
Knowledge, Attitudes and Perceptions towards COVID-19 Vaccinations: A Cross-Sectional Survey in Pakistan
 ,
,  ,
,  and
and 
Abstract
:1. Background
2. Methodology
2.1. Study Design
2.2. Study Setting
2.3. Study Duration
2.4. Inclusion and Exclusion Criteria
2.5. Sample Size and Sampling Technique
2.6. Study Tool
2.7. Questionnaires Development and Validation
2.8. Scoring Criteria and Statistical Analysis
2.9. Ethical Approval
3. Results
3.1. Demographics of Knowledge, Attitude and Perception Study
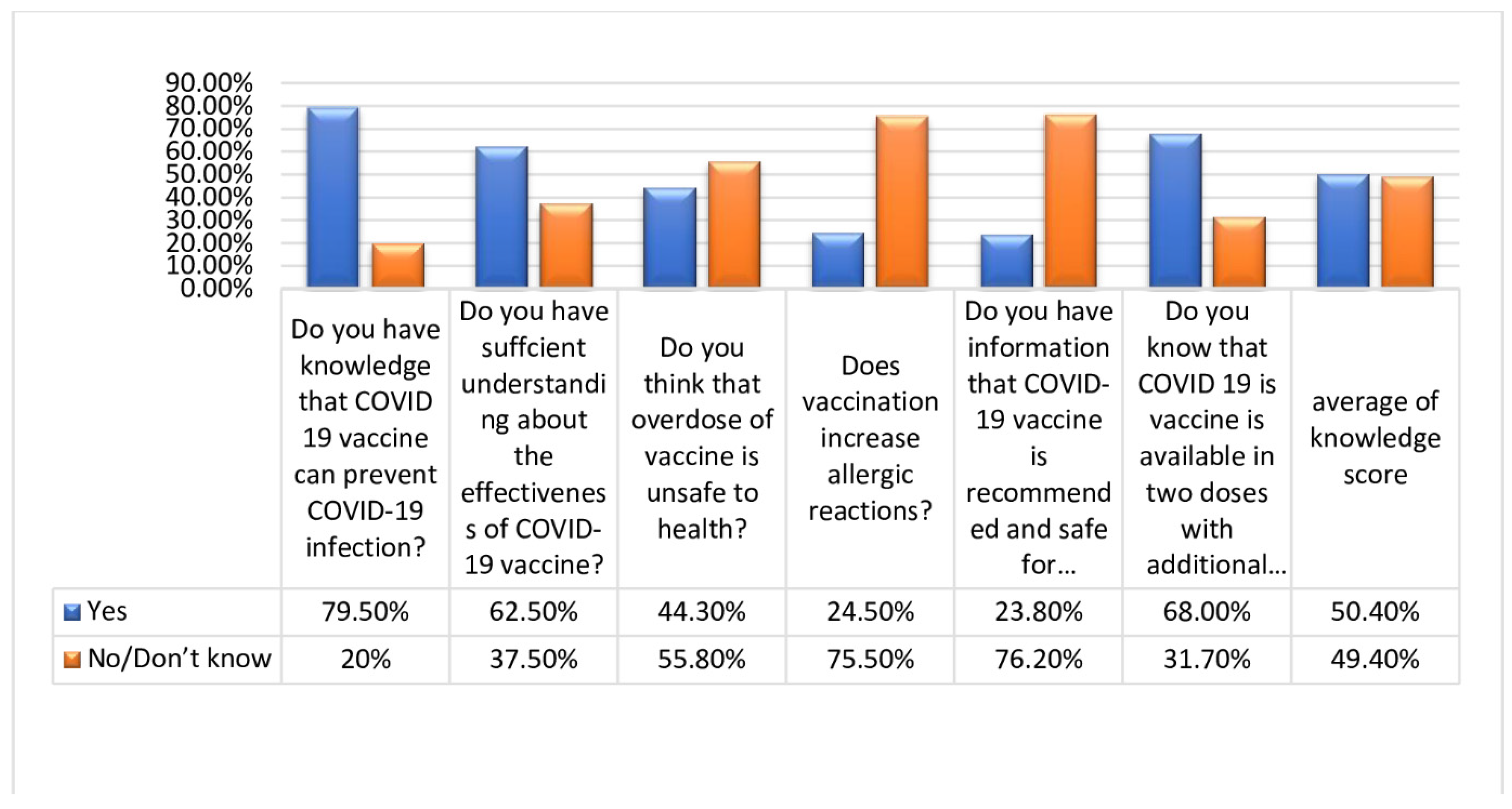
3.2. Frequency of Response to Knowledge
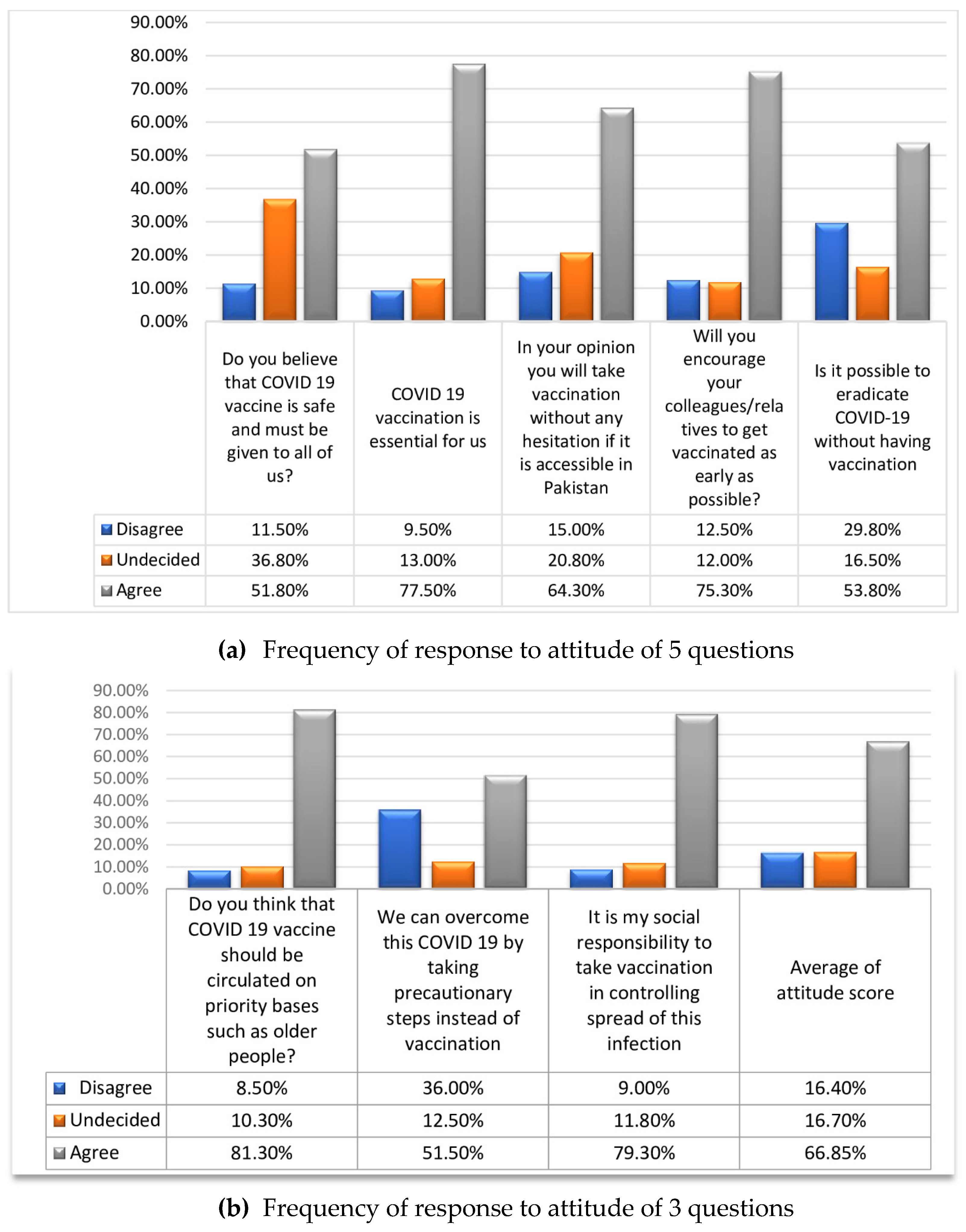
3.3. Frequency of Response to Attitude
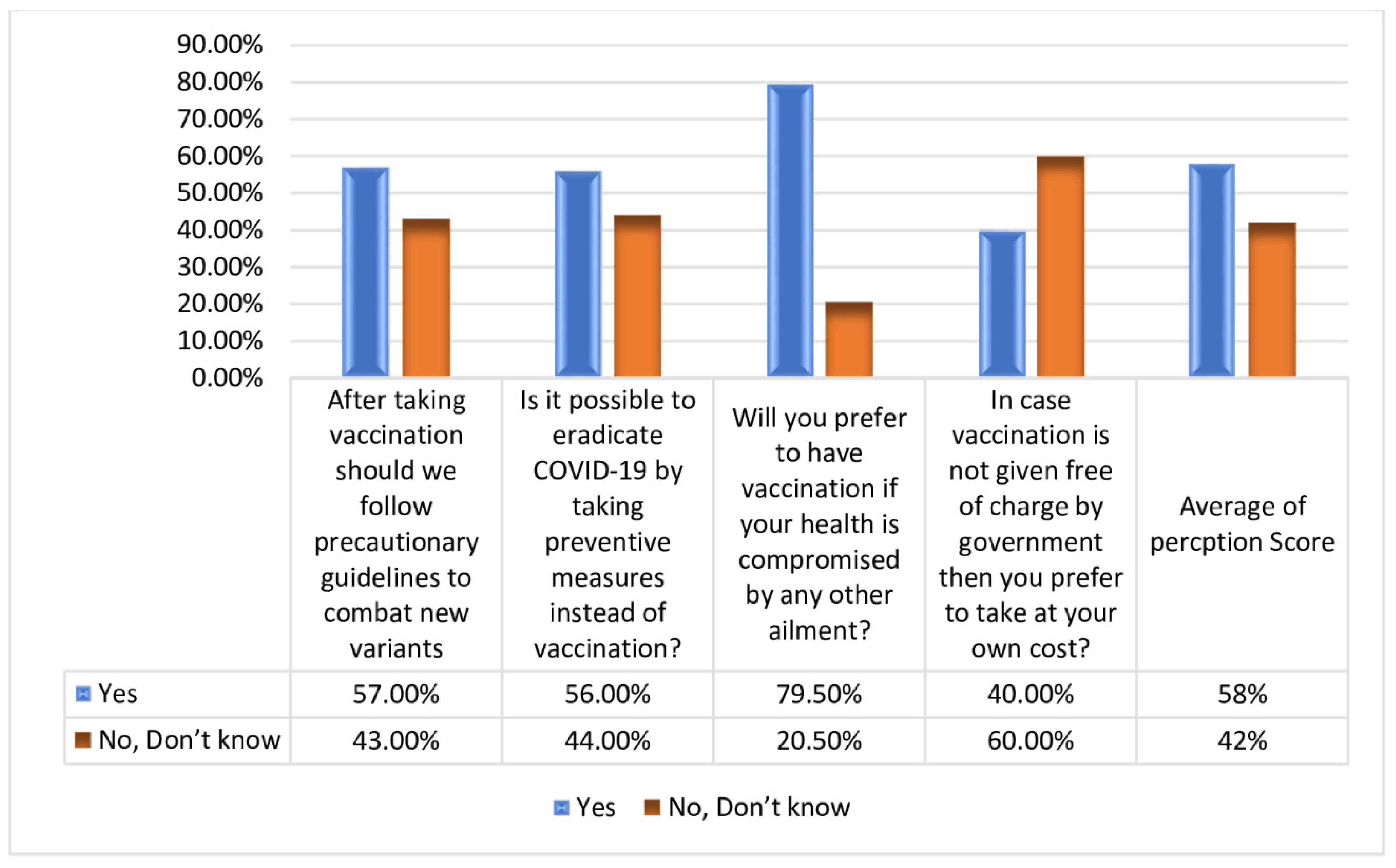
3.4. Frequency of Response to Perception
3.5. Categorization of Participant’s Score and Their Association with Demographics
3.6. Analysis of Mean Knowledge, Attitude and Perception
3.7. Factors Affecting Knowledge, Attitude and Perception Response on the Use of Vaccine
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lim, Y.; Ng, Y.; Tam, J.; Liu, D. Human Coronaviruses: A Review of Virus–Host Interactions. Diseases 