
Development of a Fully Automated Desktop Analyzer and Ultrahigh Sensitivity Digital Immunoassay for SARS-CoV-2 Nucleocapsid Antigen Detection
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens
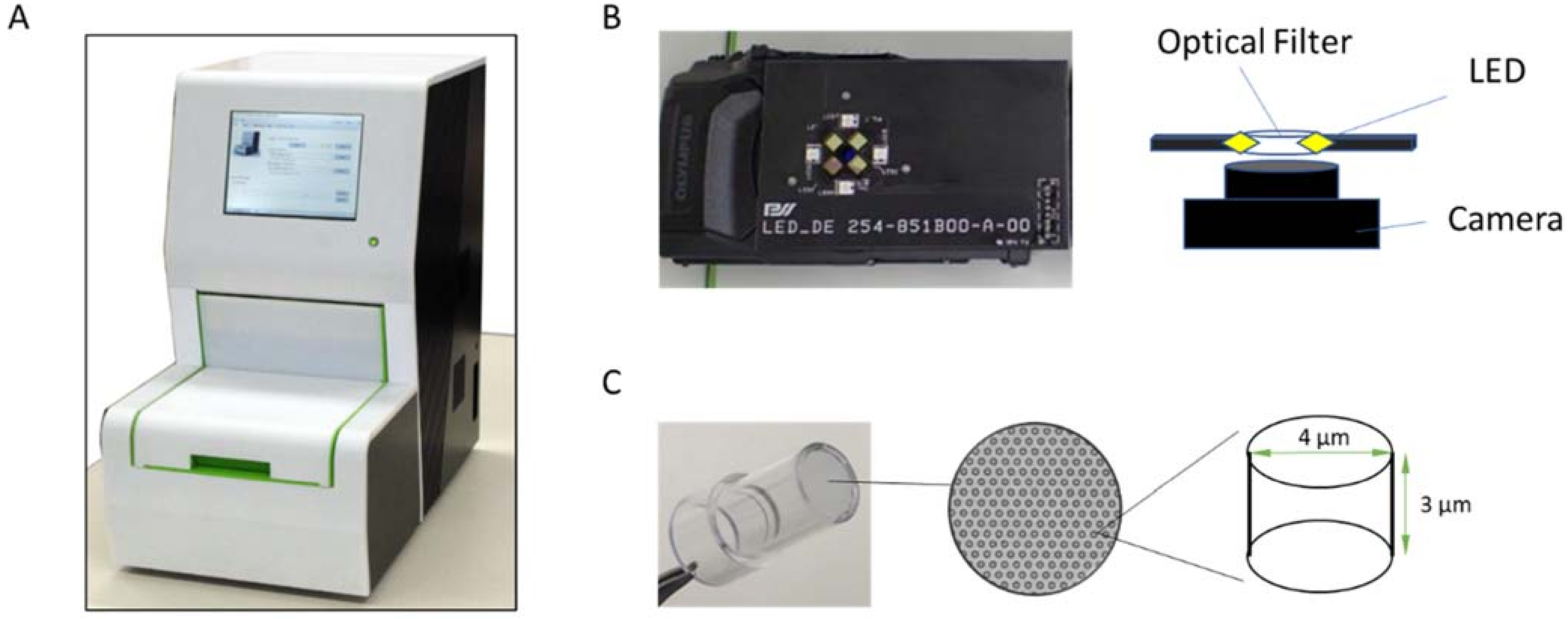
2.2. Fully Automated Desktop Analyzer
2.3. Microwell Array Device (Digital Device)
2.4. Reagents and Virus Preparation
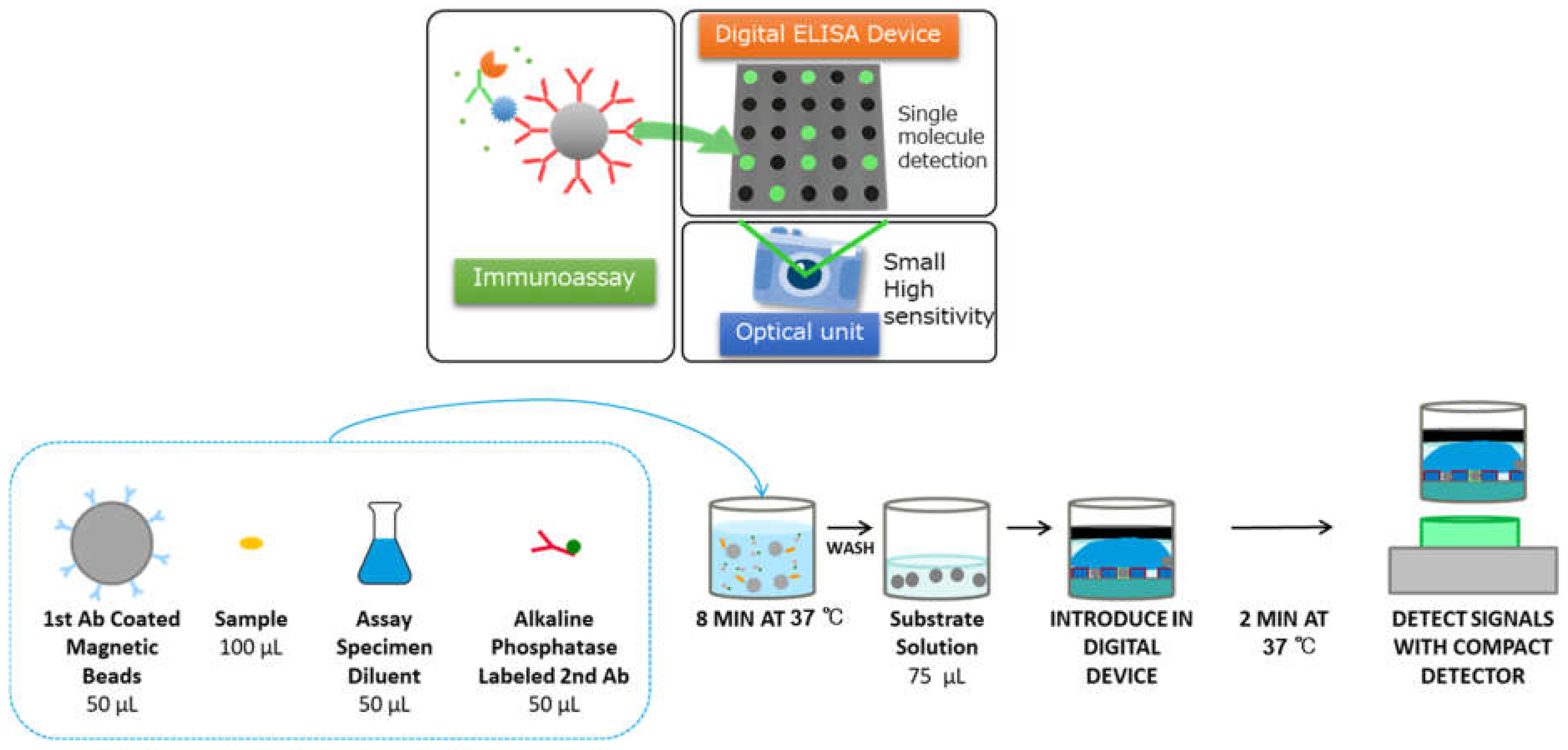
2.5. Antigen Assay
2.6. Image Processing
2.7. Data Analysis
2.8. Cross-Reactivity and Variant Detection
3. Results
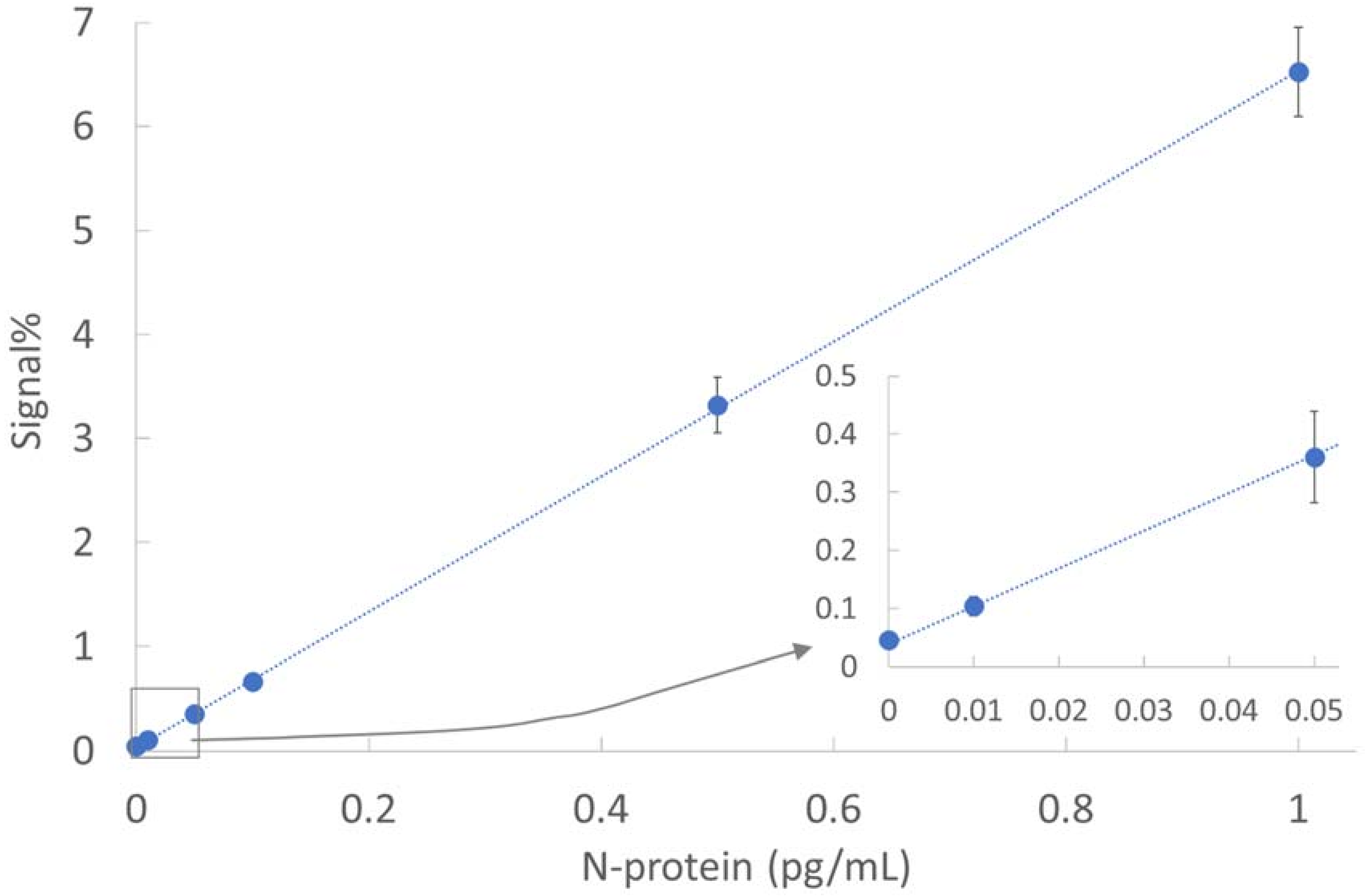
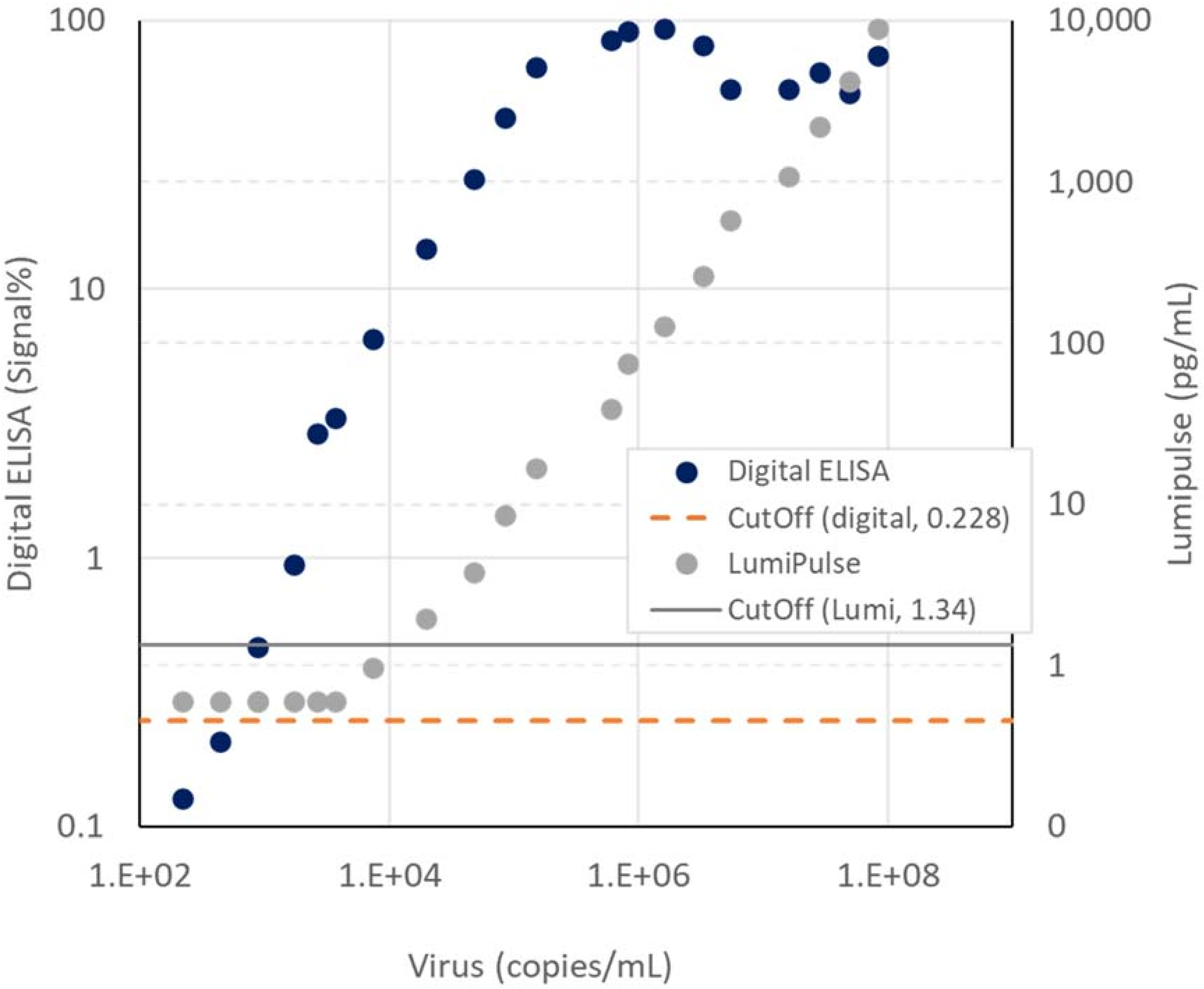
3.1. Analytical Sensitivity
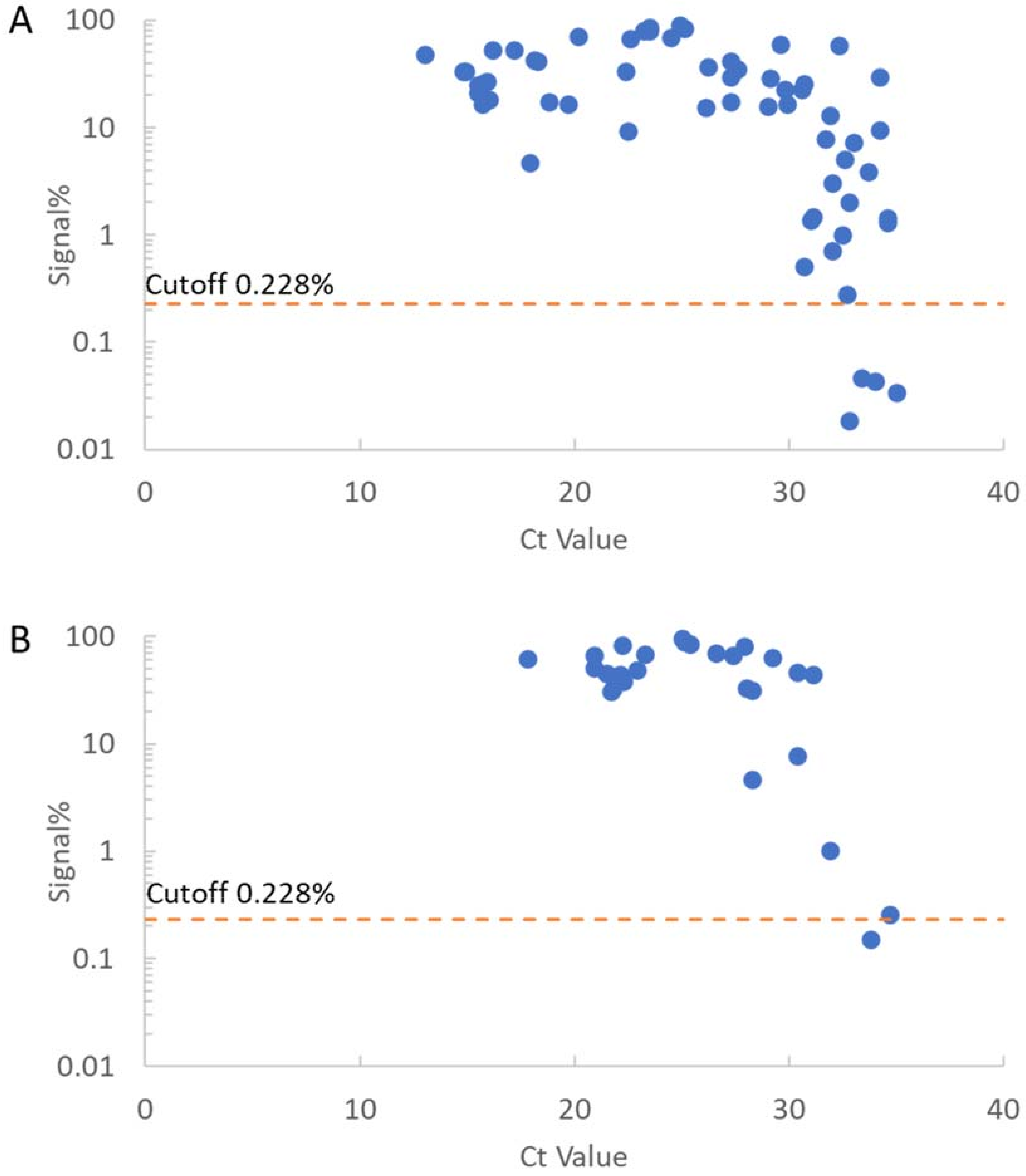
3.2. Cutoff Setting and Clinical Specificity
3.3. Clinical Sensitivity
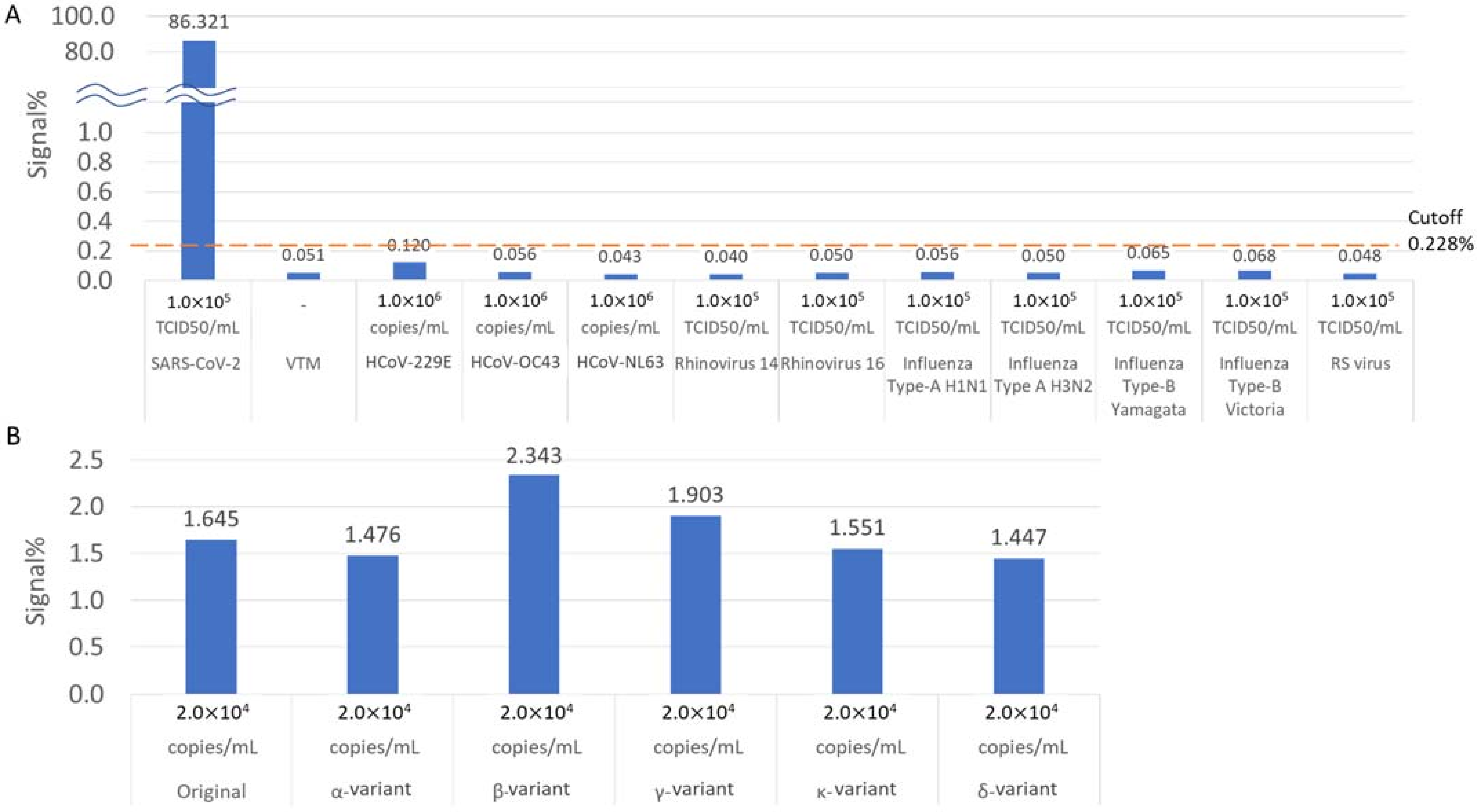
3.4. Cross-Reactivity and Variant Detection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Dattani, S.; Roser, M. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 14 September 2022).