1. Introduction
Since COVID-19, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was discovered and evolved into a pandemic, it has become a source of interest for numerous studies [
1,
2]. Initially, the SARS-CoV-2 infection was considered to compromise lung function only, but subsequently, several studies showed that many other organs could be involved, the kidneys in particular [
3,
4]. The main symptoms of SARS-CoV-2 infection are observed 2–14 days after exposure. Symptoms include fever, cough, and difficulty breathing [
5]. A severe complication of the disease is progressive respiratory failure, and death may occur in 3.4% of the infected patients [
6]. As more studies are becoming available, the knowledge of those categories of patients at increased risk of hospitalization and poor outcomes is now improving. Chronic kidney disease (CKD) has been shown to be a comorbidity associated with reduced survival in patients hospitalized for COVID-19 disease [
7,
8].
Few data are available about COVID-19 disease and arrhythmias, in particular atrial fibrillation (AF) [
9], and even less is known about this phenomenon in CKD patients [
10].
As such, the aim of the study was to investigate the role of CKD on in-hospital mortality and on incident AF in patients infected with SARS-CoV-2. The incidence of acute kidney injury (AKI) was also assessed.
2. Materials and Methods
2.1. Study Design
This multicenter study included two large hospitals in Northern Italy, the San Gerardo Hospital in Monza and the Niguarda Hospital in Milan. Adult (≥18 years of age) patients diagnosed with COVID-19 and admitted in the two centers from 27 February 2020 to 3 January 2021 were included in the study. Clinical data were merged with the hospital lab data-base and patients with at least one creatinine test taken within three days from admission were included in the study. Participants were followed-up until the first occurrence of either hospital discharge, transfer to another facility, or death.
The study (STORM) was approved by the National Institutional Review Board (Spallanzani Hospital), ClinicalTrials.gov: NCT04424992.
2.2. Renal Function Estimation
Serum creatinine measurements were used to calculate the estimated Glomerular Filtration Rate (eGFR) by using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [
11]. Chronic kidney disease was defined as eGFR < 60 mL/min. Patients with eGFR between 30 and 59 mL/min were considered to have moderate CKD and those with eGFR < 30 mL/min to have severe CKD.
2.3. Definition of Covariates
Study covariates included age, sex, history of comorbidities, and blood chemistry parameters. The comorbidities that were taken into consideration were ischemic heart disease, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, and diabetes. The history of AF and the percentage of permanent AF were included among the comorbidities as well. Blood chemistry parameters included, apart from creatinine, white blood cell (WBC) count, hemoglobin, hematocrit, platelets count, lymphocytes, C-reactive protein (CRP), urea, sodium, and potassium.
2.4. End-Points
The primary end-points were all-cause mortality and incident AF, defined as the first appearance of an AF episode during a hospital stay. The secondary end-point was AKI, defined as an increase in serum creatinine (SCr) by ≥0.3 mg/dL observed within 48 h; or an increase in SCr to ≥1.5 times the baseline creatinine value [
12].
2.5. Statistical Analysis
The study population was subdivided into three groups: normal renal function, moderate CKD, and severe CKD, according to eGFR (>60, 30–59, and <30 mL/min, respectively). Continuous data were described by medians and quartiles (first-third Q1–Q3) and compared using the Kruskal–Wallis test by ranks, while categorical data were described by counts and percentages and compared by the Chi-square (χ2) test. Chronic kidney disease group was defined at each SCr measurement, and CKD stage at admission and at the last measurement before discharge was defined in subjects with at least two creatinine measurements.
