
Effects of the COVID-19 Pandemic on Treatment Efficiency for Traumatic Brain Injury in the Emergency Department: A Multicenter Study in Taiwan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
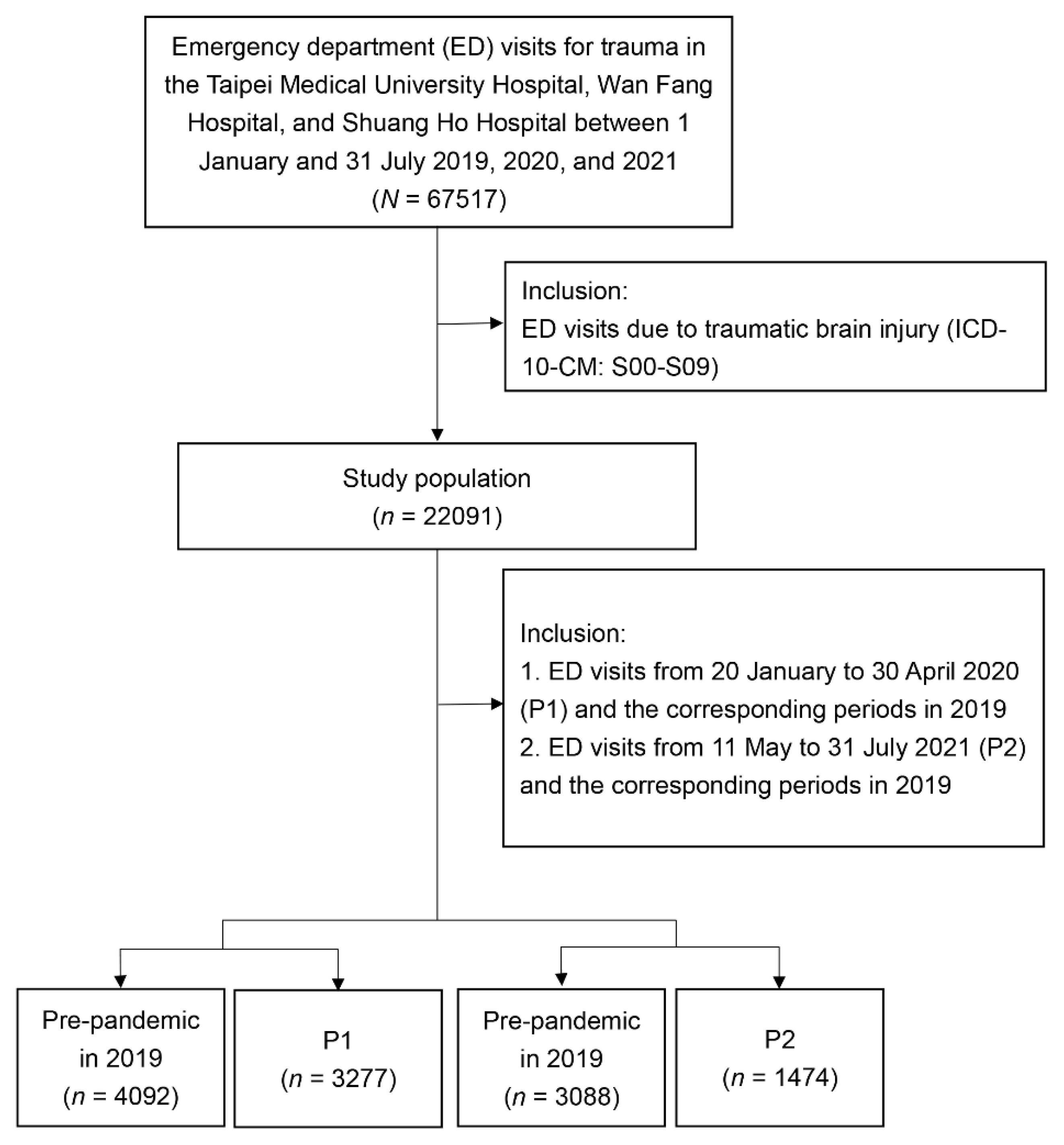
2.2. Sample Selection
2.3. Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jian, S.W.; Kao, C.T.; Chang, Y.C.; Chen, P.F.; Liu, D.P. Risk assessment for COVID-19 pandemic in Taiwan. Int. J. Infect. Dis. 2021, 104, 746–751. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Situation Reports #5—March 31 2020. Available online: https://www.ncfhcc.org/wp-content/uploads/2020/04/5_SitRep_Alliance-COVID_3.31.2020.pdf (accessed on 16 September 2021).
