
Burdens of Apprentices Caused by the COVID-19 Pandemic and How They Deal with Them: A Qualitative Study Using Content Analysis One-Year Post-Breakout

Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Prevailing COVID-19 Measures
2.3. Data Analysis
3. Results
3.1. Sample
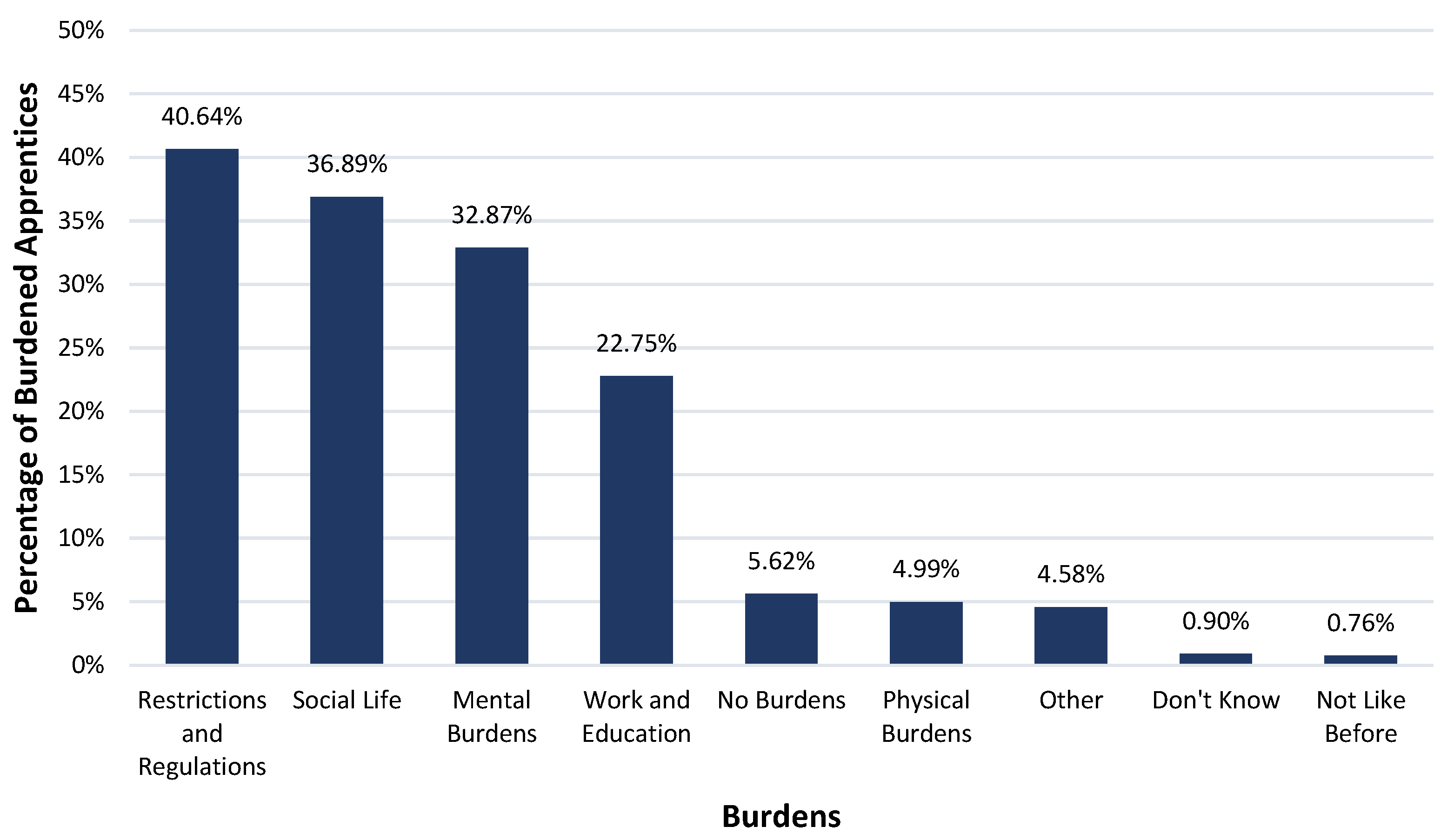
3.2. Burdens
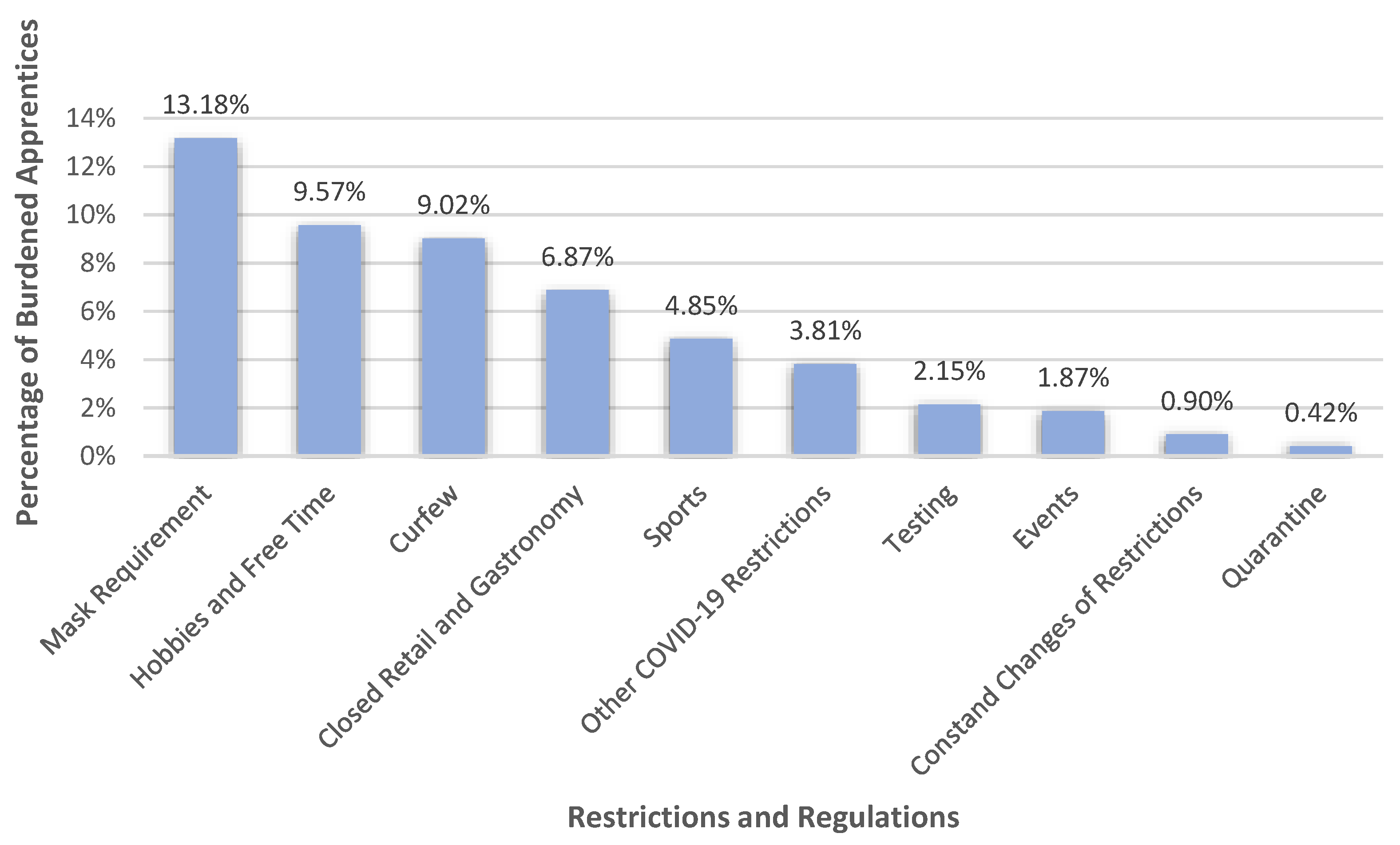
3.2.1. Restrictions and Regulations

3.2.2. Social Life
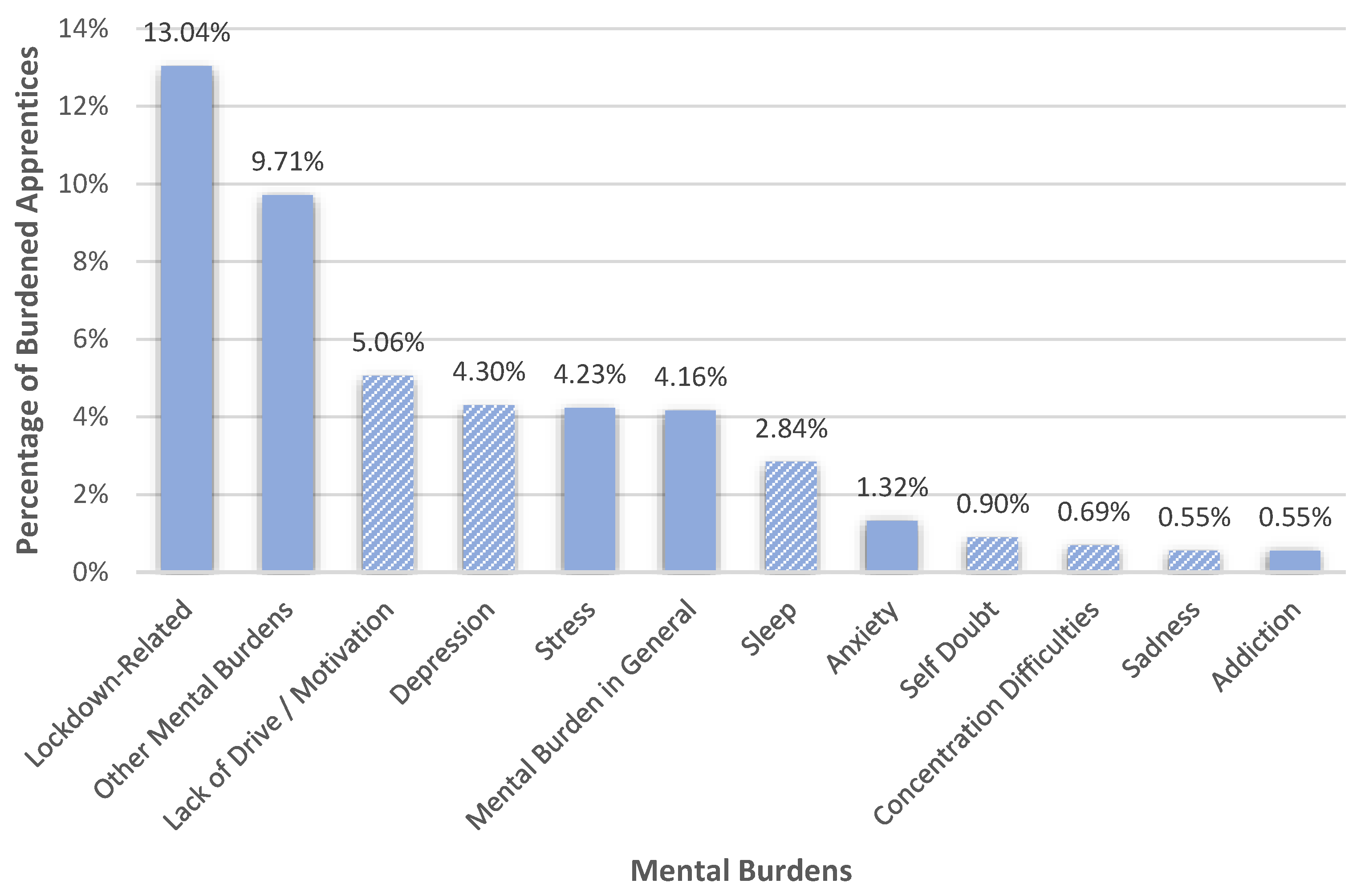
3.2.3. Mental Burdens

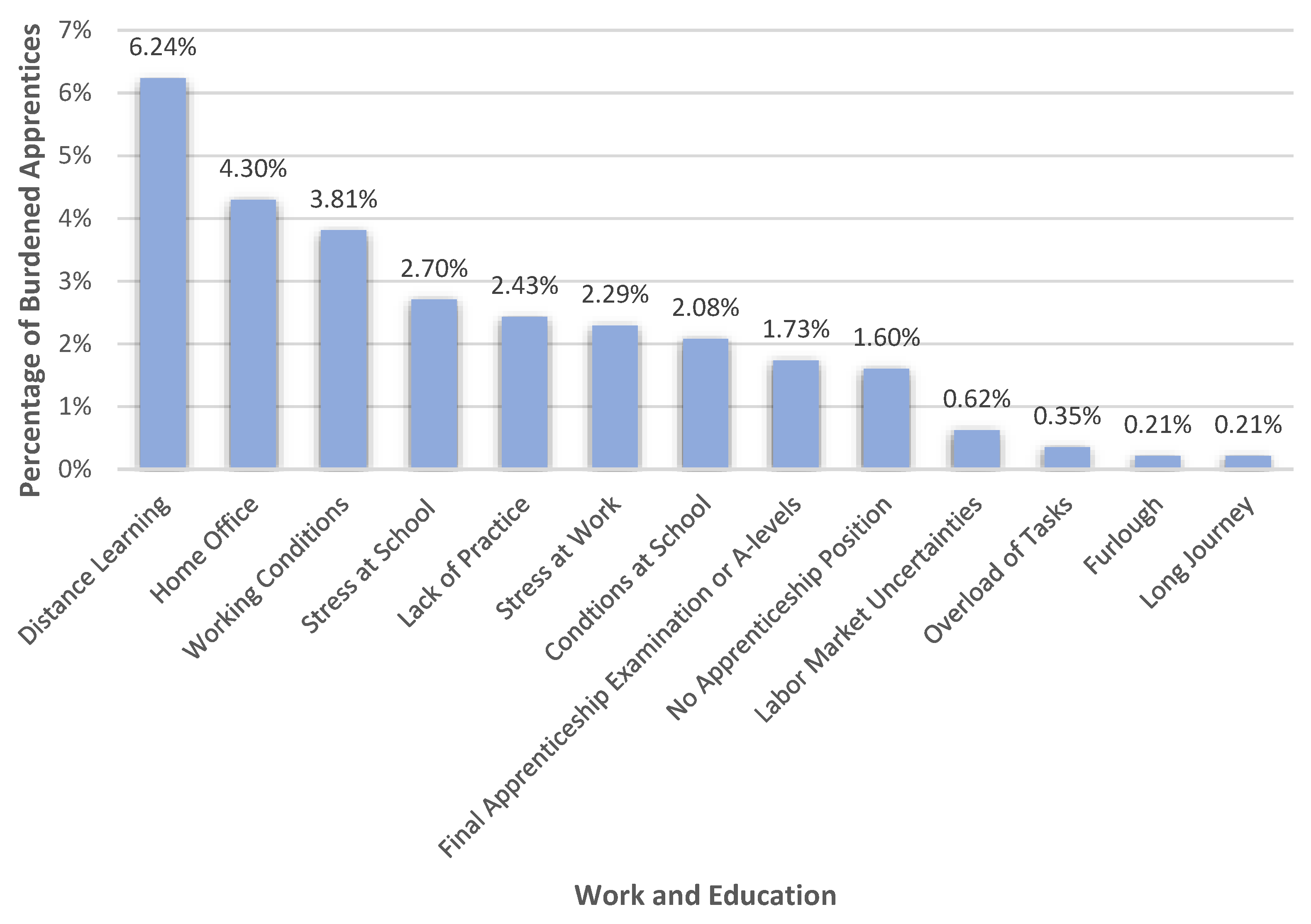
3.2.4. Work and Education

3.2.5. Physical Burdens
3.2.6. Other Answers
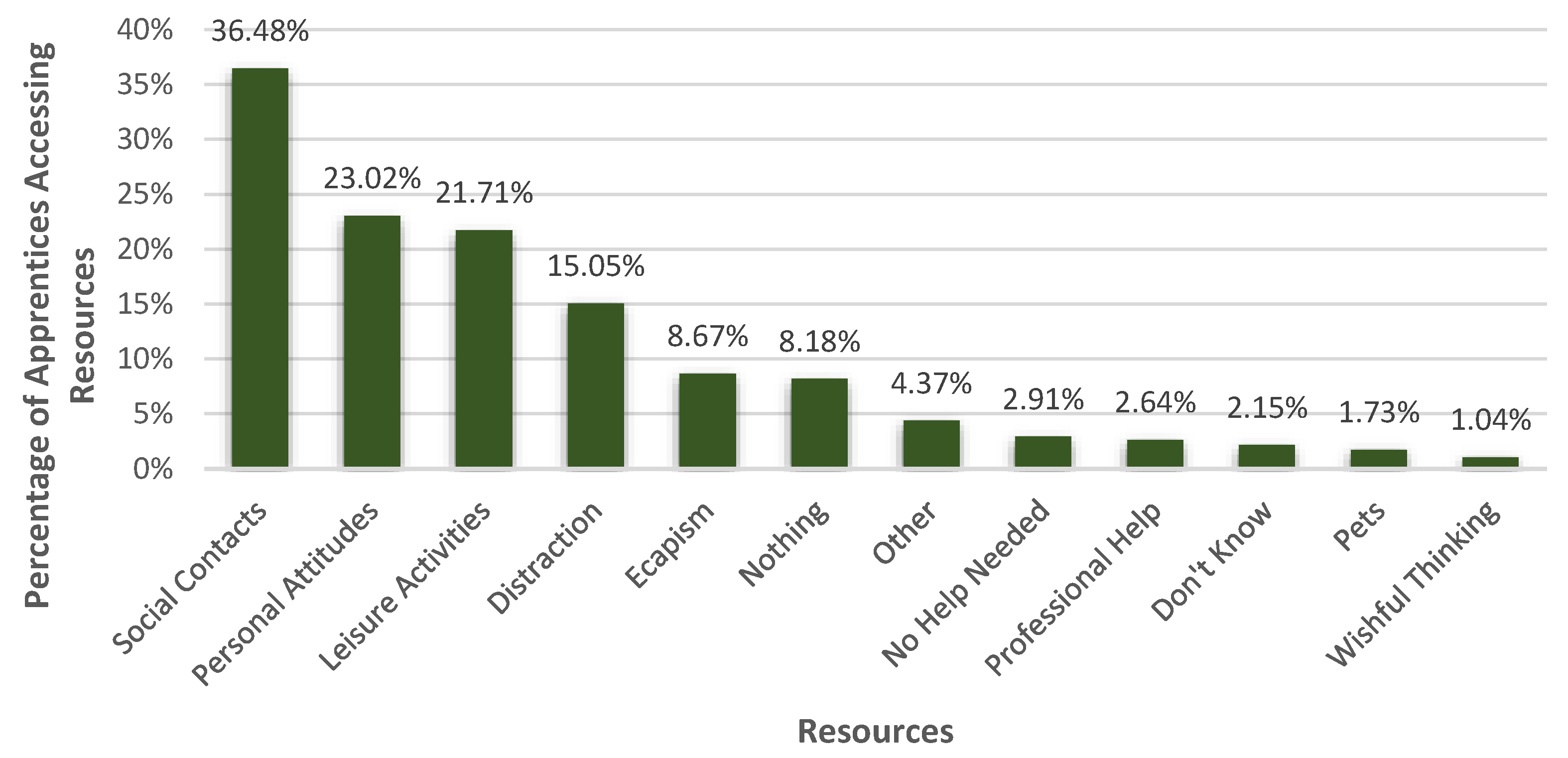
3.3. Resources
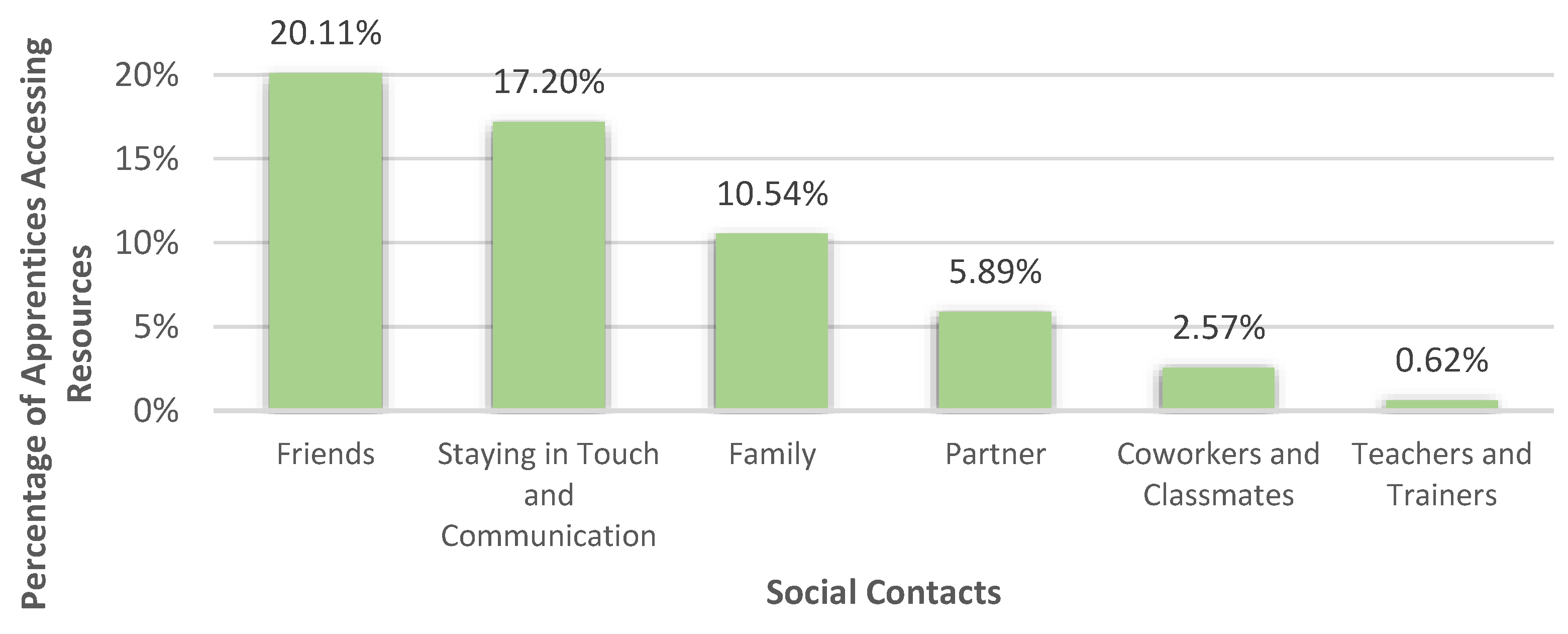
3.3.1. Social Contacts

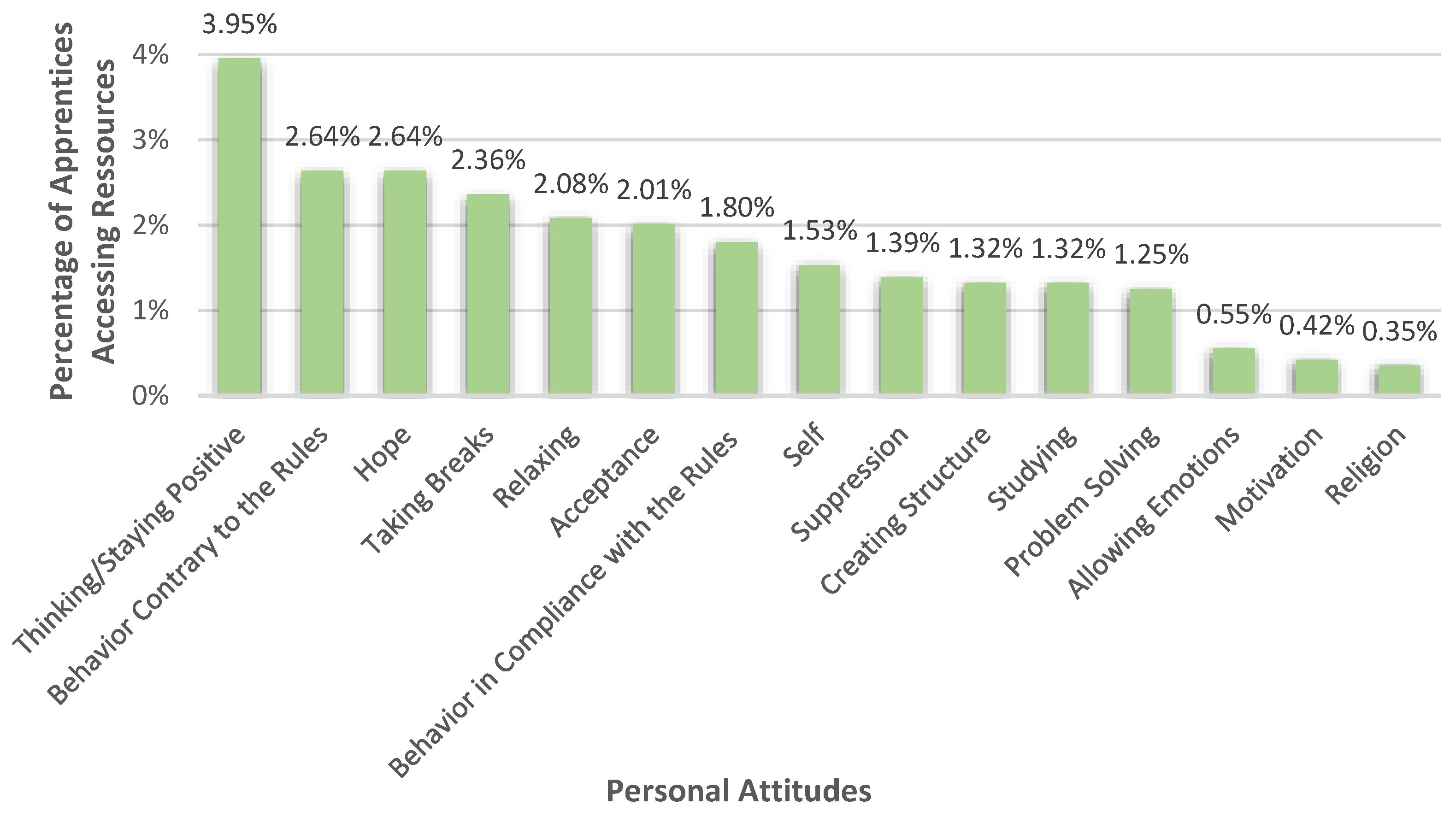
3.3.2. Personal Attitudes

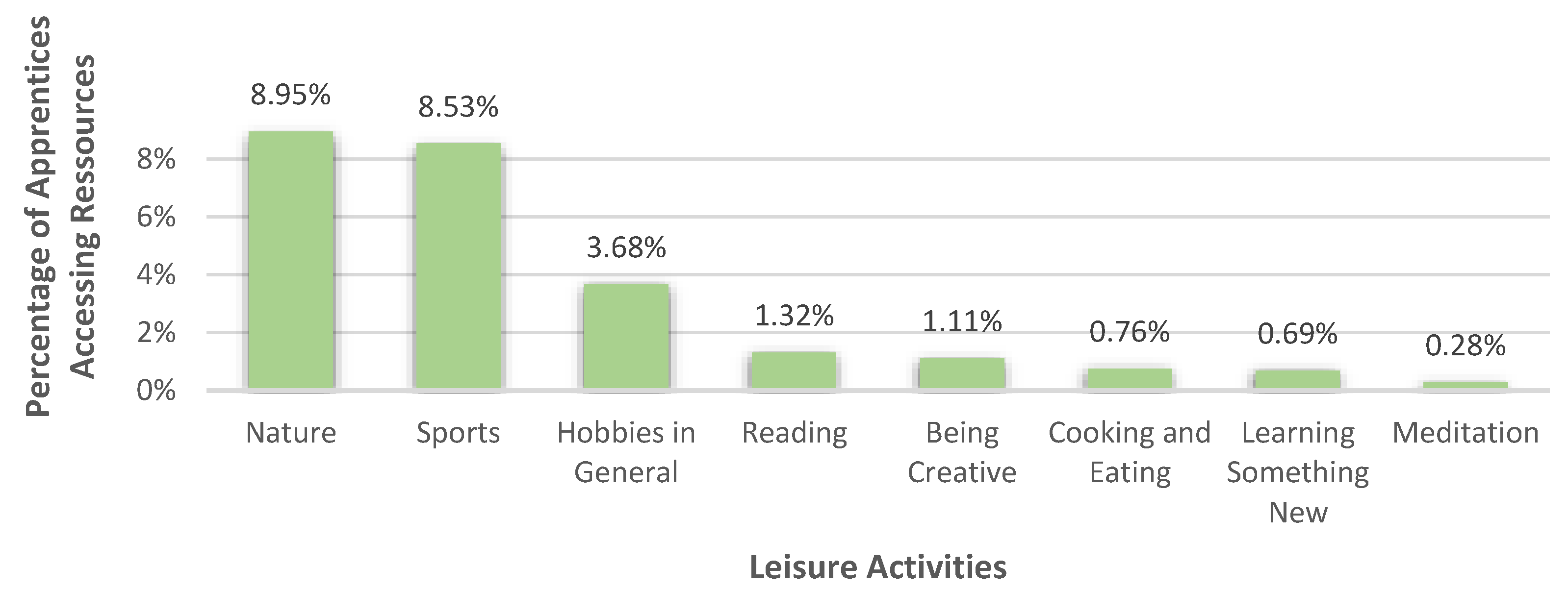
3.3.3. Leisure Activities

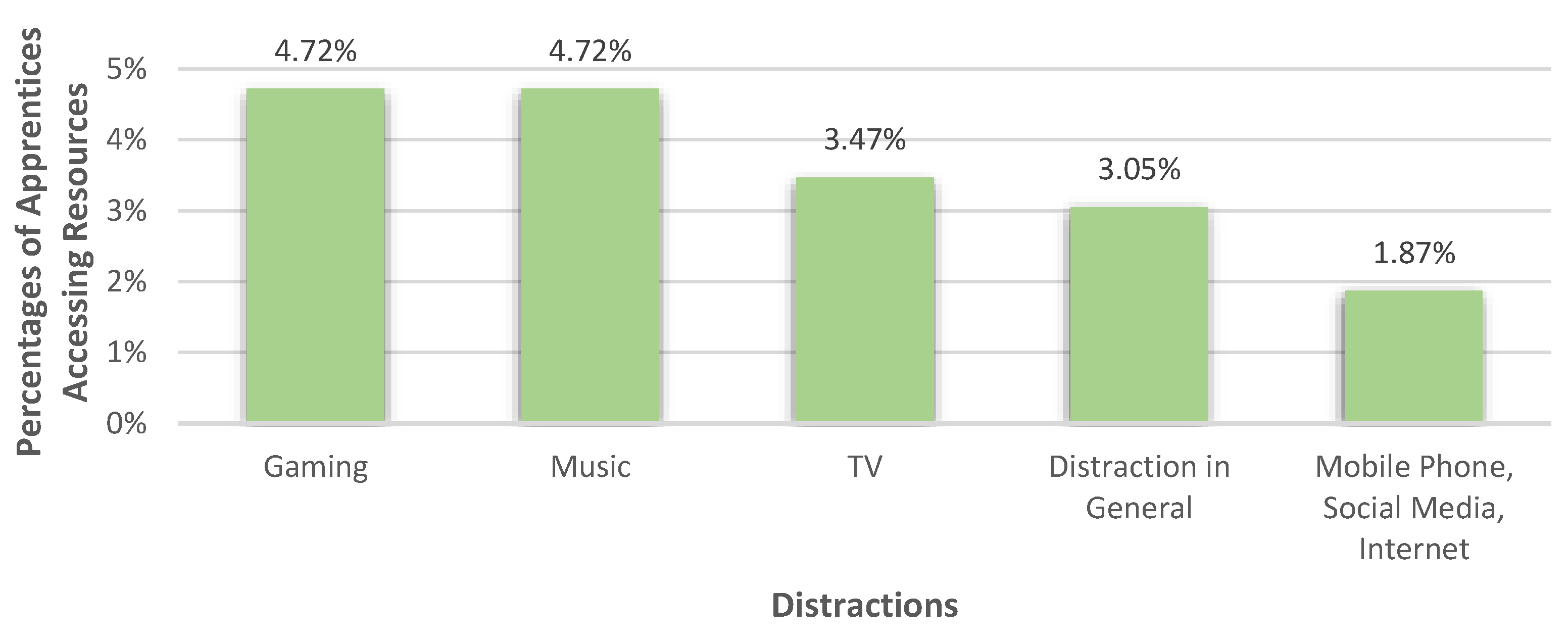
3.3.4. Distractions

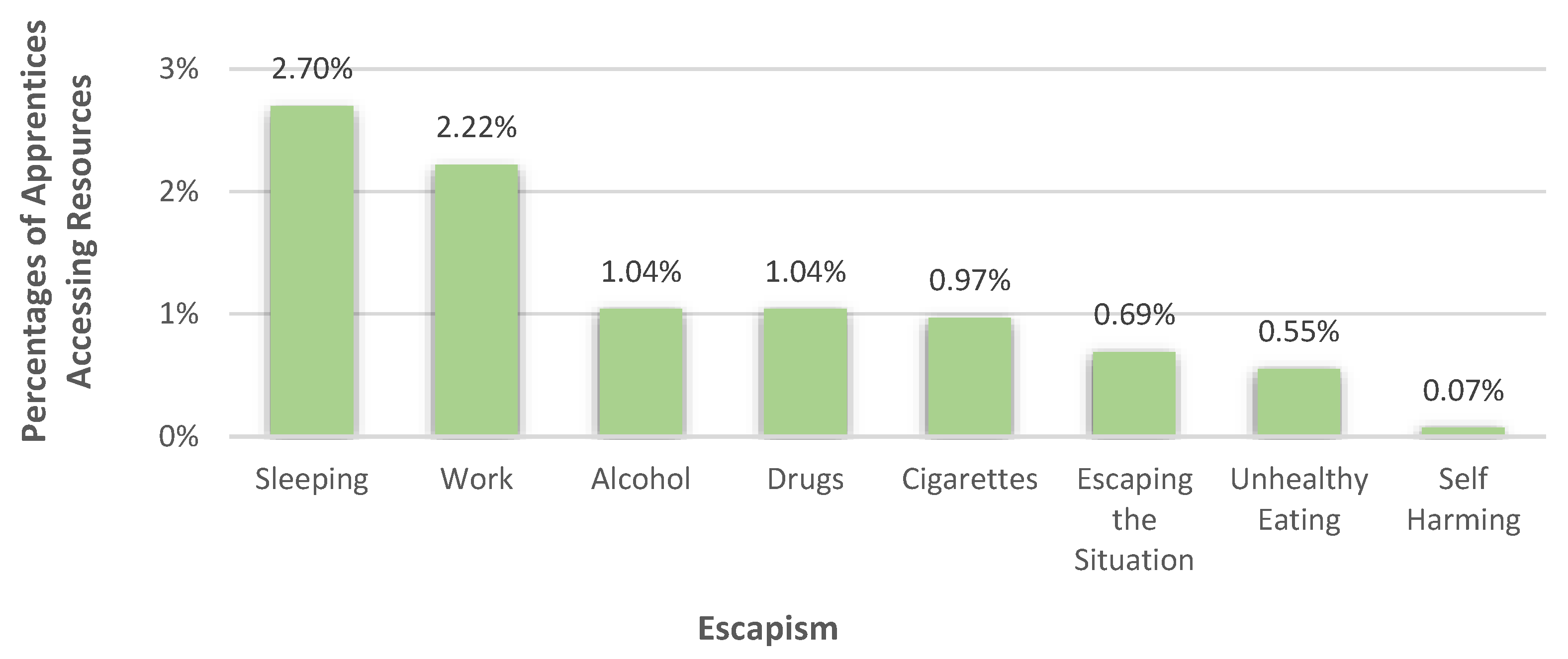
3.3.5. Escapism

3.3.6. Professional Help
3.3.7. Other Answers
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bundesministerium für Soziales, Gesundheit, Pflege und Komsumentenschutz (BMSGPK). COVID-19: Analyse der Sozialen Lage in Österreich; Federal Ministry of Social Affairs, Health, Care and Consumer Protection: Vienna, Austria, 2020. [Google Scholar]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.L.J.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000 Res. 2020, 9, 636. