
The effects of COVID-19 related shutdowns on perceived lifestyle and prevalence of musculoskeletal discomfort
Abstract
BACKGROUND:
COVID-19 caused a transition to work-from-home conditions, closures of recreation facilities and cancelation of social events.
OBJECTIVE:
This study sought to characterize and quantify the impact COVID-19 related shutdowns had on perceptions of health and wellbeing, musculoskeletal discomfort, and physical characteristics of workstation set-up in full time workers who transitioned to working from home.
METHODS:
297 participants from 8 countries completed a retrospective pre/post survey design that assessed outcomes prior to COVID-19 shutdowns and when each participant was experiencing peak pandemic-related restrictions. There were 3 categories including, health and wellbeing, musculoskeletal discomfort, and workplace ergonomics.
RESULTS:
General discomfort on a scale from 1 to 100 increased from 31.4 pre to 39.9 during COVID-19. Notable areas increasing in severity of discomfort from pre to during included the neck (41.8 to 47.7), upper back (36.3 to 41.3) and right wrist (38.7 to 43.5). The percentage of the population experiencing discomfort increased from pre to during in the low back (41.5% to 55.2%), upper back (28.7% to 40.9%), neck (45.5% to 60.9%) and right wrist (16.1% to 23.7%).
CONCLUSION:
There were three distinct groups for physical activity one group including, one maintaining and one that decreased, which did not have an impact on perceived general discomfort. There was a significant decrease in usage of a desk and adjustable chair and an increase in laptop use. Working from home in some capacity will likely be a more common occurrence which will require further ergonomic assessments and considerations to keep a healthy workforce.
1Introduction
The impact of COVID-19 varied between countries, provinces/ states and even regions; however, in many cases local restrictions resulted in a dramatic change to day-to-day lifestyle. There are many different models of health which dictate how to handle changes in lifestyle and which changes play a role in the development of disease [1]. No matter the model of health, the consensus is that a prevention approach is superior to a treatment one [2]. It is therefore notable that many COVID-19 shutdowns resulted in dramatic changes in common lifestyle mediated disease prevention approaches including the closure of recreational facilities, change to working from home, and reduction/canceling of social events. While these methods prevent the spread of an airborne virus, they come at a cost of limiting access to physical fitness resources and removing social interactions. Physical activity and social interactions are two of the key social determinates of health [3] which influence the risk of illness. The social determinates of health are developed from the biopsychosocial model [4] which takes into consideration the relationship between the entire human experience and health.
Physical activity (PA) has systemic benefits which reduce the risk of many chronic medical conditions. International guidelines recommend 150 minutes of moderate to vigorous PA per week; however, many benefits are seen with a volume much lower than this threshold [5, 6]. In addition to protecting against chronic health conditions, strength training and other forms of exercise therapy have been found to reduce physical symptoms, specifically neck and non-specific low back pain [7, 8]. There is also very strong evidence on the benefits of PA on mental health [9, 10]. While any form of PA leads to positive health outcomes, leisure/recreational PA has the most impact on mental health. Due to the wide benefits, public health messages and campaigns on getting a population more active are important. The largest determinants of individual activity habits are the ease of access and or barriers to the activities. As such, restrictions implemented in many parts of the world as a necessity to combat COVID-19, stand to directly impact these factors [1, 11].
Office spaces and workstations have been researched for decades to reduce musculoskeletal discomfort and increase worker productivity. Roughly 20–33% of the global population deals with a musculoskeletal disorder (MSD). Furthermore, MSDs are the number one lost work time claim in Canada leading to ∼$14 billion in production loss [12]. Poor posture and workplace setup is associated with many MSDs including neck and lower back pain as well as carpal tunnel syndrome [13–15]. Performing ergonomic interventions in workplaces can lead to a return on investment of 3:1 to 15:1 [16] making it worth while for companies to spend money on various interventions such as: training sessions, workstation redesigns, and accessories (chair, mice, keyboard, and monitor) [17]. As a result of large-scale implementation of ergonomic aids across many sectors, it is likely that many people do not have a comparable home office set up, which may have left individuals at risk of developing MSDs during a rapid pivot to working in an at-home environment.
This study seeks to characterize and quantify the impact COVID-19 related shutdowns have had on perceptions of health and wellbeing and musculoskeletal discomfort in full time workers. Working conditions and behaviour are evaluated before local peak shutdowns (PRE) and during (PEAK). This will allow for a better understanding of the possible detriments from prolonged/repeated shutdowns, helping future research and public health policy. Additionally, as working from home in some capacity may continue after restrictions are lifted, work from home ergonomics require further optimization. Our hypotheses are threefold, that (1) COVID-19 related shutdowns will result in an increase in sedentary behaviour, a shift towards poor dietary choices, reduced perceived access to healthcare providers and an increase in anxiety and depression, (2) COVID-19 related shutdowns will result in an increased prevalence and severity of site specific musculoskeletal discomfort and (3) there will be a decreased use of ergonomic workstation tools while working at home.
2Methods
2.1Participants
This study was approved by the university research ethics board. Prior to completing the online survey all participants provided informed consent. To be included in the study, the respondent needed to be 18 years of age or older, English speaking, working a full-time job, have access to the internet, and had to make a transition to working from home during the COVID-19 shutdowns. A convenience sample of participants were recruited voluntarily through social media posts, news articles, and word of mouth from June to December 2021.
2.2Survey development
The survey was created using QualtricsXM (Qualtrics, Seattle, WA, Provo, UT, USA) and included questions on self-reported demographics, health and wellbeing, musculoskeletal discomfort (MSD), and office ergonomics. The survey followed a retrospective pre/post design that assessed outcomes prior to COVID-19 shutdowns and when each participant was experiencing peak pandemic-related restrictions. Given the possible differences in duration and timing of regional shutdowns, the participants were asked to base their answers off when they considered their area to be at its peak restrictions and were not asked to provide specific dates. The demographics section asked about age, gender, sex, location, and occupation. The health and wellbeing section asked about hours of recreational physical activity, screen time and sedentary behaviour per week, dietary choices, exercise motivation, general anxiety and depression, and perceived access to health care. The MSD section asked about perceived discomfort prevalence and severity in general and in 11 specific sites (neck, upper and lower back, left and right shoulders, elbows, forearms, and wrists). The ergonomics section asked about workstation set up: the most used device (laptop, desktop, tablet), pointing device (mouse, track pad, stylus), monitor, chair, desk, and movement behaviour. The specific wording of questions and multiple-choice answers was pilot tested with a small group (n = 13; responses not recorded) to ensure there was no confusion to interpretation. This pilot sample consisted of young and middle-aged professionals (25–30; 35–45 years of age), including occupations such as accounting, software engineering, marketing and university professors experienced in qualitative research using surveys. All questions were optional following the completion of the informed consent process.
