
Can Self-Administered Rapid Antigen Tests (RATs) Help Rural India? An Evaluation of the CoviSelf Kit as a Response to the 2019–2022 COVID-19 Pandemic


Abstract
:1. Introduction
With CoviSelfTM, Mylab aims to make testing reach the doorstep of every Indian to help them fight the second and any subsequent waves of [sic] pandemic. Now, any citizen can test for Covid-19 themselves, isolate and seek treatment quickly. Early detection can help save thousands of lives and significantly reduce [sic] burden on hospitals. The test can be purchased without a prescription from local pharmacies and online channel partners [italics added by authors of this article]
2. RATs in Clinical Settings in India
The Urgent Need for Self-Administered RATs in Villages
3. Materials and Methods
3.1. Qualitative Framework
3.2. Our Main Data Source
3.3. Contextualising Our Main Data Source
3.4. Our Second and Third Data Sources
3.5. The Limitations of This Study
4. Results
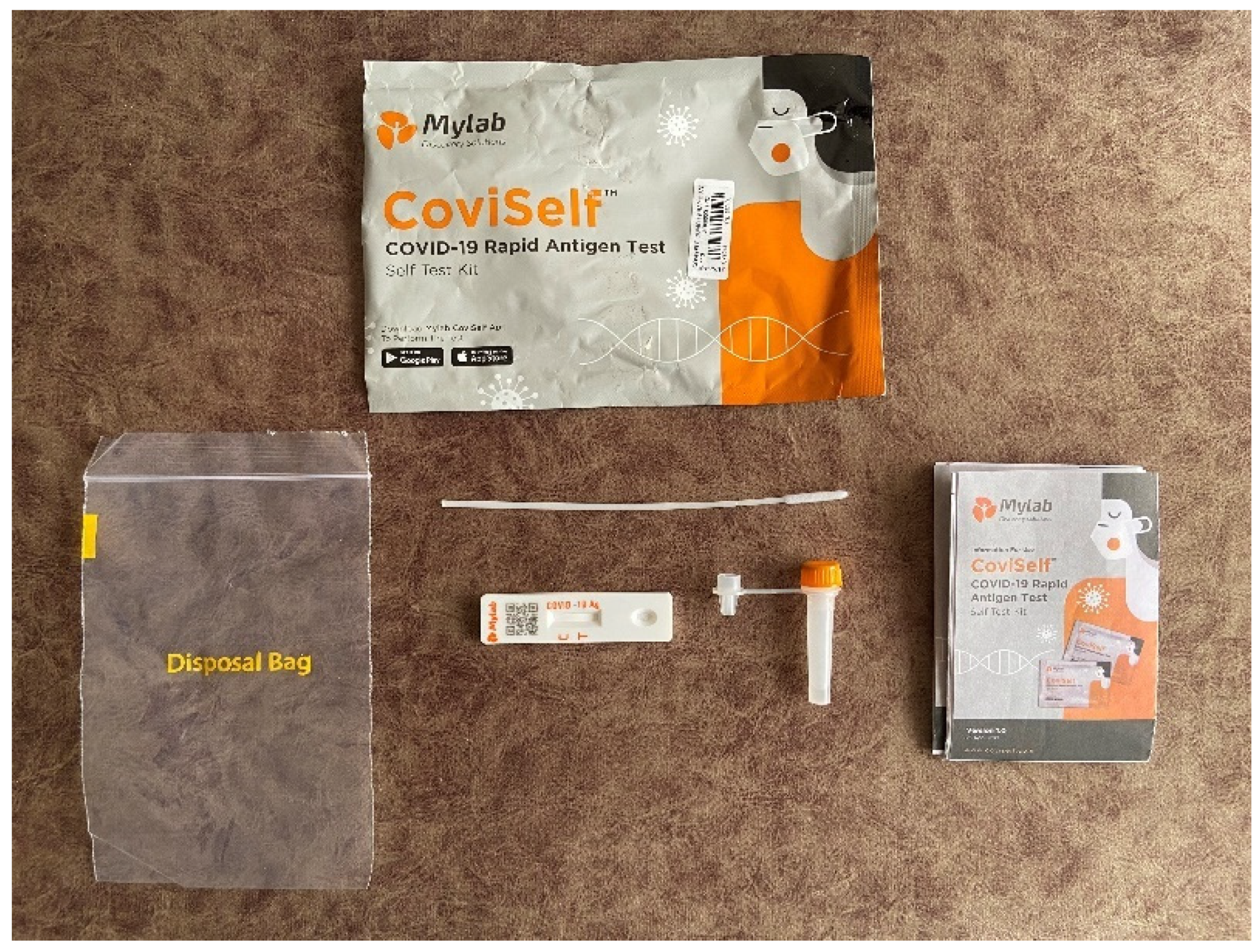
