
Confidence in a Vaccine against COVID-19 among Registered Nurses in Barcelona, Spain across Two Time Periods

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Questionnaire and Data Collection
2.3. Variables
2.4. Data Analysis
3. Results
3.1. General Results
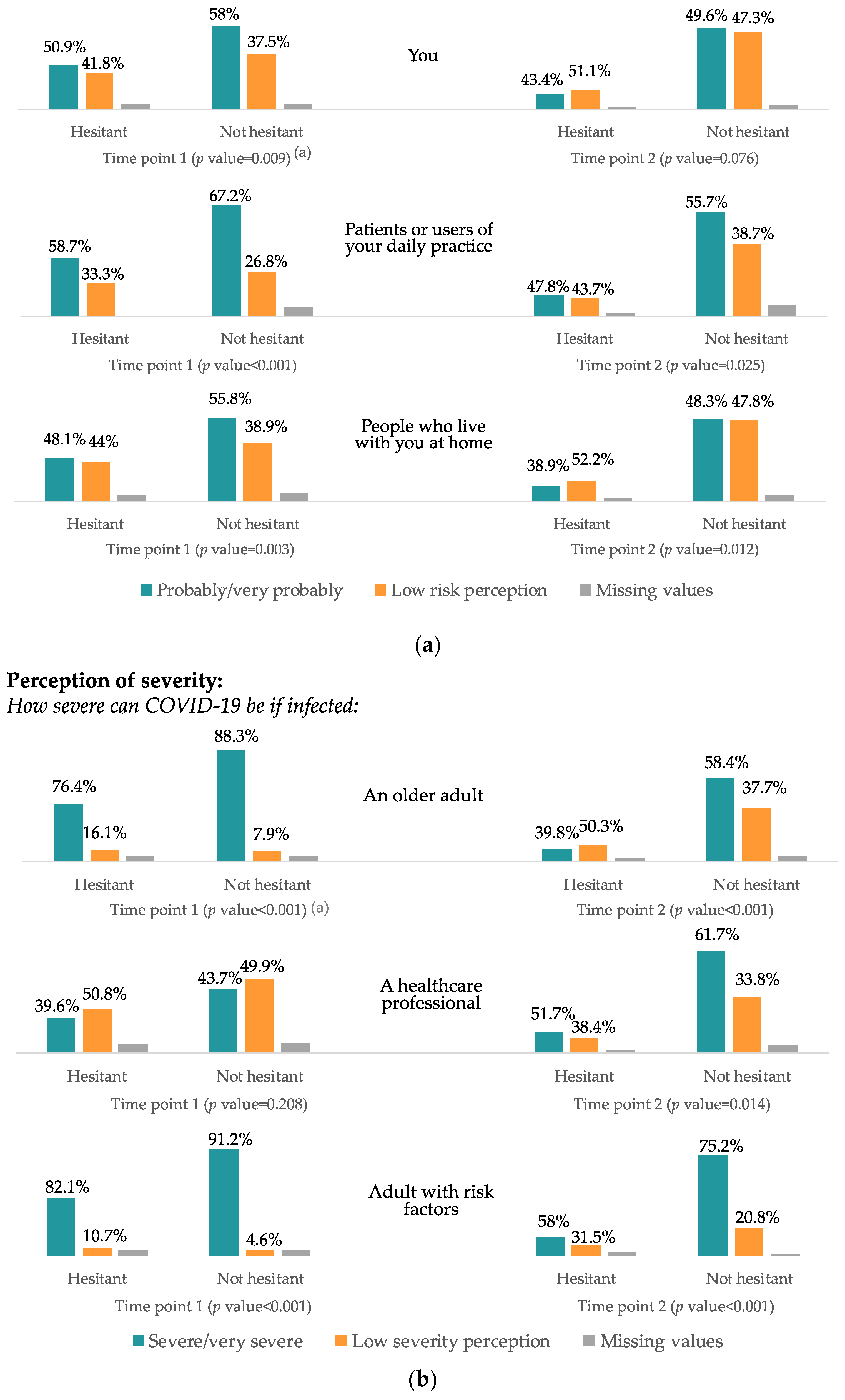
3.2. Risk Perception of the Disease