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The need for prevention and early intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of Covid-19 lockdown on mental health and sleep disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Budimir, S.; Humer, E.; Probst, T. Comparing mental health during the COVID-19 lockdown and 6 months after the lockdown in Austria: A longitudinal study. Front. Psychiatry 2021, 12, 625973. [Google Scholar] [CrossRef]
- Dale, R.; Budimir, S.; Probst, T.; Stippl, P.; Pieh, C. Mental health during the COVID-19 lockdown over the christmas period in Austria and the effects of sociodemographic and lifestyle factors. Int. J. Environ. Res. Public Health 2021, 18, 3679. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Pieh, C.; Plener, P.L.; Probst, T.; Dale, R.; Humer, E. Assessment of mental health of high school students during social distancing and remote schooling during the COVID-19 pandemic in Austria. JAMA Netw. Open 2021, 4, e2114866. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Dale, R.; Plener, P.L.; Humer, E.; Probst, T. Stress levels in high-school students after a semester of home-schooling. Eur. Child Adolesc. Psychiatry 2021, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Dale, R.; Jesser, A.; Probst, T.; Plener, P.L.; Humer, E. The impact of migration status on adolescents’ mental health during COVID-19. Healthcare 2022, 10, 176. [Google Scholar] [CrossRef]
- Dale, R.; Jesser, A.; Pieh, C.; O’Rourke, T.; Probst, T.; Humer, E. Mental health burden of high school students, and suggestions for psychosocial support, 1.5 years into the COVID-19 pandemic in Austria. Eur. Child Adolesc. Psychiatry 2022, 1–10. [Google Scholar] [CrossRef]