4.1. The CoviSelf Instruction Leaflet
4.1.1. The Structure of the Instruction Leaflet
4.1.2. The Ease of Using the Kit (the Relevant Headings in the Instruction Leaflet Are Steps 1, 2 and 3)
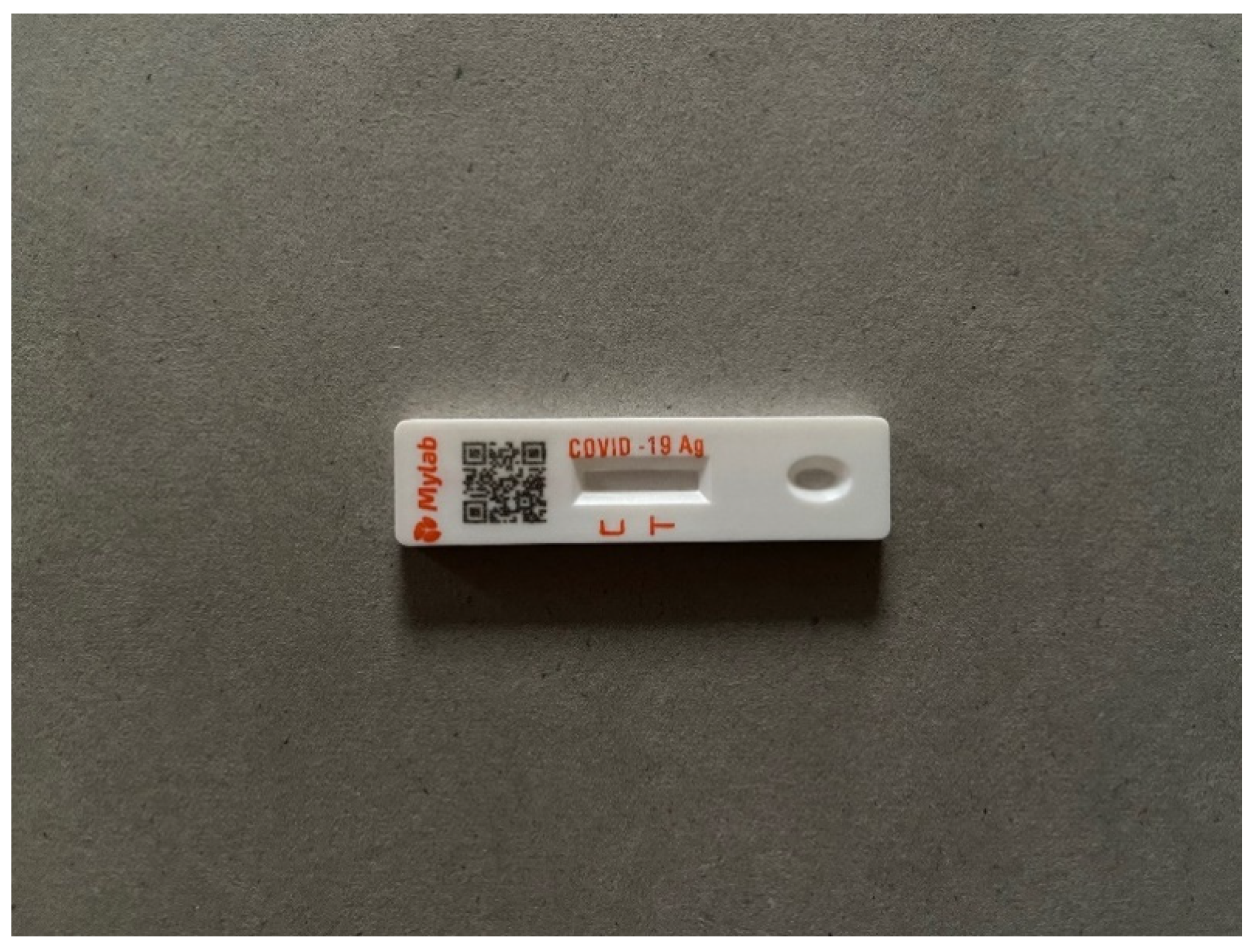
4.1.3. Reading the Test Result and the Clarity of the Leaflet’s Language (the Relevant Headings in the Instruction Leaflet Are Positive Result, Negative Result and Invalid)
4.1.4. How to Respond to the Test Results (the Relevant Headings in the Instruction Leaflet Are Positive Result and Negative Result)
4.1.5. The Test Results and the Objectives of the ICMR (the Relevant Section in the Instruction Leaflet Is Step 4)
ICMR is the regulatory body in India which is responsible for the curb of COVID-19 pandemic along with other important regulatory bodies. Reporting the results helps the body and authorities curb the spread of the disease. It thus becomes our moral obligation to help ICMR by reporting our test result data.
