
Evolution of the Clinical Profile and Outcomes of Unvaccinated Patients Affected by Critical COVID-19 Pneumonia from the Pre-Vaccination to the Post-Vaccination Waves in Italy

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
- Demographic characteristics (age, sex, and BMI);
- Smoking status (actual and former or never smokers);
- Comorbidities as arterial hypertension, obesity, diabetes, bronchial asthma, chronic obstructive pulmonary disease (COPD), malignancies, and others. The Charlson comorbidity index (CCI) was calculated by summing the assigned weighted score of 19 comorbid conditions: higher scores indicated a more severe condition and consequently a worse ten-year survival [15];
- Chest HRCT score according to Chung et al.: the total severity score, ranging from 0 to 20,was calculated by adding the score of each of the five lung lobes, as follows: score zero (no lobe involvement), score one (minimal involvement, 1–25%), score two (mild involvement, 26–50%), score three (moderate involvement, 51–75%), score four (severe involvement, 76–100%) [16];
- PaO2/FiO2 ratio and respiratory supports: non-invasive ventilation (NIV), continuous positive airway pressure (cPAP), high flow nasal cannula (HFNC), Venturi mask, or nasal cannula;
- Laboratory data: white blood cells (WBC) with neutrophil and lymphocyte percentages and neutrophil–lymphocyte ratio (NLR), C-reactive protein (CRP), interleukin (IL)-6, dimer D, procalcitonin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), nitrogen urea, creatinine, and glycemia;
- Days between the first positive SARS-CoV-2 RT-PCR test and the hospital admission and days of hospital stay;
- The occurrence of pulmonary embolism during the hospitalization;
- The exitus (death or survival).
Statistical Analysis
3. Results
3.1. No-Vax vs. Pre-Vax Group
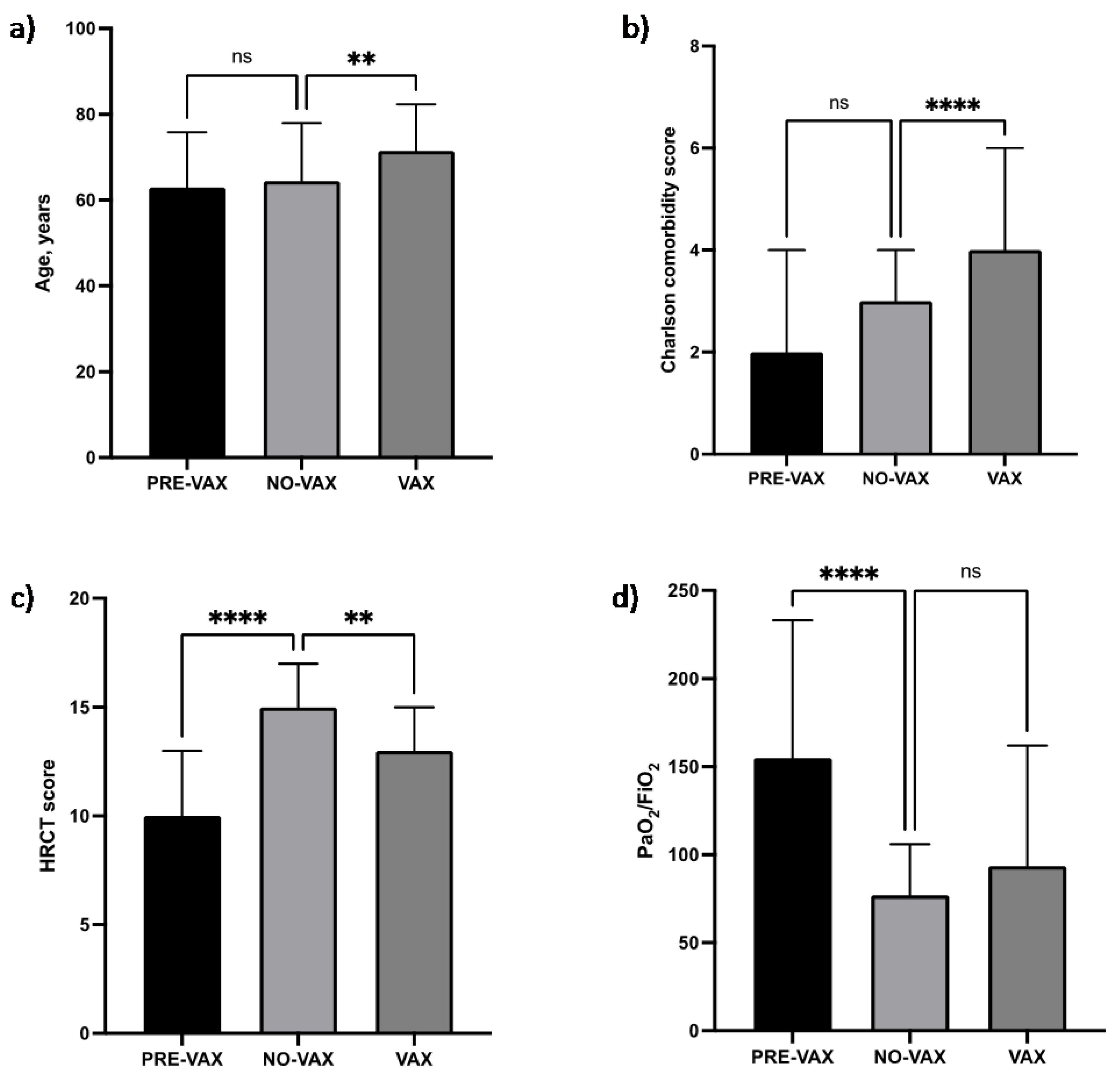
- There was no significant difference in age (Figure 1a) or BMI.
- In the No-Vax group, a significantly lower prevalence of the male gender was observed (p = 0.0007).
- The percentage of actual and former smokers was significantly higher in the No-Vax group (p = 0.0003).