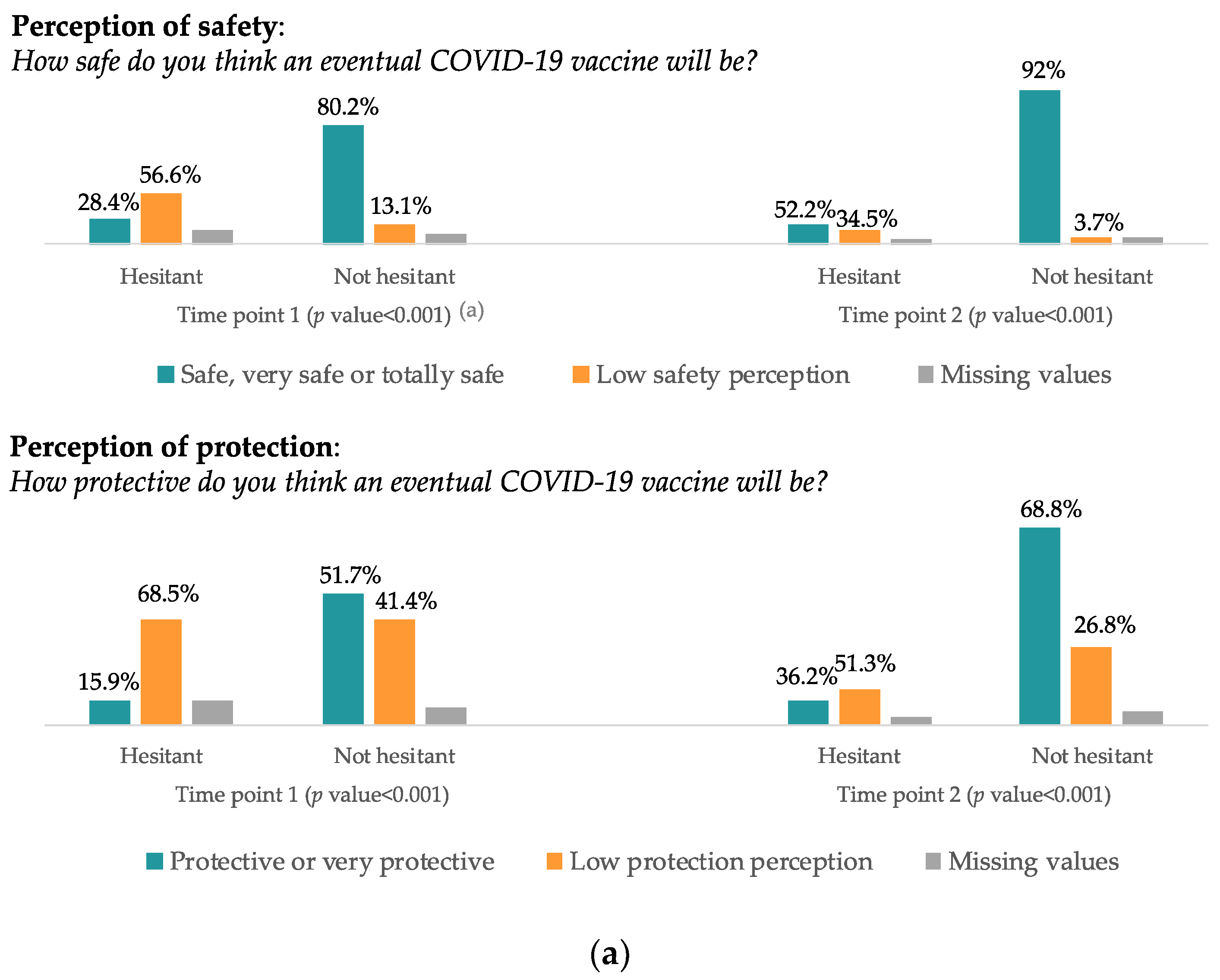
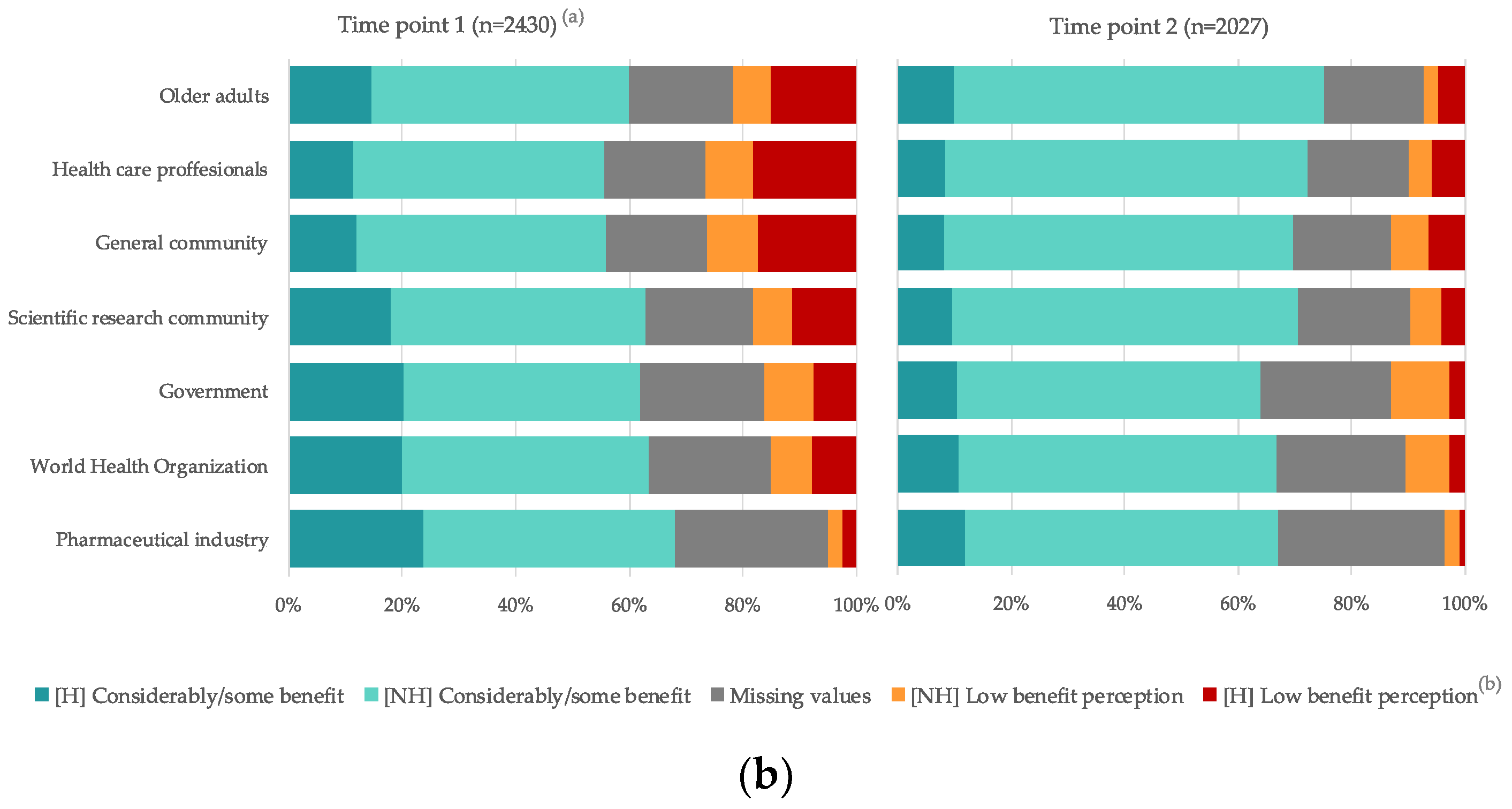
3.3. Perception of Vaccine Benefit
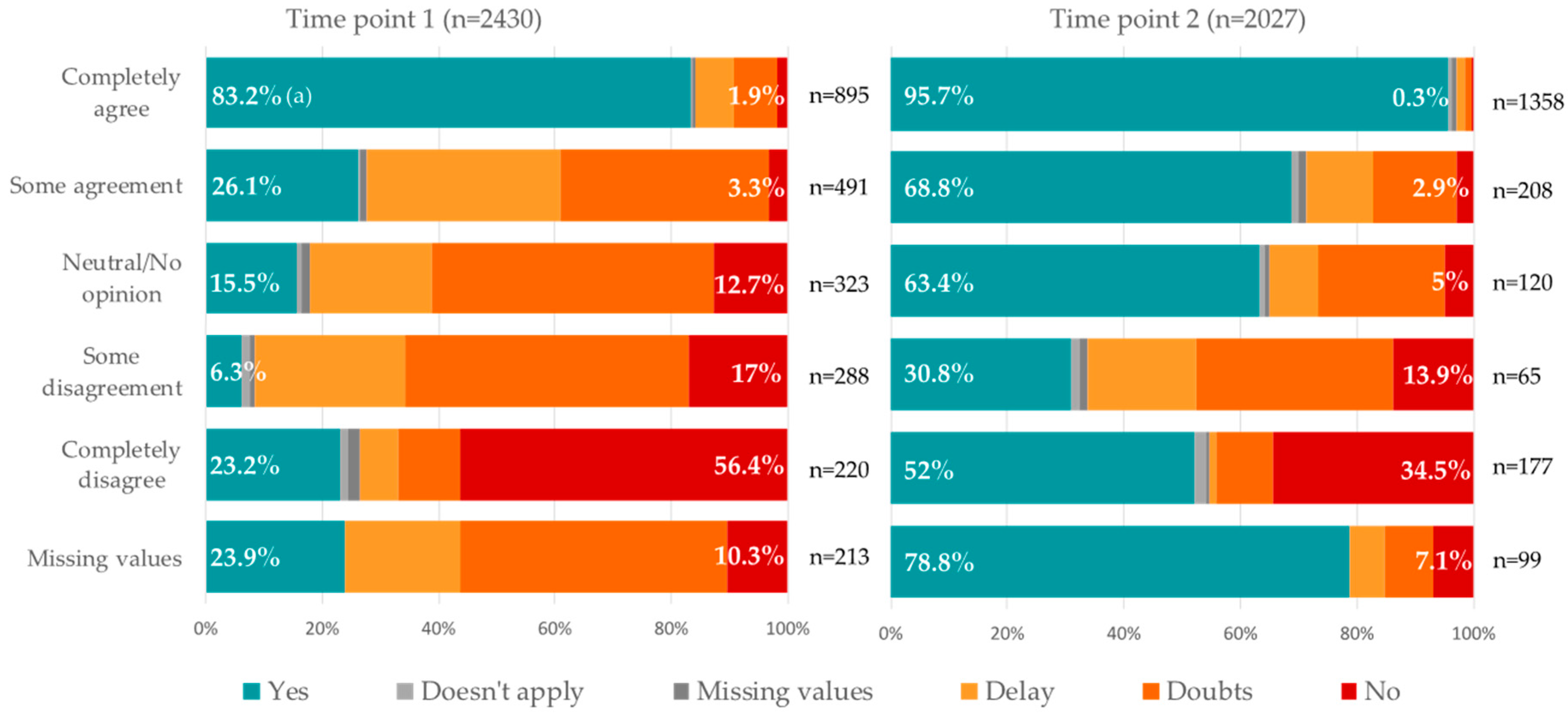
3.4. Attitudes, Beliefs and Social Norm Related to Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/feature-stories/ten-threats-to-global-health-in-2019 (accessed on 20 April 2022).