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Recommendations for National SARS-CoV-2 Testing Strategies and Diagnostic Capacities; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Pekosz, A.; Parvu, V.; Li, M.; Andrews, J.C.; Manabe, Y.C.; Kodsi, S.; Gary, D.S.; Roger-Dalbert, C.; Leitch, J.; Cooper, C.K. Antigen-Based Testing but Not Real-Time Polymerase Chain Reaction Correlates with Severe Acute Respiratory Syndrome Coronavirus 2 Viral Culture. Clin. Infect. Dis. 2021, 73, e2861–e2866. [Google Scholar] [CrossRef] [PubMed]
- U.S Food and Drug Administration. Individual EUAs for Antigen Diagnostic Tests for SARS-CoV-2; U.S Food and Drug Administration: Silver Spring, MD, USA, 2021. [Google Scholar]
- Pharmaceuticals and Medical Devices Agency. PMDA’s Efforts to Combat COVID-19; Pharmaceuticals and Medical Devices Agency: Tokyo, Japan, 2021. [Google Scholar]
- IIshii, T.; Sasaki, M.; Yamada, K.; Kato, D.; Osuka, H.; Aoki, K.; Morita, T.; Ishii, Y.; Tateda, K. Immunochromatography and chemiluminescent enzyme immunoassay for COVID-19 diagnosis. J. Infect. Chemother. 