- The Charlson comorbidity index (Figure 1b) and each comorbidity were not significantly different, except for arterial hypertension that was significantly less prevalent in the No-Vax group (p = 0.0041).
- The number of days between the onset of symptoms and the hospital admission was significantly higher in the No-Vax group (p = 0.000), and the No-Vax survivors needed a significantly shorter hospital stay (p = 0.0021).
- Upon hospital admission, No-Vax patients showed a significant greater involvement of lung parenchyma, as assessed by the HRCT Chung score (p < 0.0001) and a worse PaO2/FiO2 ratio (p < 0.0001).
- Concerning the respiratory supports, in the No-Vax group there was a significantly more frequent use of HFNC (p < 0.0001) and a less frequent use of CPAP/NIV (p < 0.0001).
- The occurrence of pulmonary embolisms was significantly less frequent in the No-Vax group (p = 0.0049).
- A greater percentage of No-Vax patients died as compared with the Pre-Vax group, although the data did not reach statistical significance (p = 0.08).
- With respect to the laboratory data, AST, LDH, and NLR were significantly higher in No-Vax patients (p = 0.0225, p < 0.0001, p < 0.0001, respectively).
3.2. No-Vax vs. Vax Group
- A statistically higher number of patients was present in the No-Vax group in comparison with the Vax group (72.4% vs. 27.6%, p < 0.0001).
- Patients belonging to the Vax group were significantly older (p = 0.0097) (Figure 1a) and did not show a statistically different BMI.
- There was no significant difference in the prevalence of the male gender or in the percentage of actual and former smokers.
- Vax patients showed a significantly higher Charlson comorbidity index (p < 0.0001) (Figure 1b); in particular, arterial hypertension (p = 0.0371), COPD (p = 0.0142), and malignancies (p = 0.0477) were significantly more prevalent.
- During hospitalization, there were no statistically significant differences in the use of HFNC or CPAP/NIV.
- The occurrence of pulmonary embolism was not significantly different between the two groups.