- Dubé, E.; E MacDonald, N. How can a global pandemic affect vaccine hesitancy? Expert Rev. Vaccines 2020, 19, 899–901. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- SAGE Working Group Dealing with Vaccine Hesitancy. Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 30 November 2020).
- Verger, P.; Dubé, E. Restoring confidence in vaccines in the COVID-19 era. Expert Rev. Vaccines 2020, 19, 991–993. [Google Scholar] [CrossRef] [PubMed]
- Picchio, C.A.; Carrasco, M.G.; Sagué-Vilavella, M.; Rius, C. Knowledge, attitudes and beliefs about vaccination in primary healthcare workers involved in the administration of systematic childhood vaccines, Barcelona, 2016/17. Eurosurveillance 2019, 24, 1800117. [Google Scholar] [CrossRef] [Green Version]
- Nowak, S.A.; Gidengil, C.A.; Parker, A.M.; Matthews, L.J. Association among trust in health care providers, friends, and family, and vaccine hesitancy. Vaccine 2021, 39, 5737–5740. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y. Multilevel determinants of COVID-19 vaccination hesitancy in the United States: A rapid systematic review. Prev. Med. Rep. 2021, 25, 101673. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Truong, J.; Bakshi, S.; Wasim, A.; Ahmad, M.; Majid, U. What factors promote vaccine hesitancy or acceptance during pandemics? A systematic review and thematic analysis. Health Promot. Int. 2022, 37, daab105. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Nehal, K.R.; Steendam, L.M.; Ponce, M.C.; van der Hoeven, M.; Smit, G.S.A. Worldwide Vaccination Willingness for COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1071. [Google Scholar] [CrossRef]
- Salomoni, M.G.; Di Valerio, Z.; Gabrielli, E.; Montalti, M.; Tedesco, D.; Guaraldi, F.; Gori, D. Hesitant or Not Hesitant? A Systematic Review on Global COVID-19 Vaccine Acceptance in Different Populations. Vaccines 2021, 9, 873. [Google Scholar] [CrossRef] [PubMed]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. eClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef] [PubMed]
- Yasmin, F.; Najeeb, H.; Moeed, A.; Naeem, U.; Asghar, M.S.; Chughtai, N.U.; Yousaf, Z.; Seboka, B.T.; Ullah, I.; Lin, C.-Y.; et al. COVID-19 Vaccine Hesitancy in the United States: A Systematic Review. Front. Public Health 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.; De Figueiredo, A.; Karafllakis, E.; Rawal, M. State of vaccine confidence in the European Union in 2018. Eur. J. Public Health 2019, 29. [Google Scholar] [CrossRef]
- Rosenthal, S.; Cummings, C.L. Influence of rapid COVID-19 vaccine development on vaccine hesitancy. Vaccine 2021, 39, 7625–7632. [Google Scholar] [CrossRef]
- Gestión Integral de la Vacunación’ GIV COVID-19, Report of activity presented in 26 August 2021. Available online: https://www.vacunacovid.gob.es/ (accessed on 20 April 2022).
- Generalitat de Cataluña, Instituto de Estadísticas de Cataluña IDESCAT. 2020. Available online: https://www.idescat.cat/pub/?id=aec&n=834&lang=es (accessed on 20 April 2022).
