
Acute Renal Vein Thrombosis Following COVID-19 in a Lupus Patient: A Case Report and Review of the Literature
 , ,
, ,
Abstract
:1. Introduction
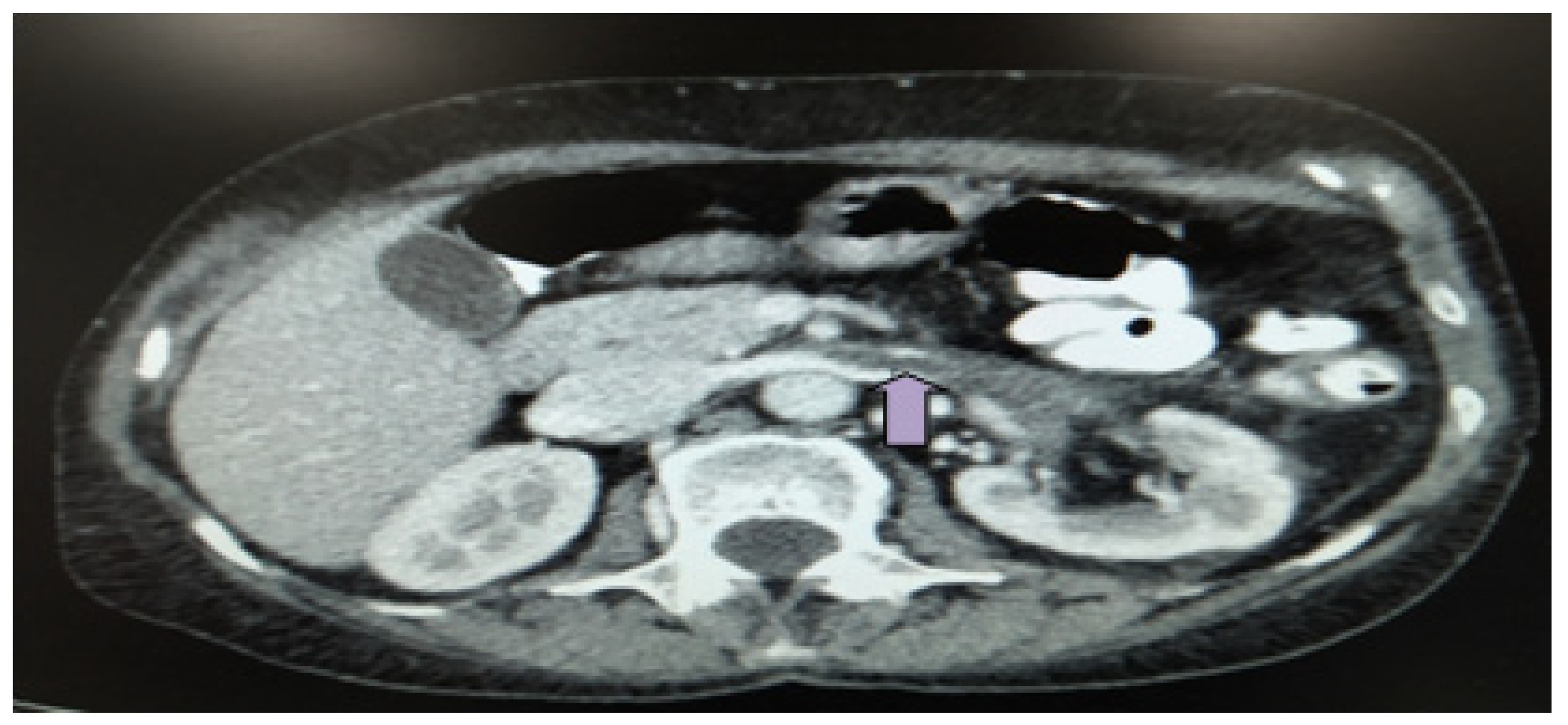
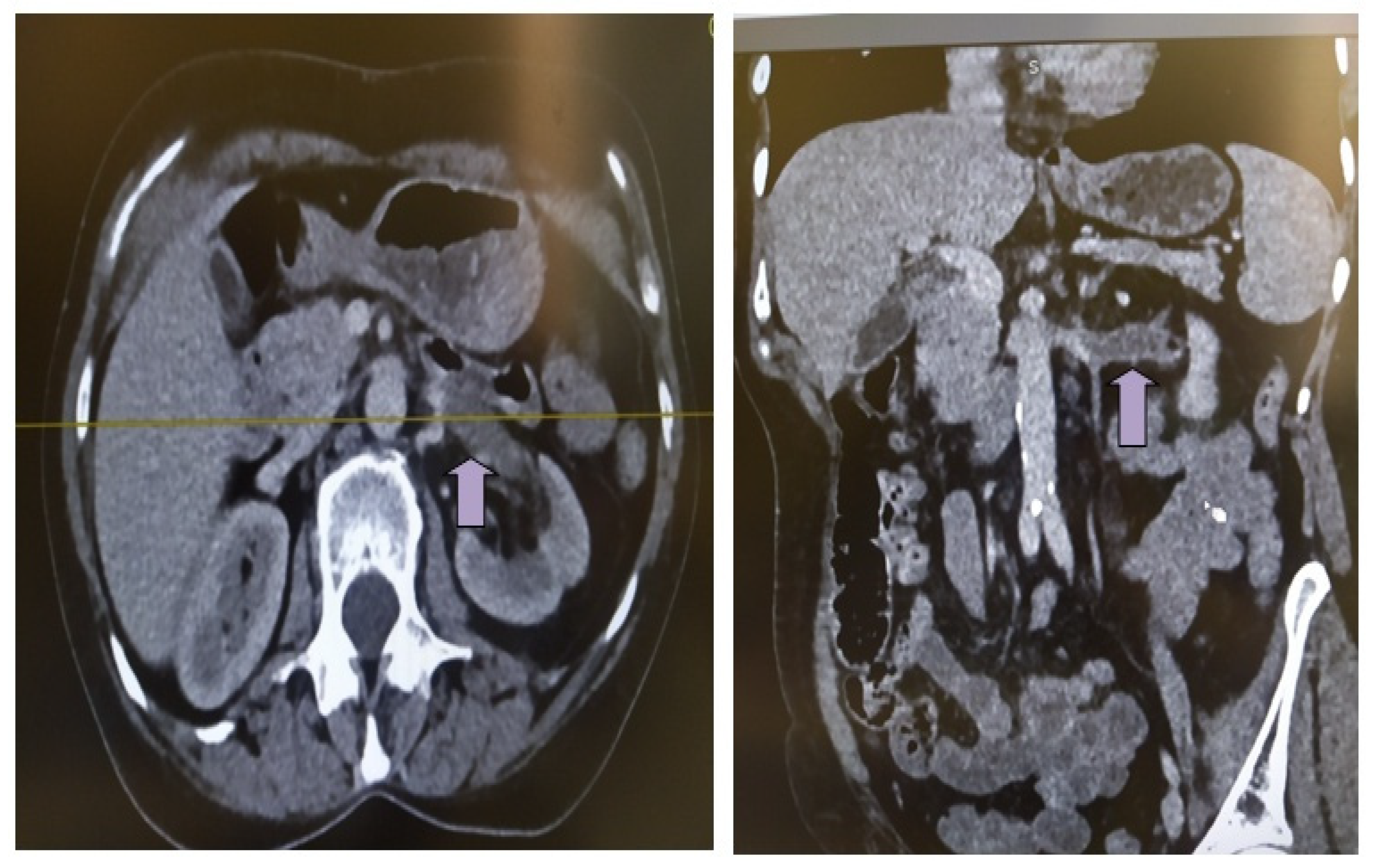
2. Case Description
3. Methods
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kichloo, A.; Dettloff, K.; Aljadah, M.; Albosta, M.; Jamal, S.; Singh, J.; Wani, F.; Kumar, A.; Vallabhaneni, S.; Khan, M.Z. COVID-19 and Hypercoagulability: A Review. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620962853. [Google Scholar] [CrossRef] [PubMed]
- Lowenstein, C.J.; Solomon, S.D. Severe COVID-19 Is a Microvascular Disease. Circulation 2020, 142, 1609–1611. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; et al. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef]
- Satturwar, S.; Fowkes, M.; Farver, C.; Wilson, A.M.; Eccher, A.; Girolami, I.; Pujadas, E.; Bryce, C.; Salem, F.; El Jamal, S.M.; et al. Postmortem Findings Associated With SARS-CoV-2: Systematic Review and Meta-analysis. Am. J. Surg. Pathol. 2021, 45, 587–603. [Google Scholar] [CrossRef]
- Basara Akin, I.; Altay, C.; ErenKutsoylu, O.; Secil, M. Possible radiologic renal signs of COVID-19. Abdom. Radiol. 2021, 46, 692–695. [Google Scholar] [CrossRef]
- Takamatsu, C.; Devis, P.; Tolouian, R. COVID-19 and renal infarct: To be or not to be on anticoagulation. Clin. Nephrol. Case Stud. 2021, 9, 117–122. [Google Scholar] [CrossRef]
- Xu, J.J.; Samaha, D.; Mondhe, S.; Massicotte-Azarniouch, D.; Knoll, G.; Ruzicka, M. Renal infarct in a COVID-19-positive kidney-pancreas transplant recipient. Am. J. Transpl. 2020, 20, 3221–3224. [Google Scholar] [CrossRef]
- Añazco, P.H.; Balta, F.M.; Córdova-Cueva, L. Bilateral renal infarction in a patient with severe COVID-19 infection. J. Bras. Nefrol. 2021, 43, 127–131. [Google Scholar] [CrossRef]
- Singh, T.; Chaudhari, R.; Gupta, A. Renal artery thrombosis and mucormycosis in a COVID-19 patient. Indian J. Urol. 2021, 37, 267–269. [Google Scholar] [CrossRef]
- El Shamy, O.; Munoz-Casablanca, N.; Coca, S.; Sharma, S.; Lookstein, R.; Uribarri, J. Bilateral Renal Artery Thrombosis in a Patient With COVID-19. Kidney Med. 2021, 3, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Anwar, S.; Siddiqui, F.S.; Shabih, S.; Manchandani, U.; Dalezman, S. Renal artery thrombosis in COVID-19. IDCases 2020, 22, e00968. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Liu, Q.; Wang, R.; Chen, R.; Ao, Q.; Wang, X.; Zhang, J.; Deng, F.; Feng, Y.; Wang, G.; et al. Clinicopathologic Features of COVID-19: A Case Report and Value of Forensic Autopsy in Studying SARS-CoV-2 Infection. Am. J. Forensic. Med. Pathol. 