- There was no significant difference in the percentages of patients who died between the two groups.
- With respect to the laboratory data, creatinine was significantly higher in Vax patients (p = 0.001), while AST and LDH were significantly higher in No-Vax patients (p = 0.0021, p = 0.0012, respectively). NLR was similar between the No-Vax and Vax groups.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Krebs, N.M.; D’Souza, G.; Bordner, C.; Allen, S.I.; Hobkirk, A.L.; Foulds, J.; Yingst, J.M. COVID-19 Vaccination Uptake and Hesitancy among Current Tobacco Users. Tob. Use Insights 2021, 14, 1179173X211068027. [Google Scholar] [CrossRef]
- Papanikolaou, V.; Chrysovergis, A.; Ragos, V.; Tsiambas, E.; Katsinis, S.; Manoli, A.; Papouliakos, S.; Roukas, D.; Mastronikolis, S.; Peschos, D.; et al. From delta to Omicron: S1-RBD/S2 mutation/deletion equilibrium in SARS-CoV-2 defined variants. Gene 2022, 814, 146134. [Google Scholar] [CrossRef]
- Centre, E.; Prevention, D. European Centre for Disease Prevention and Control First COVID-19 Vaccine Authorised for Use in the European Union. 2021. Available online: https://www.ecdc.europa.eu/en/news-events/first-covid-19-vaccine-authorised-use-european-union (accessed on 1 February 2022).
- European Medicines Agency. EMA Recommends Nuvaxovid for Authorisation in the EU. 2021. Available online: Https://Www.Ema.Europa.Eu/En/News/Ema-Recommends-Nuvaxovid-Authorisation-Eu (accessed on 1 February 2022).
- Italy COVID—Coronavirus Statistics—Worldometer, Dadax, Delaware, USA. Available online: https://www.worldometers.info/coronavirus/country/italy/ (accessed on 1 February 2022).
- Governo Italiano. Report Vaccini Anti COVID-19, Governo Italiano. 2022. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 1 February 2022).
- Coccia, M. Optimal levels of vaccination to reduce COVID-19 infected individuals and deaths: A global analysis. Environ. Res. 2021, 204, 112314. [Google Scholar] [CrossRef] [PubMed]
- Bahl, A.; Johnson, S.; Maine, G.; Garcia, M.H.; Nimmagadda, S.; Qu, L.; Chen, N.-W. Vaccination reduces need for emergency care in breakthrough COVID-19 infections: A multicenter cohort study. Lancet Reg. Health Am. 2021, 4, 100065. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, Y.; Yang, Z.; Xia, D.; Hu, Y.; Geng, S. Clinical Characteristics of Patients with Severe Pneumonia Caused by the SARS-CoV-2 in Wuhan, China. Respiration 2020, 99, 649–657. [Google Scholar] [CrossRef]
- Pastorino, R.; Pezzullo, A.M.; Villani, L.; Causio, F.A.; Axfors, C.; Contopoulos-Ioannidis, D.G.; Boccia, S.; Ioannidis, J.P. Change in age distribution of COVID-19 deaths with the introduction of COVID-19 vaccination. Environ. Res. 2021, 204, 112342. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- National Institutes of Health. Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19), COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 1 February 2022).
