
National Vaccination and Local Intervention Impacts on COVID-19 Cases

 , ,
, ,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Research Method
2.1. Data Description
2.2. Causal Impact Analysis and Neural Networks
2.3. Metrics Evaluation
3. Results and Discussion
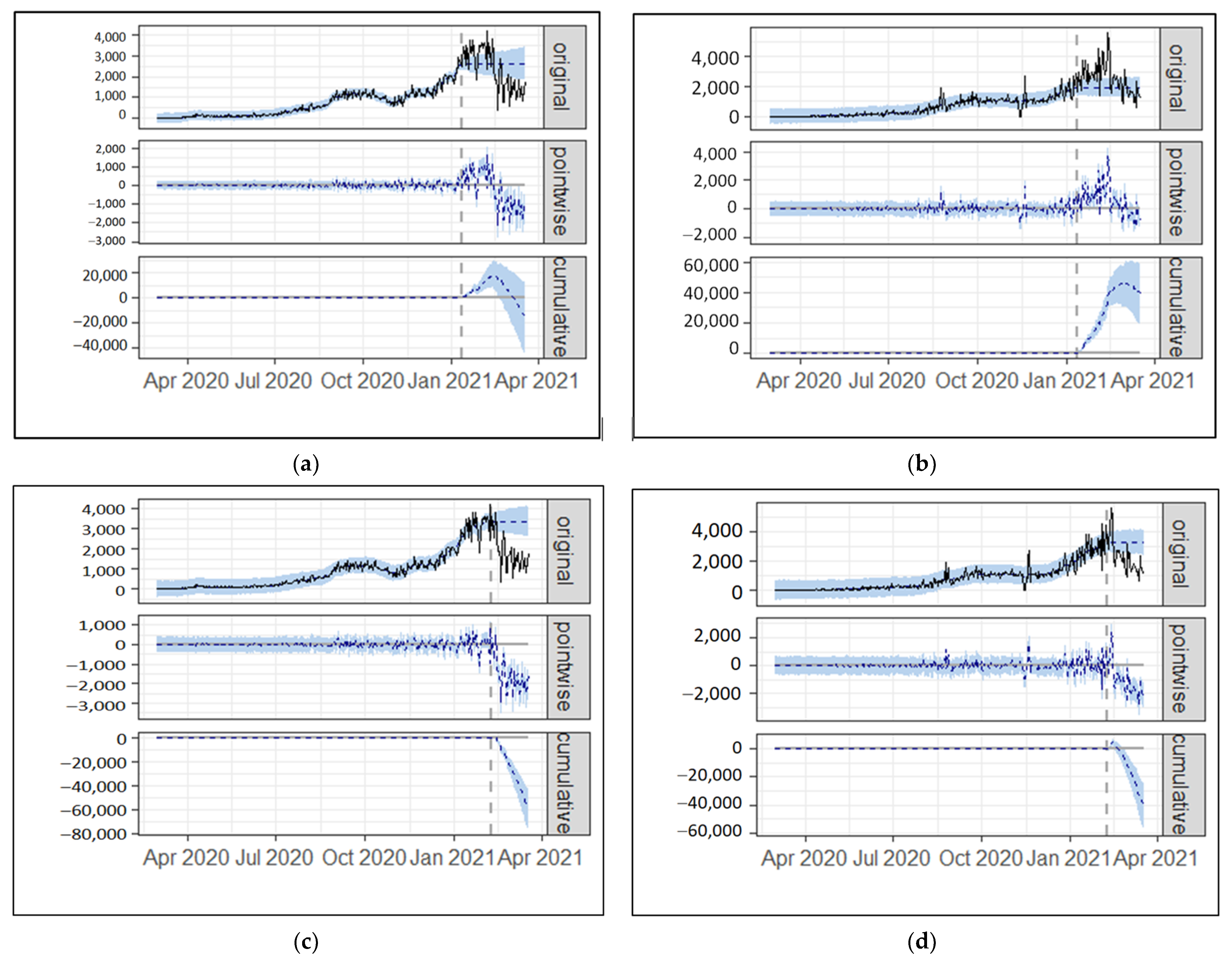
3.1. Causal Impact Analysis
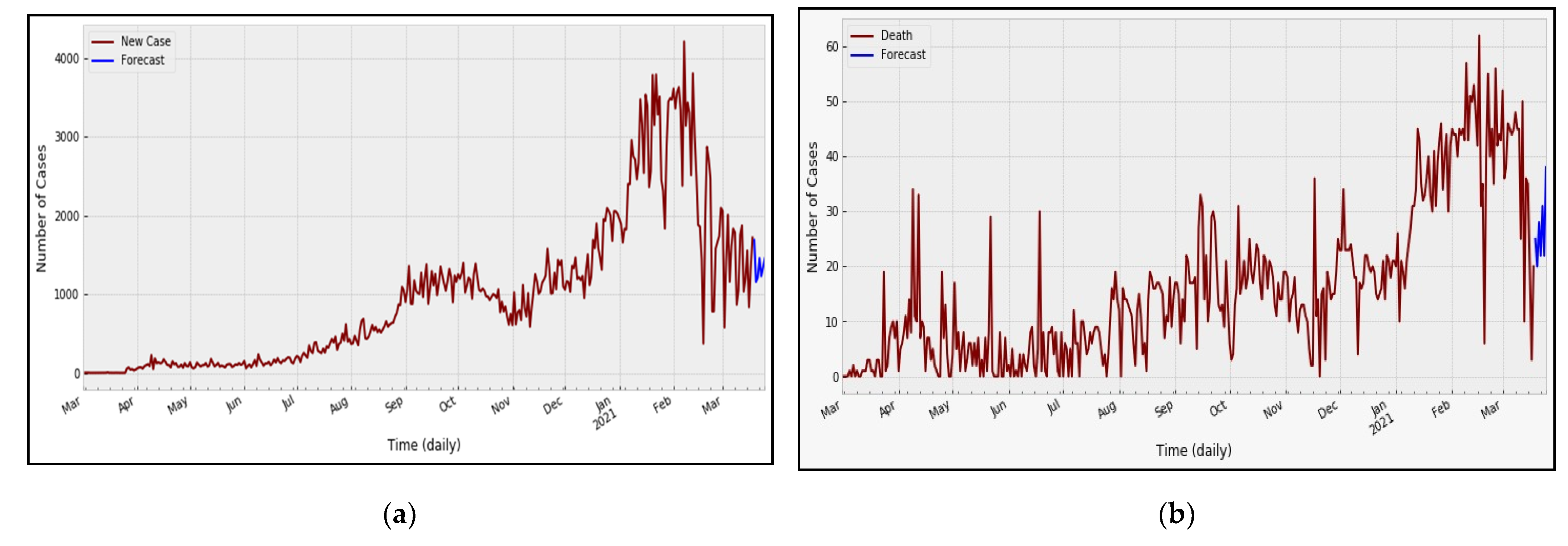
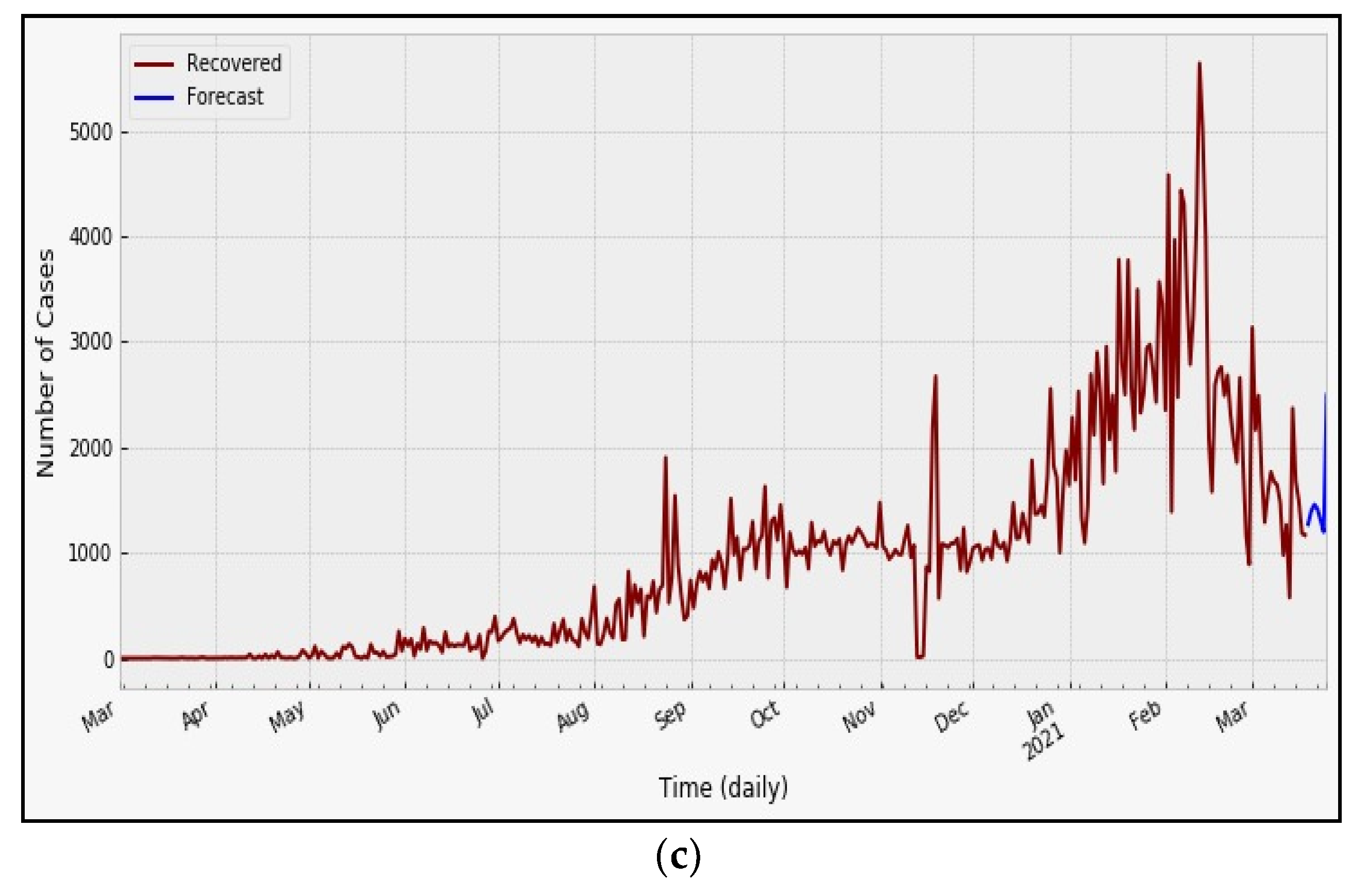
3.2. NNAR Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Djalante, R.; Lassa, J.; Nurhidayah, L.; Minh, H.V.; Mahendradhata, Y.; Ngoc, N.T. The ASEAN’s responses to COVID-19: A policy sciences analysis. PsyArXiv 2020, 368. [Google Scholar] [CrossRef]
