
Usefulness of the Measurement of Serum Paraoxonase-1 Arylesterase Activity in the Diagnoses of COVID-19

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Laboratory Procedures
2.3. Statistical Analyses
3. Results
3.1. Characteristics of the COVID-19-Positive Patients in the Study
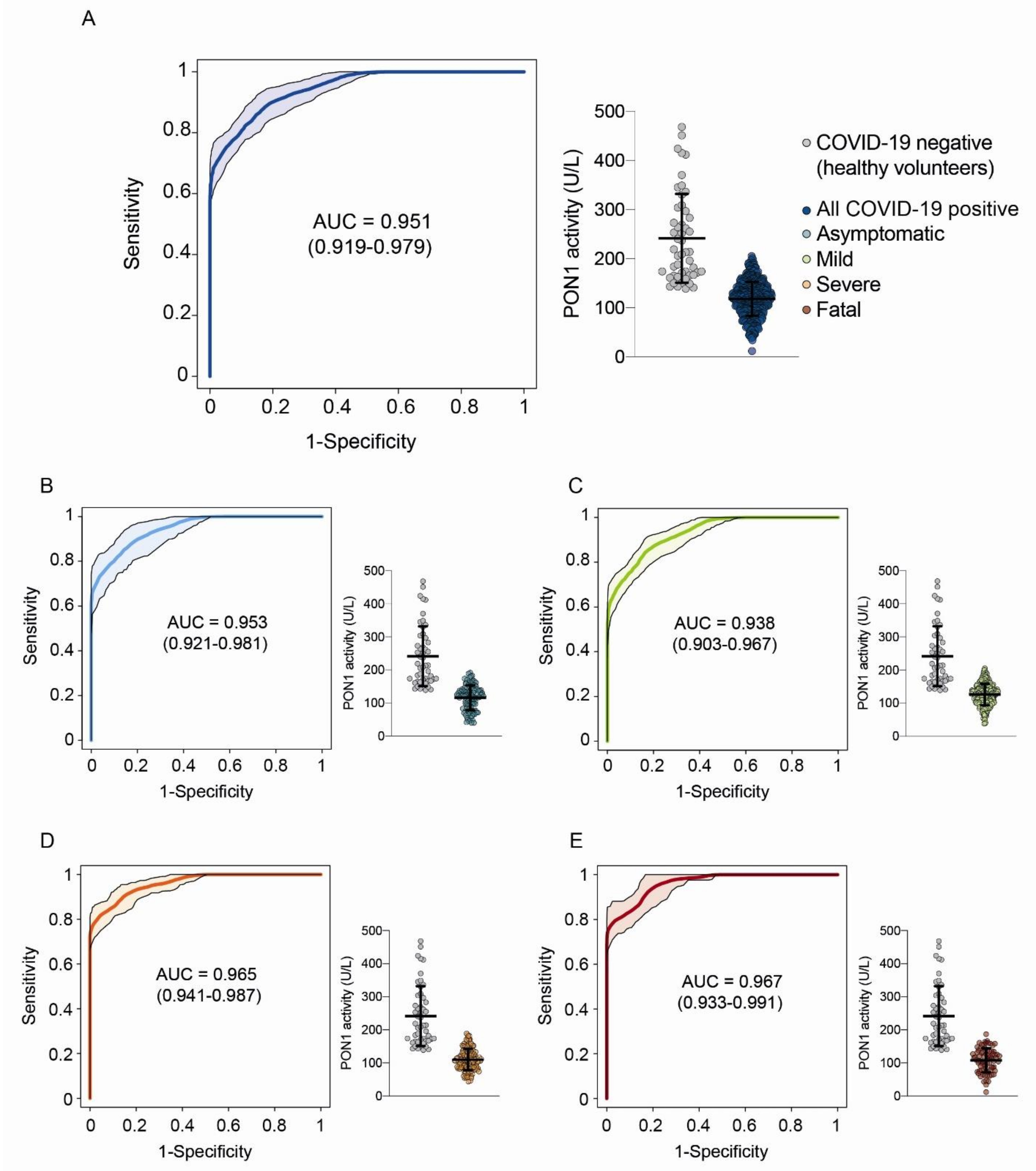
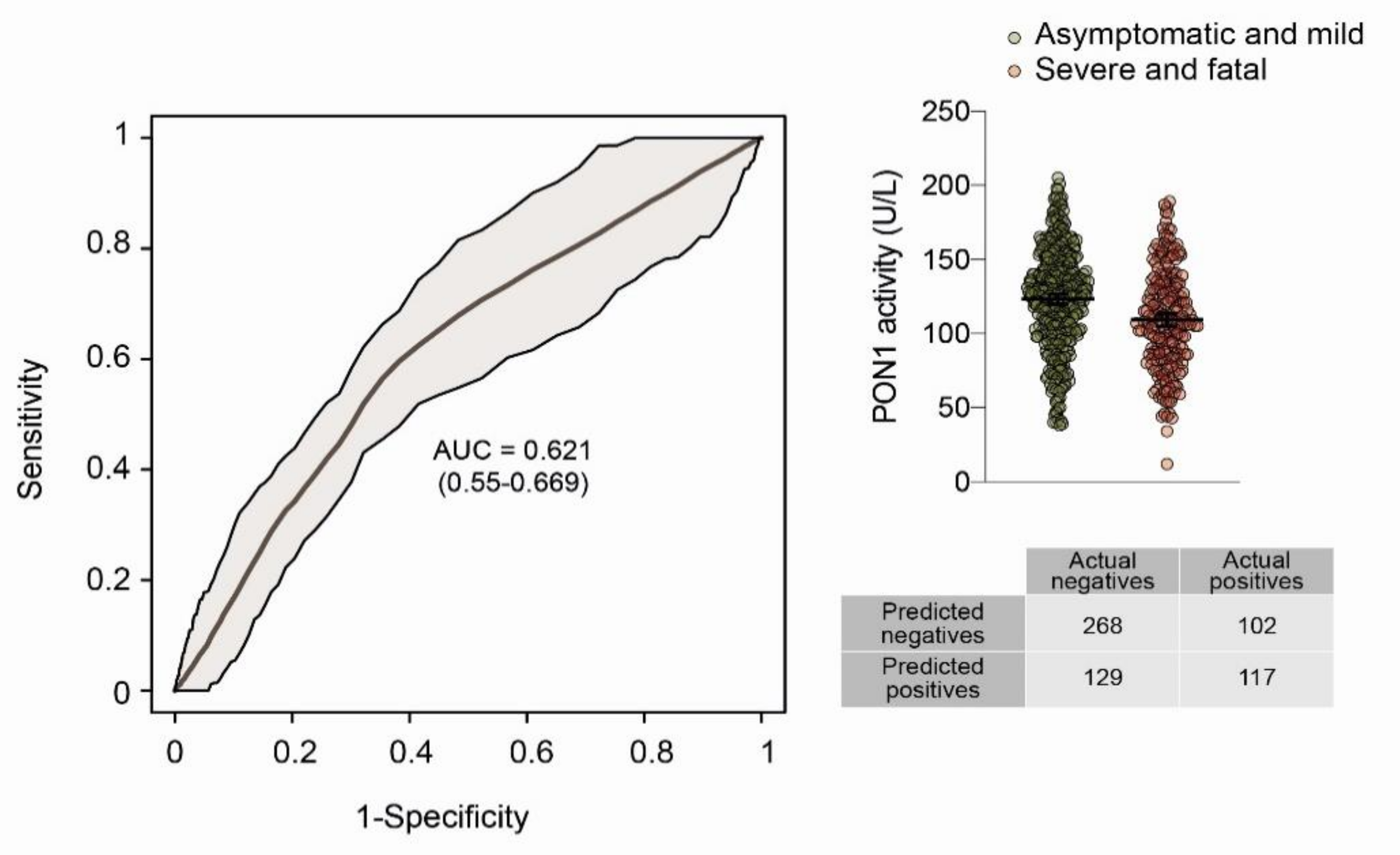
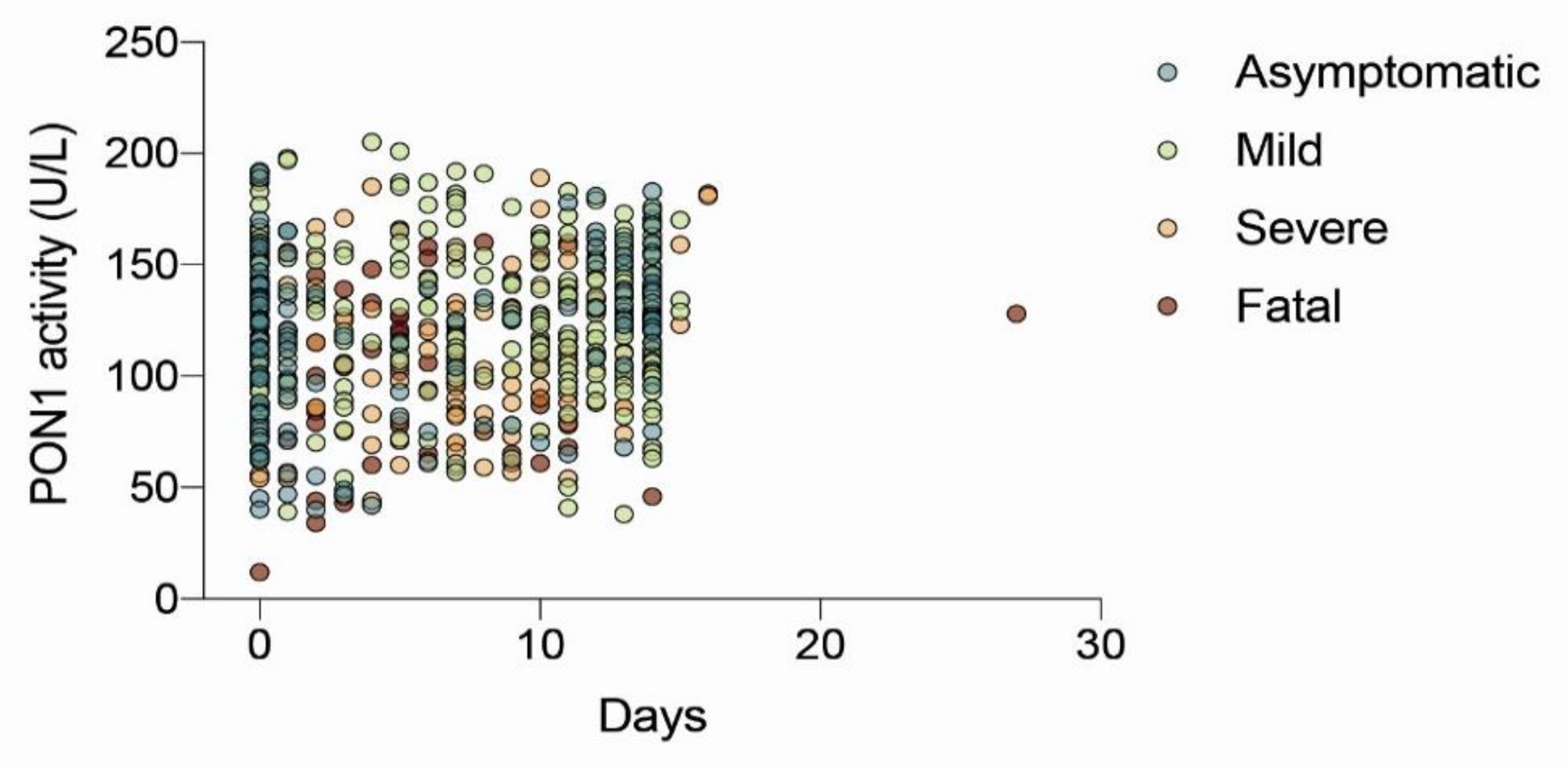