2.3Data analysis and statistics
Due to the mass distribution and online nature of the survey, the responses were reviewed to confirm they fit the inclusion criteria. This was done by discussing the goal and nature of the survey with Qualtrics employees to develop the following steps. First, we assessed unique IP addresses to prevent duplicate responses, next we evaluated for unreasonably fast completion times to reduce the chance of computer-generated responses and then critically assessed the responses to specific filtering questions to remove participants that did not fit the criteria. To do this, the occupation section was examined, and responses were removed for any occupation that could not be performed from a home setting (e.g., surgeon, driver). Next, the self-reported questions were reviewed to ensure that all responses were reasonable, and any outlying data points were removed based on natural/functional time limitations (e.g., 40+ hours/ week of physical activity, <14 or >150, hours/ week of sedentary behaviour). All incomplete surveys were automatically deleted by Qualtrics after 2 weeks of inactivity. Following data cleaning, 297 complete responses remained for further analysis. To create equal sample sizes between groups during statistical analyses, responses were chosen at random from each group to match the smallest group size. All statistical analyses are detailed below and were completed in SPSS version 28.0.0 (IBM Corporation, Armonk, NY, USA). For all analyses, significance was set to p < 0.05.
2.3.1Statistical Analysis 1 – The assessment of physical activity as a protective lifestyle measure
The first analysis was a MANOVA for the change in health and wellbeing from PRE to PEAK shutdown. During initial assessments, there were three distinct groups of change in physical activity, one that increased, one that decreased and one that maintained the exact same activity time. The three physical activity groups were evaluated with dependent variables of change in: sedentary behaviour (SB), screen time (ST), exercise motivation (EM), dietary choices (DC), perceived access to health care (HC), general anxiety (Anx), general depression (Dep), and general discomfort (GD). Any significant main effects were further investigated with Games-Howell post hoc analysis.
2.3.2Statistical Analysis 2 – The assessment of self-reported musculoskeletal discomfort
To evaluate the effect of timepoint (PRE, PEAK) on musculoskeletal discomfort a Chi square analysis was completed on the number of positive responses to general and site-specific discomfort between pre and peak shutdown timepoints to evaluate a change in prevalence. Next t-tests were performed on the severity of discomfort for general, and site-specific regions between the pre and peak shutdowntimepoints.
2.3.3Statistical Analysis 3 – The assessment of workplace ergonomics