- Weekly Epidemiological Update—14 September 2020. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update--14-september-2020 (accessed on 16 September 2021).
- Crucial Policies for Combating COVID-19. Available online: https://covid19.mohw.gov.tw/en/mp-206.html (accessed on 16 September 2021).
- Tan, T.W.; Tan, H.L.; Chang, M.N.; Lin, W.S.; Chang, C.M. Effectiveness of epidemic preventive policies and hospital strategies in combating COVID-19 outbreak in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 3456. [Google Scholar] [CrossRef]
- Chang, Y.C. Taiwanese Medical and Security Policy towards the COVID-19 Pandemic. A Best Practice; European Intelligence Academy: Athens, Greece, 2021. [Google Scholar]
- Press Releases—Taiwan Centers for Disease Control. Available online: https://www.cdc.gov.tw/En/Category/ListContent/tov1jahKUv8RGSbvmzLwFg?uaid=R1K7gSjoYa7Wojk54nW7fg (accessed on 21 September 2021).
- Sen-Crowe, B.; Sutherland, M.; McKenney, M.; Elkbuli, A. A closer look into global hospital beds capacity and resource shortages during the COVID-19 pandemic. J. Surg. Res. 2021, 260, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Kokudo, N.; Sugiyama, H. Hospital capacity during the COVID-19 pandemic. Glob. Health Med. 2021, 3, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.Y.; Lai, H.W.; Hou, I.L.; Lin, C.H.; Chen, M.K.; Chou, C.C.; Lin, Y.R. Buffer areas in emergency department to handle potential COVID-19 community infection in Taiwan. Travel Med. Infect. Dis. 2020, 36, 101635. [Google Scholar] [CrossRef]
- Garcia, S.; Albaghdadi, M.S.; Meraj, P.M.; Schmidt, C.; Garberich, R.; Jaffer, F.A.; Dixon, S.; Rade, J.J.; Tannenbaum, M.; Chambers, J.; et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J. Am. Coll. Cardiol. 2020, 75, 2871–2872. [Google Scholar] [CrossRef]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Santana, R.; Sousa, J.S.; Soares, P.; Lopes, S.; Boto, P.; Rocha, J.V. The demand for hospital emergency services: Trends during the first month of COVID-19 response. Port. J. Public Health 2020, 38, 30–36. [Google Scholar] [CrossRef]
- Bres Bullrich, M.; Fridman, S.; Mandzia, J.L.; Mai, L.M.; Khaw, A.; Vargas Gonzalez, J.C.; Bagur, R.; Sposato, L.A. COVID-19: Stroke admissions, emergency department visits, and prevention clinic referrals. Can. J. Neurol. Sci. 2020, 47, 693–696. [Google Scholar] [CrossRef]
- Choi, D.H.; Jung, J.Y.; Suh, D.; Choi, J.Y.; Lee, S.U.; Choi, Y.J.; Kwak, Y.H.; Kim, D.K. Impact of the COVID-19 outbreak on trends in emergency department utilization in children: A multicenter retrospective observational study in Seoul metropolitan area, Korea. J. Korean Med. Sci. 2021, 36, e44. [Google Scholar] [CrossRef]
- Chen, J.Y.H.; Chang, F.Y.; Lin, C.S.; Wang, C.H.; Tsai, S.H.; Lee, C.C.; Chen, S.J. Impact of the COVID-19 pandemic on the loading and quality of an emergency department in Taiwan: Enlightenment from a low-risk country in a public health crisis. J. Clin. Med. 2021, 10, 1150. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.F.; Huang, Y.H.; Cheng, C.Y.; Wu, K.H.; Tang, K.S.; Chiu, I.M. Public health interventions for the COVID-19 pandemic reduce respiratory tract infection-related visits at pediatric emergency departments in Taiwan. Front. Public Health 2020, 8, 604089. [Google Scholar] [CrossRef] [PubMed]
- Marin, J.R.; Weaver, M.D.; Yealy, D.M.; Mannix, R.C. Trends in visits for traumatic brain injury to emergency departments in the United States. JAMA 2014, 311, 1917–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandor, A.; Harnan, S.; Goodacre, S.; Pickering, A.; Fitzgerald, P.; Rees, A. Diagnostic accuracy of clinical characteristics for identifying CT abnormality after minor brain injury: A systematic review and meta-analysis. J. Neurotrauma 2012, 29, 707–718. [Google Scholar] [CrossRef]
