
Tokophobia and Anxiety in Pregnant Women during the SARS-CoV-2 Pandemic in Poland—A Prospective Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Aim of the Study
- The assessment of the severity of tokophobia in the study group;
- The assessment of state and trait anxiety in the study group;
- The assessment of the influence of sociodemographic factors such as age, level of education, medical education, place of residence, location at which delivery took place, occupational activity and financial status on the severity of tokophobia and situational anxiety evaluated on the STAI scale;
- The assessment of correlations between the duration of the pandemic and the level of tokophobia and state anxiety.
2.2. Research Hypotheses
- The SARS-CoV-2 pandemic increases the level of anxiety in women in the 3rd trimester of pregnancy;
- Sociodemographic factors influence the level of tokophobia in pregnant women;
- The duration of the SARS-CoV-2 pandemic influences the level of tokophobia in women.
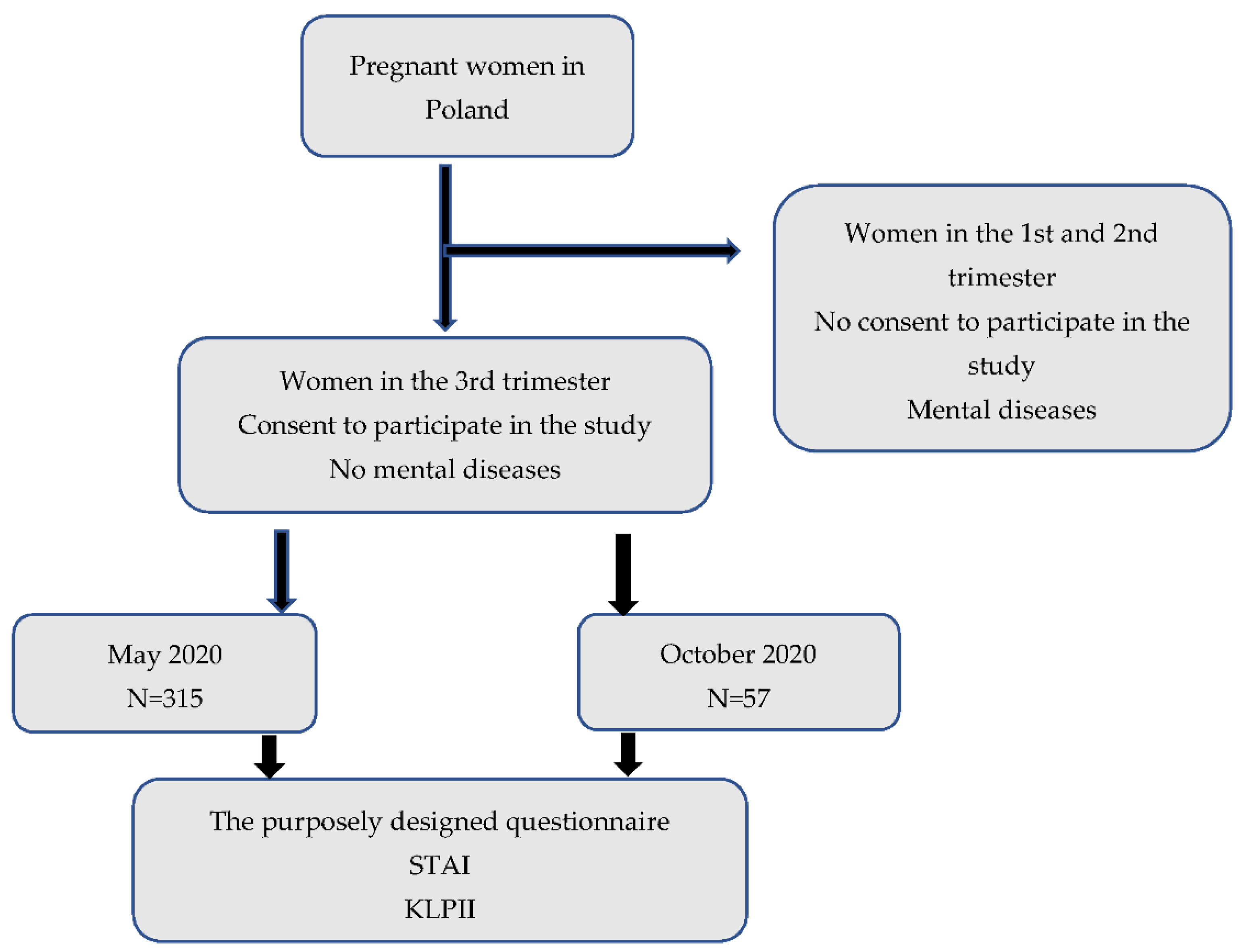
2.3. Material
- Consent to participate in the study;
- Women in the 3rd trimester of pregnancy (27–41 weeks of gestation);
- No psychiatric diseases.