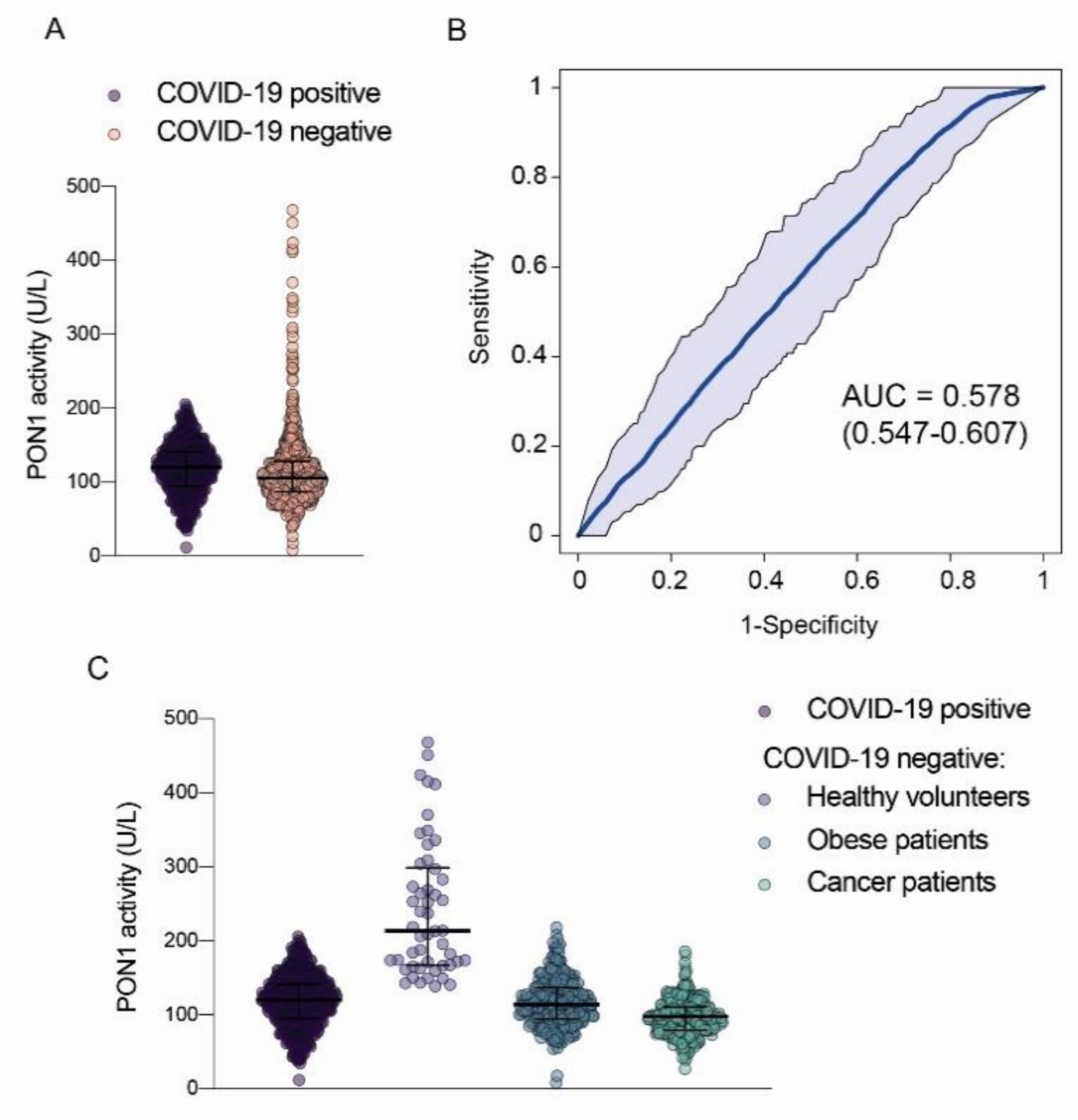
3.2. Paraoxonase-1 Activity Showed a Similar Trend toward a Decrease in COVID-19, Cancer, and Morbid Obesity Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bostan, M.; Ataman, M.; Bostan, I.S.; Bleotu. C. Targets and assay types for COVID-19 diagnosis. J. Immunoassay Immunochem. 2020, 41, 946–959. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Tomàs, E.; Iftimie, S.; Castañé, H.; Baiges-Gaya, G.; Hernández-Aguilera, A.; González-Viñas, M.; Castro, A.; Camps, J.; Joven, J. Clinical performance of paraoxonase-1-related variables and novel markers of inflammation in coronavirus disease-19. A machine learning approach. Antioxidants 2021, 10, 991. [Google Scholar] [CrossRef] [PubMed]
- Gobierno de España. Ministerio de Sanidad. Recomendaciones de Seguridad del Paciente y Profesionales en Procedimientos Intervencionistas en la Fase de Transición de la Pandemia COVID-19. Available online: https://www.sanidad.gob.es/gl/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_Procedimientos_intervencionistas.pdfhttps://www.sanidad.gob.es/gl/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_Procedimientos_intervencionistas.pdf (accessed on 20 May 2022).