4.2. India’s Digital Divide
4.2.1. The Indian Press
4.2.2. The Internet and Mobile Association of India (IAMAI) Report of 2021
4.2.3. Civil Society and the Supreme Court of India
4.3. The Conditions of Life in Rural India
4.3.1. Village Poverty and Employment
4.3.2. Village Health and Diagnostic Medical Interventions
4.3.3. Village Religion and Modern Medicine
He had good health but he brought it upon himself by drinking too much. How is our deity responsible for that? [43].
5. Discussion
6. Conclusions
I had to take three tests and the result is still inconclusive, what is the problem. The 1st test …I couldn’t squiz [sic] the liquid onto sample level and I broke the well bottom and the lines so I exited the App. But then I tried the second time and did everything right and found that results were inconclusive as I scanned later than 20 min… I tried third time and exactly waited for 15mins and it’s the same problem.
I followed all instructions yet I didn’t receive my results. Just said Invalid Casette, low server problem. Second, I understand that there might be server issue, then what’s the point of keeping another 15 min time interval when the whole kit gets invalid after 20 min. Just keep the test result appearance that’s it. Really disappointed. The manual rtpcrs are far safe and better I suppose.
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Madaan, N. ‘Self-Test Kits’ Sales Soar in Maharashtra, Health Officials Concerned over Cases Going Unreported. Times of India. 9 January 2022. Available online: https://timesofindia.indiatimes.com/city/pune/self-test-kits-sales-soar-health-officials-concerned-over-cases-going-unreported/articleshow/88783693.cms (accessed on 9 January 2022).
- Pillai, V. ICMR Says Self Rapid Antigen Test Will Be Considered Confirmatory. The Economic Times. 10 January 2022. Available online: https://economictimes.indiatimes.com/news/india/icmr-says-self-rapid-antigen-test-will-be-considered-confirmatory/articleshow/88815890.cms (accessed on 12 February 2022).
- CoviSelf by Mylab. Mylab Receives ICMR Approval for India’s First Self-Use COVID-19 Test, Resources, 10 May 2021 Press Release. Available online: https://coviself.com/img/CoviSelf-Press-Release.pdf (accessed on 11 February 2022).
- Indian Council of Medical Research (ICMR). ‘About ICMR’, Ministry of Health, Government of India Portal: Delhi, India. Available online: https://www.icmr.gov.in/aboutus.html (accessed on 28 October 2021).
- MyLab Discovery Solutions Pvt Ltd. (Maharashtra) Is a Biotechnology Company that Specialises in, amongst Other Things, Molecular Diagnostic Technology under the 98/79/EC Full Quality Assurance Systems ISO 9001, ISO 13485: ‘Welcome to Mylab’. Available online: https://mylabdiscoverysolutions.com/who-we-are/ (accessed on 28 October 2021).
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2021. [Google Scholar] [CrossRef]
- ICMR. COVID-19 Home Testing Using Rapid Antigen Tests (RATs); Ministry of Health, Government of India: Delhi, India, 2022. Available online: https://www.icmr.gov.in/pdf/covid/kits/COVID_Home_Test_Kit_13012022.pdf (accessed on 11 February 2022).
- Khalid, M.F.; Selvam, K.; Jeffry, A.J.N.; Salmi, M.F.; Najib, M.A.; Norhayati, M.N.; Aziah, I. Performance of Rapid Antigen Tests for COVID-19 Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Table for Rural Population (% of Total Population): All Countries and Economies: India 2019. Available online: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS (accessed on 25 April 2021).
