Article Text

Abstract
Aims We performed an audit to evaluate the impact of the COVID-19 pandemic-related delay in the diagnosis of major cancers at a Pathology Unit of a Secondary Care Hospital Network in Italy.
Methods A comparison was made among the number of first cellular pathological diagnoses of malignancy made from the 11th to the 20th week of the years 2018–2020.
Results Cancer diagnoses fell in 2020 by 39% compared with the average number recorded in 2018 and 2019. Prostate cancer (75%) bladder cancer (66%) and colorectal cancer (CRC; 62%) had the greatest decrease. CRC was identified as carrying a potentially important diagnostic delay.
Conclusions For CRC corrective procedures (continuing mass screening tests; patient triage by family physicians; diagnostic procedures alternative to colonoscopy; predictive evaluation on biopsy samples) were advised. Our simple audit model is widely applicable to avoid pandemic-related delay in clinical diagnosis of cancer.
- clinical audit
- colorectal neoplasms
- diagnosis
- epidemiology
- infections
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The pandemic of COVID-19 started in Italy with 16 confirmed cases in Lumbardy on 21 February 2020; on 9 March (week 11 of the year) the Italian Prime Minister imposed a ‘national lockdown’; limitations ran up to 17 May 2020 (week 20).
The Marche administrative region had the highest Italian number of COVID-19 hospitalised patients/100 000 inhabitants.1 The pandemic increased the pressure on the Regional Healthcare System, mainly in its Emergency and Intensive Care Units, that resulted in the delay of many diagnostic and therapeutic procedures on non-critical patients; mass screening pathways for colorectal cancer (CRC) and cervical cancer were interrupted.
We performed a standards-based audit2 aimed at evaluating the impact of the pandemic-related delay in the cellular pathological diagnosis of cancers by recording the number first diagnoses of tumours during the weeks 11–20 of 2020, 2019 and 2018 at a Pathologic Anatomy Unit serving a Secondary Care Hospital Network in the Province of Macerata, Italy.
Materials and methods
The procedure for a standards-based2 audit was followed as specified below.
Identifying the problem
The heavy pressure on Health System due to the COVID-19 pandemic, along with the need to reduce the risk of disease spread inside crowded hospitals induced the American Society of Clinical Oncology to recommend that ‘any clinic visits that can be postponed without risk to the patient should be postponed’.3 The COVID-19 pandemic was also expected to affect the compliance of patients towards scheduled but deferrable diagnostic and therapeutic procedures.4 All the above were expected to decrease the number of cellular pathological diagnoses of malignancy, during the ‘lockdown’ period; the extent of the reduction could be assumed to be a diagnostic delay.
Defining standards and criteria
We retrieved the number of all first, cytopathological and histopathological diagnoses of primary malignancy and metastatic disease (from a known/unknown) malignancy made in weeks 11–20 of the years 2020, and 2018–2019 (given as an average). There was a focus on the most common cancers affecting Italian population (breast, prostate, lung, CRC, bladder, stomach, non-Hodgkin’s lymphoma, liver and skin-melanoma) according to the Global Cancer Observatory 2018.5 Histopathological prognostic indices were studied for the internal malignancies with the greatest diagnosis decrease in 2020.
Collecting data
The Anatomic Pathology Unit of the General Hospital of Macerata collects all the cellular pathology samples in a Secondary Care Hospital Network in the Province of Macerata, Italy. Patient data were retrieved by means of a Laboratory Information Management system (MyKey; A. Menarini Diagnostics, Florence, I) interfaced with the Regional Population Register. Italian authors were responsible for the anonymisation of data.
Analysing of data
Scientific two-dimension graphing and statistics software (Prism V.8.4.2, GraphPad Software, San Diego, California, USA).
Audit recommendations
Identifying critical areas of potentially dangerous delay in the first diagnosis of malignancy and suggesting possible corrective actions.
Reauditing
Planned, but awaiting data collection.
Results
The number of new, or first metastatic, diagnoses of malignancy recorded in the, 10 weeks, observation period was 300 in 2020 and, on average, 489 in 2018–2019, representing a decrease, in 2020 of 39%.
Table 1 shows that the reductions in cancer diagnosis varied considerably as follows: no reduction in metastatic cancers, pancreas cancer and skin melanoma; minimal in lung (2%); slight in stomach (10%); moderate in breast (26%) and most marked in colon-rectum (62%), bladder (66%) and prostate (75%).