2016, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abid, K.; Bari, Y.A.; Younas, M.; Tahir Javaid, S.; Imran, A. Progress of COVID-19 Epidemic in Pakistan. Asia-Pac. J. Public Health 2020, 32, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Chin, B.S.; Kang, C.K.; Kim, N.J.; Kang, Y.M.; Choi, J.P.; Oh, D.H.; Kim, J.-H.; Koh, B.; Kim, S.E.; et al. Clinical course and outcomes of patients with severe acute respiratory syndrome coronavirus 2 infection: A preliminary report of the first 28 patients from the korean cohort study on COVID-19. J. Korean Med. Sci. 2020, 35, e142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, S.; Jiang, F.; Su, W.; Chen, C.; Chen, J.; Mei, W.; Zhan, L.-Y.; Jia, Y.; Zhang, L.; Liu, D.; et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 2020, 21, 100331. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Tong, Z.; Guan, X.; Du, B.; Qiu, H. Clinical Characteristics of Patients Who Died of Coronavirus Disease 2019 in China. JAMA Netw Open 2020, 3, e205619. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, R.T.; Lynch, J.B.; del Rio, C. Mild or Moderate Covid-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.-F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef]
- Helmy, Y.A.; Fawzy, M.; Elaswad, A.; Sobieh, A.; Kenney, S.P.; Shehata, A.A. The COVID-19 pandemic: A comprehensive review of taxonomy, genetics, epidemiology, diagnosis, treatment, and control. J. Clin. Med. 2020, 9, 1225. [Google Scholar] [CrossRef]
- Tang, D.; Tou, J.; Wang, J.; Chen, Q.; Wang, W.; Huang, J.; Zhao, H.; Wei, J.; Xu, Z.; Zhao, D.; et al. Prevention and control strategies for emergency, limited-term, and elective operations in pediatric surgery during the epidemic period of COVID-19. World J. Pediatr. Surg. 2020, 3, e000122. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person to person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef]
- Chirwa, G.C. “Who knows more, and why?” Explaining socioeconomic-related inequality in knowledge about HIV in Malawi. Sci. Afr. 2020, 7, e00213. [Google Scholar] [CrossRef]
- UNICEF. Another 1.2 Million Doses of COVID-19 Vaccine Reach Pakistan through COVAX. 2021. Available online: https://www.unicef.org/pakistan/press-releases/another-12-million-doses-covid-19-vaccine-reach-pakistan-through-covax (accessed on 29 July 2021).