2021, 42, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Daniel, E.; Sekulic, M.; Kudose, S.; Kubin, C.; Ye, X.; Shayan, K.; Patel, A.; Cohen, D.J.; Ratner, L.E.; Santoriello, D.; et al. Kidney allograft biopsy findings after COVID-19. Am. J. Transpl. 2021, 21, 4032–4042. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Ghosh, R.; Furment, M.M. Case Report: COVID-19 Associated Renal Infarction and Ascending Aortic Thrombosis. Am. J. Trop. Med. Hyg. 2020, 103, 1989–1992. [Google Scholar] [CrossRef] [PubMed]
- Bonello, E.C.; Casha, R.; Xerri, T.; Bonello, J.; Fsadni, C.; Azzopardi, C.M. Multiorgan thrombosis as a complication of COVID-19 pneumonia. BMJ Case Rep. 2021, 14, e243953. [Google Scholar] [CrossRef] [PubMed]
- Ammous, A.; Ghaffar, M.A.; El-Charabaty, E.; El-Sayegh, S. Renal infarction in COVID-19 patient. J. Nephrol. 2021, 34, 267–268. [Google Scholar] [CrossRef] [PubMed]
- Belfort, D.S.P.; Marcondes-Braga, F.G.; Mangini, S.; Cafezeiro, C.R.F.; Furlan, D.A.G.; Bacal, F. Aortic and Renal Artery Thrombosis as the First Clinical Manifestation of COVID-19 in a Heart Transplant Recipient. Arq. Bras. Cardiol. 2021, 117, 1045–1047. [Google Scholar] [CrossRef]
- Post, A.; den Deurwaarder, E.S.G.; Bakker, S.J.L.; de Haas, R.J.; van Meurs, M.; Gansevoort, R.T.; Berger, S.P. Kidney Infarction in Patients With COVID-19. Am. J. Kidney Dis. 2020, 76, 431–435. [Google Scholar] [CrossRef]
- Mantica, G.; De Rose, A.F. Renal infarction in a COVID-19 patient. Pan Afr. Med. J. 2020, 37, 182. [Google Scholar] [CrossRef]
- Tascón, G.C.; Chiriboga, D.E.S.; Ramos, R.L.; Díaz, D.D.; Ruiz, C.R.; Procaccini, F.L.; Aguilera, E.T.; Navarro, J.A.M.; Gómez, B.M.; Rivas, N.M.; et al. Infarto renal enpaciente con COVID-19 [Renal infaction in a patient with COVID-19]. Nefrologia 2021, 41, 84–87. (in Spanish). [Google Scholar] [CrossRef]
- Mavraganis, G.; Ioannou, S.; Kallianos, A.; Rentziou, G.; Trakada, G. A COVID-19 Patient with Simultaneous Renal Infarct, Splenic Infarct and Aortic Thrombosis during the Severe Disease. Healthcare 2022, 10, 150. [Google Scholar] [CrossRef] [PubMed]
- Jana, K.; Janga, K.C.; Greenberg, S.; Kumar, K. Bilateral renal infarction with COVID-19 pneumonia: A case report. Oxf. Med. Case Rep. 2021, 2021, omab121. [Google Scholar] [CrossRef] [PubMed]
- Varner, K.B.; Cox, E.J. COVID-19 as the cause of thrombosis: Recognising COVID-19 infection in apparently asymptomatic patients. BMJ Case Rep. 2021, 14, e241027. [Google Scholar] [CrossRef] [PubMed]
- Ramteke, V.V.; Tayade, A.; Belekar, V.; Barokar, R.; Rathi, V. Bilateral Renal Infarcts in a Patient with COVID-19 Pneumonia. Indian J. Nephrol. 2021, 31, 414–415. [Google Scholar] [CrossRef]