Five separate MANOVAs were performed between workstation tools and the severity of discomfort in all areas. The five analyses were device type (desktop, laptop, or tablet), input type (mouse, trackpad, or stylus), adjustable chair (yes or no), proper sized desk (yes or no) and external monitor/second monitor (yes or no). A Games-Howell post hoc analysis was performed when necessary to further explore significant effects. Additionally, a Chi square test was implemented to explore differences in the use of the different workstation tools between pre and peak shutdown time points.
3Results
3.1Demographics
There were 297 used responses (147 males, 148 females, 2 intersex) from 8 countries (Canada: 148, USA: 132, Australia: 11, Germany: 1, Argentina: 1, Afghanistan: 1, Jordan: 1, and Italy: 1) between the ages of 18 and 65 (34.7±10.3 years). While there can be significant diversity both between and within countries, responses from regions were not balanced preventing location specific analysis. For the entire sample, 228 participants were right-handed, 36 were left-handed, 32 were ambidextrous and 1 no response. There were 90 responses from the increase in PA group, 133 from the decrease in PA group and 74 from the maintained PA group. Table 1 provides a detailed breakdown of the groups.
Table 1
Mean±SD participant demographics
| Group (split by change in PA) | N | Male | Female | Age (years) | Change in PA (hours/week) |
| Increase | 90 | 46 | 44 | 35.1±11.0 | +8.7±12.0 |
| Decrease | 133 | 60 | 73 | 34.0±9.7 | –5.17±3.5 |
| Maintain | 74 | 41 | 31 | 35.3±10.8 | 0±0 |
3.2The assessment of physical activity as a protective lifestyle measure
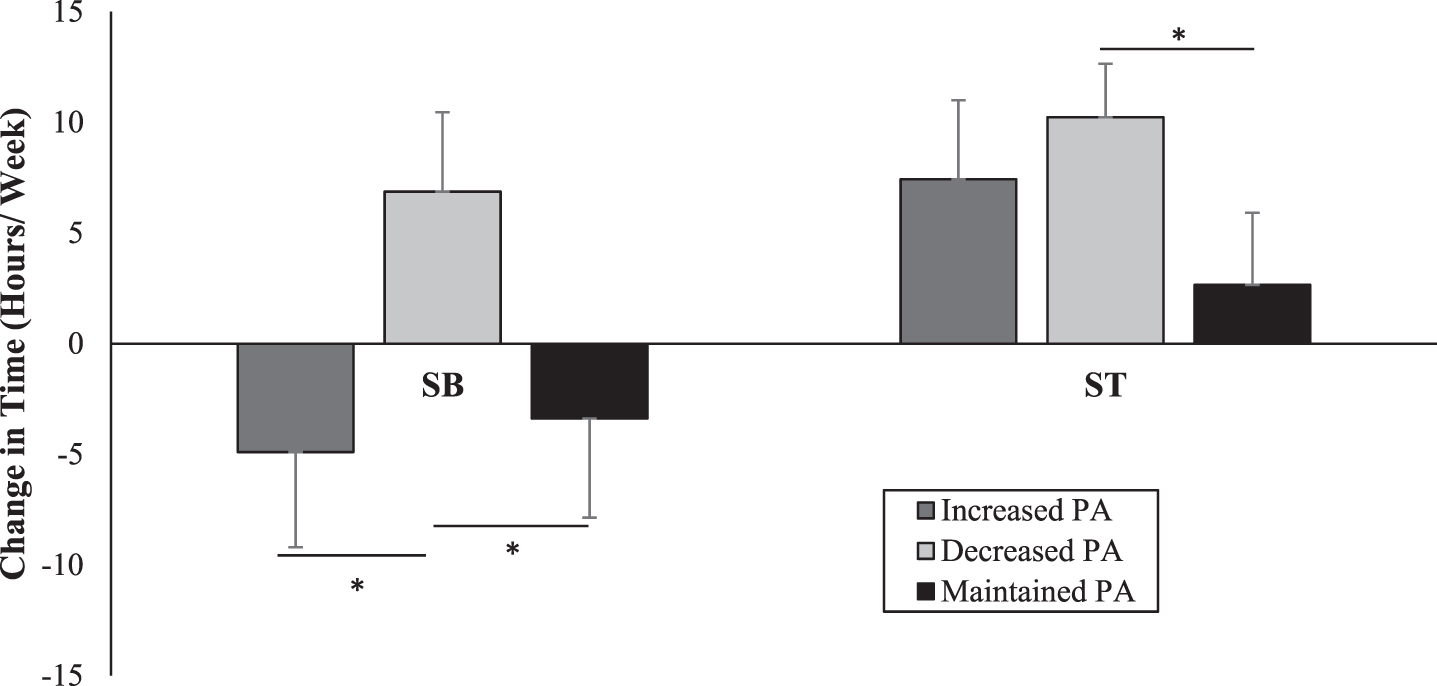
The changes in sedentary behaviour time and screen time from PRE to PEAK shutdown for each physical activity group are depicted in Fig. 1. Change in sedentary behaviour time was significantly different between the group that decreased in physical activity and the groups that increased (p = 0.019) as well as maintained physical activity level (p = 0.013). Although screen time increased, on average across all three physical activity groups, the change in screen time was significantly different between those that decreased or maintained physical activity levels (p = 0.006).
Fig. 1
Average change in time of sedentary behaviour (SB) and screen time (ST) from pre-shutdown to during peak local shutdown. Asterisks (*) denote significant differences (p < 0.05) between groups.
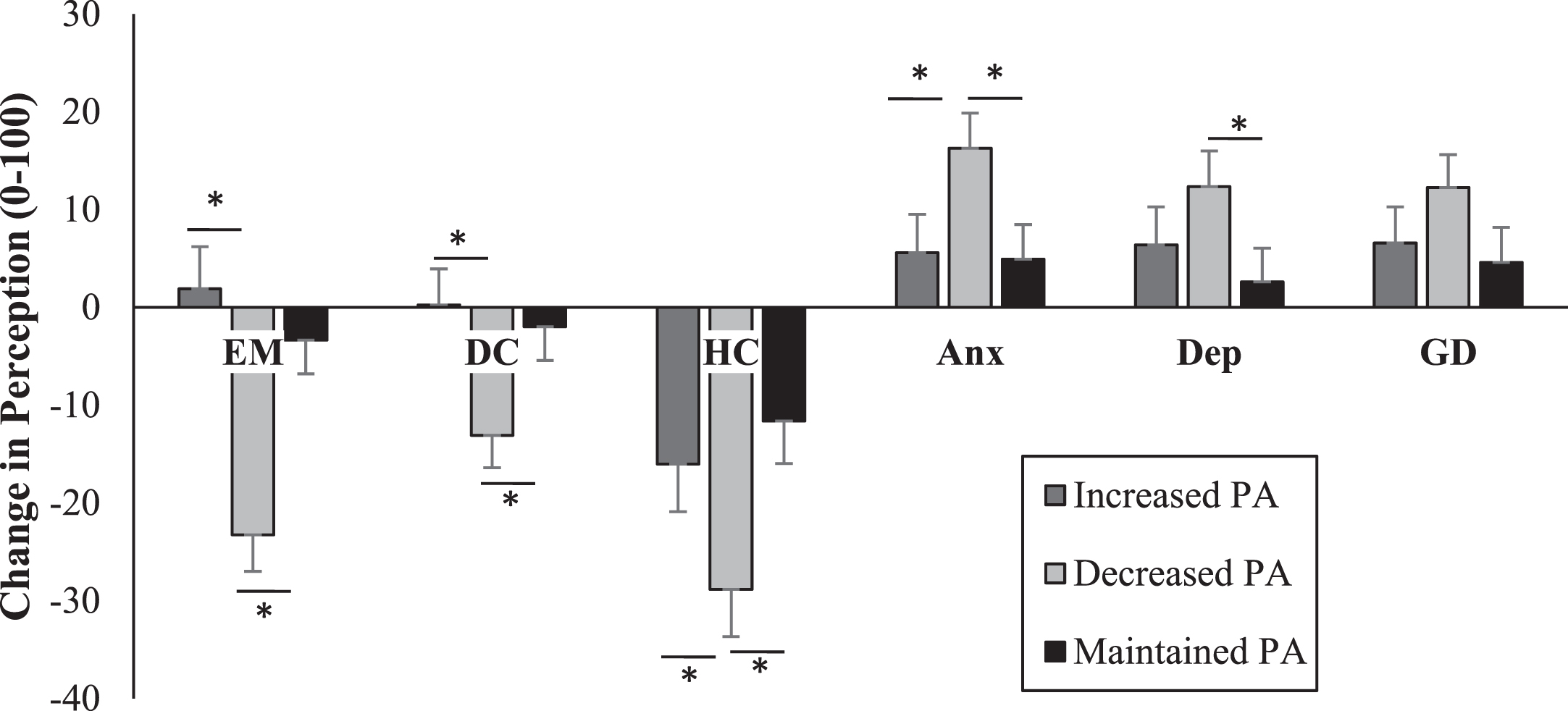
The changes in perceived health and wellbeing: EM, DC, HC, Anx, Dep, GD from pre-shutdown to during shutdown for each physical activity group are depicted in Fig. 2. Specifically, there were significant differences between the increased physical activity group and the decreased physical activity group for EM (p < 0.001), DC (p = 0.001), HC (p = 0.026), and Anx (p = 0.020). Further, there were significant differences between the maintained physical activity group and the decreased physical activity group for EM (p < 0.001), DC (p = 0.003), HC (p = 0.001), Anx (p = 0.023), and Dep (p = 0.023). No significant differences were found for change in GD or between the increased group and the decreased for any factor.