- Gralinski, L.E.; Menachery, V.D. Return of the coronavirus: 2019-nCoV. Viruses 2020, 12, 135. [Google Scholar] [CrossRef] [Green Version]
- Ren, L.L.; Wang, Y.M.; Wu, Z.Q.; Xiang, Z.C.; Guo, L.; Xu, T.; Jiang, Y.Z.; Xiong, Y.; Li, Y.J.; Li, H.; et al. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020, 133, 1015. [Google Scholar] [CrossRef]
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulter, N. Lower Blood Pressure in South Asia? Trial Evidence. N. Engl. J. Med. 2020, 382, 758–760. [Google Scholar] [CrossRef] [PubMed]
- Culp, W.C. Coronavirus Disease 2019: In-Home Isolation Room Construction. A A Pract. 2020, 14, e01218. [Google Scholar] [CrossRef]
- Tosepu, R.; Gunawan, J.; Savitri, D.; Ode, L.; Imran, A.; Lestari, H. Correlation between weather and Covid-19 pandemic in Jakarta, Indonesia. Sci. Total Environ. 2020, 725, 138436. [Google Scholar] [CrossRef] [PubMed]
- Rahmadi, A.; Fasyah, I.; Sudigyo, D.; Budiarto, A.; Mahesworo, B.; Hidayat, A.A.; Pardamean, B. Comparative study of predicted miRNA between Indonesia and China (Wuhan) SARS-CoV-2: A bioinformatics analysis. Genes Genom. 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Kristantyo Wisnubroto Momentum Perbaiki Layanan Kesehatan Nasional. Available online: https://indonesia.go.id/kategori/indonesia-dalam-angka/1970/momentum-perbaiki-layanan-kesehatan-nasional (accessed on 2 March 2021).