- Roy, A. New Covid Pill Will Be Useful for Anti-Vaxxers. Eastern Eye. 27 October 2021. Available online: https://www.easterneye.biz/new-covid-pill-will-be-useful-for-anti-vaxxers/ (accessed on 28 October 2021).
- Rawlins, M. Harveian oration: De testimonio: On the evidence for decisions about the use of therapeutic interventions. Lancet 2009, 372, 2152–2161. Available online: https://www.proquest.com/scholarly-journals/harveian-oration-de-testimonio-on-evidence/docview/199025050/se-2?accountid=12528 (accessed on 29 December 2021). [CrossRef]
- Bourgeault, I.L.; De Vries, R.; Dingwall, R. (Eds.) Introduction. In The SAGE Handbook of Qualitative Methods in Health Research; SAGE Publications: Los Angeles, CA, USA, 2010; pp. 1–16. [Google Scholar]
- Gee, J.P.; Handford, M. (Eds.) The Routledge Handbook of Discourse Analysis; Routledge: London, UK, 2013. [Google Scholar] [CrossRef]
- Sarangi, S. Practising Discourse Analysis in Healthcare Settings. In The SAGE Handbook of Qualitative Methods in Health Research; SAGE Publications: Los Angeles, CA, USA, 2010; pp. 397–416. [Google Scholar]
- Anonymous; (Engineering Faculty, Monash University, Melbourne, Australia). Personal communication, 13 August 2009.
- Cherian, P.; Krishna, S.; Menon, G.I. Optimizing testing for COVID-19 in India. PLoS Comput. Biol. 2021, 17, e1009126. [Google Scholar] [CrossRef]
- Hada, V.; Rath, R.S.; Mohanty, A.; Sahai, R.; Kumar, K.; Kumar, S.; Joshi, H.S.; Kishore, S. Comparison of Positivity Rates of Rapid Antigen Testing and Real-Time Polymerase Chain Reaction for COVID-19 During the First and Second Waves of the Pandemic in Eastern Uttar Pradesh, India. Cureus 2021, 13, e16206. [Google Scholar] [CrossRef]
- Special Correspondent. SBI Report Emphasises on Vaccination, Says Nearly Half of the New Cases in Rural India. The Hindu. 7 May 2021. Available online: https://www.thehindu.com/news/national/sbi-report-emphasises-on-vaccination-says-nearly-half-of-the-new-cases-in-rural-india/article34506912.ece (accessed on 24 January 2022).
- Kaunain Sheriff, M. O2 Beds in Villages, Push to Testing: Centre Draws up 3-tier Response Plan. Indian Express. 17 May 2021. Available online: https://indianexpress.com/article/india/oxygen-beds-rural-covid-testing-coronavirus-cases-7317953/ (accessed on 11 November 2021).
- Jawerth, N. How is the COVID-19 virus detected using real time RT–PCR? IAEA Bull. 2021, 8–11. Available online: https://www.iaea.org/sites/default/files/6120811.pdf (accessed on 29 October 2021).
- Scohy, A.; Anantharajah, A.; Bodéus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J. Clin. Cirol. 2020, 129, 104455. [Google Scholar] [CrossRef]
- Monathy, A.; Kabi, A.; Kumar, S.; Ada, V. Role of Rapid Antigen Test in the Diagnosis of COVID-19 in India. J. Adv. Med. Med. Res. 2020, 12, 77–80. [Google Scholar] [CrossRef]
- Gupta, A.; Khurana, S.; Das, R.; Srigyan, D.; Singh, A.; Mittal, A.; Singh, P.; Soneja, M.; Kumar, A.; Singh, A.K.; et al. Rapid chromatographic immunoassay-based evaluation of COVID-19: A cross-sectional, diagnostic test accuracy study & its implications for COVID-19 management in India. Indian J. Med. Res. 2020, 153, 126–131. [Google Scholar] [CrossRef]
- Kanaujia, R.; Ghosh, A.; Mohindra, R.; Singla, V.; Goyal, K.; Gudisa, R.; Sharma, V.; Mohan, L.; Kaur, N.; Mohi, G.K.; et al. Rapid antigen detection kit for the diagnosis of SARS-CoV-2—Are we missing asymptomatic patients. Indian J. Med. Microbiol. 2021, 39, 457–461. [Google Scholar] [CrossRef]
- Cohen, R.; Levy, C.; Ovetchkine, P.; Boucherat, M.; Weil-Olivier, C.; Gaudelus, J.; De La Rocque, F.; Bingen, E. Evaluation of streptococcal clinical scores, rapid antigen detection tests and cultures for childhood pharyngitis. Eur. J. Pediatrics 2004, 163, 281–282. [Google Scholar] [CrossRef]
- Weil, G.J.; Lammie, P.J.; Weiss, N. The ICT Filariasis Test: A rapid-format antigen test for diagnosis of bancroftian filariasis. Parasitol. Today 1997, 13, 401–404. [Google Scholar] [CrossRef]
- Joshi, R.; Colford, J.M.; Kalantri, S.; Reingold, A.L. Nonmalarial Acute Undifferentiated Fever in a Rural Hospital in Central India: Diagnostic Uncertainty and Overtreatment with Antimalarial Agents. Am. J. Trop. Med. Hygiene. 2008, 78, 393–398. [Google Scholar] [CrossRef]
- ICMR. Rapid Antigen Test Kits for COVID-19 (Oropharyngeal Swabs/Nasopharyngeal Swabs/Oral Saliva); Ministry of Health, Government of India: Delhi, India, 6 January 2022. Available online: https://www.icmr.gov.in/pdf/covid/kits/List_of_rapid_antigen_kits_06012022.pdf (accessed on 10 January 2022).