- Tantisattamo, E.; Dafoe, D.C.; Ferrey, A.J.; Ichii, H.; Lee, R.A.; Zuckerman, J.E.; Sisk, A.E.J.; Farzaneh, T.; Guccione, J.; Kabutey, N.-K.; et al. Kidney allograft infarction associated with transplant renal artery stenosis in a COVID-19 kidney transplant recipient. Clin. Nephrol. Case Stud. 2021, 9, 93–104. [Google Scholar] [CrossRef]
- Dimosiari, A.; Patoulias, D.; Michailidis, T.; Dimitroulas, T. How Should Concurrent Arterial and Venous Thrombosis Associated With SARS-CoV-2 Infection Be Managed? Eur. J. Case Rep. Intern. Med. 2022, 9, 003366. [Google Scholar] [CrossRef]
- Sethi, S.; Mehta, S.; Mahajan, R. Coronavirus Disease 2019 Infection Presenting with Renal Infarction: A Rare Case Report. Saudi J. Kidney Dis. Transpl. 2021, 32, 865–868. [Google Scholar]
- Ramanathan, M.; Chueng, T.; Fernandez, E.; Gonzales-Zamora, J. Concomitant renal and splenic infarction as a complication of COVID-19: A case report and literature review. Infez. Med. 2020, 28, 611–615. [Google Scholar]
- Huang, H.; Lin, C.; Chen, Y.; Wu, X.; Lin, M.; Chen, S.; Li, K. Renal artery thrombosis in SARS-CoV-2 infection: A case report. BMC Nephrol. 2022, 23, 175. [Google Scholar] [CrossRef]
- Varma, P.P.; Kute, V.B.; Bajpai, G. Renal graft artery thrombosis following COVID-19 infection. Nephrology 2021, 26, 932–933. [Google Scholar] [CrossRef] [PubMed]
- Berrichi, S.; Bouayed, Z.; Berrajaa, S.; Mezzeoui, S.E.; Moujahid, A.; Nasri, S.; Bkiyar, H.; Skiker, I.; Housni, B. Acute limb ischemia with concomitant splenic and renal infarcts: Thromboembolic events revealing COVID-19. Ann. Med. Surg. 2021, 68, 102646. [Google Scholar] [CrossRef]
- Jentzsch, M.S.; Hsueh, L.; Pallapati, K.J.; Mayans, K. Abdominal Pain Due to Renal Infarction: An Unexpected Presentation of COVID-19. Rhode Isl. Med. J. 2021, 104, 16–19. [Google Scholar]
- Farias, L.A.B.G.; Cruz, E.A.; Silva, A.M.H.P.D.; Almeida, T.Í.F. Renal infarction in a patient with Coronavirus Disease 2019: Another rare thrombotic event. Rev. Soc. Bras. Med. Trop. 2021, 54, e0038–e2021. [Google Scholar] [CrossRef] [PubMed]
- Mocerino, R.; Kumar, N. Acute Abdominal Pain in a COVID-19 Patient. Kidney360 2020, 1, 584–585. [Google Scholar] [CrossRef]
- Veterano, C.; Antunes, I.; Coelho, A.; Silva, I.; Almeida, R.; Pinto, P.S. Endovascular Treatment of Renal Artery Thrombosis in Living-Donor Kidney Transplant Recipient with Severe COVID-19 Disease. J. Endovasc. Ther. 2022, 29, 966–970. [Google Scholar] [CrossRef]
- Al-Mashdali, A.F.; Alwarqi, A.F.; Elawad, S.M. Simultaneous renal infarction and splenic infarction as a possible initial manifestation of COVID-19: A case report. Clin. Case Rep. 2021, 9, e04819. [Google Scholar] [CrossRef]