- Agarwal, N.A.; Harikar, M.; Shukla, R.; Bajpai, A. Factors determining psychological stress among Indian adolescents and young adults during the COVID-19 outbreak. Indian J. Soc. Psychiatry 2021, 37, 82–87. [Google Scholar] [CrossRef]
- Duan, L.; Shao, X.; Wang, Y.; Huang, Y.; Miao, J.; Yang, X.; Zhu, G. An investigation of mental health status of children and adolescents in china during the outbreak of COVID-19. J. Affect. Disord. 2020, 275, 112–118. [Google Scholar] [CrossRef]
- Li, S.H.; Beames, J.R.; Newby, J.M.; Maston, K.; Christensen, H.; Werner-Seidler, A. The impact of COVID-19 on the lives and mental health of Australian adolescents. Eur. Child Adolesc. Psychiatry 2021, 31, 1465–1477. [Google Scholar] [CrossRef]
- Nocentini, A.; Palladino, B.E.; Menesini, E. Adolescents’ Stress Reactions in Response to COVID-19 Pandemic at the peak of the outbreak in Italy. Clin. Psychol. Sci. 2021, 9, 507–514. [Google Scholar] [CrossRef]
- Orgilés, M.; Morales, A.; Delvecchio, E.; Mazzeschi, C.; Espada, J.P. Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. Front. Psychol. 2020, 11, 579038. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 31, 879–889. [Google Scholar] [CrossRef]
- Bonsaksen, T.; Chiu, V.; Leung, J.; Schoultz, M.; Thygesen, H.; Price, D.; Ruffolo, M.; Geirdal, A.Ø. Students’ mental health, well-being, and loneliness during the COVID-19 pandemic: A cross-national study. Healthcare 2022, 10, 996. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.-E.; Eun, D.; Jee, Y.-S. Daily life patterns, psychophysical conditions, and immunity of adolescents in the COVID-19 era: A mixed research with qualitative interviews by a quasi-experimental retrospective study. Healthcare 2022, 10, 1152. [Google Scholar] [CrossRef] [PubMed]