- Vicziany, M.; Hardikar, J. Point-of-Care Blood Tests: Do Indian Villagers Have Cultural Objections. Front. Chem. 2018, 6, 505. [Google Scholar] [CrossRef] [Green Version]
- Hardikar, J. Ramrao: The Story of India’s Farm Crisis; HarperCollins: Delhi, India, 2021. [Google Scholar]
- Ministry of Finance. Economic Survey of India, 2020–2021, Vol. 2; Government of India: Delhi, India, 2021. Available online: https://www.indiabudget.gov.in/economicsurvey/ (accessed on 31 October 2021).
- Johns Hopkins University. ‘Corona Virus Resource Centre: India Overview’. Available online: https://coronavirus.jhu.edu/region/india (accessed on 20 November 2021).
- Gettleman, J.; Yasir, S.; Kumar, H.; Raj, S.; Loke, A. As COVID-19 Devastates India, Deaths Go Undercounted. The New York Times. 24 April 2021. Available online: https://www.nytimes.com/2021/04/24/world/asia/india-coronavirus-deaths.html (accessed on 4 August 2021).
- Pradhan, B.; Chaudhary, A. Covid May Have Claimed as Many as 5 Million Lives in India. Bloomberg. 22 July 2021. Available online: https://www.bloomberg.com/news/features/2021-07-21/covid-19-may-have-claimed-as-many-as-5-million-lives-in-india (accessed on 4 August 2021).
- Anonymous. Multiply by six. Economist 2021, 439, 9249. Available online: https://www.proquest.com/magazines/multiply-six/docview/2540039166/se-2?accountid=12528 (accessed on 25 September 2021).
- Jha, P.; Deshmukh, Y.; Tumbe, C.; Suraweera, W.; Bhowmick, A.; Sharma, S.; Novosad, P.; Hang Fu, S.; Newcombe, L.; Gelband, H.; et al. COVID morality in India: National Survey Data and Health Facility Deaths. Science 2022, 375, 667–671. [Google Scholar] [CrossRef]
- Office of the Registrar General & Census Commissioner, India 2010–2013. Causes of Death Statistics, Presentation on Causes of Death in India 2010–2013, Ministry of Home Affairs, Government of India: Delhi, India, n.d.), Slide 2, ‘Background’. Available online: http://censusindia.gov.in/vital_statistics/VA_2010-13_Presentation_DRG_Release.pptx (accessed on 13 September 2021).
- Institute for Health Metrics and Evaluation. COVID-19 Results Briefing: India; University of Washington School of Medicine: Seattle, DC, USA, 2021; Available online: http://www.healthdata.org/sites/default/files/files/Projects/COVID/2021/163_briefing_India_.pdf (accessed on 29 September 2021).
- Harvey, K.; Adolphs, S. Discourse and healthcare. In The Routledge Handbook of Discourse Analysis; Routledge: London, UK, 2011; Available online: https://www.routledgehandbooks.com/DOI/10.4324/9780203809068.ch33 (accessed on 2 January 2022).