2021, 27, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Menchinelli, G.; Bordi, L.; Liotti, F.M.; Palucci, I.; Capobianchi, M.R.; Sberna, G.; Lalle, E.; Romano, L.; De Angelis, G.; Marchetti, S.; et al. Lumipulse G SARS-CoV-2 Ag assay evaluation using clinical samples from different testing groups. Clin. Chem. Lab. Med. 2021, 59, 1468–1476. [Google Scholar] [CrossRef]
- Shan, D.; Johnson, J.M.; Fernandes, S.C.; Suib, H.; Hwang, S.; Wuelfing, D.; Mendes, M.; Holdridge, M.; Burke, E.M.; Beauregard, K.; et al. N-protein presents early in blood, dried blood and saliva during asymptomatic and symptomatic SARS-CoV-2 infection. Nat. Commun. 2021, 12, 1931. [Google Scholar] [CrossRef]
- Rotman, B. Measurement of activity of single molecules of beta-D-galactosidase. Proc. Natl. Acad. Sci. USA 1961, 47, 1981–1991. [Google Scholar] [CrossRef]
- Rondelez, Y.; Tresset, G.; Tabata, K.V.; Arata, H.; Fujita, H.; Takeuchi, S.; Noji, H. Microfabricated arrays of femtoliter chambers allow single molecule enzymology. Nat. Biotechnol. 2005, 23, 361–365. [Google Scholar] [CrossRef]
- Rissin, D.M.; Walt, D.R. Digital Concentration Readout of Single Enzyme Molecules Using Femtoliter Arrays and Poisson Statistics. Nano Lett. 2006, 6, 520–523. [Google Scholar] [CrossRef]
- Sakakihara, S.; Araki, S.; Iino, R.; Noji, H. A single-molecule enzymatic assay in a directly accessible femtoliter droplet array. Lab Chip 2010, 10, 3355–3362. [Google Scholar] [CrossRef]
- Kim, S.H.; Iwai, S.; Araki, S.; Sakakihara, S.; Iino, R.; Noji, H. Large-scale femtoliter droplet array for digital counting of single biomolecules. Lab Chip 2012, 12, 4986–4991. [Google Scholar] [CrossRef]
- O’Connell, G.C.; Alder, M.L.; Smothers, C.G.; Still, C.H.; Webel, A.R.; Moore, S.M. Use of high-sensitivity digital ELISA improves the diagnostic performance of circulating brain-specific proteins for detection of traumatic brain injury during triage. Neurol. Res. 2020, 42, 346–353. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Simoa SARS-CoV-2 N Protein Antigen Test; U.S Food and Drug Administration: Silver Spring, MD, USA, 2021. [Google Scholar]
- Ogata, A.F.; Maley, A.M.; Wu, C.; Gilboa, T.; Norman, M.; Lazarovits, R.; Mao, C.P.; Newton, G.; Chang, M.; Nguyen, K.; et al. Ultra-Sensitive Serial Profiling of SARS-CoV-2 Antigens and Antibodies in Plasma to Understand Disease Progression in COVID-19 Patients with Severe Disease. Clin. Chem. 2020, 66, 1562–1572. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.H.; Rissin, D.M.; Kan, C.W.; Fournier, D.R.; Piech, T.; Campbell, T.G.; Meyer, R.E.; Fishburn, M.W.; Cabrera, C.; Patel, P.P.; et al. The Simoa HD-1 Analyzer: A Novel Fully Automated Digital Immunoassay Analyzer with Single-Molecule Sensitivity and Multiplexing. J. Lab. Autom. 2016, 21, 533–547. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Interim Guidance for Antigen Testing for SARS-CoV-2; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Mak, G.C.; Lau, S.S.; Wong, K.K.; Chow, N.L.; Lau, C.S.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Analytical sensitivity and clinical sensitivity of the three rapid antigen detection kits for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 133, 104684. [Google Scholar] [CrossRef]
- Osterman, A.; Baldauf, H.M.; Eletreby, M.; Wettengel, J.M.; Afridi, S.Q.; Fuchs, T.; Holzmann, E.; Maier, A.; Döring, J.; Grzimek-Koschewa, N.; et al. Evaluation of two rapid antigen tests to detect SARS-CoV-2 in a hospital setting. Med. Microbiol. Immunol. 2021, 210, 65–72. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Flamholz, A.; Phillips, R.; Milo, R. SARS-CoV-2 (COVID-19) by the numbers. eLife 2020, 2, 9. [Google Scholar] [CrossRef]
- Dutta, N.K.; Mazumdar, K.; Gordy, J.T. The Nucleocapsid Protein of SARS-CoV-2: A Target for Vaccine Development. J. Virol. 2020, 94, e00647-20. [Google Scholar] [CrossRef]