- Kenizou, D.; Perrin, C.; Harzallah, I.; Bresson, D.; Allimant, P.; Calcaianu, M.; Lawson, B.; Morisset, B.; Zuily, S.; Jacquemin, L.; et al. Multiple Arterial Thrombosis in a 78-Year-Old Patient: Catastrophic Thrombotic Syndrome in COVID-19. CJC Open 2021, 3, 198–200. [Google Scholar] [CrossRef]
- Imoto, W.; Kaga, S.; Noda, T.; Oshima, K.; Mizobata, Y.; Kakeya, H. Coronavirus disease with multiple infarctions. QJM 2020, 113, 907–908. [Google Scholar] [CrossRef]
- Fluss, G.; Cranwell, V.; Rao, A.; Lee, J.S.; Elshafey, R.; Wallack, M.; Finlay, D. COVID-19 Delta variant resulting in multi system thromboembolic disease. Ann. Vasc. Surg Brief. Rep. Innov. 2022, 2, 100101. [Google Scholar] [CrossRef]
- Horiguchi, T.; Tsukamoto, T.; Toyama, Y.; Sasaki, T.; Nakamura, T.; Sakurai, A.; Kuriyama, N.; Komatsu, S.; Shigeyasu, Y.; Ina, T.; et al. Fatal disseminated mucormycosis associated with COVID-19. Respirol. Case Rep. 2022, 10, e0912. [Google Scholar] [CrossRef]
- Kurien, A.A.; Srinivasaprasad, N.D.; Valavan, K.T. Renal infarction due to COVID-19-associated renal mucormycosis. Kidney Int. 2022, 101, 655. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, M.P.; Russo, G.M.; Gallo, L.; Atripaldi, U.; Tamburrini, S.; Caliendo, V.; Impieri, L.; Del Canto, M.T.; Ciani, G.; Parrella, P.; et al. Secondary Complications in COVID-19 Patients: A Case Series. Tomography 2022, 8, 1836–1850. [Google Scholar] [CrossRef]
- Al Mousa, S.S.; Ashraf, A.; Abdelrahman, A.M. Don’t overlook flank pain in apparently asymptomatic COVID-19 cases: A case report and literature review. Saudi Med. J. 2022, 43, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Vasquez Espinosa, W.A.; Santos Argueta, A.; Hurtado Tandazo, V.A.; Vasquez Espinosa, C.F. A Case Report of a Young Female With Renal Infarction Secondary to Breakthrough COVID Infection. Cureus 2022, 14, e25527. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Bector, G.; Jain, D.; Makkar, V.; Mehta, S. Renal Artery Thrombosis with Renal Infarction Secondary to COVID-19 Infection: A Rare Presentation. Indian J. Nephrol. 2022, 32, 191–192. [Google Scholar] [PubMed]
- Murray, N.P.; Fuentealba, C.; Reyes, E.; Salazar, A. Renal infarction associated with asymptomatic COVID-19 infection. Hematol. Transfus. Cell Ther. 2021, 43, 353–356. [Google Scholar] [CrossRef]
- Brem, F.L.; Tayef, T.A.A.; Rasras, H.; Mahi, O.E.; Ouafi, N.E.; Zakaria, B. Concomitant renal and splenic infarctions in a COVID-19-patient with a catastrophic thrombotic syndrome. Radiol. Case Rep. 2022, 17, 4030–4033. [Google Scholar] [CrossRef]
- Philipponnet, C.; Aniort, J.; Chabrot, P.; Souweine, B.; Heng, A.-E. Renal artery thrombosis induced by COVID-19. Clin. Kidney J. 2020, 13, 713. [Google Scholar] [CrossRef]