- NIH. COVID-19 Treatment Guidelines. Clinical Spectrum of SARS-CoV-2 Infection. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 20 May 2022).
- Fort-Gallifa, I.; García-Heredia, A.; Hernández-Aguilera, A.; Simó, J.M.; Sepúlveda, J.; Martín-Paredero, V.; Camps, J.; Joven, J. Biochemical indices of oxidative stress and inflammation in the evaluation of peripheral artery disease. Free Radic. Biol. Med. 2016, 97, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Arenas, M.; García-Heredia, A.; Cabré, N.; Luciano-Mateo, F.; Hernández-Aguilera, A.; Sabater, S.; Bonet, M.; Gascón, M.; Fernández-Arroyo, S.; Fort-Gallifa, I.; et al. Effect of radiotherapy on activity and concentration of serum paraoxonase-1 in breast cancer patients. PLoS ONE 2017, 12, e0188633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Tomàs, E.; Murcia, M.; Arenas, M.; Arguís, M.; Gil, M.; Amigó, N.; Correig, X.; Torres, L.; Sabater, S.; Baiges-Gayà, G.; et al. Serum paraoxonase-1-related variables and lipoprotein profile in patients with lung or head and neck cancer: Effect of radiotherapy. Antioxidants 2019, 8, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabré, N.; Luciano-Mateo, F.; Fernández-Arroyo, S.; Baiges-Gayà, G.; Hernández-Aguilera, A.; Fibla, M.; Fernández-Julià, R.; París, M.; Sabench, F.; Castillo, D.D.; et al. Laparoscopic sleeve gastrectomy reverses non- alcoholic fatty liver disease modulating oxidative stress and inflammation. Metabolism 2019, 99, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Tomàs, E.; Arenas, M.; Gómez, J.; Acosta, J.; Trilla, J.; López, Y.; Árquez, M.; Torres, L.; Araguas, P.; Hernández-Aguilera, A.; et al. Identification of potential metabolic biomarkers of rectal cancer and of the effect of neoadjuvant radiochemotherapy. PLoS ONE 2021, 16, e0250453. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Marsillach, J.; Joven, J. The paraoxonases: Role in human diseases and methodological difficulties in measurement. Crit. Rev. Clin. Lab. Sci. 2009, 46, 83–106. [Google Scholar] [CrossRef]
- Gaita, L.; Manzi, B.; Sacco, R.; Lintas, C.; Altieri, L.; Lombardi, F.; Pawlowski, T.L.; Redman, M.; Craig, D.W.; Huentelman, M.J.; et al. Decreased serum arylesterase activity in autism spectrum disorders. Psychiatry Res. 2010, 180, 105–113. [Google Scholar] [CrossRef]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef] [PubMed]
- Trevethan, R. Sensitivity, specificity, and predictive values: Foundations, pliabilities, and pitfalls in research and practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Castañé, H.; Rodríguez-Tomàs, E.; Baiges-Gaya, G.; Hernández-Aguilera, A.; Arenas, M.; Iftimie, S.; Joven, J. On the role of paraoxonase-1 and chemokine ligand 2 (C-C motif) in metabolic alterations linked to inflammation and disease. A 2021 Update. Biomolecules 2021, 11, 971. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Iftimie, S.; García-Heredia, A.; Castro, A.; Joven, J. Paraoxonases and infectious diseases. Clin. Biochem. 2017, 50, 804–811. [Google Scholar] [CrossRef]