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2021, 31, 62–86. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare workers’ (HCWs) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021. [Google Scholar] [CrossRef]
- Park, J.Y.; Ha, J. Factors Influencing the COVID-19 Vaccination Intentions in Nurses: Korea, 21. J. Korean Acad. Nurs. 2021, 51, 537–548. [Google Scholar] [CrossRef]
- Bauernfeind, S.; Hitzenbichler, F.; Huppertz, G.; Zeman, F.; Koller, M.; Schmidt, B.; Plentz, A.; Bauswein, M.; Mohr, A.; Salzberger, B. Brief report: Attitudes towards COVID-19 vaccination among hospital employees in a tertiary care university hospital in Germany in December 2020. Infection 2021, 49, 1307–1311. [Google Scholar] [CrossRef]
- Lundberg, A.L.; Lorenzo-Redondo, R.; A Ozer, E.; A Hawkins, C.; Hultquist, J.F.; Welch, S.B.; Prasad, P.V.; Oehmke, J.F.; Achenbach, C.J.; Murphy, R.L.; et al. Has Omicron Changed the Evolution of the Pandemic? JMIR Public Health Surveill. 2022, 8, e35763. [Google Scholar] [CrossRef] [PubMed]
- Noushad, M.; Rastam, S.; Nassani, M.Z.; Al-Saqqaf, I.S.; Hussain, M.; Yaroko, A.A.; Arshad, M.; Kirfi, A.M.; Koppolu, P.; Niazi, F.H.; et al. A Global Survey of COVID-19 Vaccine Acceptance Among Healthcare Workers. Front. Public Health 2022, 9, 794673. [Google Scholar] [CrossRef] [PubMed]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the acceptance of COVID-19 vaccine among healthcare workers and general population using health belief model. J. Evaluation Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef] [PubMed]
- Peirolo, A.; Posfay-Barbe, K.M.; Rohner, D.; Wagner, N.; Blanchard-Rohner, G. Acceptability of COVID-19 Vaccine Among Hospital Employees in the Department of Paediatrics, Gynaecology and Obstetrics in the University Hospitals of Geneva, Switzerland. Front. Public Health 2022, 9, 781562. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Scronias, D. Changes in general practitioners’ attitudes toward COVID-19 vaccination after first interim results: A longitudinal approach in France. Hum. Vaccines Immunother. 2021, 17, 3408–3412. [Google Scholar] [CrossRef]
- Abuown, A.; Ellis, T.; Miller, J.; Davidson, R.; Kachwala, Q.; Medeiros, M.; Mejia, K.; Manoraj, S.; Sidhu, M.; Whittington, A.M.; et al. COVID-19 vaccination intent among London healthcare workers. Occup. Med. 2021, 71, 211–214. [Google Scholar] [CrossRef]
- Khamis, F.; Badahdah, A.; Al Mahyijari, N.; Al Lawati, F.; Al Noamani, J.; Al Salmi, I.; Al Bahrani, M. Attitudes Towards COVID-19 Vaccine: A Survey of Health Care Workers in Oman. J. Epidemiol. Glob. Health 2021, 12, 1–6. [Google Scholar] [CrossRef]
- Luk, T.T.; Zhao, S.; Wu, Y.; Wong, J.Y.-H.; Wang, M.P.; Lam, T.H. Prevalence and determinants of SARS-CoV-2 vaccine hesitancy in Hong Kong: A population-based survey. Vaccine 2021, 39, 3602–3607. [Google Scholar] [CrossRef]
- Mohammed, R.; Nguse, T.M.; Habte, B.M.; Fentie, A.M.; Gebretekle, G.B. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS ONE 2021, 16, e0261125. [Google Scholar] [CrossRef]
- Esen, B.K.; Can, G.; Pirdal, B.Z.; Aydin, S.N.; Ozdil, A.; Balkan, I.I.; Budak, B.; Keskindemirci, Y.; Karaali, R.; Saltoglu, N. COVID-19 Vaccine Hesitancy in Healthcare Personnel: A University Hospital Experience. Vaccines 2021, 9, 1343. [Google Scholar] [CrossRef]