- Mancini, M.; Randazzo, G.; Piazza, G.; Moro, F.D. Arterial Thrombotic Complications in COVID-19: A Case of Renal Infarction. Biomedicines 2022, 10, 2354. [Google Scholar] [CrossRef]
- Asleson, L.; Zalabani, M.; Selim, M. A Case of Renal Vein Thrombosis Associated With COVID-19 Treated with Rivaroxaban. Cureus 2022, 14, e29491. [Google Scholar] [CrossRef]
- Mirfakhraee, H.; Larijani, S.S.; Zandieh, Z.; Tizmaghaze, A.; Olamaeian, F.; Tayebi, A.; Niksolat, M. Renal vein thrombosis in a recent COVID-19 patient; a case report. J. Ren. Inj. Prev. 2022, 12, e319972022. [Google Scholar] [CrossRef]
- Kincaid, K.J.; Simpkins, A.N. Failure of Anticoagulation to Prevent Stroke in Context of Lupus-Associated Anti-Phospholipid Syndrome and Mild COVID-19. J. Stroke Cerebrovasc. Dis. 2021, 30, 105817. [Google Scholar] [CrossRef]
- Yarkan Tuğsal, H.; İzdeş, S.; Küçükşahin, O. 20-Year-old female with fever, cough, and dyspnea: Acute lupus pneumonitis during the pandemic of coronavirus disease 2019 (COVID-19). Lupus 2021, 30, 1856–1862. [Google Scholar] [CrossRef] [PubMed]
- Aguirre-Alastuey, M.E.; Suárez-Díaz, S.; Rodríguez-Jerez, F.; Coto-Hernández, R.; Caminal-Montero, L. Venous thrombosis in a systemic lupus erythematosuspatient with antiphospholipid antibodies coinciding with mild COVID-19. Lupus 2021, 30, 172–174. [Google Scholar] [CrossRef]
- Nespola, M.; Sirignano, P.; Fermani, N.; Battocchio, C.; Tosti, F.; Pranteda, C.; Taurino, M. Treatment-Resistant Acute Upper Limb Ischemia in a Patient with Systemic Lupus Erythematous and Concomitant SARS-CoV-2 Infection: A Case Report. Ann. Vasc. Surg. 2021, 76, 289–292. [Google Scholar] [CrossRef]
- Plotz, B.; Castillo, R.; Melamed, J.; Nuovo, G.; Magro, C.; Rosenthal, P.; Belmont, H.M. Focal small bowelthrombotic microvascular injury in COVID-19 mediated by the lectin complement pathway masquerading as lupus enteritis. Rheumatology 2020, 60, e61–e63. [Google Scholar] [CrossRef]
- Mantovani Cardoso, E.; Hundal, J.; Feterman, D.; Magaldi, J. Con-comitant new diagnosis of systemic lupus erythematosus andCOVID-19 with possible antiphospholipid syndrome. Just a coincidence? A case report and review of intertwining pathophysiology. Clin. Rheumatol. 2020, 39, 2811–2815. [Google Scholar] [CrossRef] [PubMed]
- Kollias, A.; Kyriakoulis, K.G.; Lagou, S.; Kontopantelis, E.; Stergiou, G.S.; Syrigos, K. Venous thromboembolism in COVID-19: A systematic review and meta-analysis. Vasc. Med. 2021, 26, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Sauerberg, N.; Khan, Y.S. Renal Artery Thrombosis. 2022 May 3. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Oh, Y.K.; Yang, C.W.; Kim, Y.-L.; Kang, S.-W.; Park, C.W.; Kim, Y.S.; Lee, E.Y.; Han, B.G.; Lee, S.H.; Kim, S.