Comparison between the number of new diagnoses of cancer made in the weeks 11–20 of 2020 with the number of diagnoses made in the same period of 2018 and 2019 (given as an average)
Regarding the prognostic indices among the most ‘underdiagnosed’ cancers, for prostate, the number of diagnoses of high-grade lesions (prostatic cancer grading groups 4 and 5)6 showed irrelevant variations (4.5 cases in 2018–2019; 4 cases in 2020), suggesting the reduction mainly involved low-grade and intermediate-grade lesions. Insufficient resections of bladder cancer and CRC were performed in the observation period of 2020 to allow reliable assessment of prognostic data.
Discussion
The number of new or first metastatic malignant diagnoses at a Secondary Care Hospital Network during the COVID-19 pandemic in Italy (weeks 11–20 of the year 2020) was substantially lower than the same period of the previous 2 years. Among internal malignancies, the drop in CRC diagnosis was considered the most important area for action.
The heavy pressure on health systems due to the COVID-19 pandemic has hopefully passed the peak in Europe. Current projections, however, indicate that the COVID-19-related disruption may last for 18 months or more7; thus, healthcare prioritisation and resource reallocation are warranted in order to minimise the negative impact of delayed diagnosis and therapy for oncological patients.
Sud et al 7 have estimated that even modest delays in surgery for cancer will incur significant impact on survival, with a delay of 3–6 months expected to mitigate 19%–43% of life-years gained by hospitalisation of an equivalent volume of admissions for community acquired COVID-19. Sud et al’s data,7 however, do not consider that further potentially avoidable cancer deaths may be due to the delay in clinical procedures aimed at achieving a cellular pathological diagnosis. We performed a not-for-cause standards-based audit2 aimed at evaluating the COVID-19-related diagnostic delay by comparing the number of new diagnoses of malignancy recorded during weeks 11–20 of 2018–2020 at the Anatomic Pathology Unit of Macerata Hospital. The Unit collects the cellular pathology samples of a Hospital Network covering 10732 miles with roughly 320 000 inhabitants and is composed by 1 primary and 3 secondary care hospitals with a total of 736 beds.
Our audit showed no reduction in new metastatic malignancy, in new pancreatic cancer, and in skin melanoma; and minimal and small reduction in lung and stomach cancers.
The new diagnoses of breast cancer were moderately reduced (26%), probably as a result of a specific strategy aimed at preserving the mass screening procedures.
Prostate and bladder cancer underwent the greatest reduction (75% and 66%, respectively); however, the former patients underwent a rigorous clinical triage, so the decrement exclusively involved low-grade and intermediate-grade malignancies. Since no adverse clinical outcome is associated with a 12-month delayed surgery even in high-risk prostatic cancers,8 the COVID-19-related diagnostic delay is expected to have a negligible clinical impact.
Regarding bladder cancer, our data are less clear but we emphasize the importance of the early clinical identification of patients with putatively muscle-invasive tumours, because delaying cystectomy by 90 days in ≥pT2 cases is associated with a higher pathologic stage and a worse prognosis.9
The 62% decrease in the number of diagnoses of CRC in our study is considered to be concerning. An observational cancer registry study, from Taiwan, on 39 000 newly diagnosed CRC found the risk of death significantly increased, across all cancer stages, depending on the time from diagnosis to treatment interval, as follows: compared to an interval ≤ 30 days, for 31–150 days HR 1.51; (95% CI 1.43 to 1.59); for ≥151 days 1.64; (95% CI 1.54 to 1.76).10
Considering this data and our audit findings, corrective actions appear to be most warranted for CRC. We have proposed the following: reintroduce mass screening by faecal occult blood test (and retain during any future lockdown conditions; promote the triage of patients by family physicians according to standard guidelines11; in case of excessive wait times for colonoscopy, consider CT colonography or double-contrast barium enema for patient triage; on adequate biopsy samples, assess the tumour grade and undertake preoperative evaluation of the predictive markers (immunohistochemistry for mismatch repair proteins; mutation analysis for KRAS, NRAS, BRAF and PIK3CA) based on their known prognostic value,12 are useful for clinical triage.
Ongoing reaudit may clarify the benefit (if any) of these procedures for patients with suspected CRC. Figure 1 summarises the methodology and the main results of the present study.