- Calabrese, C.; Pafundi, P.C.; Mollica, M.; Annunziata, A.; Imitazione, P.; Lanza, M.; Polistina, G.; Flora, M.; Guarino, S.; Palumbo, C.; et al. Effectiveness of corticosteroids on chest high-resolution computed tomography features of COVID-19 pneumonia. Ther. Adv. Respir. Dis. 2021, 15, 17534666211042533. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT imaging features of 2019 novel coronavirus (2019–nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Luk, T.T.; Zhao, S.; Wu, Y.; Wong, J.Y.-H.; Wang, M.P.; Lam, T.H. Prevalence and determinants of SARS-CoV-2 vaccine hesitancy in Hong Kong: A population-based survey. Vaccine 2021, 39, 3602–3607. [Google Scholar] [CrossRef] [PubMed]
- Bem, R.A.; van Mourik, N.; Klein-Blommert, R.; Spijkerman, I.J.; Kooij, S.; Bonn, D.; Vlaar, A.P. Risk of Aerosol Formation During High-Flow Nasal Cannula Treatment in Critically Ill Subjects. Respir. Care 2021, 66, 891–896. [Google Scholar] [CrossRef]
- Agarwal, A.; Basmaji, J.; Muttalib, F.; Granton, D.; Chaudhuri, D.; Chetan, D.; Hu, M.; Fernando, S.M.; Honarmand, K.; Bakaa, L.; et al. High-flow nasal cannula for acute hypoxemic respiratory failure in patients with COVID-19: Systematic reviews of effectiveness and its risks of aerosolization, dispersion, and infection transmission. Can. J. Anesth. 2020, 67, 1217–1248. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Mankodi, D.; Shaharyar, S.; Ravindranathan, S.; Danckers, M.; Herscovici, P.; Moor, M.; Ferrer, G. High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: A systematic review. Respir. Med. 2016, 121, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, E.X.; Zahir, S.M.I.S.M.; Ng, K.T.; Teoh, W.Y.; Hasan, M.S.; Ruslan, S.R.B.; Abosamak, M.F. Effect of prone versus supine position in COVID-19 patients: A systematic review and meta-analysis. J. Clin. Anesth. 2021, 74, 110406. [Google Scholar] [CrossRef]
- Crimi, C.; Pierucci, P.; Renda, T.; Pisani, L.; Carlucci, A. High-Flow Nasal Cannula and COVID-19: A Clinical Review. Respir. Care 2021, 67, 227–240. [Google Scholar] [CrossRef]
- Kurahara, Y.; Kobayashi, T.; Shintani, S.; Matsuda, Y.; Tamiya, A.; Sugawara, R.; Arai, T.; Tachibana, K.; Okishio, K.; Matsui, H.; et al. Clinical characteristics of COVID-19 in Osaka, Japan: Comparison of the first–third waves with the fourth wave. Respir. Investig. 2021, 59, 810–818. [Google Scholar] [CrossRef]
- Vianello, A.; Guarnieri, G.; Lionello, F. Unvaccinated COVID-19 patients in the ICU: Views from both sides of the barrier. Pulmonology 2022, 28, 161–163. [Google Scholar] [CrossRef]
- Lau, B.H.P.; Yuen, S.W.H.; Yue, R.P.H.; Grépin, K.A. Understanding the societal factors of vaccine acceptance and hesitancy: Evidence from Hong Kong. Public Health 2022, 207, 39–45. [Google Scholar] [CrossRef]
- Stamm, T.A.; Partheymüller, J.; Mosor, E.; Ritschl, V.; Kritzinger, S.; Eberl, J.-M. Coronavirus vaccine hesitancy among unvaccinated Austrians: Assessing underlying motivations and the effectiveness of interventions based on a cross-sectional survey with two embedded conjoint experiments. Lancet Reg. Health Eur. 2022, 17, 100389. [Google Scholar] [CrossRef]