- Đorđić, V.; Cvetković, M.; Popović, B.; Radanović, D.; Lazić, M.; Cvetković, B.; Andrašić, S.; Buišić, S.; Marković, M. Physical activity, eating habits and mental health during COVID-19 lockdown period in Serbian adolescents. Healthcare 2022, 10, 834. [Google Scholar] [CrossRef]
- Ruiz-Zaldibar, C.; García-Garcés, L.; Vicario-Merino, Á.; Mayoral-Gonzalo, N.; Lluesma-Vidal, M.; Ruiz-López, M.; Pérez-Manchón, D. The Impact of COVID-19 on the lifestyles of university students: A Spanish online survey. Healthcare 2022, 10, 309. [Google Scholar] [CrossRef] [PubMed]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.A.K.; Mitra, A.K.; Bhuiyan, A.R. Impact of COVID-19 on mental health in adolescents: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 2470. [Google Scholar] [CrossRef]
- Ma, L.; Mazidi, M.; Li, K.; Li, Y.; Chen, S.; Kirwan, R.; Zhou, H.; Yan, N.; Rahman, A.; Wang, W.; et al. Prevalence of mental health problems among children and adolescents during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 293, 78–89. [Google Scholar] [CrossRef]
- Panchal, U.; Salazar de Pablo, G.; Franco, M.; Moreno, C.; Parellada, M.; Arango, C.; Fusar-Poli, P. The impact of COVID-19 lockdown on child and adolescent mental health: Systematic review. Eur. Child Adolesc. Psychiatry 2021, 18, 1–27. [Google Scholar] [CrossRef]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Review: Mental health impacts of the COVID-19 pandemic on children and youth-a systematic review. Child Adolesc. Ment. Health 2022, 27, 173–189. [Google Scholar] [CrossRef]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113300. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Erhart, M.; Devine, J.; Gilbert, M.; Reiss, F.; Barkmann, C.; Siegel, N.A.; Simon, A.M.; Hurrelmann, K.; Schlack, R.; et al. Child and sdolescent mental health during the COVID-19 pandemic: Results of the three-wave longitudinal COPSY study. J. Adolesc Health 2022, 7, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Dale, R.; O’Rourke, T.; Humer, E.; Jesser, A.; Plener, P.L.; Pieh, C. Mental health of apprentices during the COVID-19 pandemic in Austria and the effect of gender, migration background, and work situation. Int. J. Environ. Res. Public Health 2021, 18, 8933. [Google Scholar] [CrossRef] [PubMed]
- Einboden, R.; Choi, I.; Ryan, R.; Petrie, K.; Johnston, D.; Harvey, S.B.; Glozier, N.; Wray, A.; Deady, M. ‘Having a thick skin is essential’: Mental health challenges for young apprentices in Australia. J. Youth Stud. 2020, 24, 355–371. [Google Scholar] [CrossRef]
- Scharinger, C. Gesundheitsförderung mit Jungen Arbeitnehmer/Innen in der Überbetrieblichen Lehrausbildung: Gesundheitsbefragung 2015. No. 12; Fonds Gesundes Österreich, ein Geschäftsbereich der Gesundheit Österreich GmbH: Vienna, Austria, 2015. [Google Scholar]
- Ross, V.; Mathieu, S.L.; Wardhani, R.; Gullestrup, J.; Kolves, K. Factors associated with workplace bullying and the mental health of construction industry apprentices: A mixed methods study. Front. Psychiatry 2021, 12, 629262. [Google Scholar] [CrossRef]
- Pidd, K.; Duraisingam, V.; Roche, A.; Trifonoff, A. Young construction workers: Substance use, mental health, and workplace psychosocial factors. Adv. Dual Diagn. 2017, 10, 155–168. [Google Scholar] [CrossRef]