- Clerehan, R.; Buchbinder, R. Towards a more valid account of functional text quality: The case of the patient information leaflet. Text Talk 2006, 26, 39–68. [Google Scholar] [CrossRef]
- Mylab Discovery Solutions. Information for Use: CoviSelf, COVID-19 Rapid Antigen Test, Self Test Kit, Version 1. 26 April 2021. Available online: https://CoviSelf.com/ifu-leaflet/CoviSelf-IFU-English.pdf (accessed on 28 October 2021).
- Lindsay Prior. Documents in Health Research. In The SAGE Handbook of Qualitative Methods in Health Research; SAGE Publications: Los Angeles, CA, USA, 2010; pp. 417–432. [Google Scholar]
- Vicziany, M.; Hardikar, J. India’s Rural Medical Revolution: The Attitudes of Villagers to Village-Level Blood Testing in Maharashtra. S. Asia J. S. Asian Stud. 2021, 44, 1146–1166. [Google Scholar] [CrossRef]
- CoviSelf by Mylab, Product Video. Available online: https://coviself.com (accessed on 11 February 2022).
- CDC. When and How to Wash Your Hands; CDC: Atlanta, GA, USA, 2022. Available online: https://www.cdc.gov/handwashing/when-how-handwashing.html (accessed on 1 February 2022).
- Pomeroy, R. (Ed.) World Economic Forum: The Davos Agenda: Does Omicron Mean the End for COVID-19? Anthony Fauci and Other Experts on Radio Davos. Geneva: 18 January 2022. Available online: https://www.weforum.org/agenda/2022/01/omicron-end-of-covid-19-anthony-fauci-radio-davos/ (accessed on 2 February 2022).
- Vicziany, M. The Modernisation of South Asia’s Disease Burden: 1950 to 2021. S. Asia J. S. Asian Stud. 2021, 44, 1114–1130. [Google Scholar] [CrossRef]
- CoviSelf by Mylab, Resources: FAQs. Available online: https://coviself.com/faqs.php (accessed on 12 February 2022).
- Data Meant for CoWIN Portal Leaked Online, over 20,000 Indians Likely Affected. Hindustan Times. 21 January 2022. Available online: https://www.hindustantimes.com/india-news/data-meant-for-cowin-portal-leaked-online-over-20-000-indians-likely-affected-101642767559692.html (accessed on 30 January 2022).
- Patel, A.V.; (International Association of Rural Health and Medicine, Pune, Maharashtra, India). Personal communication, 10 November 2021.
- Annan, K. On the Digital Divide; United Nations Secretary General: New York, NY, USA, 5 November 2002; Available online: https://www.un.org/sg/en/content/sg/articles/2002-11-05/digital-divide (accessed on 7 January 2022).
- Lohchab, H. Overall India Handset Market Growth to Fall in 2020. Economic Times. 24 December 2019. Available online: https://economictimes.indiatimes.com/tech/hardware/overall-india-handset-market-growth-to-fall-in-2020/articleshow/72950192.cms?from=mdr (accessed on 30 October 2021).
- Kantar IMRB/MMA. Feature Phone Usage and Behaviour Report [Overview]—India, 2016–2017; Mobile Marketing Association (MMA): New York, NY, USA, 2017; Available online: https://www.mmaglobal.com/files/documents/mma_kimrb_featurephone_report_overview_for_pr_c5.pdf (accessed on 7 January 2022).
- Jain, M. Why India’s Digital Divide Is Hampering Vaccine Access. Devex. 20 May 2021. Available online: https://www.devex.com/news/why-india-s-digital-divide-is-hampering-vaccine-access-99943 (accessed on 29 September 2021).
- Census of India. Trends in Urbanisation; Chapter IV; Government of India: Delhi, India, 2011. Available online: https://censusindia.gov.in/2011-prov-results/paper2-vol2/data_files/Meghalaya/CHAPTER_IV.pdf (accessed on 7 January 2022).
- Darji, P. Suo Motu Cognizance by the Indian Judiciary. Myadvo. 7 March 2018. Available online: https://www.myadvo.in/blog/suo-motu-cognizance-by-the-indian-judiciary/ (accessed on 31 October 2021).
- SLFC. SFLC.in Files an Intervention Application in the Supreme Court of India. Re Distribution of Essential Supplies and Services during Pandemic Challenging the Mandatory Imposition of CoWIN. 29 May 2021. Available online: https://sflc.in/sflcin-files-intervention-application-supreme-court-india-re-distribution-essential-supplies-and?fbclid=IwAR2IvPU2Gt3c3RzIK0MVNB-E3JamUGlcyDOPHlpZX3PuvxYCLRi7-NF_7eQ (accessed on 30 October 2021).