- Djalante, R.; Lassa, J.; Setiamarga, D.; Mahfud, C.; Sudjatma, A.; Indrawan, M.; Haryanto, B.; Sinapoy, M.S.; Rafliana, I.; Djalante, S.; et al. Review and analysis of current responses to COVID-19 in Indonesia: Period of January to March 2020. Prog. Disaster Sci. 2020, 6, 100091. [Google Scholar] [CrossRef] [PubMed]
- Hudaefi, F.A.; Caraka, R.E.; Wahid, H. Zakāh administration in times of Covid-19 pandemic in Indonesia: A knowledge discovery via text mining. Int. J. Islamic Middle East. Financ. Manag. 2021. [Google Scholar] [CrossRef]
- Hudaefi, F.A.; Beik, I.S. Digital zakah campaign in time of Covid-19 pandemic in Indonesia: A netnographic study. J. Islam. Mark. 2021, 12, 498–517. [Google Scholar] [CrossRef]
- Isaifan, R.J. The dramatic impact of coronavirus outbreak on air quality: Has it saved as much as it has killed so far? Glob. J. Environ. Sci. Manag. 2020, 6, 275–288. [Google Scholar] [CrossRef]
- Caraka, R.E.; Lee, Y.; Kurniawan, R.; Herliansyah, R.; Kaban, P.A.; Nasution, B.I.; Gio, P.U.; Chen, R.C.; Toharudin, T.; Pardamean, B. Impact of COVID-19 large scale restriction on environment and economy in Indonesia. Glob. J. Environ. Sci. Manag. 2020, 6, 65–84. [Google Scholar] [CrossRef]
- Shammi, M.; Bodrud-Doza, M.; Towfiqul Islam, A.R.M.; Rahman, M.M. COVID-19 pandemic, socioeconomic crisis and human stress in resource-limited settings: A case from Bangladesh. Heliyon 2020, 6, e04063. [Google Scholar] [CrossRef]
- Caraka, R.E.; Yusra, Y.; Toharudin, T.; Chen, R.C.; Basyuni, M.; Juned, V.; Gio, P.U.; Pardamean, B. Did Noise Pollution Really Improve during COVID-19 ? Evidence from Taiwan. Sustainability 2021, 13, 5946. [Google Scholar] [CrossRef]
- Susanto, A.P.; Findyartini, A.; Taher, A.; Susilaradeya, D.P.; Ariawan, I.; Dartanto, T.; Takwin, B.; Prasodjo, I.B.; Yusuf, P.A.; Sudarmono, P.P.; et al. COVID-19 in Indonesia: Challenges and Multidisciplinary Perspectives for a Safe and Productive New Normal. Acta Med. Indones. 2020, 52, 423–430. [Google Scholar] [PubMed]
- Sparrow, R.; Dartanto, T.; Hartwig, R. Indonesia Under the New Normal: Challenges and the Way Ahead. Bull. Indones. Econ. Stud. 2020, 56, 269–299. [Google Scholar] [CrossRef]
- Gao, Q.; Bao, L.; Mao, H. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77–81. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Riad, A.; Sağıroğlu, D.; Üstün, B.; Attia, S.; Klugar, M. Prevalence and Risk Factors of CoronaVac Side Effects: An Independent Cross-Sectional Study Among Healthcare Workers in Turkey. J. Clin. Med. 2021, 10, 2629. [Google Scholar] [CrossRef]
- Zhao, H.; Merchant, N.N.; McNulty, A.; Radcliff, T.A.; Cote, M.J.; Fischer, R.S.B.; Sang, H.; Ory, M.G. COVID-19: Short term prediction model using daily incidence data. PLoS ONE 2021, 16, 1–14. [Google Scholar] [CrossRef]
- Nurlaila, I.; Hidayat, A.A.; Pardamean, B. Lockdown strategy worth lives: The SEIRD modelling in COVID-19 outbreak in Indonesia. In Proceedings of the IOP Conference Series: Earth and Environmental Science, Jakarta, Indonesia, 23–24 June 2020; Volume 729. [Google Scholar] [CrossRef]
- Soyiri, I.N.; Reidpath, D.D. An overview of health forecasting. Environ. Health Prev. Med. 2013, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Muhyiddin, M. Covid-19, New Normal, dan Perencanaan Pembangunan di Indonesia. J. Perenc. Pembang. Indones. J. Dev. Plan. 2020, 4, 240–252. [Google Scholar] [CrossRef]
- Toharudin, T.; Pontoh, R.S.; Caraka, R.E.; Zahroh, S.; Akbar, A.; Pardamean, B.; Chen, R.-C. Indonesia in Facing New Normal: An Evidence Hybrid Forecasting of COVID-19 Cases Using. Eng. Lett. 2021, 29, 1–10. [Google Scholar]
- Petropoulos, F.; Makridakis, S.; Stylianou, N. COVID-19: Forecasting confirmed cases and deaths with a simple time series model. Int. J. Forecast. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brodersen, K.H.; Gallusser, F.; Koehler, J.; Remy, N.; Scott, S.L. Inferring causal impact using bayesian structural time-series models. Ann. Appl. Stat. 2015, 9, 247–274. [Google Scholar] [CrossRef]
- Scott, S.L.; Varian, H.R. Predicting the present with Bayesian structural time series. Int. J. Math. Model. Numer. Optim. 2014, 5, 4–23. [Google Scholar] [CrossRef]
- Brodersen, K.H.; Hauser, A. Package CausalImpact. Available online: https://cran.r-project.org/web/packages/CausalImpact/vignettes/CausalImpact.html (accessed on 1 January 2021).