- Santing, J.A.L.; van den Brand, C.L.; Jellema, K. Traumatic brain injury during the SARS-CoV-2 pandemic. Neurotrauma Rep. 2020, 1, 5–7. [Google Scholar] [CrossRef]
- Jayakumar, N.; Kennion, O.; Villabona, A.R.; Paranathala, M.; Holliman, D. Neurosurgical referral patterns during the coronavirus disease 2019 pandemic: A United Kingdom experience. World Neurosurg. 2020, 144, e414–e420. [Google Scholar] [CrossRef]
- Karthigeyan, M.; Dhandapani, S.; Salunke, P.; Sahoo, S.K.; Kataria, M.S.; Singh, A.; Gendle, C.; Panchal, C.; Chhabra, R.; Jain, K.; et al. The collateral fallout of COVID19 lockdown on patients with head injury from north-west India. Acta Neurochir. 2021, 163, 1053–1060. [Google Scholar] [CrossRef]
- Horan, J.; Duddy, J.C.; Gilmartin, B.; Amoo, M.; Nolan, D.; Corr, P.; Husien, M.B.; Bolger, C. The impact of COVID-19 on trauma referrals to a National Neurosurgical Centre. Ir. J. Med. Sci. 2021, 190, 1281–1293. [Google Scholar] [CrossRef]
- Agarwal, M.; Udare, A.; Alabousi, A.; van der Pol, C.B.; Ramonas, L.; Mascola, K.; Edmonds, B.; Ramonas, M. Impact of the COVID-19 pandemic on emergency CT head utilization in Ontario—An observational study of tertiary academic hospitals. Emerg. Radiol. 2020, 27, 791–797. [Google Scholar] [CrossRef]
- Esteban, P.L.; Querolt Coll, J.; Xicola Martínez, M.; Camí Biayna, J.; Delgado-Flores, L. Has COVID-19 affected the number and severity of visits to a traumatology emergency department? Bone Jt. Open 2020, 1, 617–620. [Google Scholar] [CrossRef]
- Faried, A.; Hidajat, N.N.; Harsono, A.B.; Giwangkancana, G.W.; Hartantri, Y.; Imron, A.; Arifin, M.Z. Delayed definitive treatment of life-threatening neurosurgery patient with suspected coronavirus disease 2019 infection in the midst of pandemic: Report of two cases. Surg. Neurol. Int. 2021, 12, 18. [Google Scholar] [CrossRef]
- Servadei, F.; Cannizzaro, D. Effects on traumatic brain injured patients of COVID pandemia: Which responses from neurosurgical departments? Acta Neurochir. 2021, 163, 1051–1052. [Google Scholar] [CrossRef]
- Al Saiegh, F.; Mouchtouris, N.; Khanna, O.; Baldassari, M.; Theofanis, T.; Ghosh, R.; Tjoumakaris, S.; Gooch, M.R.; Herial, N.; Zarzour, H.; et al. Battle-tested guidelines and operational protocols for neurosurgical practice in times of a pandemic: Lessons learned from COVID-19. World Neurosurg. 2021, 146, 20–25. [Google Scholar] [CrossRef]
- Chen, P.; Xiong, X.H.; Chen, Y.; Wang, K.; Zhang, Q.T.; Zhou, W.; Deng, Y.B. Perioperative management strategy of severe traumatic brain injury during the outbreak of COVID-19. Chin. J. Traumatol. 2020, 23, 202–206. [Google Scholar] [CrossRef]
- Hernigou, J.; Morel, X.; Callewier, A.; Bath, O.; Hernigou, P. Staying home during “COVID-19” decreased fractures, but trauma did not quarantine in one hundred and twelve adults and twenty eight children and the “tsunami of recommendations” could not lockdown twelve elective operations. Int. Orthop. 2020, 44, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Megaloikonomos, P.D.; Thaler, M.; Igoumenou, V.G.; Bonanzinga, T.; Ostojic, M.; Couto, A.F.; Diallo, J.; Khosravi, I. Impact of the COVID-19 pandemic on orthopaedic and trauma surgery training in Europe. Int. Orthop. 2020, 44, 1611–1619. [Google Scholar] [CrossRef]
- Why Taiwan is Beating COVID-19—Again. Available online: https://thediplomat.com/2021/07/why-taiwan-is-beating-covid-19-again/ (accessed on 21 September 2021).