- SFLC. SFLC Writes to National Health Authority against Mandatory Imposition of CoWIN. 29 April 2021. Available online: https://sflc.in/sflcin-writes-national-health-authority-against-mandatory-imposition-cowin (accessed on 30 October 2021).
- Legal Correspondent. Wake up to the Digital Divide, SC Tells Centre, in Jab at Vaccine Policy. The Hindu Businessline. 31 May 2021. Available online: https://www.thehindubusinessline.com/news/apex-court-raises-questions-on-centres-plan-to-inoculate-entire-population-by-year-end/article34690372.ece (accessed on 30 October 2021).
- Mendelsohn, O.; Vicziany, M. The Untouchables: Subordination, Poverty and the State in Modern India; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar] [CrossRef]
- Vicziany, M. Coercion in a Soft State: The Family-Planning Program of India: Part I: The Myth of Voluntarism. Pac. Aff. 1982, 55, 373–402. [Google Scholar] [CrossRef]
- Vicziany, M. Coercion in a Soft State: The Family-Planning Program of India: Part 2: The Sources of Coercion. Pac. Aff. 1982, 55, 557–592. [Google Scholar] [CrossRef]
- Vicziany, M.; Plahe, J. Food Security and Traditional Knowledge in India: The Issues. S. Asia J. S. Asian Stud. 2017, 40, 566–581. [Google Scholar] [CrossRef]
- Vicziany, M.; Chattopadhyay, D.; Bhattacharyya, S. Food from Sewage: Fish from the East Kolkata Wetlands and the Limits of Traditional Knowledge. S. Asia J. S. Asian Stud. 2017, 40, 619–644. [Google Scholar] [CrossRef]
- Vicziany, M.; Plahe, J. Extending Traditional Food Knowledge into New Marketing Institutions for Small Farmers in India. S. Asia J. S. Asian Stud. 2017, 40, 645–668. [Google Scholar] [CrossRef]
- Vicziany, M.; Bapat, B.J.; Kesarkar-Gavankar, A. Weapons of the Weak: The Seven Water Spirits (Saat Asaaras) and the Indian Courts in the Kolis’ Struggle against Environmental Destruction. In Goddesses and the South Asian Environment; Vicziany, M., Bapat, B.J., Eds.; Monash University Publishing: Melbourne, Australia, 2022. [Google Scholar]
- Hardikar, J. A Village Awaits Doomsday; Penguin India: Delhi, India, 2013. [Google Scholar]
- Supreme Court of India, Civil Original Jurisdiction, Petition No. 3 of 2021. In Re: Distribution of Essential Supplies and Services during Pandemic, Section E.5 Digital Divide and Conclusion, Delhi, India: 31 May 2021. Available online: https://main.sci.gov.in/supremecourt/2021/11001/11001_2021_35_301_28040_Judgement_31-May-2021.pdf (accessed on 7 January 2021).
- Bureau of Labour. Wages Rate Data Dec. 2021; Ministry of Labour and Employment, Government of India: Delhi, India, 2021. Available online: http://labourbureaunew.gov.in/UserContent/Wage_Rate_Dec_2021.pdf (accessed on 9 February 2022).
- UNDP; Oxford Poverty and Human Development Initiative Oxford University. Global Multidimensional Poverty Index 2021: Statistical Tables; Oxford University: Oxford, UK, 2021; Available online: http://hdr.undp.org/sites/default/files/2021_mpi_statistical_data_table_1_and_2_en.pdf (accessed on 9 January 2022).
- NITI Aayog; UNDP; OPHI. India: National Multidimensional Poverty Index; Government of India: Delhi, India, 2021. Available online: https://www.niti.gov.in/sites/default/files/2021-11/National_MPI_India-11242021.pdf (accessed on 9 January 2022).
- UNDP; OPHI. Global Multidimensional Poverty Index 2021: Unmasking Disparities by Ethnicity, Caste and Gender; UNDP/OPHI: Geneva, Switzerland; Oxford, UK, 2021; Available online: http://hdr.undp.org/sites/default/files/2021_mpi_report_en.pdf (accessed on 9 January 2022).