- Obata, K.; Segawa, O.; Yakabe, M.; Ishida, Y.; Kuroita, T.; Ikeda, K.; Kawakami, B.; Kawamura, Y.; Yohda, M.; Matsunaga, T.; et al. Development of a novel method for operating magnetic particles, Magtration Technology, and its use for automating nucleic acid purification. J. Biosci. Bioeng. 2001, 91, 500–503. [Google Scholar] [CrossRef]
- Yamaoka, Y.; Miyakawa, K.; Jeremiah, S.S.; Funabashi, R.; Okudela, K.; Kikuchi, S.; Katada, J.; Wada, A.; Takei, T.; Nishi, M.; et al. Highly specific monoclonal antibodies and epitope identification against SARS-CoV-2 nucleocapsid protein for antigen detection tests. Cell Rep. Med. 2021, 2, 100311. [Google Scholar] [CrossRef]
- Sato, E.; Chiba, K.; Hoshi, M.; Kanaoka, Y. Pyranine Phosphate as a New Fluorogenic Substrate for Acidic and Alkaline Phosphatases. Chem. Pharm. Bull. 1992, 40, 786–788. [Google Scholar] [CrossRef] [Green Version]
- Noji, H.; Yamauchi, L. Method for Sealing Substances, Method for Detecting Target Molecule, Array, Kit, and Target Molecule Detection Device. U.S. Patent US2015008 7547A1, 2015.
