
Chest CT Findings and SARS-CoV-2 Infection in Trauma Patients—Is There a Prediction towards Higher Complication Rates?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Study Design
2.2. Definitions
2.3. Statistics
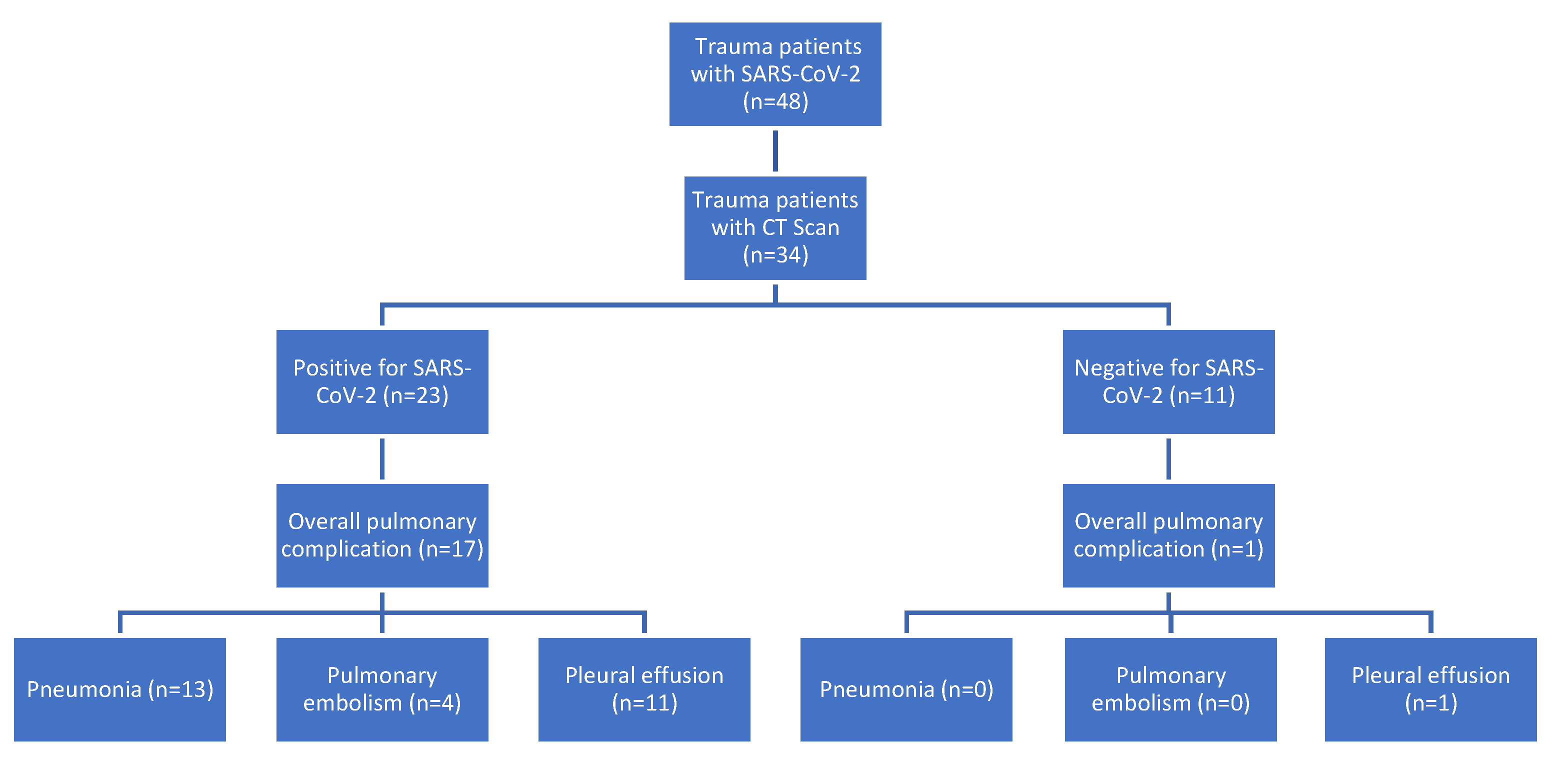
3. Results
Patient Data and Demographics
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Gavrilov, D.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; et al. Coronavirus Pandemic (COVID-19). 2021. Available online: https://ourworldindata.org/coronavirus (accessed on 22 November 2021).