Fig. 2
Average change in perceived difference in exercise motivation (EM), dietary choices (DC), access to health care (HC), anxiety (Anx), depression (Dep) and general discomfort (GD) from pre-shutdown to during peak local shutdown. Asterisks (*) denote significant differences (p < 0.05) between groups.
3.3The assessment of self-reported musculoskeletal discomfort
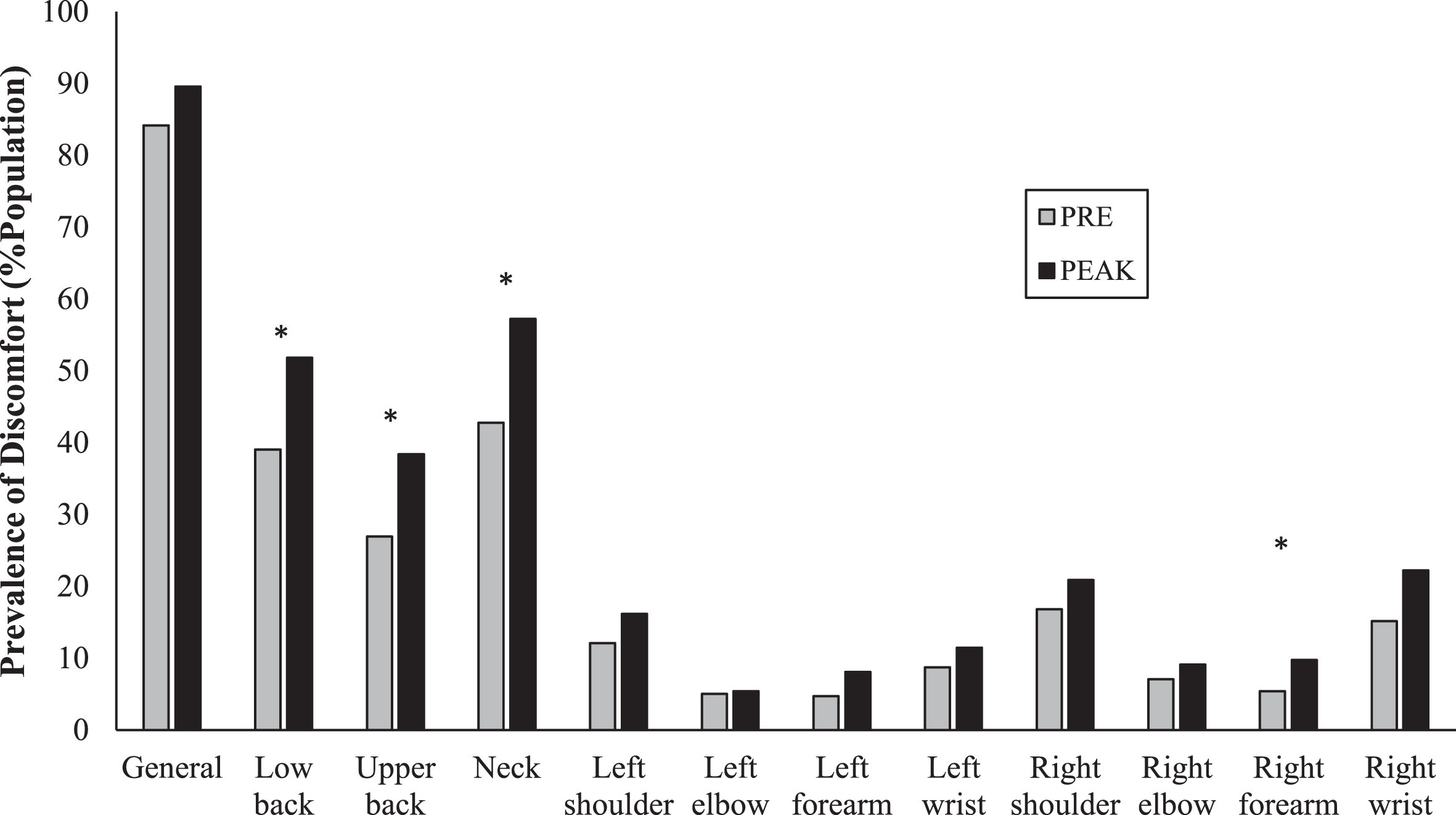
The change in prevalence of site-specific discomfort between and PRE and PEAK shutdown time points are depicted in Fig. 3. Specifically, there were statistically significant increases in the perceived discomfort of the low back (p = 0.021) from 41.5% to 55.2%, the upper back (p = 0.015) from 28.7% to 40.9%, the neck (p = 0.013) from 45.5% to 60.9%, and the right wrist (p = 0.046) from 16.1% to 23.7%.
Fig. 3
The change in prevalence of site-specific discomfort as a percentage of the population between PRE and during PEAK shutdown. Asterisks (*) denote significant differences between the time points (p < 0.05).