- No consent to participate in the study;
- Women in the 1st and 2nd trimester of pregnancy;
- Women treated for psychiatric diseases.
2.4. Method
2.4.1. The Purposely Designed Questionnaire
2.4.2. Labor Anxiety Questionnaire (KLPII)
- From 14 to 15 points—elevated level of tokophobia;
- From 16 to 17 points—high level of tokophobia;
- From 18 to 27 points—very high level of tokophobia.
2.4.3. State-Trait Anxiety Inventory STAI
- From 1 to 3 sten scores—low state anxiety and trait anxiety;
- From 4 to 7 sten scores—moderate state anxiety and trait anxiety;
- From 8 to 10 sten scores—high state anxiety and trait anxiety.
2.5. Statistics
3. Results
3.1. Characteristics of the Group
3.2. Anxiety Assessment
3.2.1. Labor Anxiety Questionnaire (KLPII)
3.2.2. State-Trait Anxiety Inventory (STAI)
4. Discussion
4.1. Limitations of the Study
4.2. Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaźmierczak, M.; Gebuza, G.; Gierszewska, M. Zaburzenia Emocjonalne Okresu Poporodowego. Nurs. Probl. 2010, 18, 503–511. [Google Scholar]
- Bhatia, M.S.; Jhanjee, A. Tokophobia: A Dread of Pregnancy. Ind. Psychiatry J. 2012, 21, 158–159. [Google Scholar] [CrossRef]
- Billert, H. Tokophobia—A multidisciplinary problem. Ginekol. Pol. 2007, 78, 807–811. [Google Scholar] [PubMed]
- Kamasz, E.; Pilarska, N.; Włodarczyk, A. Znaczenie Traumatycznych Narracji Porodowych Oraz Oceny Opieki Ginekologicznej Jako Czynnika Rozwoju Tokofobii w Oczach Młodych Kobiet. Fides Et Ratio 2020, 3, 320–333. [Google Scholar]
- Coussons-Read, M.E. Effects of Prenatal Stress on Pregnancy and Human Development: Mechanisms and Pathways. Obstet. Med. 2013, 6, 52–57. [Google Scholar] [CrossRef] [Green Version]
- Makara-Studzińska, M.; Iwanowicz-Palus, G. Psychologia w Położnictwie i Ginekologii; PZWL: Warszawa, Poland, 2008; ISBN 978-83-200-3648-0. [Google Scholar]
- Kaźmierczak, M.; Sołdyńska, M.; Gierszewska, M.; Gebuza, G.; Mieczkowska, E. Ocena lęku przed porodem u kobiet ciężarnych. Piel. Zdr. Publ. 2017, 26, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Bjelica, A.; Kapor-Stanulović, N. Pregnancy as a psychological event. Med. Pregl. 2004, 57, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Soma-Pillay, P.; Nelson-Piercy, C.; Tolppanen, H.; Mebazaa, A. Physiological Changes in Pregnancy. Cardiovasc. J. Afr. 2016, 27, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, K.M.; Suthar, M.S. Comprehensive Analysis of COVID-19 during Pregnancy. Biochem. Biophys. Res. Commun. 2021, 538, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Studniczek, A.; Kossakowska, K. Ciąża i poród w czasach pandemii COVID-19: Wybrane aspekty psychologiczne. Fides Et Ratio 2020, 29, 274–284. [Google Scholar]
- Wojaczek, M. Kształtowanie się zmian i percepcja poczętego dziecka w poszczególnych etapach ciąży. Piel. Zdr. Publ. 2012, 2, 73–77. [Google Scholar]
- Schetter, C.D.; Tanner, L. Anxiety, Depression and Stress in Pregnancy: Implications for Mothers, Children, Research, and Practice. Curr. Opin. Psychiatry 2012, 25, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalesi, Z.B.; Bokaie, M. The Association between Pregnancy-Specific Anxiety and Preterm Birth: A Cohort Study. Afr. Health Sci. 2018, 18, 569–575. [Google Scholar] [CrossRef]