- Mallah, S.I.; Ghorab, O.K.; Al-Salmi, S.; Abdellatif, O.S.; Tharmaratnam, T.; Iskandar, M.A.; Sefen, J.A.N.; Sidhu, P.; Atallah, B.; El-Lababidi, R.; et al. COVID-19: Breaking down a global health crisis. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 35. [Google Scholar] [CrossRef] [PubMed]
- Moletta, L.; Pierobon, E.S.; Capovilla, G.; Costantini, M.; Salvador, R.; Merigliano, S.; Valmasoni, M. International guidelines and recommendations for surgery during Covid-19 pandemic: A Systematic Review. Int. J. Surg. 2020, 79, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, R.; Edwards, S.; Kurihara, H.; Bass, G.A.; Balogh, Z.J.; Tilsed, J.; Faccincani, R.; Carlucci, M.; Casas, I.M.; Gaarder, C.; et al. European Society of Trauma and Emergency Surgery (ESTES) recommendations for trauma and emergency surgery preparation during times of COVID-19 infection. Eur. J. Trauma Emerg. Surg. 2020, 46, 505–510. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: An international cohort study. Lancet 2020, 396, 27–38. [Google Scholar] [CrossRef]
- Halvachizadeh, S.; Baradaran, L.; Cinelli, P.; Pfeifer, R.; Sprengel, K.; Pape, H.-C. How to detect a polytrauma patient at risk of complications: A validation and database analysis of four published scales. PLoS ONE 2020, 15, e0228082. [Google Scholar] [CrossRef]
- WHO. The Top 10 Causes of Death. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 20 November 2021).
- Pfeifer, R.; Pape, H.C. Diagnostics and treatment strategies for multiple trauma patients. Chirurg 2016, 87, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Pape, H.C.; Giannoudis, P.V.; Krettek, C.; Trentz, O. Timing of fixation of major fractures in blunt polytrauma: Role of conventional indicators in clinical decision making. J. Orthop. Trauma 2005, 19, 551–562. [Google Scholar] [CrossRef]
- Pape, H.-C.; Tornetta, P.; Tarkin, I.; Tzioupis, C.; Sabeson, V.; Olson, S.A. Timing of Fracture Fixation in Multitrauma Patients: The Role of Early Total Care and Damage Control Surgery. J. Am. Acad. Orthop. Surg. 2009, 17, 541–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copes, W.S.; Champion, H.R.; Sacco, W.J.; Lawnick, M.M.; Keast, S.L.; Bain, L.W. The Injury Severity Score Revisited. J. Trauma: Inj. Infect. Crit. Care 1988, 28, 69–77. [Google Scholar] [CrossRef] [PubMed]
- von Rüden, C.; Bühren, V.; Perl, M. Polytrauma Management-Treatment of Severely Injured Patients in ER and OR. Z Orthop. Unfall. 2017, 155, 603–622. [Google Scholar]
- Vasquez, C.R.; Disanto, T.; Reilly, J.P.; Forker, C.M.; Holena, D.N.; Wu, Q.; Lanken, P.N.; Christie, J.D.; Shashaty, M.G. Relationship of body mass index, serum creatine kinase, and acute kidney injury after severe trauma. J. Trauma Acute Care Surg. 2020, 89, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Loftis, K.L.; Price, J.; Gillich, P.J. Evolution of the Abbreviated Injury Scale: 1990–2015. Traffic Inj. Prev. 2018, 19, S109–S113. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA-Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Rossaint, R.; Bouillon, B.; Cerny, V.; Coats, T.J.; Duranteau, J.; Fernández-Mondéjar, E.