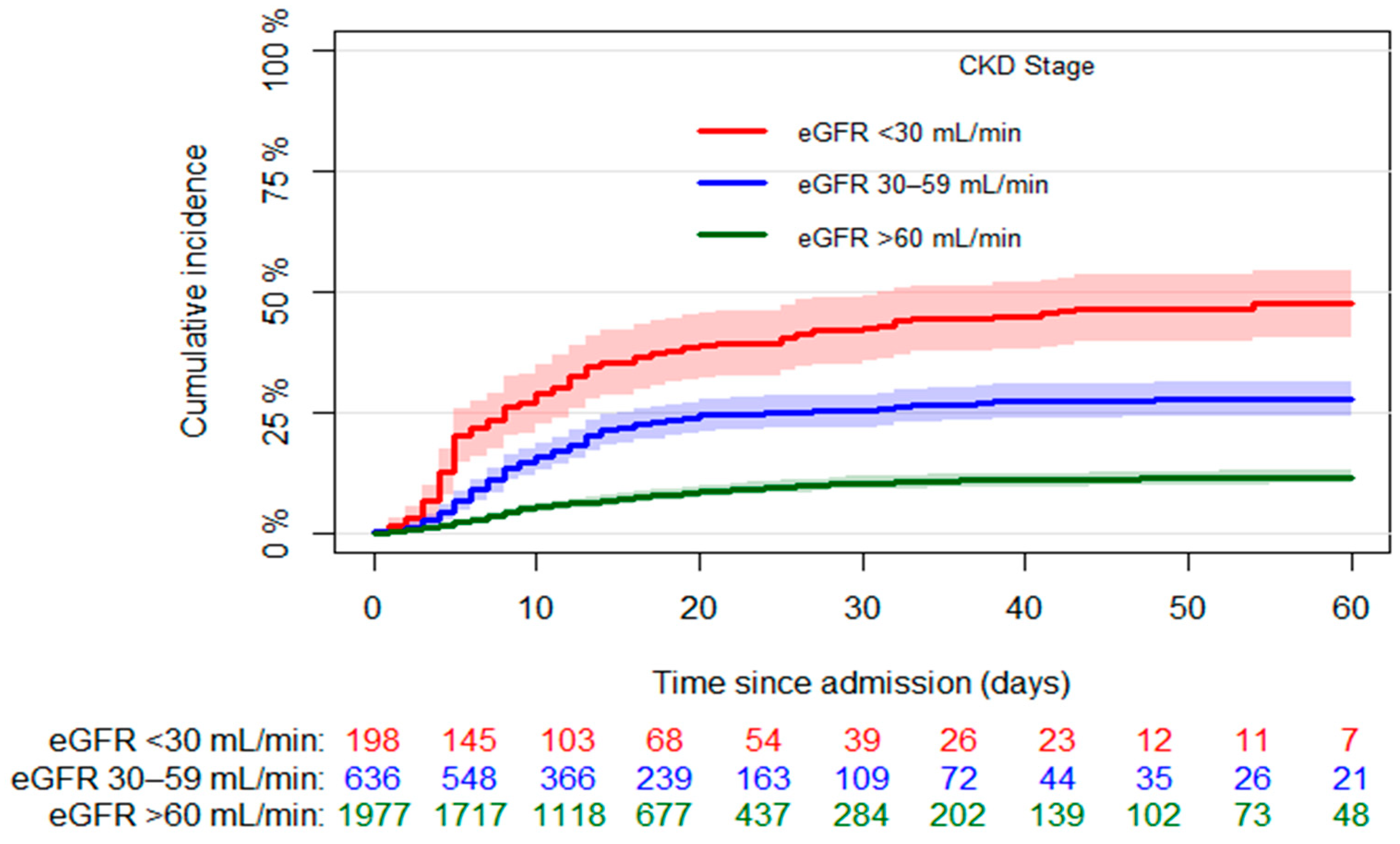
The Aalen–Johansen estimator was used to estimate the crude cumulative incidence of mortality accounting for discharge as competing event, and the Gray test was used to test the null hypothesis of no difference in mortality among the three groups. A cause-specific Cox proportional-hazards regression model was used for investigating the association between CKD groups and all-cause mortality. Logistic regressions were applied to evaluate the association of CKD with the occurrence of AF and AKI during hospitalization. Patients with permanent AF were excluded from the model on AF, while patients with only one SCr measurement were excluded from the AKI model.
Potential confounders considered in the models were age, sex, ischemic heart disease, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, diabetes, platelet count, and plasma concentration of hemoglobin, C-reactive protein and potassium. Odds ratios (ORs) or Hazard Ratios (HRs) with 95% confidence intervals (CIs) were reported. SAS 9.4 was used for the statistical analyses and the first type error was set at 0.05 (two-tailed).