- Zürcher, K.; Mugglin, C.; Egger, M.; Müller, S.; Fluri, M.; Bolick, L.; Jan Piso, R.; Hoffmann, M.; Fenner, L. Vaccination willingness for COVID-19 among healthcare workers: A cross-sectional survey in a Swiss canton. Swiss Med. Wkly. 2021, 151, w30061. [Google Scholar] [CrossRef]
- Chudasama, R.V.; Khunti, K.; Ekezie, W.C.; Pareek, M.; Zaccardi, F.; Gillies, C.L.; Seidu, S.; Davies, M.J.; Chudasama, Y.V. COVID-19 vaccine uptake and hesitancy opinions from frontline health care and social care workers: Survey data from 37 countries. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 16, 102361. [Google Scholar] [CrossRef]
- Baniak, L.; Luyster, F.; Raible, C.; McCray, E.; Strollo, P. COVID-19 Vaccine Hesitancy and Uptake among Nursing Staff during an Active Vaccine Rollout. Vaccines 2021, 9, 858. [Google Scholar] [CrossRef]
- Aurilio, M.T.; Mennini, F.; Gazzillo, S.; Massini, L.; Bolcato, M.; Feola, A.; Ferrari, C.; Coppeta, L. Intention to Be Vaccinated for COVID-19 among Italian Nurses during the Pandemic. Vaccines 2021, 9, 500. [Google Scholar] [CrossRef]
- Xin, M.; Luo, S.; She, R.; Chen, X.; Li, L.; Li, L.; Chen, X.; Lau, J.T.F. The Impact of Social Media Exposure and Interpersonal Discussion on Intention of COVID-19 Vaccination among Nurses. Vaccines 2021, 9, 1204. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Vásquez-Vera, H.; León-Gómez, B.B.; Borrell, C.; Jacques-Aviñó, C.; López, M.J.; Medina-Perucha, L.; Pasarin, M.; Sánchez-Ledesma, E.; Pérez, K. Inequities in the distribution of COVID-19: An adaptation of WHO’s conceptual framework. Gac. Sanit. 2021; in press. [Google Scholar] [CrossRef]
- Shakeel, C.S.; Mujeeb, A.A.; Mirza, M.S.; Chaudhry, B.; Khan, S.J. Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines 2022, 10, 110. [Google Scholar] [CrossRef]
- Paschoalotto, M.A.C.; Costa, E.P.P.A.; Almeida, S.V.; Cima, J.; Costa, J.G.D.; Santos, J.V.; Barros, P.P.; Passador, C.S.; Passador, J.L. Running away from the jab: Factors associated with COVID-19 vaccine hesitancy in Brazil. Rev. Saude Publica 2021, 55, 97, Erratum in Rev. Saude Publica 2022, 55, 120err. [Google Scholar] [CrossRef]
- Holzmann-Littig, C.; Braunisch, M.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef]
- Vignier, N.; Brureau, K.; Granier, S.; Breton, J.; Michaud, C.; Gaillet, M.; Agostini, C.; Ballet, M.; Nacher, M.; Valdes, A.; et al. Attitudes towards the COVID-19 Vaccine and Willingness to Get Vaccinated among Healthcare Workers in French Guiana: The Influence of Geographical Origin. Vaccines 2021, 9, 682. [Google Scholar] [CrossRef]
- Leung, C.L.K.; Li, K.-K.; Wei, V.W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S.; Kwok, K.O. Profiling vaccine believers and skeptics in nurses: A latent profile analysis. Int. J. Nurs. Stud. 2021, 126, 104142. [Google Scholar] [CrossRef] [PubMed]
- Patelarou, A.; Saliaj, A.; Galanis, P.; Pulomenaj, V.; Prifti, V.; Sopjani, I.; Mechili, E.A.; Laredo-Aguilera, J.A.; Kicaj, E.; Kalokairinou, A.; et al. Predictors of nurses’ intention to accept COVID-19 vaccination: A cross-sectional study in five European countries. J. Clin. Nurs. 2021, 31, 1258–1266. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef]