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Nardi, G.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fourth edition. Crit. Care 2016, 20, 100. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, B.; Probst, C.; Maegele, M.; Wafaisade, A.; Helm, P.; Mutschler, M.; Brockamp, T.; Shafizadeh, S.; Paffrath, T. Emergency room management of multiple trauma: ATLS® and S3 guidelines. Chirurg 2013, 84, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, B.; Marzi, I. The updated German “Polytrauma–Guideline”: An extensive literature evaluation and treatment recommendation for the care of the critically injured patient. Eur. J. Trauma Emerg. Surg. 2018, 44, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvagno, S.M.; Nahmias, J.T.; Young, D.A. Advanced Trauma Life Support® Update 2019: Management and Applications for Adults and Special Populations. Anesthesiol. Clin. 2019, 37, 13–32. [Google Scholar] [CrossRef]
- Echeverría-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; Cuscó, M.D.-A.; Ferrández, O.; Horcajada, J.P.; Grau, S. Azithromycin in the treatment of COVID-19: A review. Expert Rev. Anti-Infect. Ther. 2020, 19, 147–163. [Google Scholar] [CrossRef]
- Parasher, A. COVID-19: Current understanding of its Pathophysiology, Clinical presentation and Treatment. Postgrad. Med. J. 2021, 97, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Chrysou, K.; Halat, G.; Hoksch, B.; Schmid, R.A.; Kocher, G.J. Lessons from a large trauma center: Impact of blunt chest trauma in polytrauma patients-still a relevant problem? Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 42. [Google Scholar] [CrossRef]
- Knudson, M.M.; Collins, J.A.; Goodman, S.B.; McCRORY, D.W. Thromboembolism Following Multiple Trauma. J. Trauma Inj. Infect. Crit. Care 1992, 32, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Tilliridou, V.; Kirkbride, R.; Dickinson, R.; Tiernan, J.; Yong, G.L.; van Beek, E.J.; Murchison, J.T.; Williams, M.C. Pulmonary embolism severity before and during the COVID-19 pandemic. Br. J. Radiol. 2021, 94, 20210264. [Google Scholar] [CrossRef] [PubMed]
- Radomski, M.; Zettervall, S.; Schroeder, M.E.; Messing, J.; Dunne, J.; Sarani, B. Critical Care for the Patient with Multiple Trauma. J. Intensiv. Care Med. 2016, 31, 307–318. [Google Scholar] [CrossRef]
- Anderson, F.A., Jr.; Spencer, F.A. Risk factors for venous thromboembolism. Circulation 2003, 107, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glover, T.E.; Sumpter, J.E.; Ercole, A.; Newcombe, V.F.; Lavinio, A.; Carrothers, A.D.; Menon, D.K.; O’Leary, R. Pulmonary embolism following complex trauma: UK MTC observational study. Emerg. Med. J. 2019, 36, 608–612. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Singh, S.P.; Pritam, M.; Pandey, B.; Yadav, T.P. Microstructure, pathophysiology, and potential therapeutics of COVID-19: A comprehensive review. J. Med. Virol. 2021, 93, 275–299. [Google Scholar] [CrossRef]
- Teuwen, L.-A.; Geldhof, V.; Pasut, A.; Carmeliet, P. Author Correction: COVID-19: The vasculature unleashed. Nat. Rev. Immunol. 2020, 20, 448. [Google Scholar] [CrossRef]