- Yasin, H.; Warsito, B.; Santoso, R.; Suparti, S. Soft Computation Vector Autoregressive Neural Network (VAR-NN) GUI-Based. In Proceedings of the E3S Web of Conferences, Semarang, Indonesia, 14–15 August 2018; Volume 73, p. 13008. [CrossRef] [Green Version]
- Endharta, A.J. Short term load demand forecasting in Indonesia by using double seasonal recurrent Neural networks. Int. J. Math. Model. Methods Appl. Sci. 2009, 3, 171–178. [Google Scholar]
- Suhermi, N.; Permata, R.P.; Rahayu, S.P. Forecasting the Search Trend of Muslim Clothing in Indonesia on Google Trends Data Using ARIMAX and Neural Network. In Proceedings of the Communications in Computer and Information Science, Iizuka, Japan, 28–29 August 2019. [Google Scholar]
- Warsito, B.; Yasin, H.; Prahutama, A. Particle Swarm Optimization to Obtain Weights in Neural Network. Matematika 2019, 35. [Google Scholar] [CrossRef]
- Caraka, R.E.; Chen, R.C.; Yasin, H.; Pardamean, B.; Toharudin, T.; Wu, S.H. Prediction of Status Particulate Matter 2.5 using State Markov Chain Stochastic Process and HYBRID VAR-NN-PSO. IEEE Access 2019, 7, 161654–161665. [Google Scholar] [CrossRef]
- Patan, K. Neural Networks. In Studies in Systems, Decision and Control; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Haykin, S.S. Neural Networks and Learning Machines; Prentice Hall: New York, NY, USA, 2009; Volume 3, ISBN 9780131471399. [Google Scholar]
- Suhermi, N.; Prastyo, D.D.; Ali, B. Roll motion prediction using a hybrid deep learning and ARIMA model. Procedia Comput. Sci. 2018, 144, 251–258. [Google Scholar] [CrossRef]
- Caraka, R.E.; Chen, R.C.; Yasin, H.; Lee, Y.; Pardamean, B. Hybrid Vector Autoregression Feedforward Neural Network with Genetic Algorithm Model for Forecasting Space-Time Pollution Data. Indones. J. Sci. Technol. 2021, 6, 243–266. [Google Scholar]
- Gers, F.A.; Schmidhuber, J.; Cummins, F. Learning to forget: Continual prediction with LSTM. Neural Comput. 2000, 12, 2451–2471. [Google Scholar] [CrossRef]
- Yasin, H.; Warsito, B.; Santoso, R. Feed Forward Neural Network Modeling for Rainfall Prediction. In Proceedings of the E3S Web of Conferences, Semarang, Indonesia, 14–15 August 2018; pp. 1–5. [Google Scholar]
- Toharudin, T.; Pontoh, R.S.; Caraka, R.E.; Zahroh, S.; Lee, Y.; Chen, R.C. Employing Long Short-Term Memory and Facebook Prophet Model in Air Temperature Forecasting. Commun. Stat. Simul. Comput. 2021, 1–24. [Google Scholar] [CrossRef]
- Kaimian, H.; Li, Q.; Wu, C.; Qi, Y.; Mo, Y.; Chen, G.; Zhang, X.; Sachdeva, S. Evaluation of different machine learning approaches to forecasting PM2.5 mass concentrations. Aerosol Air Qual. Res. 2019, 19, 1400–1410. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, S.; Prastuti, M. S-GSTAR-SUR model for seasonal spatio temporal data forecasting. Malays. J. Math. Sci. 2016, 10, 53–65. [Google Scholar]
- De Gooijer, J.G.; Hyndman, R.J. 25 years of time series forecasting. Int. J. Forecast. 2006, 22, 443–473. [Google Scholar] [CrossRef] [Green Version]