- Binagwaho, A.; Mathewos, K.; Davis, S. Time for the ethical management of COVID-19 vaccines. Lancet Glob. Health 2021, 9, e1169–e1171. [Google Scholar] [CrossRef]
- Belkebir, S.; Maraqa, B.; Nazzal, Z.; Abdullah, A.; Yasin, F.; Al-Shakhrah, K.; Zink, T. Exploring the Perceptions of Nurses on Receiving the SARS CoV-2 Vaccine in Palestine: A Qualitative Study. Can. J. Nurs. Res. 2021, 16, 8445621211066721. [Google Scholar] [CrossRef]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Point 1 XII 2020–II 2021 (n = 2430) a | Time Point 2 VI–VIII 2021 (n = 2027) a | p Value b | |||
|---|---|---|---|---|---|
| Variable | n | % | n | % | |
| Age (Median + IQR) | 43.4 | 42.8–44.0 | 45.5 | 44.8–46.1 | 0.0002 |
| Years of work (Median + IQR) | 18.2 | 17.7–18.7 | 20.2 | 20.2–21.4 | <0.001 |
| Gender | |||||
| Female | 1596 | 86.37% | 1381 | 86.37% | 0.192 |
| Male | 242 | 13.32% | 213 | 13.32% | |
| Other | 1 | 0.05% | 5 | 0.31% | |
| Type of practice | |||||
| Mainly public practice | 1666 | 69.47% | 887 | 68.71% | 0.236 |
| Mainly private practice | 413 | 17.22% | 248 | 19.21% | |
| Similar public and private practice | 319 | 13.30% | 156 | 12.08% | |
| Contact with COVID-19 patients | |||||
| Yes, COVID-19 patients as main task | 763 | 31.45% | 538 | 26.62% | 0.002 |
| Yes, but COVID-19(+) cases not as main task | 437 | 18.01% | 352 | 17.42% | |
| Yes, but COVID-19(+) cases are sporadic | 769 | 31.70% | 692 | 34.24% | |
| I have no contact with COVID-19(+) patients | 426 | 17.52% | 415 | 20.53% | |
| DN/NR | 32 | 1.32% | 24 | 1.19% | |
| Live with any dependents (minor under 14 years old, over 65 years old or sick people under care) | |||||
| Dependents | 844 | 34.73% | 739 | 36.46% | 0.231 |
| None of the above | 1586 | 65.27% | 1288 | 63.54% | |
| Has been infected with COVID-19 | |||||
| Yes | 508 | 21.18% | 368 | 18.26% | 0.015 |
| No | 1890 | 78.82% | 1647 | 81.74% | |
| Severity if have been infected with COVID-19 | |||||
| Mild | 186 | 39.08% | 120 | 33.52% | 0.440 |
| Moderate | 260 | 54.62% | 218 | 60.89% | |
| Severe | 29 | 6.09% | 19 | 5.31% | |
| Very severe | 1 | 0.21% | 1 | 0.28% | |
| Has been vaccinated against the flu this year | |||||
| Yes | 1216 | 59.84% | 835 | 62.45% | 0.129 |
| I haven’t/won’t be vaccinated | 816 | 40.16% | 502 | 37.55% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palma, D.; Hernández, A.; Picchio, C.A.; Jodar, G.; Galbany-Estragués, P.; Simón, P.; Guillaumes, M.; Diez, E.; Rius, C. Confidence in a Vaccine against COVID-19 among Registered Nurses in Barcelona, Spain across Two Time Periods. Vaccines 2022, 10, 873. https://doi.org/10.3390/vaccines10060873
Palma D, Hernández A, Picchio CA, Jodar G, Galbany-Estragués P, Simón P, Guillaumes M, Diez E, Rius C. Confidence in a Vaccine against COVID-19 among Registered Nurses in Barcelona, Spain across Two Time Periods. Vaccines. 2022; 10(6):873. https://doi.org/10.3390/vaccines10060873
Chicago/Turabian StylePalma, David, Anna Hernández, Camila A. Picchio, Glòria Jodar, Paola Galbany-Estragués, Pere Simón, Montserrat Guillaumes, Elia Diez, and Cristina Rius. 2022. "Confidence in a Vaccine against COVID-19 among Registered Nurses in Barcelona, Spain across Two Time Periods" Vaccines 10, no. 6: 873. https://doi.org/10.3390/vaccines10060873