- Ross, V.; Caton, N.; Gullestrup, J.; Kolves, K. Understanding the barriers and pathways to male help-seeking and help-offering: A mixed methods study of the impact of the mates in construction program. Int. J. Environ. Res. Public Health 2019, 16, 2979. [Google Scholar] [CrossRef] [Green Version]
- Broadbent, R.; Papadopoulos, T. Improving mental health and wellbeing for young men in the building and construction industry. J. Child Adolesc. Ment. Health 2014, 26, 217–227. [Google Scholar] [CrossRef]
- O’Rourke, T.; Dale, R.; Humer, E.; Plener, P.; Pieh, C. Problematic alcohol use in Austrian apprentices during the COVID-19 pandemic. Addict. Behav. Rep. 2022, 15, 100414. [Google Scholar] [CrossRef]
- O’Rourke, T.; Dale, R.; Humer, E.; Probst, T.; Plener, P.; Pieh, C. Health behaviors in Austrian apprentices and school students during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1049. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap). A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Pollak, M.; Kowarz, N.; Partheymüller, J. Chronologie zur Corona-Krise in Österreich-Teil 5: Dritte Welle, Regionale Lockdowns und Impffortschritt. Available online: https://viecer.univie.ac.at/corona-blog/corona-blog-beitraege/blog112/ (accessed on 30 September 2022).
- Bock-Schappelwein, J.; Famira-Mühlberger, U.; Huemer, U.; Hyll, W. Der Österreichische Arbeitsmarkt im Zeichen der COVID-19 Pandemie; Österreichisches Institut für Wirtschaftsforschung: Vienna, Austria, 2021; pp. 371–388. [Google Scholar]