- Streiff, M.B.; Agnelli, G.; Connors, J.M.; Crowther, M.; Eichinger, S.; Lopes, R.D.; McBane, R.D.; Moll, S.; Ansell, J. Erratum to: Guidance for the treatment of deep vein thrombosis and pulmonary embolism. J. Thromb. Thrombolysis 2016, 41, 548. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.; Patel, P.; Bhatt, M.; Braun, C.; Begum, H.; Wiercioch, W.; Varghese, J.; Wooldridge, D.; Alturkmani, H.; Thomas, M.; et al. Systematic review and meta-analysis of test accuracy for the diagnosis of suspected pulmonary embolism. Blood Adv. 2020, 4, 4296–4311. [Google Scholar] [CrossRef]
- Schot, M.J.C.; Dekker, A.R.J.; Giorgi, W.G.; Hopstaken, R.M.; De Wit, N.J.; Verheij, T.J.M.; Cals, J.W.L. Diagnostic value of signs, symptoms and diagnostic tests for diagnosing pneumonia in ambulant children in developed countries: A systematic review. NPJ Prim. Care Respir. Med. 2018, 28, 40. [Google Scholar] [CrossRef] [PubMed]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Schälte, G.; Salzberger, B.; Gastmeier, P.; Langer, F.; Wepler, M.; Westhoff, M.; et al. German recommendations for treatment of critically ill patients with COVID-19-version 3. Der Pneumol. 2020, 17, 406–425. [Google Scholar] [CrossRef] [PubMed]
- Kozak, R.; Armstrong, S.M.; Salvant, E.; Ritzker, C.; Feld, J.; Biondi, M.J.; Tsui, H. Recognition of Long-COVID-19 Patients in a Canadian Tertiary Hospital Setting: A Retrospective Analysis of Their Clinical and Laboratory Characteristics. Pathogens 2021, 10, 1246. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ISS ≥ 16 | ISS < 16 | ||
|---|---|---|---|
| Count, n | 48 | 15 | 33 |
| Gender, n = male (%) | 33 (69) | 13 (87) | 20 (61) |
| Mean age, (SD) | 60.3 (19.3) | 55.0 (18.4) | 62.7 (19.6) |
| Median ISS, (SD) | 10 (7.0) | 22.0 (4.7) | 9.0 (2.6) |
| Median AIS head/neck, (SD) | 2 (1.34) | 2.5 (1.1) | 1.3 (1.3) |
| Median AIS chest, (SD) | 0 (1.0) | 0.8 (1.37) | 0.2 (0.73) |
| Median AIS abdomen, (SD) | 0 (1.8) | 1.5 (2.0) | 0.2 (1.6) |
| Median AIS pelvis/extremity, (SD) | 0 (1.9) | 1.5 (1.9) | 1.3 (2.0) |
| Median AIS external, (SD) | 0 (1.92) | 0.7 (0.7) | 0.4 (0.6) |
| Whole-body CT on admission (%) | 34 (71) | 15 (100) | 19 (56) |
| Overall pulmonary complications, n (%) | 19 (40) | 8 (53) | 11 (34) |
| Pulmonary embolism, n (%) | 4 (8) | 3 (20) | 1 (3) |
| Pneumonia, n (%) | 14 (29) | 8 (53) | 6 (19) |
| Pleural effusion, n (%) | 13 (27) | 5 (33) | 8 (25) |
| mortality during admission, n (%) | 4 (8) | 1 (7) | 3 (9) |
| Readmission < 30 days, n (%) | 3 (6) | 1 (7) | 2 (6) |
| Length of stay, mean days (SD) | 9.6 (8.4) | 11 (7.9) | 9.4 (8.7) |
| BMI > 25 kg/m2, n (%) | 18 (38) | 7 (47) | 11 (34) |
| CT Findings Positive for SARS-CoV-2 Pneumonia | CT Findings Negative for SARS-CoV-2 Pneumonia | p Value | ||
|---|---|---|---|---|
| Count (Whole-body CT on admission), n | 34 | 23 | 11 | |
| Median ISS, (SD) | 9 (7.2) | 14.1 (6.9) | 17.5 (7.5) | 0.213 |
| Gender, n = male (%) | 28 (82) | 19 (83) | 9 (82) | |
| Mean age, (SD) | 59.5 (19.1) | 69.3 (14.5) | 37.1 (14.8) | 0.001 |