- Iftimie, S.; García-Heredia, A.; Pujol, I.; Ballester, F.; Fort-Gallifa, I.; Simó, J.M.; Joven, J.; Camps, J.; Castro, A. Preliminary study on serum paraoxonase-1 status and chemokine (C-C motif) ligand 2 in hospitalized elderly patients with catheter- associated asymptomatic bacteriuria. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Iftimie, S.; García-Heredia, A.; Pujol, I.; Ballester, F.; Fort-Gallifa, I.; Simó, J.M.; Joven, J.; Castro, A.; Camps, J. A preliminary study of paraoxonase-1 in infected patients with an indwelling central venous catheter. Clin. Biochem. 2016, 49, 449–457. [Google Scholar] [CrossRef]
- Papotti, B.; Macchi, C.; Favero, C.; Iodice, S.; Adorni, M.P.; Zimetti, F.; Corsini, A.; Aliberti, S.; Blasi, F.; Carugo, S.; et al. HDL in COVID-19 patients: Evidence from an Italian cross-sectional study. J. Clin. Med. 2021, 10, 5955. [Google Scholar] [CrossRef]
- Villar, M.; Urra, J.M.; Rodríguez-Del-Río, F.J.; Artigas-Jerónimo, S.; Jiménez-Collados, N.; Ferreras-Colino, E.; Contreras, M.; de Mera, I.G.F.; Estrada-Peña, A.; Gortázar, C.; et al. Characterization by quantitative serum proteomics of immune-related prognostic biomarkers for COVID-19 symptomatology. Front. Immunol. 2021, 12, 730710. [Google Scholar] [CrossRef]
- Geyer, P.E.; Arend, F.M.; Doll, S.; Louiset, M.L.; Virreira Winter, S.; Müller-Reif, J.B.; Torun, F.M.; Weigand, M.; Eichhorn, P.; Bruegel, M.; et al. High-resolution serum proteome trajectories in COVID-19 reveal patient-specific seroconversion. EMBO Mol. Med. 2021, 13, e14167. [Google Scholar] [CrossRef]
- Begue, F.; Tanaka, S.; Mouktadi, Z.; Rondeau, P.; Veeren, B.; Diotel, N.; Tran-Dinh, A.; Robert, T.; Vélia, E.; Mavingui, P.; et al. Altered high-density lipoprotein composition and functions during severe COVID-19. Sci. Rep. 2021, 11, 2291. [Google Scholar] [CrossRef]
- Iftimie, S.; López-Azcona, A.F.; Vicente-Miralles, M.; Descarrega-Reina, R.; Hernández-Aguilera, A.; Riu, F.; Simó, J.M.; Garrido, P.; Joven, J.; Camps, J.; et al. Risk factors associated with mortality in hospitalized patients with SARS-CoV-2 infection. A prospective, longitudinal, unicenter study in Reus, Spain. PLoS ONE 2020, 15, e0234452. [Google Scholar] [CrossRef]
- Farsalinos, K.; Barbouni, A.; Niaura, R. Systematic review of the prevalence of current smoking among hospitalized COVID-19 patients in China: Could nicotine be a therapeutic option? Intern. Emerg. Med. 2020, 15, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Tindle, H.A.; Newhouse, P.A.; Freiberg, M.S. Beyond smoking cessation: Investigating medicinal nicotine to prevent and treat COVID-19. Nicotine Tob. Res. 2020, 22, 1669–1670. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Healthy Subjects (n = 50) | Asymptomatic COVID-19 (n = 113) | Mild COVID-19 (n = 284) | Severe COVID-19 (n = 143) | Fatal COVID-19 (n = 75) |
|---|---|---|---|---|---|
| Age (years) | 76 (67–80) | 50 (33–70) | 45 (32–56) | 73 (57–84) | 72 (53–86) |
| Sex | |||||
| Men (%) | 38 (76) | 70 (61.9) | 79 (27.7) | 83 (58.0) | 44 (61.1) |