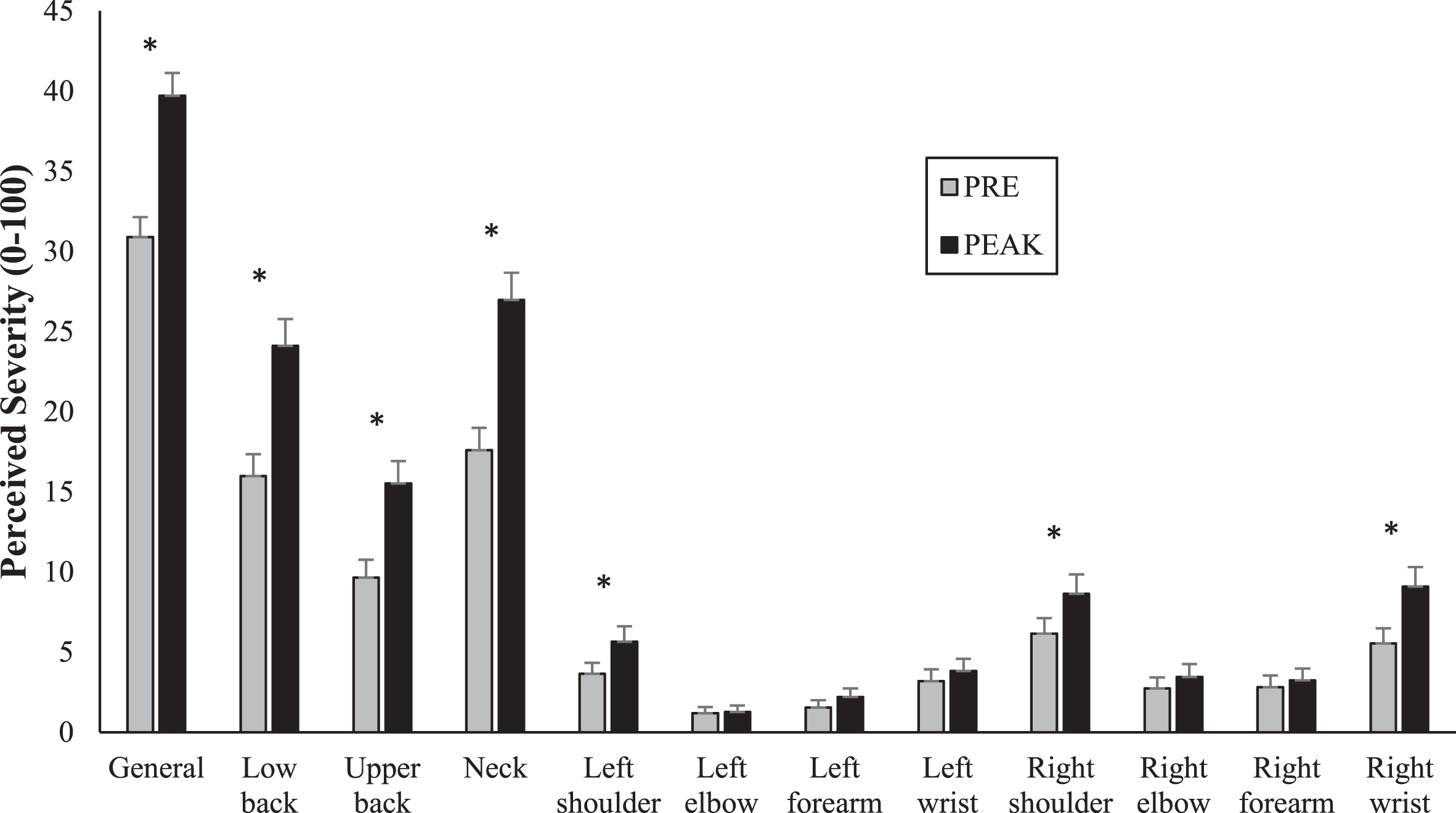
The change in severity of general and site-specific discomfort between the PRE and PEAK shutdown timepoints is depicted in Fig. 4. Specifically, there were significant increases in general pain severity (p < 0.001) from 30.90 to 39.72, and pain severity localized to the low back (p < 0.001) from 15.95 to 24.28, the upper back (p < 0.001) from 9.81 to 15.93, the neck (p < 0.001) from 17.77 to 27.21, the left shoulder (p = 0.013) from 3.85 to 5.98, the right shoulder (p = 0.011) from 6.44 to 8.95 and, the right wrist (p < 0.001) from 5.77 to 9.36.
Fig. 4
The change in perceived severity of general and site-specific discomfort on a scale of 0–100 between PRE and during PEAK shutdown. Asterisks (*) denote significant differences between the time points (p < 0.05).
3.4The assessment of workplace ergonomics
The results from the five MANOVAs on workstation set up are as follows. For device (desktop, laptop, tablet) use: the use of a tablet resulted in less discomfort in the low back than a laptop (p = 0.019) and had less discomfort than a desktop in the right elbow (p = 0.025), right forearm (p = 0.046), and right wrist (p = 0.036). There were no differences in discomfort between any of the input devices (mouse, trackpad, and stylus) for any location. Using a monitor resulted in lower discomfort in the right forearm (p = 0.010); however, there were no further significant differences. The use of a properly sized desk resulted in a lower general discomfort (p = 0.008), as well as reduced discomfort in the lower back (p < 0.001), right forearm (p = 0.012), and right wrist (p = 0.045). The use of an adjustable chair resulted in a lower discomfort in the lower back (p = 0.045).