- Mielimąka, M.; Rutkowski, K.; Cyranka, K.; Sobański, J.; Müldner-Nieckowski, Ł.; Dembińska, E.; Smiatek-Mazgaj, B.; Klasa, K. Effectiveness of Intensive Group Psychotherapy in Treatment of Neurotic and Personality Disorders. Psychiatr. Pol. 2015, 49, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Maj, A. Zjawisko Lęku w Personalistycznej Perspektywie. RPed 2020, 12, 111–124. [Google Scholar] [CrossRef]
- Bhatia, P.; Chhabra, S. Physiological and Anatomical Changes of Pregnancy: Implications for Anaesthesia. Indian J. Anaesth 2018, 62, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Sokół-Szawłowska, M. Wpływ Kwarantanny Na Zdrowie Psychiczne Podczas Pandemii COVID-19. Psychiatria 2021, 18, 57–62. [Google Scholar] [CrossRef]
- Hwang, T.-J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and Social Isolation during the COVID-19 Pan-demic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef]
- Abu-Raya, B.; Michalski, C.; Sadarangani, M.; Lavoie, P.M. Maternal Immunological Adaptation During Normal Pregnancy. Front. Immunol. 2020, 11, 575197. [Google Scholar] [CrossRef] [PubMed]
- Zgliczyńska, M.; Kosińska-Kaczyńska, K. Przebieg Infekcji SARS-CoV-2 u Kobiet Ciężarnych—Przegląd Literatury. Wiedza Med. 2020, 24–30. [Google Scholar] [CrossRef]
- Fernández-Carrasco, F.J.; Vázquez-Lara, J.M.; González-Mey, U.; Gómez-Salgado, J.; Parrón-Carreño, T.; Rodríguez-Díaz, L. Coronavirus Covid-19 infection and breastfeeding: An exploratory review. Rev. Esp. Salud. Publica 2020, 94, e202005055. [Google Scholar] [PubMed]
- Shanbehzadeh, S.; Tavahomi, M.; Zanjari, N.; Ebrahimi-Takamjani, I.; Amiri-Arimi, S. Physical and Mental Health Compli-cations Post-COVID-19: Scoping Review. J. Psychosom. Res. 2021, 147, 110525. [Google Scholar] [CrossRef]
- Widiger, T.A.; Oltmanns, J.R. Neuroticism Is a Fundamental Domain of Personality with Enormous Public Health Implica-tions. World Psychiatry 2017, 16, 144–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mróz, J. Communication and Loneliness and Life Satisfaction during the Pandemi. Fides Et Ratio 2020, 42, 214–226. [Google Scholar] [CrossRef]
- Creinin, M.D.; Grossman, D.A.; Committee on Practice Bulletins. Medication Abortion Up to 70 Days of Gestation: ACOG Practice Bulletin, Number 225. Obstet. Gynecol. 2020, 136, e31–e47. [Google Scholar] [CrossRef]
- Ruengorn, C.; Awiphan, R.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S.; Health Outcomes and Mental Health Care Evaluation Survey Research Group (HOME-Survey). Association of Job Loss, Income Loss, and Financial Burden with Ad-verse Mental Health Outcomes during Coronavirus Disease 2019 Pandemic in Thailand: A Nationwide Cross-Sectional Study. Depress Anxiety 2021, 38, 648–660. [Google Scholar] [CrossRef] [PubMed]
- Robertson, E.; Grace, S.; Wallington, T.; Stewart, D.E. Antenatal Risk Factors for Postpartum Depression: A Synthesis of Recent Literature. Gen. Hosp. Psychiatry 2004, 26, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Paciorek, M.; Putyński, L. Kwestionariusz Lęku Porodowego (KLP II) Wersja Zrewidowana : Konstrukcja i właściwości psychometryczne. Acta Universitatis Lodziensis. Folia Psychol. 2008, 12, 129–133. Available online: https://bazhum.muzhp.pl/media/files/Acta_Universitatis_Lodziensis_Folia_Psychologica/Acta_Universitatis_Lodziensis_Folia_Psychologica-r2008-t12/Acta_Universitatis_Lodziensis_Folia_Psychologica-r2008-t12-s129-133/Acta_Universitatis_Lodziensis_Folia_Psychologica-r2008-t12-s129-133.pdf (accessed on 1 January 2022).