| Women (%) | 12 (24) | 43 (38.1) | 205 (72.2) | 60 (42.0) | 28 (38.9) |
| Symptoms | |||||
| Pneumonia (%) | - | - | 12 (4.2) | 37 (25.9) | 17 (22.7) |
| Cough (%) | - | - | 91 (32.0) | 79 (55.2) | 40 (53.3) |
| Fever (%) | - | - | 115 (40.5) | 85 (59.4) | 39 (52.0) |
| Chills (%) | - | - | 5 (1.8) | 2 (1.4) | 5 (6.7) |
| Dyspnea (%) | - | - | 47 (16.5) | 73 (51.0) | 54 (72.0) |
| Vomiting (%) | - | - | 15 (5.3) | 9 (6.3) | 5 (6.7) |
| Diarrhea (%) | - | - | 36 (12.7) | 20 (14.0) | 11 (14.7) |
| Anosmia (%) | - | - | 49 (17.2) | 8 (5.6) | 1 (1.3) |
| Ageusia (%) | - | - | 40 (14.1) | 10 (7.0) | 2 (2.7) |
| Odynophagia (%) | - | - | 24 (8.5) | 7 (4.9) | 2 (2.7) |
| Headache (%) | - | - | 82 (28.9) | 11 (7.7) | 9 (12.0) |
| Anorexia/hyporexia (%) | - | - | 8 (2.8) | 8 (5.6) | 3 (4.0) |
| Myalgia (%) | - | - | 39 (13.7) | 15 (10.5) | 5 (6.7) |
| Arthralgia (%) | - | - | 31 (10.9) | 12 (8.4) | 4 (5.3) |
| Respiratory failure (%) | - | - | 5 (1.8) | 6 (4.2) | 12 (16.0) |
| Hospital stay (days) | - | - | - | 9 (6–14) | 13 (7–32) |
| Vaccine * | |||||
| Vaccinated (%) | - | 32 (28.3) | 50 (17.6) | 43 (30.1) | 20 (26.7) |
| 1st dose (%) | - | 11 (9.7) | 11 (3.9) | 16 (11.2) | 9 (12) |
| 2nd dose (%) | - | 20 (17.7) | 39 (13.7) | 27 (18.9) | 11 (14.7) |
| 3rd dose (%) | - | 1 (0.9) | 0 (0) | 0 (0) | 0 (0) |
| Deceased (%) | - | - | - | - | 31 (41.3) |
| PON1 Activity (U/L) | Diagnosis | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |||
|---|---|---|---|---|---|---|---|---|
| Negative | Positive | Total | ||||||
| 161 | Negative | 41 | 61 | 102 | 90.1 (87.4–92.3) | 82.0 (68.1–91.0) | 98.4 (96.9–99.2) | 40.2 (30.8–50.4) |
| Positive | 9 | 554 | 564 | |||||
| Total | 50 | 615 | 665 | |||||
| 205 | Negative | 28 | 0 | 28 | 100.0 (100.0–100.0) | 56.0 (41.4–69.8) | 96.6 (94.7–97.8) | 100.0 (100.0–100.0) |
| Positive | 22 | 615 | 637 | |||||
| Total | 50 | 615 | 665 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabaldó, X.; Juanpere, M.; Castañé, H.; Rodríguez-Tomàs, E.; López-Azcona, A.F.; Baiges-Gaya, G.; Castro, L.; Valverde-Díaz, E.; Muñoz-Blázquez, A.; Giménez-Cuenca, L.; et al. Usefulness of the Measurement of Serum Paraoxonase-1 Arylesterase Activity in the Diagnoses of COVID-19. Biomolecules 2022, 12, 879. https://doi.org/10.3390/biom12070879
Gabaldó X, Juanpere M, Castañé H, Rodríguez-Tomàs E, López-Azcona AF, Baiges-Gaya G, Castro L, Valverde-Díaz E, Muñoz-Blázquez A, Giménez-Cuenca L, et al. Usefulness of the Measurement of Serum Paraoxonase-1 Arylesterase Activity in the Diagnoses of COVID-19. Biomolecules. 2022; 12(7):879. https://doi.org/10.3390/biom12070879
Chicago/Turabian StyleGabaldó, Xavier, Màrius Juanpere, Helena Castañé, Elisabet Rodríguez-Tomàs, Ana Felisa López-Azcona, Gerard Baiges-Gaya, Lourdes Castro, Enrique Valverde-Díaz, Aida Muñoz-Blázquez, Laura Giménez-Cuenca, and et al. 2022. "Usefulness of the Measurement of Serum Paraoxonase-1 Arylesterase Activity in the Diagnoses of COVID-19" Biomolecules 12, no. 7: 879. https://doi.org/10.3390/biom12070879