- Establishment and Application of Traffic Accident Injury Data Collection System (2/2). Available online: https://www.iot.gov.tw/cp-78-12430-1759c-1.html (accessed on 16 November 2020). (In Chinese)
- Ahmad, I.A.; Osei, E. Occupational health and safety measures in healthcare settings during COVID-19: Strategies for protecting staff, patients and visitors. Disaster Med. Public Health Prep. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- McCabe, R.; Schmit, N.; Christen, P.; D’Aeth, J.C.; Løchen, A.; Rizmie, D.; Nayagam, S.; Miraldo, M.; Aylin, P.; Bottle, A.; et al. Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC Med. 2020, 18, 329. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Pre-Pandemic Period Corresponding to P1 | P1 | p | Pre-Pandemic Period Corresponding to P2 | P2 | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
| Trauma population | ||||||||||
| TBI | 0.472 | 0.007 | ||||||||
| No | 8318 | 67.00 | 6523 | 66.55 | 6800 | 68.73 | 2925 | 66.43 | ||
| Yes | 4096 | 33.00 | 3279 | 33.45 | 3094 | 31.27 | 1478 | 33.57 | ||
| TBI population | ||||||||||
| Mild head injury | 0.083 | 0.001 | ||||||||
| No | 505 | 12.33 | 449 | 13.69 | 402 | 12.99 | 248 | 16.78 | ||
| Yes | 3591 | 87.67 | 2830 | 86.31 | 2692 | 87.01 | 1230 | 83.22 | ||
| Serious head injury | 0.089 | <0.0001 | ||||||||
| No | 3864 | 94.34 | 3062 | 93.38 | 2915 | 94.21 | 1311 | 88.70 | ||
| Yes | 232 | 5.66 | 217 | 6.62 | 179 | 5.79 | 167 | 11.30 | ||