- Iwata, N.; Mishima, N.; Shimizu, T.; Mizoue, T.; Fukuhara, M.; Hidano, T.; Spielberg, C.D. The Japanese adaptation of the STAI Form Y in Japanese working adults—The presence or absence of anxiety. Ind. Health 1998, 36, 8–13. [Google Scholar] [CrossRef]
- Wojdyła, Z.; Żurawiecka, D.; Łuczak, I.; Zimnowoda, M. Zaburzenia Zdrowia Psychicznego u Kobiet w Okresie Ciąży, Porodu i Połogu. Wybrane Asp. Opieki Pielęgniarskiej I Położniczej W Różnych Spec. Med. 2019, 7, 197–205. [Google Scholar]
- Nakić Radoš, S. Anxiety During Pregnancy and Postpartum: Course, Predictors and Comorbidity with Postpartum Depres-sion. ACC 2018, 57, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.; Lee, S.; Shakespeare, J.; Ayers, S. Diagnosis and Management of Perinatal Depression and Anxiety in General Practice: A Meta-Synthesis of Qualitative Studies. Br. J. Gen. Pract. 2017, 67, e538–e546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuccia, A.; Caradonna, C. The Relationship between the Stomatognathic System and Body Posture. Clinics 2009, 64, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Data | N = Number of Subjects | % | |
|---|---|---|---|
| Marital status | Married Domestic partnership | 228 87 | 72.4% 27.6% |
| Education | Tertiary Secondary Vocational Primary | 184 109 17 5 | 58.4% 34.6% 5.4% 1.6% |
| Place of residence | Village Town <10,000 inhabit. Big town >10,000<100,000 inhabit. City >100,000 inhabit. City >500,000 inhabit. | 94 28 80 57 56 | 29.8% 8.9% 25.4% 18.1% 17.8% |
| Financial status of the family | Very good Good Average Poor | 43 180 88 2 | 13.8% 57.1% 27.9% 0.6% |
| Professional activity | Yes No | 107 208 | 34.0% 66% |
| Data | N = Number of Subjects | % | |
|---|---|---|---|
| Number of children | 0 1 2 3 | 215 64 31 5 | 68.2% 20.3% 9.8% 1.6% |
| History of miscarriage | Yes No | 55 260 | 17.2% 82.5% |
| Present pregnancy risks | Yes No | 21 295 | 6.7% 93.7% |
| Regular gynecological appointments during pregnancy | Yes No | 301 14 | 95.6% 4.4% |
| Levels of Tokophobia | n | % | Chi2 | p-Value |
|---|---|---|---|---|
| Low and moderate level of tokophobia | 50 | 15.9% | 19.387 | <0.001 * |
| Elevated level of tokophobia | 78 | 24.8% | ||
| High level of tokophobia | 105 | 33.3% | ||
| Very high level of tokophobia | 82 | 26.0% |
| The Level of State Anxiety | n | % | Chi2 | p-Value |
|---|---|---|---|---|
| Low levels of state anxiety | 34 | 10.8% | 82.533 | <0.001 * |
| Moderate levels of state anxiety | 117 | 37.1% | ||
| High levels of state anxiety | 164 | 52.1% |
| Variable | Level of Tokophobia | Mean | F Test | p-Value |
|---|---|---|---|---|
| Age | Low and moderate level of tokophobia | 29 | 2.952 | 0.033 * |
| Elevated level of tokophobia | 29 | |||
| High level of tokophobia | 27 | |||
| Very high level of tokophobia | 27 |
| Financial Status | Low | Moderate | High | Chi2 | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Very good | 13 | 38.2% | 13 | 11.2% | 17 | 10.4% | 26.755 | <0.001 * |
| Good | 17 | 50.0% | 74 | 63.2% | 89 | 54.3% | ||
| Average | 4 | 11.8% | 30 | 25.6% | 54 | 32.9% | ||
| Poor | 0 | 0.0% | 0 | 0.0% | 2 | 1.2% | ||
| Very poor | 0 | 0.0% | 0 | 0.0% | 2 | 1.2% | ||
| Level of Tokophobia | May | October | Chi2 | p-Value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Low and moderate levels of tokophobia | 46 | 17.8% | 4 | 7.0% | 8.286 | 0.04 * |
| Elevated levels of tokophobia | 58 | 22.5% | 20 | 35.1% | ||
| High levels of tokophobia | 90 | 34.9% | 15 | 26.3% | ||
| Very high levels of tokophobia | 64 | 24.8% | 18 | 31.6% | ||
| SITUATIONAL Anxiety | May | October | Chi2 | p-Value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Low anxiety | 29 | 11.2% | 5 | 8.8% | 18.709 | <0.001 * |
| Moderate anxiety | 109 | 42.2% | 8 | 14.0% | ||
| High anxiety | 120 | 46.5% | 44 | 77.2% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makara-Studzińska, M.; Zaręba, K.; Kawa, N.; Matuszyk, D. Tokophobia and Anxiety in Pregnant Women during the SARS-CoV-2 Pandemic in Poland—A Prospective Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 714. https://doi.org/10.3390/ijerph19020714
Makara-Studzińska M, Zaręba K, Kawa N, Matuszyk D. Tokophobia and Anxiety in Pregnant Women during the SARS-CoV-2 Pandemic in Poland—A Prospective Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(2):714. https://doi.org/10.3390/ijerph19020714
Chicago/Turabian StyleMakara-Studzińska, Marta, Kornelia Zaręba, Natalia Kawa, and Dorota Matuszyk. 2022. "Tokophobia and Anxiety in Pregnant Women during the SARS-CoV-2 Pandemic in Poland—A Prospective Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 2: 714. https://doi.org/10.3390/ijerph19020714