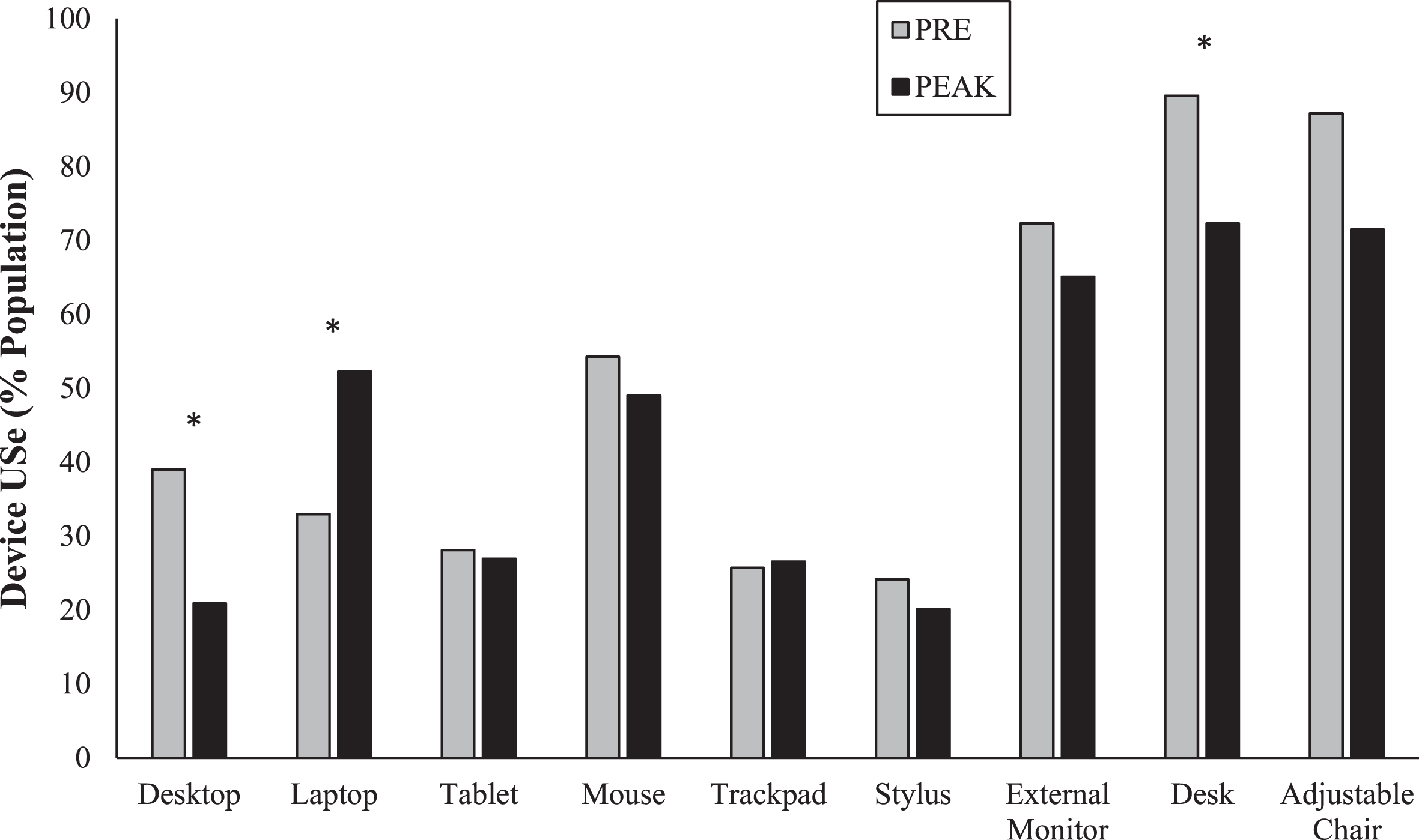
The change in prevalence of ergonomic tool usage between PRE and PEAK shutdown timepoints are depicted in Fig. 5. Specifically, there were significant decreases in desktop usage (p < 0.001) from 38.9% to 20.9%, and properly designed desk usage (p = 0.032) from 89.6% to 72.3%. Further, there was a statistically significant increase in laptop usage (p < 0.001) from 32.9% to 52.2%.
Fig. 5
The change in usage of different occupational devices as a percentage of the population between PRE and during PEAK shutdown. Asterisks (*) denote significant differences between the time points (p < 0.05).
4Discussion
4.1The assessment of physical activity as a protective lifestyle measure
Our initial expectation for physical activity would be that it would decrease during COVID-19 shutdowns due to the closure of fitness facilities. This hypothesis came from the health belief model in which there are four broad factors that impact a person’s adoption of a health behaviour, perceived susceptibility to disease, perceived severity of disease, perceived cost and barriers, and motivation [11]. Our belief was that people would perceive that by increasing the difficulty of performing exercise, the benefits no longer outweigh the costs. The result was more complicated that this, we found three groups, one which decreased, one that maintained and one that increased recreational physical activity. A key difference between these groups was their motivation to exercise; the decrease group had a larger reduction in exercise motivation than the other two while the increase group also increased motivation to exercise. An important factor which was not looked into was the access to alternative forms of exercise. The majority of our responses came from developed countries which have invested into the development and planning of a city to promote healthier lifestyles. This may be a trend that cities can look into to put less of a reliance on typical forms of physical activity. While there were no differences in physical discomfort, the maintained and increased group had less screen time and made healthier dietary choices. Research has been done on the effect of changing working environment during the pandemic [18]. The change to working from home resulted in significantly lower physical activity compared to workers who maintained their previous working style, either on site or hybrid. This finding was done with workers from the same region under similar restrictions. While at a workplace, many companies advocate for moving around to reduce the sedentary behaviour, they may need to adopt a similar strategy to encourage movement while working from home [19]. With an increased amount of freedom and opportunity for midday exercise, there may need to be changes to what is considered a to be a normal workday, including working hours.
All three physical activity groups experienced an increase in general anxiety, depression, and physical discomfort during the shutdown. The increases in general anxiety and depression during the COVID-19 shutdowns has been demonstrated by previous research as social distancing behaviour increases [20]. Our results also agree with the effect of recreational physical activity as a mediating agent for mental health. Our results show that increasing physical activity is not related to higher benefits but that decreasing is related to worse mental health and healthy lifestyle choices. This result may be do less to the activity itself but more to the sense of normalcy that it provides. Previous research has demonstrated a positive association with health-related quality of life measures and physical activity [10]. Our results compliment these findings that maintaining or increasing reduces the negative changes to health-related quality of life from the COVID-19 shutdowns.
4.2The assessment of self-reported musculoskeletal discomfort
Given there was no effect on amount of physical activity and general discomfort, prevalence, and severity, all data were evaluated as a single group across the different PRE and PEAK timepoints. The lack of impact of physical activity on general discomfort contradicts previous findings [6, 21]. While there was no increase in general discomfort prevalence during the PRE/PEAK timepoints, there were significant increases in site-specific areas (Fig. 4). We reported a significant change in the prevalence (from PRE/PEAK) of MSK discomfort of 15.1%, 13.6% and 7.1% for the neck, low back, and right wrist, respectively. Further, these changes in musculoskeletal discomfort are associated with our reports of workstation ergonomics [13, 14, 22]. We also found that the reporting of severity for general discomfort changed by 9/100, low back by 8/100 and the neck by 10/100. The increase in severity of discomfort across the musculoskeletal regions identified here is concerning but the increase of prevalence is more of a sign that there is a widespread problem. The prevalence of self-reported discomfort across body regions is particularly elevated during the PEAK shutdown timepoint, and these results mirror those reported in response to online learning during COVID-19 related shutdowns [23]. Given that the job stayed the same and the location changed, these results highlight the importance of assessing the effects on COVID-19 related shutdowns on workplace ergonomics in a home-based setting.