- Bai, Y.; Ma, K.; Li, J.; Li, J.; Bi, C.; Shan, A. Deoxynivalenol exposure induces liver damage in mice: Inflammation and immune responses, oxidative stress, and protective effects of Lactobacillus rhamnosus GG. Food Chem. Toxicol. 2021, 156, 112514. [Google Scholar] [CrossRef] [PubMed]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-lymphocyte ratio on admission to predict the severity and mortality of COVID-19 patients: A meta-analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Sari, R.; Karakurt, Z.; Ay, M.; Çelik, M.E.; Tekan, Y.; Çiyiltepe, F.; Kargin, F.; Saltürk, C.; Moçin, Y.; Güngör, G.; et al. Neutrophil to lymphocyte ratio as a predictor of treatment response and mortality in septic shock patients in the intensive care unit. Turk. J. Med. Sci. 2019, 49, 1336–1349. [Google Scholar] [CrossRef] [PubMed]
- Bhat, T.; Teli, S.; Rijal, J.; Bhat, H.; Raza, M.; Khoueiry, G.; Meghani, M.; Akhtar, M.; Costantino, T. Neutrophil to lymphocyte ratio and cardiovascular diseases: A review. Expert Rev. Cardiovasc. Ther. 2013, 11, 55–59. [Google Scholar] [CrossRef]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Ma, Y.; Shi, N.; Fan, Y.; Wang, J.; Zhao, C.; Li, J.; Zhang, X.; Bai, W.; Xiao, F.; Wang, J.; et al. Predictive value of the neutrophil-to-lymphocyte ratio (NLR) for diagnosis and worse clinical course of the COVID-19: Findings from ten provinces in China, 2020. World J. Emerg. Med. 2021, 12, 79–80. [Google Scholar] [CrossRef]
- Cong-Ying, S.; Jia, X.; Jian, Q.; Yuan-Qiang, L. COVID-19 early warning score: A multi-parameter screening tool to identify highly suspected patients. MedXRiv 2020. preprint. [Google Scholar] [CrossRef] [Green Version]
- Yan, X.; Li, F.; Wang, X.; Yan, J.; Zhu, F.; Tang, S.; Deng, Y.; Wang, H.; Chen, R.; Yu, Z.; et al. Neutrophil to lymphocyte ratio as prognostic and predictive factor in patients with coronavirus disease 2019: A retrospective cross—Sectional study. J. Med. Virol. 2020, 92, 2573–2581. [Google Scholar] [CrossRef]
- Zhou, J.; Huang, L.; Chen, J.; Yuan, X.; Shen, Q.; Dong, S.; Cheng, B.; Guo, T.-M. Clinical features predicting mortality risk in older patients with COVID-19. Curr. Med. Res. Opin. 2020, 36, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Zhang, J.; Zhang, T. Immunomodulatory activities of polysaccharides from Ganoderma on immune effector cells. Food Chem. 2020, 340, 127933. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Tian, S.; Lu, D.; Yang, J.; Zeng, H.; Zhang, F.; Tu, D.; Ge, G.; Zheng, Y.; Shi, T.; et al. Systems pharmacological study illustrates the immune regulation, anti-infection, anti-inflammation, and multi-organ protection mechanism of Qing-Fei-Pai-Du decoction in the treatment of COVID-19. Phytomedicine 2020, 85, 153315. [Google Scholar] [CrossRef] [PubMed]