| Variable | Pre-Pandemic Period Corresponding to P1 (n = 4092) | P1 (n = 3277) | p | Pre-Pandemic Period Corresponding to P2 (n = 3088) | P2 (n = 1474) | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
| Sex | 0.403 | 0.117 | ||||||||
| Female | 1808 | 44.18 | 1416 | 43.21 | 1417 | 45.89 | 640 | 43.42 | ||
| Male | 2284 | 55.82 | 1861 | 56.79 | 1671 | 54.11 | 834 | 56.58 | ||
| Age (years), median (IQR) | 42 | (19–66) | 44 | (22–68) | <0.001 | 42 | (19–66) | 54 | (29–73) | <0.0001 |
| Age (years) | 0.001 | <0.0001 | ||||||||
| 0–14 | 812 | 19.84 | 537 | 16.39 | 620 | 20.08 | 188 | 12.75 | ||
| 15–24 | 522 | 12.76 | 397 | 12.11 | 409 | 13.24 | 128 | 8.68 | ||
| 25–44 | 833 | 20.36 | 728 | 22.22 | 598 | 19.37 | 274 | 18.59 | ||
| 45–64 | 857 | 20.94 | 683 | 20.84 | 632 | 20.47 | 347 | 23.54 | ||
| 65+ | 1068 | 26.10 | 932 | 28.44 | 829 | 26.85 | 537 | 36.43 | ||
| Triage | <0.001 | <0.0001 | ||||||||
| Critical (Levels I and II) | 488 | 11.93 | 446 | 13.61 | 365 | 11.82 | 333 | 22.59 | ||
| Urgent (Level III) | 3479 | 85.02 | 2772 | 84.59 | 2619 | 84.81 | 1120 | 75.98 | ||
| Less urgent (Levels IV and V) | 125 | 3.05 | 59 | 1.80 | 104 | 3.37 | 21 | 1.42 | ||
| Variable | Pre-Pandemic Period Corresponding to P1 (n = 4092) | P1 (n = 3277) | p | Pre-Pandemic Period Corresponding to P2 (n = 3088) | P2 (n = 1474) | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
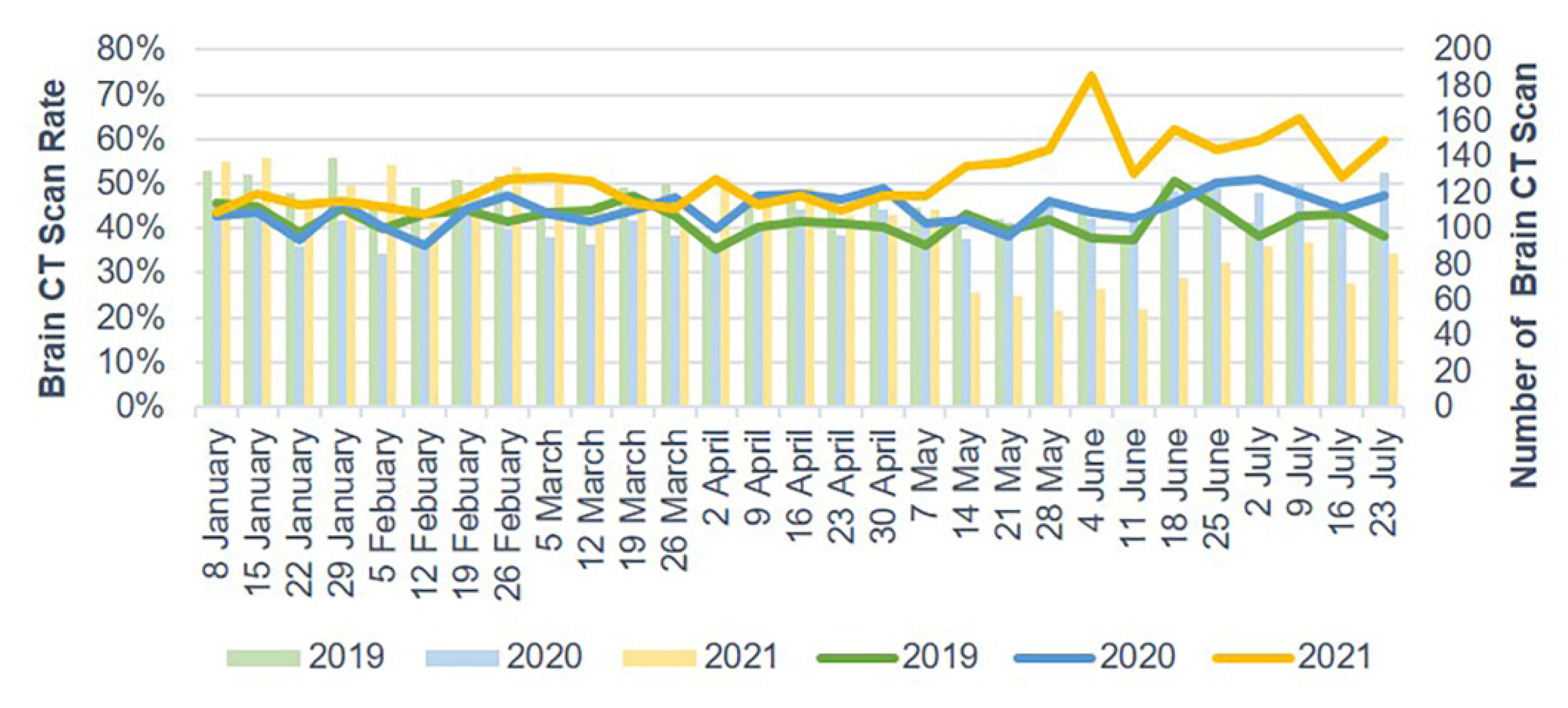
| Brain CT scan | 0.205 | <0.0001 | ||||||||
| No | 2379 | 58.14 | 1857 | 56.67 | 1803 | 58.39 | 619 | 41.99 | ||