4.3The assessment of workplace ergonomics
Our evaluation of home-based workstations was done in two parts, the first analysis evaluated the effect of an ergonomic tool on self-reported musculoskeletal discomfort. The first analysis was examined as a single sample regardless of timepoint (i.e., PRE/PEAK). Using a laptop or a desktop did not have an influence on the prevalence of discomfort for any body area. There was also no difference in prevalence of discomfort across pointing devices (using a trackpad, mouse, stylus) or using an external monitor. Both findings go against previous research on recommended workstation ergonomics, suggesting that an external mouse and monitor can improve posture and reduce discomfort [24]. Our work found that simply working from a desk yields reductions in general, low back, right forearm, and wrist discomfort. Poorly fitted desks force the worker to make decisions on functionality and space instead of ergonomics such as changing keyboard and mouseposition [25].
The second analysis evaluated how use of ergonomic tools changed due to the shutdown. Previous research has found that more than half of people working from home do not have an ergonomically designed office space to work in and 18% of people do not have a designated working area [25]. Further, there has been some evidence of elevated ROSA scores, where half of one sample had scores over 5 which is at the threshold for a high risk of WMSD [26]. While our results did not demonstrate a relationship between reported discomfort and device use, there was a significant shift from desktop to laptop use during the shutdown. We found that desktop use decreased by 18% and laptop use increased by 19% from pre to peak. There was a decrease in adjustable chair use by 16%, however this was not a significant change. This may be due to our broad question that failed to specify exactly the definition or classification of an adjustable chair. There is a large difference between a chair that adjusts in vertical height versus a chair that is fully adjustable (arms, lumbar, seat pan tilt, etc.) as each of these play a role in the risk of development of MSD [24]. To expand on the current results, it would be beneficial to do a more thorough breakdown on the quality of chair workers have while at home versus at work. Furthermore, there was also a significant decrease in use of a desk while working from home. Many respondents shared a workspace with other members in the household, having the space for one desk or even multiple may be a limitation for many people. The effectiveness of space friendly desk solutions should be evaluated and may be a growing market as working from home becomes more common. We found no changes in peripheral/pointing device (mouse, trackpad, or stylus) used from pre to post. Seat height and monitor distance changes how the worker interacts with the rest of the workstation and can be associated with greater discomfort [25]. We found increased laptop use and decreased (not significant) external monitor use and when coupled with lack of access to an adjustable chair and/or desk, together these variables likely correspond with increased severity of discomfort to the low back, neck,and wrist.
If working from home or hybrid continues and the reported increases in prevalence and severity of discomfort are, at least in part, due to at home workstations, this can have large implications for workplace injury and insurance claims. While at work, companies often supply proper work chairs and desk for their employees. From our sample, very few received assistance from their work to create their home workstation. The respondents that did receive assistance were given their work computers or monitors and only one reported being provided a chair. This will be a topic that needs more research from ethical, legal, and economic perspectives; however, the results reported here suggest that workers need to optimize at home workplace ergonomics to limit the occurrence of discomfort.
4.4Limitations
Given the breadth of our survey to cover three main topics, health and wellbeing, musculoskeletal discomfort, and ergonomics there were limitations. Our questions were structured to capture a wide population and was not occupation specific; occupation has an important role in injury risk, suggesting that occupation should be assessed individually in future studies. All surveys have unique individual interpretation of the questions, resulting in some subjective interpretation; however, our pilot testing on a small group helped limit variety in question interpretation. There were also retrospective questions, requiring participants to recall behaviour to their peak pandemic-related restrictions, which could have bias. Additionally, our free-form design allowed respondents to report any value for physical activity. While we removed responses that were unreasonable, more control over the time or stringent guideline may yield different results. Many geographical areas and regions had different strategies for COVID-19 related restrictions/shutdowns and as well as economic status, unbalanced sample sizes prevented a detailed analysis on the effect of location. While we limited our evaluation to consider only changes to working from home and closure of recreation facilities, a more location specific analysis should be performed to stratify the analysis for specific national and internationalregions.
5Conclusions
For many, COVID-19 related shutdowns greatly changed our lives for a period of time and some people will continue to be influenced by the changes. Working from home could be viewed with many positive changes such as reduced commuting, more family time and freedom with scheduling; these changes may make a work from home model continue in some capacity moving forward [27]. Along with the positive came some negative consequences to health. However, many of the reported negatives can be resolved with proper intervention. Staying active helps moderate negative mental health changes from reduced socialization. Physical activity also helps moderate healthier lifestyle characteristics such as dietary choices and sedentary time. During the COVID-19 shutdown, there were increases in both severity and prevalence of discomfort in areas commonly affected by workstation set up and ergonomics. Proper home workspace ergonomics (fully adjustable chair and desk) can reduce the physical symptoms experienced. Companies need to be aware of these changes and should be responsible for ensuring their employees have what they need, just as they are while the employee is at the workplace.
Ethical approval
This study was approved by the Brock University Office of Research Ethics (REB #20-344).
Conflict of interest
The authors have no conflict of interest to disclose.
Acknowledgments
The authors thank the participants for their time and valuable contribution.
Funding
This work was funded by grants from the Natural Sciences and Engineering Research Council (NSERC) of Canada (RGPIN 2020-05195; RGPIN 2015-05765) and the Canada Research Chairs program (231151 NSERC CRC).