- Brosh-Nissimov, T.; Orenbuch-Harroch, E.; Chowers, M.; Elbaz, M.; Nesher, L.; Stein, M.; Maor, Y.; Cohen, R.; Hussein, K.; Weinberger, M.; et al. BNT162b2 vaccine breakthrough: Clinical characteristics of 152 fully vaccinated hospitalized COVID-19 patients in Israel. Clin. Microbiol. Infect. 2021, 27, 1652–1657. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043. [Google Scholar] [CrossRef]
- Myers, L.C.; Kipnis, P.; Greene, J.; Lawson, B.; Escobar, G.J.; Fireman, B.H.; Klein, N.P.; Liu, V.X. Adults hospitalized with breakthrough COVID-19 have lower mortality than matched unvaccinated adults. J. Intern. Med. 2022. [Google Scholar] [CrossRef]
- Schwarz, T.; Tober-Lau, P.; Hillus, D.; Helbig, E.T.; Lippert, L.J.; Thibeault, C.; Koch, W.; Landgraf, I.; Michel, J.; Bergfeld, L.; et al. Delayed Antibody and T-Cell Response to BNT162b2 Vaccination in the Elderly, Germany. Emerg. Infect. Dis. 2021, 27, 2174–2178. [Google Scholar] [CrossRef]
- Gerayeli, F.V.; Milne, S.; Cheung, C.; Li, X.; Yang, C.W.T.; Tam, A.; Choi, L.H.; Bae, A.; Sin, D.D. COPD and the risk of poor outcomes in COVID-19: A systematic review and meta-analysis. eClinicalMedicine 2021, 33, 100789. [Google Scholar] [CrossRef]
- Leung, J.M.; Yang, C.X.; Tam, A.; Shaipanich, T.; Hackett, T.-L.; Singhera, G.K.; Dorscheid, D.R.; Sin, D.D. ACE-2 expression in the small airway epithelia of smokers and COPD patients: Implications for COVID-19. Eur. Respir. J. 2020, 55, 2000688. [Google Scholar] [CrossRef] [Green Version]
- Milne, S.; Yang, C.X.; Timens, W.; Bossé, Y.; Sin, D.D. SARS-CoV-2 receptor ACE2 gene expression and RAAS inhibitors. Lancet Respir. Med. 2020, 8, e50–e51. [Google Scholar] [CrossRef]
- Herr, C.; Beisswenger, C.; Hess, C.; Kandler, K.; Suttorp, N.; Welte, T.; Schroeder, J.-M.; Vogelmeier, C.; R Bals for the CAPNETZ Study Group. Group Suppression of pulmonary innate host defence in smokers. Thorax 2009, 64, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Mallia, P.; Message, S.D.; Gielen, V.; Contoli, M.; Gray, K.; Kebadze, T.; Aniscenko, J.; Laza-Stanca, V.; Edwards, M.R.; Slater, L.; et al. Experimental Rhinovirus Infection as a Human Model of Chronic Obstructive Pulmonary Disease Exacerbation. Am. J. Respir. Crit. Care Med. 2011, 183, 734–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakkar, A.; Pradhan, K.; Jindal, S.; Cui, Z.; Rockwell, B.; Shah, A.P.; Packer, S.; Sica, R.A.; Sparano, J.; Goldstein, D.Y.; et al. Patterns of seroconversion for SARS-CoV-2 IgG in patients with malignant disease and association with anticancer therapy. Nat. Cancer 2021, 2, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Jin, Y.; Li, R.; Zhang, Z.; Sun, R.; Chen, D. Prevalence and impact of acute renal impairment on COVID-19: A systematic review and meta-analysis. Crit. Care 2020, 24, 356. [Google Scholar] [CrossRef] [PubMed]