-H.; et al. Clinical Characteristics and Outcomes of Renal Infarction. Am. J. Kidney Dis. 2016, 67, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Asghar, M.; Ahmed, K.; Shah, S.S.; Siddique, M.K.; Dasgupta, P.; Khan, M.S. Renal vein thrombosis. Eur. J. Vasc. Endovasc Surg. 2007, 34, 217–223. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, D.P. Renal manifestations of the antiphospholipid syndrome. Lupus 2005, 14, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Llach, F.; Papper, S.; Massry, S.G. The clinical spectrum of renal vein thrombosis: Acute and chronic. Am. J. Med. 1980, 69, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Kelddal, S.; Hvas, A.M.; Grove, E.L.; Birn, H. Safety and effectiveness of direct oral anticoagulants in patients with nephrotic syndrome: A report of 21 cases. BMC Nephrol. 2022, 23, 305. [Google Scholar] [CrossRef]
- Rodríguez, Y.; Novelli, L.; Rojas, M.; De Santis, M.; Acosta-Ampudia, Y.; Monsalve, D.M.; Ramírez-Santana, C.; Costanzo, A.; Ridgway, W.M.; Ansari, A.A.; et al. Autoinflammatory and autoimmune conditions at the crossroad of COVID-19. J. Autoimmun. 2020, 114, 102506. [Google Scholar] [CrossRef]
- Zhong, J.; Shen, G.; Yang, H.; Huang, A.; Chen, X.; Dong, L.; Wu, B.; Su, L.; Hou, X.; Song, S.; et al. COVID-19 in patients with rheumatic disease in Hubei province, China: A multicentre retrospective observational study. Lancet Rheumatol. 2020, 2, e557–e564. [Google Scholar] [CrossRef]
- Reyes Gil, M.; Barouqa, M.; Szymanski, J.; Gonzalez-Lugo, J.D.; Rahman, S.; Billett, H.H. Assessment of Lupus Anticoagulant Positivity in Patients with Coronavirus Disease 2019 (COVID-19). JAMA Netw. Open. 2020, 3, e2017539. [Google Scholar] [CrossRef]
- Sakthiswary, R.; Chuah, H.Y.; Chiang, K.S.; Liew, Y.S.; Muhammad Aizat, N.A. COVID-19 in systemic lupus erythematosus: A pooled analysis and systematic review of case reports and series. Lupus 2021, 30, 1946–1954. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before COVID-19 (2 Months Prior) | After COVID-19 (20 Days Prior) | Upon Presentation | Follow-Up (3 Months After) | |
|---|---|---|---|---|
| WBC (103/μL) | 9.700 | 9900 | 10.100 | 6.500 |
| Neut (103/μL) | 8.383 | |||
| Hgb(gr/dL) | 13 | 13.5 | 12 | 13.5 |
| PLT (103/μL) | 200.000 | 234.000 | 152.000 | 248.000 |
| CRP (mg/dL) | 4 | 9 | 85 | 5 |
| Serum Urea (mg/dL) | 61 | 72 | 56 | 270 |
| Serum Creat (mg/dL) | 1.1 | 1.2 | 1 | 1.1 |
| eGFR (mL/min/1.73 m2) | 52 | 47 | 58 | 52 |
| Na+ (mmol/L) | 143 | 143 | 138 | 142 |
| K+ (mmol/L) | 4.1 | 4.2 | 4.4 | 4.4 |
| Ca2+ (mg/dL) | 9.2 | 9.2 | 8.8 | 9.3 |
| alb (g/dL) | 3.3 | 3.4 | 3.5 | 3.6 |
| Urine | RBC 2–3/hpf | RBC 1–2/hpf | RBC 10–20/hpf, | RBC 2–3/hpf |
| WBC 0–2/hpf | WBC 1–2/hpf | WBC 0–2/hpf | WBC 1–2/hpf | |