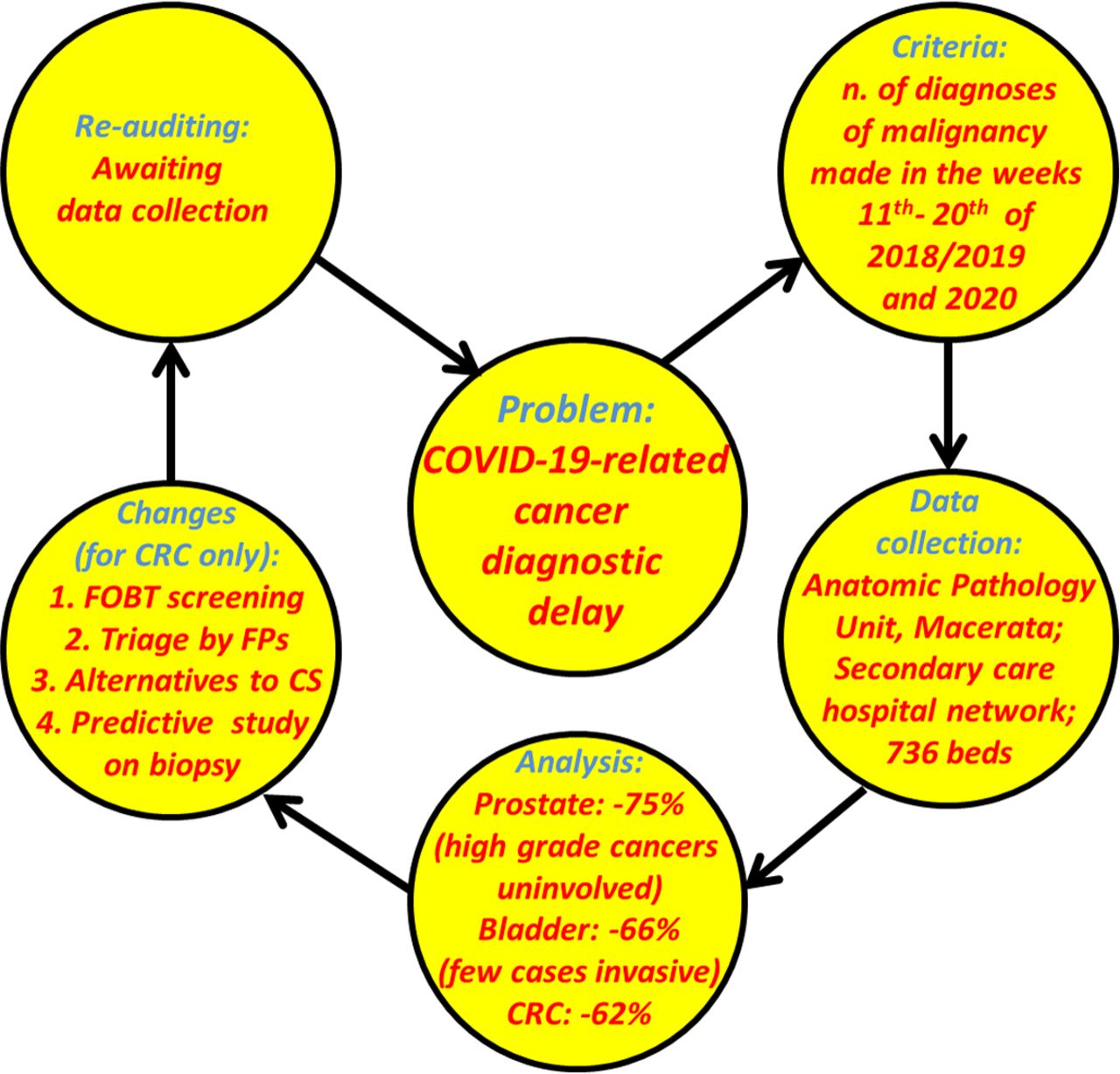
{kind=link}
The procedure and the main results of the present not-for-cause, standards-based internal audit (routine Quality Improvement review). CRC, colorectal cancer; CS, colonoscopy; FOBT, faecal occult blood test; FPs, family physicians.
In conclusion, our internal audit highlighted CRC as a major area for intervention in order to minimise the clinical impact of a diagnostic delay due to COVID-19-related dysfunctions. Our simple audit procedure, using cellular pathological diagnosis, can be universally applied, given the worldwide nature of the COVID-19 pandemic, so that local, regional and national healthcare systems can target the most relevant delays in cancer diagnosis.
Footnotes
Handling editor Runjan Chetty.
Contributors All the authors contributed to the study design and the manuscript preparation to a relevant extent.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.