- Bock-Schappelwein, J.; Huemer, U.; Hyll, W. COVID-19 Pandemie: Weniger Sommerjobs für Jugendliche im Juli; Österreichisches Institut für Wirtschaftsforschung: Vienna, Austria, 2020; pp. 1–9. [Google Scholar]
- ATLAS. ti 22 Windows; ATLAS.ti Scientific Software Development GmbH: Berlin, Germany, 2022. [Google Scholar]
- Jesser, A.; Schaffler, Y.; Gachter, A.; Dale, R.; Humer, E.; Pieh, C. School students’ concerns and support after one year of COVID-19 in Austria: A qualitative study using content analysis. Healthcare 2022, 10, 1334. [Google Scholar] [CrossRef] [PubMed]
- Cicognani, E. Coping strategies with minor stressors in adolescence: Relationships with social support, self-efficacy, and psychological well-being. J. Appl. Soc. Psychol. 2011, 41, 559–578. [Google Scholar] [CrossRef]
- Mohd Fadhli, S.A.; Liew Suet Yan, J.; Ab Halim, A.S.; Ab Razak, A.; Ab Rahman, A. Finding the link between cyberbullying and suicidal behaviour among adolescents in Peninsular Malaysia. Healthcare 2022, 10, 856. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary care evaluation of mental disorders. Patient Health Questionnaire. Jama 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Burns, J.R.; Rapee, R.M. Adolescent mental health literacy: Young people’s knowledge of depression and help seeking. J. Adolesc. 2006, 29, 225–239. [Google Scholar] [CrossRef]
- Mohr, M. Durchschnittliches Brutto- und Nettoeinkommen von Lehrlingen in Österreich nach Geschlecht 2020; Statista: Hamburg, Germany, 2021. [Google Scholar]
- Rechnungshof Österreich. Allgemeiner Einkommensbericht 2020; Bericht des Rechnungshofes: Vienna, Austria, 2020; pp. 1–236.