| Yes | 1713 | 41.86 | 1420 | 43.33 | 1285 | 41.61 | 855 | 58.01 | ||
| Time from ED arrival to brain CT scan (minute), median (IQR) | 30 | (20–45) | 22 | (14–35) | <0.0001 | 27 | (18–42) | 21 | (13–34) | <0.0001 |
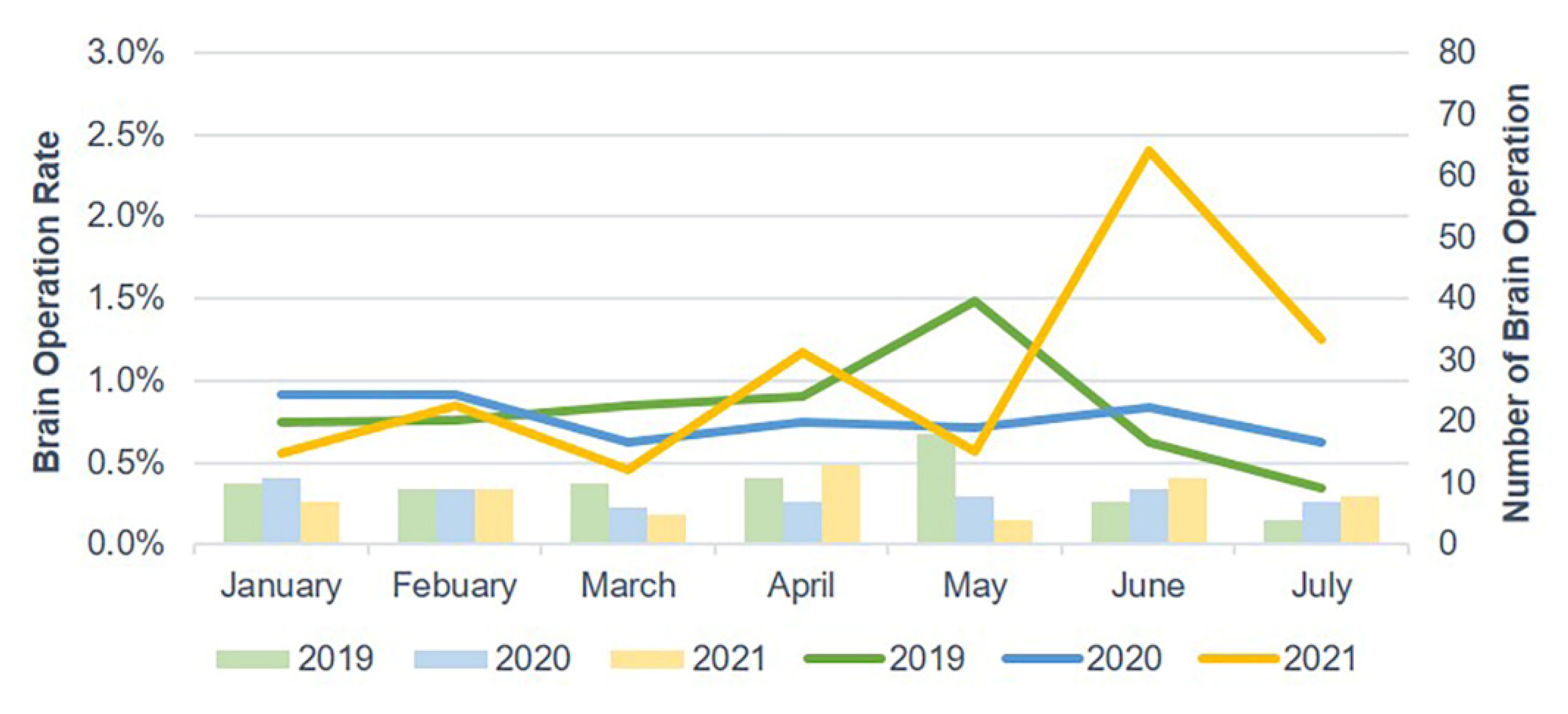
| Brain operation | 0.459 | 0.020 | ||||||||
| No | 4057 | 99.14 | 3254 | 99.30 | 3066 | 99.29 | 1453 | 98.58 | ||
| Yes | 35 | 0.86 | 23 | 0.70 | 22 | 0.71 | 21 | 1.42 | ||
| Time from ED arrival to brain operation (hour), median (IQR) | 6 | (3–15) | 4 | (2–6) | 0.174 | 5 | (3–8) | 5 | (3–7) | 0.788 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, C.; Yen, J.-C.; Wu, C.-C.; Lin, H.-Y.; Hsu, M.-H. Effects of the COVID-19 Pandemic on Treatment Efficiency for Traumatic Brain Injury in the Emergency Department: A Multicenter Study in Taiwan. J. Clin. Med. 2021, 10, 5314. https://doi.org/10.3390/jcm10225314
Lam C, Yen J-C, Wu C-C, Lin H-Y, Hsu M-H. Effects of the COVID-19 Pandemic on Treatment Efficiency for Traumatic Brain Injury in the Emergency Department: A Multicenter Study in Taiwan. Journal of Clinical Medicine. 2021; 10(22):5314. https://doi.org/10.3390/jcm10225314
Chicago/Turabian StyleLam, Carlos, Ju-Chuan Yen, Chia-Chieh Wu, Heng-Yu Lin, and Min-Huei Hsu. 2021. "Effects of the COVID-19 Pandemic on Treatment Efficiency for Traumatic Brain Injury in the Emergency Department: A Multicenter Study in Taiwan" Journal of Clinical Medicine 10, no. 22: 5314. https://doi.org/10.3390/jcm10225314