- Pontoh, R.S.; Solichatus, Z.; Hidayat, Y.; Aldella, R.; Jiwani, N.M. Sukono Covid-19 modelling in south korea using a time series approach. Int. J. Adv. Sci. Technol. 2020, 29, 1620–1632. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.C.; Chan, K.N.; Hu, W.H.; Lam, W.K.; Zheng, L.; Tipoe, G.L.; Sun, J.; Leung, R.; Tsang, K.W. The effect of aging on nasal mucociliary clearance, beat frequency, and ultrastructure of respiratory cilia. Am. J. Respir. Crit. Care Med. 2001, 163, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BASE Medicine Task Force. COVID-19: Facts and Recommendations from A to Z. Sci. Insigt. 2020, 33, 138–158. [Google Scholar] [CrossRef]
- Yousefifard, M.; Zali, A.; Mohamed Ali, K.; Madani Neishaboori, A.; Zarghi, A.; Hosseini, M.; Safari, S.; Ali, M.K.; Neishaboori, M.A. Antiviral Therapy in Man-agement of COVID-19: A Systematic Review on Current Evidence. Arch. Acad. Emerg. Med. 2020, 8, 45. [Google Scholar]
- Scagnolari, C.; Vicenzi, E.; Bellomi, F.; Stillitano, M.G.; Pinna, D.; Poli, G.; Clementi, M.; Dianzani, F.; Antonelli, G. Increased sensitivity of SARS-coronavirus to a combination of human type I and type II interferons. Antivir. Ther. 2004, 9, 1003–1011. [Google Scholar]
- Stockman, L.J.; Bellamy, R.; Garner, P. SARS: Systematic review of treatment effects. PLoS Med. 2006, 3, 1525–1531. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Suhartono, D.E.A.; Prastyo, D.D.; Kuswanto, H.; Lee, M.H. Deep neural network for forecasting inflow and outflow in Indonesia. Sains Malays. 2019, 48, 1787–1798. [Google Scholar] [CrossRef]
- Sunaryo, S.; Suhartono, J.A. Double Seasonal Recurrent Neural Networks for Forecasting Short Term Electricity Load Demand in Indonesia. In Recurrent Neural Networks for Temporal Data Processing; IntechOpen: London, UK, 2011; pp. 1–16. [Google Scholar]
- Suhartono, S.; Prastyo, D.D.; Kuswanto, H.; Lee, M.H. Comparison between VAR, GSTAR, FFNN-VAR and FFNN-GSTAR Models for Forecasting Oil Production Methods. Mat. Malays. J. Ind. Appl. Math. 2018, 34, 103–111. [Google Scholar]
- Ng’andu, S.K.; Haambokoma, N.M.; Milingo, T.L.C. The Contribution of Behavioural Theories of Learning to Education; The University Of Zambia School of Education: Zuka, Zambia, 2002. [Google Scholar]
- Sudiana, K.; Sule, E.T.; Soemaryani, I.; Yunizar, Y. The development and validation of the Penta Helix construct. Bus. Theory Pract. 2020, 21, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, M.; McCollum, D.; Echeverri, L.G.; Riahi, K.; Parkinson, S. A Guide To SDG Interactions: From Science to Implementation. In A Guide To SDG Interactions: From Science to Implementation; International Council for Science: Paris, France, 2017; ISBN 9781844078943. [Google Scholar]
- Lin, C.; Braund, W.E.; Auerbach, J.; Chou, J.-H.; Teng, J.-H.; Tu, P.; Mullen, J. Policy Decisions and Use of Information Technology to Fight 2019 Novel Coronavirus Disease, Taiwan. Emerg. Infect. Dis. 2020, 26, 1506. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Daily New Cases | Recovered Cases |
|---|---|---|
| Vaccination | 0.16649 | 0.00219 |