| Median AIS head/neck, (SD) | 2 (1.2) | 2.2 (1.3) | 1.8 (1.3) | 0.567 |
| Median AIS chest, (SD) | 0 (1.2) | 0.5 (1.2) | 0.3 (1.2) | 0.957 |
| Median AIS abdomen, (SD) | 0 (2.1) | 0.8 (2.2) | 0.9 (2.0) | 0.822 |
| Median AIS pelvis/extremity, (SD) | 0 (2.1) | 0.8 (1.4) | 1.6 (2.9) | 0.077 |
| Median AIS external, (SD) | 0 (0.7) | 0.4 (0.6) | 0.7 (0.8) | 0.137 |
| Overall pulmonary complications, n (%) | 18 (53) | 17 (74) | 1 (9) | 0.001 |
| Pulmonary embolism, n (%) | 4 (12) | 4 (17) | 0 (0) | 0.141 |
| Pneumonia, n (%) | 13 (38) | 13 (57) | 0 (0) | 0.002 |
| Pleural effusion, n (%) | 12 (35) | 11 (48) | 1 (9) | 0.027 |
| Mortality during admission, n (%) | 3 (9) | 3 (13) | 0 (0) | 0.210 |
| Readmission < 30 days, n (%) | 3 (9) | 2 (9) | 1 (9) | 0.952 |
| Length of stay, mean days (SD) | 10.6 (9.0) | 13.1 (10.4) | 7.5 (3.5) | 0.171 |
| BMI > 25 kg/m2, n (%) | 13 (38) | 9 (39) | 4 (34) | 0.215 |
| CT Findings Positive for SARS-CoV-2 Pneumonia | CT Findings Negative for SARS-CoV-2 Pneumonia | p Value | ||
|---|---|---|---|---|
| Count, n | 18 | 9 | 9 | |
| Median ISS, (SD) | 16.1 (7.7) | 16.0 (7.2) | 18.2 (8.0) | 0.256 |
| Gender, n = male (%) | 17 | 9 (100) | 8 (89) | |
| Mean age, (SD) | 49.8 (9.9) | 55.3 (7.5) | 46.5 (11.2) | 0.165 |
| Median AIS head/neck, (SD) | 1.7 (1.2) | 1.6 (1.3) | 1.6 (1.2) | 0.854 |
| Median AIS chest, (SD) | 0.5 (1.2) | 0.7 (1.3) | 0.3 (1.0) | 0.556 |
| Median AIS abdomen, (SD) | 1.6 (2.6) | 1.4 (3.1) | 1.1 (2.2) | 0.438 |
| Median AIS pelvis/extremity, (SD) | 1.7 (2.5) | 0.7 (1.3) | 2.0 (3.0) | 0.089 |
| Media AIS external, (SD) | 0.6 (0.7) | 0.4 (0.5) | 0.7 (0.8) | 0.326 |
| Overall pulmonary complications, n (%) | 6 (33) | 5 (56) | 1 (11) | 0.046 |
| Pulmonary embolism, n (%) | 2 (11) | 2 (22) | 0 (0) | 0.580 |
| Pneumonia, n (%) | 4 (22) | 4 (44) | 0 (0) | 0.023 |
| Pleural effusion, n (%) | 5 (28) | 4 (44) | 1 (11) | 0.114 |
| Mortality during admission, n (%) | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Readmission < 30 days, n (%) | 2 (11) | 1 (11) | 1 (11) | 1.000 |
| Length of stay, mean days (SD) | 11.9 (9.3) | 15.0 (12.6) | 8.8 (2.4) | 0.165 |
| BMI > 25 kg/m2, n (%) | 9 (50) | 5 (56) | 4 (44) | 0.637 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheurer, F.; Halvachizadeh, S.; Berk, T.; Pape, H.-C.; Pfeifer, R. Chest CT Findings and SARS-CoV-2 Infection in Trauma Patients—Is There a Prediction towards Higher Complication Rates? J. Clin. Med. 2022, 11, 6401. https://doi.org/10.3390/jcm11216401
Scheurer F, Halvachizadeh S, Berk T, Pape H-C, Pfeifer R. Chest CT Findings and SARS-CoV-2 Infection in Trauma Patients—Is There a Prediction towards Higher Complication Rates? Journal of Clinical Medicine. 2022; 11(21):6401. https://doi.org/10.3390/jcm11216401
Chicago/Turabian StyleScheurer, Fabrice, Sascha Halvachizadeh, Till Berk, Hans-Christoph Pape, and Roman Pfeifer. 2022. "Chest CT Findings and SARS-CoV-2 Infection in Trauma Patients—Is There a Prediction towards Higher Complication Rates?" Journal of Clinical Medicine 11, no. 21: 6401. https://doi.org/10.3390/jcm11216401