- Ikeda, T.; Abbott Japan LLC. Optical Imaging System Using Lateral Illumination for Digital Assays. European Patent PCT/JP2017/045823, 20 December 2017. [Google Scholar]
- Vijigen, L.; Keyaerts, E.; Moes, E.; Maes, P.; Duson, G.; Ranst, M.V. Development of One-Step, Real-Time, Quantitative Reverse Transcriptase PCR Assays for Absolute Quantitation of Human Coronaviruses OC43 and 229E. J. Clin. Microbiol. 2005, 43, 5452–5456. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, C.; Yamayoshi, S.; Akimoto, M.; Nakamura, K.; Miura, H.; Fujisaki, S.; Pattinson, D.J.; Shimizu, K.; Ozawa, H.; Momoki, T.; et al. Genetic and antigenic characterisation of influenza A(H3N2) viruses isolated in Yokohama during the 2016/17 and 2017/18 influenza seasons. Eurosurveillance 2019, 24, 1800467. [Google Scholar] [CrossRef] [PubMed]
- Kan, C.W.; Rivnak, A.J.; Campbell, T.G.; Piech, T.; Rissin, D.M.; Mosl, M.; Peterça, A.; Niederberger, H.P.; Minnehan, K.A.; Patel, P.P.; et al. Isolation and detection of single molecules on paramagnetic beads using sequential fluid flows in microfabricated polymer array assemblies. Lab Chip 2012, 12, 977–985. [Google Scholar] [CrossRef]
- Sule, W.F.; Oluwayelu, D.O. Real-time RT-PCR for COVID-19 diagnosis: Challenges and prospects. Pan Afr. Med. J. 2020, 35 (Suppl. S2), 121. [Google Scholar] [CrossRef]
- Hirotsu, Y.; Maejima, M.; Shibusawa, M.; Amemiya, K.; Nagakubo, Y.; Hosaka, K.; Sueki, H.; Hayakawa, M.; Mochizuki, H.; Tsutsui, T.; et al. Prospective study of 1308 nasopharyngeal swabs from 1033 patients using the LUMIPULSE SARS-CoV-2 antigen test: Comparison with RT-qPCR. Int. J. Infect. Dis. 2021, 105, 7–14. [Google Scholar] [CrossRef]
- Ascoli, C.A. Could mutations of SARS-CoV-2 suppress diagnostic detection? Nat. Biotechnol. 2021, 39, 274–275. [Google Scholar] [CrossRef]
- Futase, A.; Abbott Japan LLC. Method for Reducing Noise in a Signal-Generating Digital Assays. U.S. Patent 11,047,854, 6 February 2021. [Google Scholar]
- Rissin, D.M.; Fournier, D.R.; Piech, T.; Kan, C.W.; Campbell, T.G.; Song, L.; Chang, L.; Rivnak, A.J.; Patel, P.P.; Provuncher, G.K.; et al. Simultaneous Detection of Single Molecules and Singulated Ensembles of Molecules Enables Immunoassays with Broad Dynamic Range. Anal. Chem. 2011, 83, 2279–2285. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PCR Ct | PPA with RT-PCR |
|---|---|
| <35 | 94.3% (83/88) |
| <30 | 100.0% (58/58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiba, R.; Miyakawa, K.; Aoki, K.; Morikawa, T.J.; Moriizumi, Y.; Degawa, T.; Arai, Y.; Segawa, O.; Tanaka, K.; Tajima, H.; et al. Development of a Fully Automated Desktop Analyzer and Ultrahigh Sensitivity Digital Immunoassay for SARS-CoV-2 Nucleocapsid Antigen Detection. Biomedicines 2022, 10, 2291. https://doi.org/10.3390/biomedicines10092291
Chiba R, Miyakawa K, Aoki K, Morikawa TJ, Moriizumi Y, Degawa T, Arai Y, Segawa O, Tanaka K, Tajima H, et al. Development of a Fully Automated Desktop Analyzer and Ultrahigh Sensitivity Digital Immunoassay for SARS-CoV-2 Nucleocapsid Antigen Detection. Biomedicines. 2022; 10(9):2291. https://doi.org/10.3390/biomedicines10092291
Chicago/Turabian StyleChiba, Ryotaro, Kei Miyakawa, Kotaro Aoki, Takamitsu J. Morikawa, Yoshiki Moriizumi, Takuma Degawa, Yoshiyuki Arai, Osamu Segawa, Kengo Tanaka, Hideji Tajima, and et al. 2022. "Development of a Fully Automated Desktop Analyzer and Ultrahigh Sensitivity Digital Immunoassay for SARS-CoV-2 Nucleocapsid Antigen Detection" Biomedicines 10, no. 9: 2291. https://doi.org/10.3390/biomedicines10092291