| PPKM Jakarta | 0.00106 | 0.00109 |
| Number of Hidden Nodes | Number of Lags | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | ||
| Daily New Cases | 1 | 31.53 | 28.73 | 28.66 | 28.86 | 29.63 | 32.89 | 38.82 | 37.97 | 39.94 |
| 2 | 28.22 | 26.97 | 27.46 | 26.66 | 28.03 | 27.97 | 29.92 | 29.26 | 26.67 | |
| 3 | 19.88 | 19.02 | 19.66 | 18.62 | 18.37 | 17.84 | 16.93 | 16.03 | 13.15 | |
| 4 | 14.19 | 11.24 | 11.93 | 11.03 | 9.74 | 9.86 | 8.72 | 9.49 | 7.25 | |
| 5 | 9.26 | 8.2 | 8.09 | 6.11 | 5.86 | 5.22 | 5.18 | 4.54 | 4.44 | |
| 6 | 5.85 | 5.9 | 5.19 | 4.37 | 3.99 | 3.18 | 2.63 | 3.58 | 2.83 | |
| 7 | 5.87 | 3.7 | 2.69 | 3.24 | 2.42 | 2.36 | 2.2 | 2.29 | 2.03 | |
| 8 | 3.6 | 2.76 | 2.64 | 1.95 | 1.99 | 1.76 | 1.79 | 1.71 | 1.7 | |
| 9 | 3.12 | 2.14 | 2.08 | 1.89 | 1.77 | 1.61 | 1.53 | 1.62 | 1.31 | |
| 10 | 2.57 | 1.8 | 1.63 | 1.42 | 1.46 | 1.43 | 1.41 | 1.29 | 1.25 | |
| 11 | 2.09 | 1.95 | 1.74 | 1.51 | 1.37 | 1.27 | 1.27 | 1.28 | 1.26 | |
| 12 | 1.9 | 1.55 | 1.53 | 1.28 | 1.28 | 1.28 | 1.23 | 1.2 | 1.16 | |
| 13 | 1.8 | 1.48 | 1.45 | 1.24 | 1.25 | 1.24 | 1.21 | 1.2 | 1.17 | |
| 14 | 1.72 | 1.48 | 1.27 | 1.22 | 1.21 | 1.28 | 1.15 | 1.14 | 1.13 | |
| Death | 1 | 99.08 | 104.59 | 104.89 | 105.47 | 104.63 | 106.52 | 108.36 | 110.75 | 110.61 |
| 2 | 89.23 | 88.9 | 89.96 | 97.03 | 91.16 | 85.81 | 90.94 | 84.49 | 87.03 | |
| 3 | 58.97 | 57.52 | 52.62 | 58.28 | 60.69 | 55.34 | 56.36 | 60.05 | 42.11 | |
| 4 | 39.79 | 38.61 | 32.31 | 37.23 | 36.02 | 33.87 | 28.06 | 26.69 | 24.47 | |
| 5 | 29.91 | 24.98 | 25.71 | 21.73 | 21.74 | 18.23 | 16.89 | 13.12 | 15.7 | |
| 6 | 22.56 | 18.76 | 16.32 | 14.18 | 14.92 | 10.89 | 10.69 | 10.31 | 11.8 | |
| 7 | 15.14 | 14.84 | 13.85 | 11.05 | 11.03 | 8.8 | 8.13 | 8.7 | 7.33 | |
| 8 | 13.65 | 12.62 | 12.67 | 8.63 | 8.35 | 7.06 | 7.56 | 7.55 | 7.72 | |
| 9 | 12.04 | 11.03 | 9.76 | 7.53 | 7.71 | 6.65 | 6.78 | 6.95 | 6.63 | |
| 10 | 11.31 | 10.23 | 9.42 | 7.34 | 6.98 | 6.36 | 6.46 | 6.15 | 6.3 | |
| 11 | 10.47 | 9.21 | 8.6 | 6.59 | 6.37 | 6.12 | 6.04 | 6.51 | 6.11 | |
| 12 | 10.18 | 9.51 | 8.33 | 6.33 | 6.4 | 6.08 | 5.88 | 6.1 | 5.95 | |
| 13 | 9.2 | 8.29 | 7.97 | 6.2 | 6.39 | 6.2 | 6.14 | 5.87 | 5.89 | |
| 14 | 9.13 | 8.06 | 7.72 | 6.15 | 6.16 | 6.12 | 6.1 | 5.86 | 5.98 | |
| Recovered | 1 | 25.75 | 27.65 | 27.98 | 27.58 | 29.84 | 29.24 | 29.42 | 28.98 | 28.98 |
| 2 | 29.67 | 29.63 | 29.41 | 29.77 | 30.53 | 31.12 | 30.43 | 32.01 | 32.01 | |
| 3 | 27 | 25.75 | 25.17 | 24.92 | 26.33 | 23.27 | 23.34 | 22.4 | 22.4 | |
| 4 | 24.76 | 21.31 | 20.82 | 22.36 | 16.73 | 15.14 | 15.58 | 15.87 | 15.87 | |
| 5 | 21.67 | 18.8 | 17.33 | 16.44 | 13.75 | 12.76 | 12.17 | 12.04 | 12.04 | |
| 6 | 18.97 | 15.47 | 13.93 | 12.9 | 10.54 | 10.45 | 9.89 | 9.25 | 9.25 | |
| 7 | 14.35 | 14.41 | 10.8 | 10.93 | 8.99 | 9.34 | 8.28 | 8.39 | 8.39 | |
| 8 | 13.09 | 11.72 | 10.43 | 9.84 | 8.87 | 8.19 | 7.8 | 7.83 | 7.83 | |
| 9 | 11.36 | 10.44 | 9.97 | 8.92 | 8 | 7.66 | 7.62 | 7.72 | 7.72 | |
| 10 | 10.7 | 9.099 | 8.565 | 8.431 | 7.647 | 7.571 | 7.246 | 7.277 | 7.277 | |
| 11 | 10.2 | 8.421 | 8.048 | 7.976 | 7.509 | 7.359 | 7.33 | 7.399 | 7.399 | |