- Kai, H.; Kai, M. Interactions of coronaviruses with ACE2, angiotensin II, and RAS inhibitors—lessons from available evidence and insights into COVID-19. Hypertens. Res. 2020, 43, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Vikse, J.; Benoit, S.; Favaloro, E.J.; Lippi, G. Hyperinflammation and derangement of renin-angiotensin-aldosterone system in COVID-19: A novel hypothesis for clinically suspected hypercoagulopathy and microvascular immunothrombosis. Clin. Chim. Acta 2020, 507, 167–173. [Google Scholar] [CrossRef]
- Rosero-Bixby, L. The Effectiveness of Pfizer-BioNTech and Oxford-AstraZeneca Vaccines to Prevent Severe COVID-19 in Costa Rica: Nationwide, Ecological Study of Hospitalization Prevalence. JMIR Public Health Surveill. 2022, 8, e35054. [Google Scholar] [CrossRef]
- Sharma, A.; Oda, G.; Holodniy, M. Effectiveness of mRNA-based vaccines during the emergence of SARS-CoV-2 Omicron variant. Clin. Infect. Dis. 2022, ciac325. [Google Scholar] [CrossRef]
- McAlister, F.A.; Nabipoor, M.; Chu, A.; Lee, D.S.; Saxinger, L.; Bakal, J.A. The impact of shifting demographics, variants of concern and vaccination on outcomes during the first 3 COVID-19 waves in Alberta and Ontario: A retrospective cohort study. CMAJ Open 2022, 10, E400–E408. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C.A.; Mehta, N.; Keogh, R.H.; Diaz-Ordaz, K.; Khunti, K.; Lyons, R.A.; Kee, F.; Sheikh, A.; Rahman, S.; et al. Risk prediction of covid-19 related death and hospital admission in adults after covid-19 vaccination: National prospective cohort study. BMJ 2021, 374, n2244. [Google Scholar] [CrossRef]
- Peralta-Santos, A.; Rodrigues, E.F.; Moreno, J.; Ricoca, V.; Casaca, P.; Fernandes, E.; Gomes, J.P.; Ferreira, R.; Isidro, J.; Pinto, M.; et al. Omicron (BA.1) SARS-CoV-2 variant is associated with reduced risk of hospitalization and length of stay compared with Delta (B.1.617.2). medRxiv 2022. [Google Scholar] [CrossRef]


{kind=link}
| Pre-Vax | No-Vax | Vax | p | p | |
|---|---|---|---|---|---|
| (n = 132) | (n = 105) | (n = 40) | Pre-Vax vs. No-Vax | No-Vax vs. Vax | |
| Age, years, median [IQR] | 62.9 ± 12.9 | 64.5 ± 13.5 | 71.5 ± 10.8 | 0.63 | 0.0097 |
| Male sex, % | 76.52 | 55.66 | 70.0 | 0.0007 | 0.1331 |
| BMI, kg/m2, median [IQR] | 28.0 [27.0–31.0] | 27.7 [26.0–31.2] | 26.0 [24.0–28.0] | 0.5 | 0.0542 |
| Smokers, % | 26.0 | 51.6 | 40.0 | 0.0003 | 0.1184 |
| CC index median [IQR] | 2.0 [1.0–4.0] | 3.0 [1.0–4.0] | 4.0 [3.0–6.0] | >0.9999 | <0.0001 |
| Arterial hypertension, (%) | 70.63 | 51.96 | 72.50 | 0.0041 | 0.0371 |
| Obesity, (%) | 37.50 | 29.29 | 17.50 | 0.2509 | 0.2001 |
| Diabetes, (%) | 25.21 | 23.53 | 37.50 | 0.8754 | 0.0999 |
| COPD, (%) | 13.91 | 12.87 | 32.50 | 0.8444 | 0.0142 |
| Asthma, (%) | 3.48 | 3.96 | 0.00 | >0.9999 | 0.5747 |
| Neoplasms, (%) | 6.06 | 9.90 | 24.32 | 0.3261 | 0.0477 |
| HRCT score median [IQR] | 10.0 [7.0–13.0] | 15.0 [13.5–17.0] | 13.0 [10.0–15.0] | <0.0001 | 0.0015 |
| PaO2/FiO2 median [IQR] | 155.0 [110.0–233.0] | 77.0 [63.5–106.0] | 93.5 [71.3–162.0] | <0.0001 | 0.0518 |
| HFNC, (%) | 14.4 | 60.0 | 42.5 | <0.0001 | 0.0644 |
| CPAP/NIV, (%) | 45.5 | 16.2 | 10.0 | <0.0001 | 0.4352 |
| Pulmonary embolism, (%) | 27.73 | 12.38 | 5.0 | 0.0049 | 0.2375 |