4. Discussion
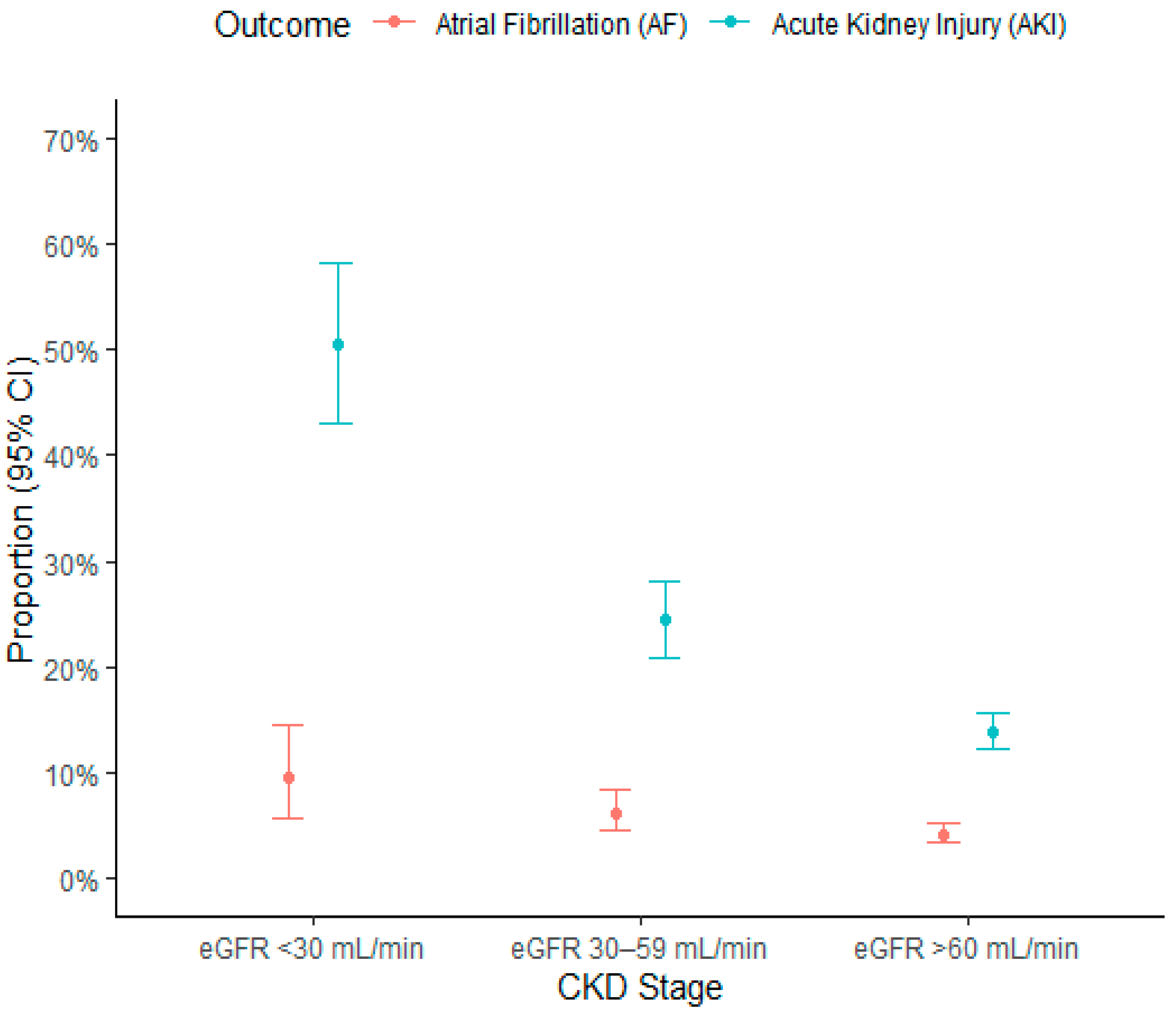
In a large population of patients hospitalized for COVID-19 disease, the presence of severe CKD on admission is an independent predictor of in-hospital mortality. The number of cases of incident AF increases as eGFR decreases, but renal function does not predict incident AF after correction for possible confounders. In contrast, incident AF is significantly associated with the onset of AKI.
Approximately one third of the study population had CKD at hospital admission, a finding in agreement with that described in other studies, that have reported a prevalence of CKD in COVID-19 patients between 22 and 38% [
13,
14]. The incidence of in-hospital mortality in this study was 18%. As already described by other authors [
15,
16,
17], the presence of reduced renal function increases mortality rate. In most studies, CKD is defined as the presence of eGFR <60 mL/min, with no further differentiation between the various stages of renal disease. Importantly, in our study, a significant increase in mortality was evident as the stage of CKD worsened (from 28% in patients with moderate CKD to 48% in those with severe CKD). After adjustment for age and comorbidities, the presence of eGFR between 30 and 59 mL/min was significantly associated with a 30% increase in mortality, and that of eGFR < 30 mL/min doubled the risk of death. When factors related to the severity of COVID-19 disease were also included in the model, only severe CKD and not moderate CKD remained an independent predictor of reduced in-hospital survival (HR 1.74). When incident AKI was added to the final survival model, it was a predictor of mortality, whereas CKD was no longer so. This finding strongly suggests that AKI is a mediator of mortality in COVID-19 disease, particularly in patients with CKD at baseline: CKD patients who die experience an abrupt impairment of renal function before death. In addition, some patients who undergo AKI die even if they show normal eGFR at baseline. Previously, a meta-analysis including 26 studies (
n = 5497 patients) showed that, in COVID-19 patients, the presence of AKI was associated with a more than 10-fold increased risk of mortality [
18]. An interesting finding of our study is the strong association between higher potassium values and mortality. Various studies have described hyperkalemia as a risk factor for survival in populations with several types of heart or kidney diseases. [
19,
20,
21]. The present study shows that this relationship is also confirmed in COVID-19 patients, independently of the presence of CKD.