References
[1] | Sutton S . Health behavior: Psychosocial theories. International Encyclopedia of the Social & Behavioral Sciences. 2001;6499-506. Elsevier. https://doi.org/10.1016/B0-08-043076-7/03872-9 |
[2] | Bolton D , Gillett G . The Biopsychosocial Model of Health and Disease: New philosophical and scientific developments. Springer International Publishing. (2019) . https://doi.org/10.1007/978-3-030-11899-0 |
[3] | Marmot M . Fair society, healthy lives: Strategic review of health inequalities in England post-2010. London, UK: Department of Health, (2010) . |
[4] | Engel GL . The need for a new medical model: A challenge for biomedicine. Science. (1977) ;196(4286):129–36. |
[5] | Warburton DER , Bredin SSD . Health benefits of physical activity: A systematic review of current systematic reviews. Current Opinion in Cardiology. (2017) ;32: (5):541–56. https://doi.org/10.1097/HCO.0000000000000437 |
[6] | Sitthipornvorakul E , Janwantanakul P , Purepong N , Pensri P , van der Beek AJ . The association between physical activity and neck and low back pain: A systematic review. European Spine Journal. (2011) ;20: (5):677–89. https://doi.org/10.1007/s00586-010-1630-4 |
[7] | Hayden J , van Tulder MW , Malmivaara A , Koes BW . Exercise therapy for treatment of non-specific low back pain. Cochrane Database of Systematic Reviews. (2005) . https://doi.org/10.1002/14651858.CD000335.pub2 |
[8] | Henchoz Y , Kai-Lik So A . Exercise and nonspecific low back pain: A literature review. Joint Bone Spine. (2008) ;75: (5):533–9. https://doi.org/10.1016/j.jbspin.2008.03.003 |
[9] | White RL , Babic MJ , Parker PD , Lubans DR , Astell-Burt T , Lonsdale C . Domain-specific physical activity and mental health: A meta-analysis. American Journal of Preventive Medicine. (2017) ;52: (5):653–66. https://doi.org/10.1016/j.amepre.2016.12.008 |
[10] | Bize R , Johnson JA , Plotnikoff RC . Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine. (2007) ;45: (6):401–15. https://doi.org/10.1016/j.ypmed.2007.07.017 |
[11] | Becker MH . The health belief model and sick role behavior. Health Education Monographs. (1974) ;2: (4):409–19. https://doi.org/10.1177/109019817400200407 |
[12] | Crawford JO , Berkovic D , Erwin J , Copsey SM , Davis A , Giagloglou E , Yazdani A , Hartvigsen J , Graveling R , Woolf A . Musculoskeletal health in the workplace. Best Practice & Research Clinical Rheumatology. (2020) ;34: (5):101558. https://doi.org/10.1016/j.berh.2020.101558 |
[13] | Bontrup C , Taylor WR , Fliesser M , Visscher R , Green T , Wippert P-M , Zemp R . Low back pain and its relationship with sitting behaviour among sedentary office workers. Applied Ergonomics. (2019) ;81: :102894. https://doi.org/10.1016/j.apergo.2019.102894 |
[14] | Pereira M , Comans T , Sjøgaard G , Straker L , Melloh M , O’Leary S , Chen X , Johnston V . The impact of workplace ergonomics and neck-specific exercise versus ergonomics and health promotion interventions on office worker productivity: A cluster-randomized trial. Scandinavian Journal of Work, Environment & Health. (2019) ;45: (1):42–52. |
[15] | Barcenilla A , March LM , Chen JS , Sambrook PN . Carpal tunnel syndrome and its relationship to occupation: A meta-analysis. Rheumatology. (2012) ;51: (2):250–61. https://doi.org/10.1093/rheumatology/ker108 |
[16] | Heller-Ono A . A prospective study of a macroergonomics process over five years demonstrates significant prevention of workers’ compensation claims resulting in projected savings. Worksite International. (2014) . |
[17] | Leyshon R , Chalova K , Gerson L , Savtchenko A , Zakrzewski R , Howie A , Shaw L . Ergonomic interventions for office workers with musculoskeletal disorders: A systematic review. Work. (2010) ;35: (3):335–48. https://doi.org/10.3233/WOR-2010-0994 |
[18] | Loef B , van Oostrom SH , van der Noordt M , Lifelines Corona Research initiative, Proper KI. Working from home during the COVID-19 pandemic and its longitudinal association with physical activity and sedentary behavior. Scandinavian Journal of Work, Environment & Health. 2022. https://doi.org/10.5271/sjweh.4027 |
[19] | Gilson N , Coenen P , Hallman D , Holtermann A , Mathiassen SE , Straker L . Postpandemic hybrid work: Opportunities and challenges for physical activity and public health. British Journal of Sports Medicine. 2022. bjsports-2022-105664. https://doi.org/10.1136/bjsports-2022-105664 |
[20] | Marroquín B , Vine V , Morgan R . Mental health during the COVID-19 pandemic: Effects of stay-at-home policies, social distancing behavior, and social resources. Psychiatry Research. (2020) ;293: :113419. https://doi.org/10.1016/j.psychres.2020.113419 |
[21] | Martínez-López EJ , Hita-Contreras F , Moral-García JE , Grao-Cruces A , Ruiz JR , Redecillas-Peiró MT , Martínez-Amat A . Association of low weekly physical activity and sedentary lifestyle with self-perceived health, pain, and well-being in a Spanish teenage population. Science & Sports. (2015) ;30: (6):342–51. https://doi.org/10.1016/j.scispo.2015.04.007 |
[22] | Celik S , Celik K , Dirimese E , Taşdemir N , Arik T , Büyükkara ı . Determination of pain in musculoskeletal system reported by office workers and the pain risk factors. International Journal of Occupational Medicine and Environmental Health. (2017) . https://doi.org/org/10.13075/ijomeh.1896.00901 |
[23] | Karingada KT , Sony M . Demonstration of the relationship between MSD and online learning during the COVID-19 pandemic. Journal of Applied Research in Higher Education. (2022) ;14: (1):200–22. https://doi.org/10.1108/JARHE-08-2020-0269 |
[24] | Sonne M , Villalta DL , Andrews DM . Development and evaluation of an office ergonomic risk checklist: ROSA – Rapid office strain assessment. Applied Ergonomics. (2012) ;43: (1):98–108. https://doi.org/10.1016/j.apergo.2011.03.008 |
[25] | MacLean KFE , Neyedli HF , Dewis C , Frayne RJ . The role of at home workstation ergonomics and gender on musculoskeletal pain. Work. (2022) ;71: (2):309–18. https://doi.org/10.3233/WOR-210692 |
[26] | Black NL , St-Onge S . Measuring pandemic home-work conditions to determine ergonomic recommendation relevance. Work. (2022) ;71: (2):299–308. https://doi.org/10.3233/WOR-210726 |
[27] | Bloom NA . Why working from home will stick. National Bureau of Economic Research Working Paper Series. (2021) . |