- Ministry of Health and Family Welfare. Rural Health Statistics 2019–2020; Government of India: Delhi, India, 2020; Available online: https://ruralindiaonline.org/en/library/search?q=rural+health+statistics&type=resource (accessed on 31 January 2022).
- Das, J. Two Indias: The structure of primary health care markets in rural Indian villages with implications for policy. Soc. Sci. Med. 2020, in press. [CrossRef] [PubMed]
- Radhakrishnan, V. Vaccination in Rural India Trails Urban Areas Even as Cases Surge. The Hindu. 18 May 2021. Available online: https://www.thehindu.com/news/national/vaccination-in-rural-india-trails-urban-areas-even-as-cases-surge/article34589734.ece (accessed on 21 January 2022).
- TICA; IDFC Institute. India COVID-19 Vaccination Distribution Report; IDFC: Mumbai, India, 2021; Available online: https://www.idfcinstitute.org/site/assets/files/16432/tica_distribution_report_web_v1.pdf (accessed on 22 January 2022).
- State Bank of India. COVID-19: Third Wave, the Beginning of the End? SBI: Mumbai, India, 2022; Available online: https://sbi.co.in/documents/13958/10990811/180122-COVID%20Third%20wave%20_Jan%2022.pdf/c07ea843-e94a-d1c4-904e-2eb609110784?t=1642510256902 (accessed on 22 January 2022).
- Kulkarni, P.; Akarte, S.V.; Mankeshwar, R.M.; Bhawalkar, J.S.; Banerjee, A.; Kulkarni, A.D. Non-Adherence of New Pulmonary Tuberculosis Patients to Anti-Tuberculosis Treatment. Ann. Med. Health Sci. Res. 2013, 3, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Google Play, Mylab CoviSelf Reviews. Available online: https://play.google.com/store/apps/details?id=netsurf.mylab.coviself&hl=en_AU&gl=US (accessed on 12 February 2022).



{kind=link}
{kind=link}
| Variables | All India | Urban | Rural |
|---|---|---|---|
| Population in millions | 1433 mil | 485 mil | 948 mil |
| Active internet users (AIUs) | 622 | 323 | 299 |
| % growth in AIUs during last 12 months | 4 | 13 | |
| % of AIUs in urban/rural India | 67 | 31 | |
| Top 9 cities’ share of urban AIUs as a % | 33 | ||
| Share of AIUs in villages with populations over 1000 | 85 | ||
| Highest usage state in India: Maharashtra with highest % of AIUs relative to state population | 61 | ||
| Lowest usage state in India: Bihar with lowest % of AIUs relative to state population | 24 | ||
| Ratio of male: female AIUs | 57:43 | 58:42 | |
| % AIUs using mobiles | 100 | 100 | |
| % AIUs using PCs | 22 | 13 | |
| % AIUs using other, e.g., tablets, smart TVs etc. | 7 | 5 | |
| Average duration of AIUs on internet in mins | 115 | 99 | |
| % of AIUs using internet for entertainment | 96 | 96 | |
| % of AIUs using internet for Communication | 92 | 87 | |
| % of AIUs using internet for social media | 84 | 79 | |
| % of AIUs using internet for net commerce | 59 | 30 | |
| % of AIUs using internet for online Shopping | 43 | 13 | |
| % AIUs texting & emailing | 87 | 79 | |
| % of AIUs voice & video messaging | 54 | 57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicziany, M.; Hardikar, J. Can Self-Administered Rapid Antigen Tests (RATs) Help Rural India? An Evaluation of the CoviSelf Kit as a Response to the 2019–2022 COVID-19 Pandemic. Diagnostics 2022, 12, 644. https://doi.org/10.3390/diagnostics12030644
Vicziany M, Hardikar J. Can Self-Administered Rapid Antigen Tests (RATs) Help Rural India? An Evaluation of the CoviSelf Kit as a Response to the 2019–2022 COVID-19 Pandemic. Diagnostics. 2022; 12(3):644. https://doi.org/10.3390/diagnostics12030644
Chicago/Turabian StyleVicziany, Marika, and Jaideep Hardikar. 2022. "Can Self-Administered Rapid Antigen Tests (RATs) Help Rural India? An Evaluation of the CoviSelf Kit as a Response to the 2019–2022 COVID-19 Pandemic" Diagnostics 12, no. 3: 644. https://doi.org/10.3390/diagnostics12030644