| 12 | 9.56 | 8.068 | 7.96 | 7.862 | 7.402 | 7.378 | 7.279 | 7.238 | 7.238 | |
| 13 | 8.93 | 8.096 | 7.984 | 7.611 | 7.368 | 7.345 | 7.182 | 7.179 | 7.179 | |
| 14 | 8.57 | 7.954 | 7.528 | 7.625 | 7.396 | 7.335 | 7.268 | 7.183 | 7.183 | |
| Hidden Nodes | Split Ratio | |||||
|---|---|---|---|---|---|---|
| 80/20 | 70/30 | |||||
| Recovered | New Case | Death | Recovered | New Case | Death | |
| 1 | 32.66 | 32.69 | 45.00 | 27.63 | 25.96 | 38.76 |
| 2 | 22.59 | 20.91 | 36.95 | 19.89 | 17.58 | 32.22 |
| 3 | 14.90 | 12.42 | 25.86 | 13.99 | 12.39 | 24.40 |
| 4 | 9.43 | 7.38 | 17.06 | 9.35 | 8.57 | 17.32 |
| 5 | 5.87 | 4.26 | 10.76 | 7.11 | 5.78 | 12.90 |
| 6 | 3.75 | 2.40 | 8.45 | 4.88 | 3.84 | 9.76 |
| 7 | 2.54 | 1.19 | 5.12 | 3.41 | 3.02 | 7.60 |
| 8 | 2.10 | 0.79 | 3.44 | 2.45 | 2.23 | 6.14 |
| 9 | 1.71 | 0.65 | 2.82 | 1.97 | 1.73 | 4.68 |
| 10 | 1.65 | 0.45 | 1.70 | 1.79 | 1.38 | 3.99 |
| 11 | 1.51 | 0.33 | 1.56 | 1.42 | 1.17 | 2.96 |
| 12 | 1.48 | 0.30 | 0.99 | 1.32 | 1.09 | 2.68 |
| 13 | 1.42 | 0.28 | 0.96 | 1.19 | 0.91 | 2.20 |
| 14 | 1.45 | 0.26 | 0.78 | 1.06 | 0.87 | 1.82 |
| Cases | Model | RMSE | MAE |
|---|---|---|---|
| Daily new | NNAR (14,14) | 50.74 | 30.64 |
| Death | NNAR (14,14) | 2.79 | 1.45 |
| Recovered | NNAR (14,14) | 76.48 | 41.16 |
| Date | Daily New Cases | Death Cases | Recovered Cases | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lo 95 | Point | Hi 95 | Actual | Lo 95 | Point | Hi 95 | Actual | Lo 95 | Point | Hi 95 | Actual | |
| 19/03/2021 | 1464 | 1568 | 1678 | 1588 | 19 | 25 | 30 | 24 | 1097 | 1245 | 1388 | 1175 |
| 20/03/2021 | 1179 | 1282 | 1385 | 1935 | 15 | 20 | 26 | 22 | 1246 | 1401 | 1561 | 1184 |
| 21/03/2021 | 1103 | 1209 | 1313 | 1638 | 23 | 28 | 34 | 23 | 1297 | 1453 | 1599 | 1884 |
| 22/03/2021 | 1259 | 1364 | 1466 | 1474 | 16 | 22 | 28 | 8 | 1293 | 1432 | 1575 | 1715 |
| 23/03/2021 | 1259 | 1371 | 1481 | 816 | 26 | 31 | 37 | 11 | 1162 | 1314 | 1467 | 1691 |
| 24/03/2021 | 1219 | 1321 | 1415 | 890 | 15 | 21 | 27 | 11 | 1063 | 1222 | 1396 | 1986 |
| 25/03/2021 | 1334 | 1431 | 1533 | 1727 | 32 | 38 | 43 | 12 | 2333 | 2485 | 2643 | 490 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toharudin, T.; Pontoh, R.S.; Caraka, R.E.; Zahroh, S.; Kendogo, P.; Sijabat, N.; Sari, M.D.P.; Gio, P.U.; Basyuni, M.; Pardamean, B. National Vaccination and Local Intervention Impacts on COVID-19 Cases. Sustainability 2021, 13, 8282. https://doi.org/10.3390/su13158282
Toharudin T, Pontoh RS, Caraka RE, Zahroh S, Kendogo P, Sijabat N, Sari MDP, Gio PU, Basyuni M, Pardamean B. National Vaccination and Local Intervention Impacts on COVID-19 Cases. Sustainability. 2021; 13(15):8282. https://doi.org/10.3390/su13158282
Chicago/Turabian StyleToharudin, Toni, Resa Septiani Pontoh, Rezzy Eko Caraka, Solichatus Zahroh, Panji Kendogo, Novika Sijabat, Mentari Dara Puspita Sari, Prana Ugiana Gio, Mohammad Basyuni, and Bens Pardamean. 2021. "National Vaccination and Local Intervention Impacts on COVID-19 Cases" Sustainability 13, no. 15: 8282. https://doi.org/10.3390/su13158282