not even include stroke in my differential because of the impossibility that I could be having a stroke. My top differential was Bell’s palsy. That morning, I got in my car and drove to pick up my children. I was on the phone the entire drive with my sister, who could not tell I had slurred speech. Within a few hours, it appeared to have subsided. At around noon, I started to feel the weakness radiating throughout my arm and my speech began to slur again. I walked up to my sister’s home and could not take off my zipped sneaker. When I sat on her couch, I could not articulate any words that made sense. My brother, who is an emergency medicine PA, called 911 and reported I was having a stroke.
The paramedics came immediately and brought me to emergency department. I received a CT scan and was examined by a neurologist who determined that I needed immediate tissue plasminogen activator (t-PA). Within 30 min of receiving the t-PA, I appeared more coherent and started to be more responsive.
Several physical examinations, tests and consults were performed and it was determined that I had a free-floating clot in my left carotid. The neurology team suspected it was COVID-19-related but needed to perform a complete work-up to rule out other sources. Over the course of the next couple of days, I received heparin, a duplex of my carotids, an echo, an MRI and CT scan.
On the second hospital day, the vascular surgery team told me I needed to go for emergency surgery because of the free-floating clot. I was very scared and nervous as I am a widowed mother of three minor children. Early that afternoon, I went to surgery and in a few hours was in recovery. The surgeon told me they were able to get the entire clot out and I should recover well.
On the third day of hospitalisation, I was able to get out of bed to a chair and later that evening was able to walk to the bathroom. On hospital day 4, I was discharged home on blood thinners after all the tests performed returned normal results with no indication of a causal connection to the clot.
I rested for a week then slowly returned back to my normal activities of driving and exercising. By the second week, I returned to work as an attorney. I have followed up with vascular surgery, neurology, rheumatology and cardiology teams. I have also seen a neurologist at Columbia Presbyterian Hospital to study my case. With all the blood work, including genetic testing returning with normal values, the neurologist explained that we can now say definitively this was a COVID-CLOT.
I have managed to not need any physical or occupational therapy and physically have no residual effects. At times, I do notice, although not noticeable by others, that I don’t find it as easy as before to find words fast when articulating my thoughts. For me it appears as if I have a bit of a delay when articulating my thoughts in a succinct manner.
I continue to be grateful that I am living a second chance at life. After seeing the clot that was removed, it is obvious that I was saved from a higher being because I should have died or been paralysed. Notwithstanding my gratitude, I continue to struggle with how the clot was formed in the absence of any medical reason or rationale, how the clot remained after 3–4 weeks with normal blood flow running through my body, what did the pathology of the clot show and why did I need to be tested like this. Hopefully, this experience will provide some insight to the medical professionals on their treatment or prophylaxis treatments for COVID-related diagnosis.
Learning points
A high index of suspicion is needed when dealing with acute ischaemic presentations in those with COVID-19.
COVID-19 hypercoagulability, apart from its pulmonary manifestations, can also present as large-vessel thrombosis, especially in the carotid artery.
The unpredictable nature of COVID-19 arterial complications affecting multiple vascular beds requires extended imaging evaluation beyond the traditional stroke work-up.
Careful administration of tissue plasminogen activator is required and should be judged on an individual case basis to avoid complications of incomplete thrombus lysis with potential thromboembolisation to brain tissue.
Ethics statements
Footnotes
Contributors KL: acquisition of data, interpretation of work, concept design, drafting, final approval, communication with patient and agreement to be accountable for all aspects of the work in ensuring questions related to the accuracy or integrity of any part of the work. IW-G: interpretation of work, concept design, drafting, final approval and agreement to be accountable for all aspects of the work in ensuring questions related to the accuracy or integrity of any part of the work. JS and MG: interpretation and conceptualisation of work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.