| Days in hospital, median [IQR] | 23.0 [15.0–32.0] | 16.0 [12.0–24.0] | 18.5 [12.5–25.0] | 0.0021 | >0.9999 |
| Death, (%) | 33.85 | 45.71 | 35.0 | 0.08 | 0.26 |
| CRP, mg/dL median [IQR] | 9.4 [4.9–16.4] | 8.9 [4.4–15.4] | 9.3 [4.1–13.4] | >0.9999 | >0.9999 |
| IL-6, pg/mL median [IQR] | 38.9 [21.0–79.3] | 28.45 [18.8–64.6] | 40.4 [15.2–84.6] | 0.4307 | >0.9999 |
| D-dimer, ng/mL median [IQR] | 389.0 [243.0–1104] | 396.0 [237.8–1163] | 464.0 [286.5–871.3] | >0.9999 | >0.9999 |
| PCT, ug/L median [IQR] | 0.14 [0.07–0.36] | 0.12 [0.07–0.35] | 0.19 [0.08–0.45] | >0.9999 | 0.7100 |
| AST, U/L median [IQR] | 38.0 [25.0–59.0] | 48.5 [34.0–73.3] | 36.5 [19.0–47.0] | 0.0225 | 0.0021 |
| ALT, U/L median [IQR] | 35.0 [21.0–70.0] | 36.0 [27.5–71.0] | 27.0 [19.0–43.8] | >0.9999 | 0.0522 |
| LDH, IU/L median [IQR] | 305.0 [240.0–483.0] | 448.0 [343.5–649.8] | 370.0 [245.3–473.3] | <0.0001 | 0.0012 |
| Azotemia, mg/dL median [IQR] | 50.0 [38.0–69.0] | 56.0 [44.0–75.6] | 79.0 [44.8–113.8] | 0.2521 | 0.1048 |
| Creatinine, mg/dL median [IQR] | 0.8 [0.7–1.0] | 0.8 [0.6–0.9] | 1.0 [0.8–1.7] | 0.4208 | 0.0010 |
| Glycemia, mg/dL median [IQR] | 122.0 [101.0–170.0] | 125.5 [105.3–174.3] | 129.5 [107.5–183.0] | >0.9999 | >0.9999 |
| WBC, ×109/L median [IQR] | 7.9 [5.86–11.3] | 8.5 [5.5–11.5] | 9.4 [6.0–12.4] | >0.9999 | >0.9999 |
| Lymphocytes,% median [IQR] | 11.9 [6.9–16.3] | 7.5 [5.0–11.2] | 8.5 [6.0–12.8] | <0.0001 | >0.9999 |
| Neutrophils,% median [IQR] | 80.7 [75.1–86.7] | 86.8 [81.7–90.4] | 84.7 [78.5–89.3] | <0.0001 | 0.7678 |
| NLR median [IQR] | 6.87 [4.59–12.84] | 11.60 [7.36–17.94] | 9.85 [6.42–14.88] | <0.0001 | >0.9999 |
| CRP, mg/dL median [IQR] | 9.4 [4.9–16.4] | 8.9 [4.4–15.4] | 9.3 [4.1–13.4] | >0.9999 | >0.9999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calabrese, C.; Annunziata, A.; Mariniello, D.F.; Coppola, A.; Mirizzi, A.I.; Simioli, F.; Pelaia, C.; Atripaldi, L.; Pugliese, G.; Guarino, S.; et al. Evolution of the Clinical Profile and Outcomes of Unvaccinated Patients Affected by Critical COVID-19 Pneumonia from the Pre-Vaccination to the Post-Vaccination Waves in Italy. Pathogens 2022, 11, 793. https://doi.org/10.3390/pathogens11070793
Calabrese C, Annunziata A, Mariniello DF, Coppola A, Mirizzi AI, Simioli F, Pelaia C, Atripaldi L, Pugliese G, Guarino S, et al. Evolution of the Clinical Profile and Outcomes of Unvaccinated Patients Affected by Critical COVID-19 Pneumonia from the Pre-Vaccination to the Post-Vaccination Waves in Italy. Pathogens. 2022; 11(7):793. https://doi.org/10.3390/pathogens11070793
Chicago/Turabian StyleCalabrese, Cecilia, Anna Annunziata, Domenica Francesca Mariniello, Antonietta Coppola, Angela Irene Mirizzi, Francesca Simioli, Corrado Pelaia, Lidia Atripaldi, Gaia Pugliese, Salvatore Guarino, and et al. 2022. "Evolution of the Clinical Profile and Outcomes of Unvaccinated Patients Affected by Critical COVID-19 Pneumonia from the Pre-Vaccination to the Post-Vaccination Waves in Italy" Pathogens 11, no. 7: 793. https://doi.org/10.3390/pathogens11070793