| Proteinuria (mg/24 h) | 650 | NA | 850 | 900 |
| Author- Continent | S | Infarction Type (A/V) | Native/ Allograft | Gender -Age | SLE | CKD | AF | Unilateral /Bilateral |
|---|---|---|---|---|---|---|---|---|
| Kudose et al [4], USA | 1 | A | Na | M50 | N | N | N | U |
| Satturwar et al. [5], USA | 4 | A | Na | M52,M53, F48, F49 | N | N | N | 1B 3U |
| Akin et al. [6], AS | 1 | A | Na | M48 | N | N | N | U |
| Takamatsu et al. [7], USA | 1 | A | Na | M71 | N | N | N | B |
| Xu et al. [8], USA | 1 | A | Allo | M46 | N | Y | N | U |
| Añazco et al [9], SA | 1 | A | Na | F41 | N | N | N | B |
| Singh et al. [10], AS | 1 | A | Na | M32 | N | N | N | U |
| El Shamy et al. [11], USA | 1 | A | Na | F60 | N | N | Y | B |
| Acharya et al. [12], USA | 1 | A | Na | F77 | N | N | N | U |
| Ren et al. [13], AS | 1 | A | Na | F53 | N | N | N | U |
| Daniel et al [14], USA | 1 | A | Allo | M29 | N | Y | N | U |
| Mukherjee et al. [15], US | 1 | A | Na | M71 | N | N | N | U |
| Bonello et al. [16], EU | 1 | A | Na | M47 | N | N | N | B |
| Ammous et al. [17], USA | 1 | A | Na | M62 | N | N | N | U |
| Belfort et al. [18], USA | 1 | A | Na | M28 | N | N | N | U |
| Post et al. [19], EU | 2 | A A | Allo Na | M62 M58 | N N | Y N | N N | U U |
| Mantica et al. [20], EU | 1 | A | Na | F67 | N | N | N | U |
| Tascón et al. [21], EU | 1 | A | Na | M56 | N | N | N | U |
| Mavraganis et al. [22], EU | 1 | A | Na | M64 | N | N | N | U |
| Jana et al. [23], USA | 1 | A | Na | M37 | N | N | N | B |
| Varmer et al. [24], USA | 1 | A | Na | M46 | N | N | N | U |
| Rametke et al. [25], AS | 1 | A | Na | M66 | N | N | N | B |
| Tantisattamo et al. [26], USA | 1 | A | Allo | F33 | N | N | N | U |
| Dimosiari et al. [27], EU | 1 | A | Na | M75 | N | N | N | B |
| Sethi et al. [28], AS | 1 | A | Na | M62 | N | N | N | U |
| Ramanthan et al. [29], USA | 1 | A | Na | M54 | N | N | N | U |
| Huang et al. [30], AS | 1 | A | Na | M62 | N | N | N | U |
| Varma et al. [31], AS | 1 | A | Allo | M47 | N | N | N | U |
| Berrichi et al. [32], AFR | 1 | A | Na | M45 | N | N | N | B |
| Jentzsch et al. [33], USA | 1 | A | Na | F28 | N | N | N | U |
| Farias et al. [34], SA | 1 | A | Na | M37 | N | N | N | U |
| Mocerino et al. [35], USA | 1 | A | Na | F69 | N | N | N | U |
| Veterano et al. [36], EU | 1 | A | Allo | F56 | N | Y | N | U |
| Al-Mashdali et al. [37], AS | 1 | A | Na | M43 | N | N | N | U |
| Kenizou et al. [38], EU | 1 | A | Na | M78 | N | N | N | U |
| Imoto et al. [39], AS | 1 | A | Na | M64 | N | N | N | B |
| Fluss et al. [40], USA | 1 | A | Na | M60 | N | N | N | U |
| Horiguchi et al. [41], AS | 1 | A | Na | M58 | N | N | N | U |