Atrial fibrillation is a frequently occurring arrhythmia in patients with CKD [
22,
23,
24] and an increased incidence has been described in critically ill patients [
25]. The presence of pre-existing CKD is by itself a risk factor for AF in patients with acute sepsis [
26]. Few authors have studied the association between AF and COVID-19 disease. In patients hospitalized in cardiology wards for Sars-CoV-2 infection, the Cardio-COVID-Italy study showed an incidence of in-hospital AF of 12.5% [
27], while García-Granja et al. observed an incidence of 10.4% [
9]. Russo et al. found that in patients with COVID-19 admitted to emergency department, the incidence of AF was higher, equal to 17.1% [
10]. To our knowledge, there are very few data about the relationship between incident AF and renal function in COVID-19 patients. Russo et al. showed an association between CKD and incident AF in patients admitted in emergency units for COVID-19 disease, which, however, was not confirmed after adjustment for possible confounders [
10]. As expected, CKD patients in our study population had a higher prevalence of a positive history of AF. Episodes of incident AF increased as eGFR decreased, approaching 10% in patients with eGFR < 30 mL/min. This phenomenon was closely associated with the higher age of patients with reduced renal function (median 78 vs. 59 years of age). However, it is interesting to point out that in our population, when age was removed from the confounding factors in the multivariable model, a significant association with a higher incidence of AF was found only for the presence of CKD and not for the cardiac comorbidities. It is likely that the factors that predisposed CKD patients to be more liable to AF were only indirectly associated with the presence of reduced eGFR (older age, higher prevalence of heart disease, frequent presence of structural remodeling and cardiac fibrosis) and that this is the reason why CKD, although associated with a higher incidence of AF, was not found to be an independent predictive factor. In our study population, incident AF did not have an impact on in-hospital mortality, however, it was closely associated with the onset of AKI, which in turn appears to be an important mediator of mortality. It will be interesting to see whether in-hospital AF might have an effect on patients’ long-term survival after discharge.
The incidence of AKI in our patients was 19%, in agreement with the incidence reported in previous studies that ranges from 18% to 30.6% [
28,
29]. Various studies have described AKI in COVID-19 patients and the factors associated with this outcome [
30,
31]. This phenomenon is probably underestimated in our population. In fact, we see that a percentage of patients (12%) improved their CKD stage at discharge, suggesting that these are individuals who arrived in the emergency department with an ongoing AKI that resolved as the disease-causing admission resolved. Understanding the true incidence of COVID-19-related AKI is important, as our data demonstrated that patients who experienced an AKI event left the hospital with worsened kidney function more often than hospitalized patients without AKI. Our results indicate lower hemoglobin levels and higher C-reactive protein values as factors that may be associated with in-hospital AKI, suggesting the importance of considering subjects with low hematocrit with special care, especially in case of elevated inflammatory indices. A new and interesting result of the present study is the association between AKI and incident AF. It has been previously described that the arrhythmia most frequently associated with AKI in the intensive care units is AF [
25]. The onset of AF in critically ill patients is an independent predictor of AKI [
32,
33]; in turn, the incidence of AF is almost double in critically ill patients who suffered AKI compared to those with normal renal function [
34]. In our population, the risk of AKI is two and a half times higher in patients with incident AF. One reason could be that the onset of arrhythmia creates hemodynamic instability, with a reduction in left ventricular ejection fraction and a consequent drop in renal perfusion. From our results, it seems that the subjects at greater risk of experiencing AKI are those with lower hemoglobin values and higher indices of inflammation. It is possible to hypothesize that the association of the three factors (anemia, inflammation, and arrhythmia) may constitute a critical clinical situation for the onset of AKI.
In conclusion, although the data were collected retrospectively, our study provides some new information that may be clinically useful in understanding the complex relationship between kidney function and Sars-CoV-2 infection. The mortality rate from COVID-19 is not only higher in CKD patients (with eGFR< 60 mL/min), but it also increases significantly when moving from moderate to severe CKD. In addition, patients who underwent AKI during hospitalization had a doubled risk of death. COVID-19 appears to increase the incidence of in-hospital AF, particularly in patients with CKD, and, in turn, patients who experience an episode of in-hospital AF are also more likely to suffer from AKI.


 ,
, 
{kind=link}
{kind=link}