- Lachmayr, N.; Mayerl, M. 4. Österreichischer Lehrlingsmonitor: Ergebnisse einer bundesweiten Befragung von Lehrlingen; Österreichisches Institut für Berufsbildungsforschung: Vienna, Austria, 2021. [Google Scholar]
- Felder-Puig, R.; Teufl, L. Die psychische Gesundheit österreichischer Schülerinnen und Schüler: HBSC-Factsheet 01: Ergebnisse der HBSC-Studie 2018; Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentschutz: Vienna, Austria, 2019. [Google Scholar]
- Jesser, A.; Schmalwieser, S.; Mädge, A.-L.; Culen, C.; Schrank, B.; Böckle, M. Chancen niederschwelliger online Peer-to-Peer Begleitung für Jugendliche am Beispiel der Online-Plattform OPEN. Psychother. Forum 2021, 25, 154–160. [Google Scholar] [CrossRef]
- O’Driscoll, C.; Heary, C.; Hennessy, E.; McKeague, L. Explicit and implicit stigma towards peers with mental health problems in childhood and adolescence. J. Child Psychol. Psychiatry 2012, 53, 1054–1062. [Google Scholar] [CrossRef]
- de Girolamo, G.; Dagani, J.; Purcell, R.; Cocchi, A.; McGorry, P.D. Age of onset of mental disorders and use of mental health services: Needs, opportunities and obstacles. Epidemiol. Psychiatr. Sci. 2012, 21, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Moses, T. Stigma and self-concept among adolescents receiving mental health treatment. Am. J. Orthopsychiatry 2009, 79, 261–274. [Google Scholar] [CrossRef]
- Schachter, H.M.; Girardi, A.; Ly, M.; Lacroix, D.; Lumb, A.B.; van Berkom, J.; Gill, R. Effects of school-based interventions on mental health stigmatization: A systematic review. Child Adolesc. Psychiatry Ment. Health 2008, 2, 18. [Google Scholar] [CrossRef]
- Hilbert, K.; Boeken, O.; Asbrand, J.; Seemann, S.; Langhammer, T.; Praxl, B.; Horvath, L.; Ertle, A.; Lueken, U. Who is seeking help for psychological distress associated with the COVID-19 pandemic? Characterization of risk factors in 1269 participants accessing low-threshold psychological help. PLoS ONE 2022, 17, e0271468. [Google Scholar] [CrossRef] [PubMed]
- Tambling, R.R.; Russell, B.S.; Fendrich, M.; Park, C.L. Predictors of mental health help-seeking during COVID-19: Social support, emotion regulation, and mental health symptoms. J. Behav. Health Serv. Res. 2022, 1–12. [Google Scholar] [CrossRef]
- Kutcher, S.; Wei, Y.; Coniglio, C. Mental health literacy: Past, present, and future. Can. J. Psychiatry 2016, 61, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Skre, I.; Friborg, O.; Breivik, C.; Johnsen, L.I.; Arnesen, Y.; Wang, C.E. A school intervention for mental health literacy in adolescents: Effects of a non-randomized cluster controlled trial. BMC Public Health 2013, 13, 873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundesministerium für Finanzen. Bundesrecht konsolidiert: Gesamte Rechtsvorschrift für Lehrpläne für Berufsschulen (Lehrplan 2016); Federal Ministry of Finance: Vienna, Austria, 2022.
- Bundesministerium für Bildung, Wissenschaft und Forschung. Lehrpläne der berufsbildenden Schulen. Available online: https://www.bmbwf.gv.at/Themen/schule/schulpraxis/lp/lp_bbs.html (accessed on 27 October 2022).
- Pinfold, V.; Stuart, H.; Thornicroft, G.; Arboleda-Flórez, J. Working with young people: The impact of mental health awareness programmes in school in the UK and Canada. World Psychiatry 2005, 4, 48–52. [Google Scholar]
- Corrigan, P.W.; River, L.; Lundin, R.K.; Penn, D.L.; Uphoff-Wasowski, K.; Campion, J.; Mathisen, J.; Gagnon, C.; Bergman, M.; Goldstein, H.; et al. Three strategies for changing attributions about severe mental illness. Schizophr. Bull. 2001, 27, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Österreischischer Berufsverband für Psychotherapie. Fit4SCHOOL: Psychotherapeutische Beratung in der Schule; Österreischischer Berufsverband für Psychotherapie: Vienna, Austria, 2022; pp. 1–12. [Google Scholar]
- Berufsverband Österreichischer Psychologinnen und Psychologen. Gesund aus der Krise. Available online: https://gesundausderkrise.at/ (accessed on 16 September 2022).
- Kim, S.; Son, H.-G.; Lee, S.; Park, H.; Jeong, K.-H. A study on the relationship between depression change types and suicide ideation before and after COVID-19. Healthcare 2022, 10, 1610. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N | % |
|---|---|---|
| Age | ||
| 15 | 70 | 4.9 |
| 16 | 215 | 14.9 |
| 17 | 363 | 25.2 |
| 18 | 292 | 20.2 |
| 19 | 191 | 13.2 |
| 20 | 130 | 9.0 |
| >20 | 181 | 12.6 |
| Gender | ||
| Female | 771 | 53.5 |
| Male | 655 | 45.4 |
| Diverse | 16 | 1.1 |
| Migration background | ||
| No | 1022 | 70.9 |
| Yes | 420 | 29.1 |
| Region | ||
| Vienna | 531 | 36.8 |
| Lower Austria | 256 | 17.8 |
| Upper Austria | 389 | 27.0 |
| Carinthia | 73 | 5.1 |
| Styria | 52 | 3.6 |
| Burgenland | 54 | 3.7 |
| Salzburg | 26 | 1.8 |
| Tyrol | 53 | 3.7 |
| Vorarlberg | 8 | 0.5 |
| Work sector | ||
| Craft and Trade | 334 | 23.2 |
| Industry | 279 | 19.3 |
| Commerce | 223 | 15.5 |
| Bank/insurance | 77 | 5.3 |
| Information/consulting | 75 | 5.2 |
| Gastronomy/tourism | 66 | 4.6 |
| Transport/traffic | 51 | 3.5 |
| Close-contact services | 44 | 3.1 |
| Other | 293 | 20.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, K.; Humer, E.; Pieh, C.; Plener, P.L.; Jesser, A. Burdens of Apprentices Caused by the COVID-19 Pandemic and How They Deal with Them: A Qualitative Study Using Content Analysis One-Year Post-Breakout. Healthcare 2022, 10, 2206. https://doi.org/10.3390/healthcare10112206
Haider K, Humer E, Pieh C, Plener PL, Jesser A. Burdens of Apprentices Caused by the COVID-19 Pandemic and How They Deal with Them: A Qualitative Study Using Content Analysis One-Year Post-Breakout. Healthcare. 2022; 10(11):2206. https://doi.org/10.3390/healthcare10112206
Chicago/Turabian StyleHaider, Katja, Elke Humer, Christoph Pieh, Paul L. Plener, and Andrea Jesser. 2022. "Burdens of Apprentices Caused by the COVID-19 Pandemic and How They Deal with Them: A Qualitative Study Using Content Analysis One-Year Post-Breakout" Healthcare 10, no. 11: 2206. https://doi.org/10.3390/healthcare10112206