| Kurien et al. [42], AS | 1 | A | Na | M32 | N | N | N | B |
| Belfiore et al. [43], EU | 1 | A | Na | F76 | N | N | N | B |
| Al Mousa et al. [44], AS | 1 | A | Na | M31 | N | N | N | U |
| Espinosa et al. [45], USA | 1 | A | Na | F21 | N | N | N | U |
| Jain et al. [46], AS | 1 | A | Na | M62 | N | N | N | U |
| Murray et al. [47], SA | 1 | A | Na | M25 | N | N | N | U |
| Brem et al. [48], AFR | 1 | A | Na | M59 | N | N | N | U |
| Philipponnet et al. [49], EU | 1 | A | Na | M52 | N | Y | N | U |
| Mancini et al. [50], EU | 1 | A | Na | M43 | N | N | N | U |
| Asleson et al. [51], USA | 1 | V | Na | F44 | N | N | N | U |
| Mirfakhraee et al. [52], AS | 1 | V | Na | M74 | N | N | N | U |
| Author- Continent | S | Gender -Age | SLE Duration | Prior History of APS | System Involvement | Immunological Factors | SLE Medications | Type of Coagulopathy |
|---|---|---|---|---|---|---|---|---|
| Kincaid et al. [53], USA | 1 | F43 | 10 years | Y | Neuropsychiatric | NA | HCQ, MMF, Oral CS, Warfarin | Acute ischemic cerebral stroke |
| Tuğsal et al. [54], AS | 1 | F20 | New-onset | N | Respiratory, pleural effusions, pericardial effusion | Positive ANA, anti-ds DNA | NA | Spleen infarct |
| Aguirre-Alastuey et al. [55], EU | 1 | F22 | 2 years | N | Arthritis, thrombocytopenia | Positive ANA, anti-ds DNA, aPL | HCQ MTX Oral CS aspirine | DVT, PE, Secondary APS |
| Nespola et al. [56], EU | 1 | F47 | NA | N | NA | Positive LA | Oral CS | Acute treatment-resistant recuurent upper limb ischemia |
| Plotz et al. [57], USA | 1 | F27 | 4 years | N | Haematological, Cutaneous, arthritis | Positive ANA, anti-ds DNA, anti-Ro, anti-La, Low c3,c4 | NA | Smallintestinalmicrovascularthrombosis |
| Mantovani et al. [58], USA | 1 | F18 | New-onset | N | Haematological, renal, respiratory, pleural effusions, pericardial effusion, and tamponade | NA | NA | DVT, Secondary APS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrou, D.; Sardeli, A.; Vlachoyiannopoulos, P.; Moschovaki-Zeiger, O.; Lionaki, S. Acute Renal Vein Thrombosis Following COVID-19 in a Lupus Patient: A Case Report and Review of the Literature. Life 2023, 13, 1252. https://doi.org/10.3390/life13061252
Petrou D, Sardeli A, Vlachoyiannopoulos P, Moschovaki-Zeiger O, Lionaki S. Acute Renal Vein Thrombosis Following COVID-19 in a Lupus Patient: A Case Report and Review of the Literature. Life. 2023; 13(6):1252. https://doi.org/10.3390/life13061252
Chicago/Turabian StylePetrou, Dimitra, Aggeliki Sardeli, Panayiotis Vlachoyiannopoulos, Ornella Moschovaki-Zeiger, and Sophia Lionaki. 2023. "Acute Renal Vein Thrombosis Following COVID-19 in a Lupus Patient: A Case Report and Review of the Literature" Life 13, no. 6: 1252. https://doi.org/10.3390/life13061252