- Farooq, U.; Pakistan to Receive 13 Million Doses of Pfizer Vaccine—Minister. Reuters. Sec. Asia Pacific. 2021. Available online: https://www.reuters.com/world/asia-pacific/pakistan-receive-13-mln-doses-pfizer-vaccine-minister-2021-06-22/ (accessed on 31 July 2021).
- Hussain, S.; Pakistan Set to Procure 30 Million Doses of Coronavirus Vaccine. Yahoo! News. 2021. Available online: https://in.news.yahoo.com/pakistan-set-procure-30-million-120755420.html (accessed on 31 July 2021).
- Widakuswara, P. US Ships Moderna Vaccine to Pakistan Amid Delta Variant Surge | Voice of America—English. Voice of America. 2021. Available online: https://www.voanews.com/covid-19-pandemic/us-ships-moderna-vaccine-pakistan-amid-delta-variant-surge (accessed on 31 July 2021).
- Shahzad, A.; Pakistan Commits $1.1 Bln for COVID Vaccine to Cover Eligible Population. Reuters. Sec. Asia Pacific. 2021. Available online: https://www.reuters.com/world/asia-pacific/pakistan-administers-10-mln-covid-vaccine-doses-eyes-70-mln-target-2021-06-09/ (accessed on 31 July 2021).
- Government of Pakistan. Covid-19 Situation. 2021. Available online: https://covid.gov.pk/ (accessed on 31 July 2021).
- Gavi the Vaccine Alliance. Pakistan Progressing on Immunization Efforts. 2016. Available online: https://www.gavi.org/news/media-room/pakistan-progressing-immunisation-efforts (accessed on 31 July 2021).
- Khan, M.S.; Improving the Covid-19 Vaccination Rate in Pakistan—A Multipronged Policy Approach. Front. Public Health 2021. Available online: https://www.frontiersin.org/article/10.3389/fpubh.2021.729102 (accessed on 29 July 2021).
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, S.; Gokce, A.; Boz, G.; Saritas, H.; Unsal, S.; Ozer, A.; Akbulut, M.S.; Colak, C. Evaluation of Vaccine Hesitancy and Anxiety Levels among Hospital Cleaning Staff and Caregivers during COVID-19 Pandemic. Vaccines 2022, 10, 1426. [Google Scholar] [CrossRef] [PubMed]
- İkiışık, H.; Akif Sezerol, M.; Taşçı, Y.; Maral, I. COVID-19 vaccine hesitancy: A community-based research in Turkey. Int. J. Clin. Pract. 2021, 75, e14336. [Google Scholar] [CrossRef] [PubMed]
- Khamis, F.; Badahdah, A.; Al Mahyijari, N.; Al Lawati, F.; Al Noamani, J.; Al Salmi, I.; Al Bahrani, M. Attitudes Towards COVID-19 Vaccine: A Survey of Health Care Workers in Oman. J. Epidemiol. Glob. Health 2022, 12, 1–6. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.A.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Yakut, S.; Karagülle, B.; Atçalı, T.; Öztürk, Y.; Açık, M.N.; Çetinkaya, B. Knowledge, attitudes, practices and some characteristic features of people recovered from COVID-19 in Turkey. Medicina 2021, 57, 431. [Google Scholar] [CrossRef]
- Al-Marshoudi, S.; Al-Balushi, H.; Al-Wahaibi, A.; Al-Khalili, S.; Al-Maani, A.; Al-Farsi, N.; Al-Jahwari, A.; Al-Habsi, Z.; Al-Shaibi, M.; Al-Msharfi, M.; et al. Knowledge, attitudes, and practices (Kap) toward the covid-19 vaccine in oman: A pre-campaign cross-sectional study. Vaccines 2021, 9, 602. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Akhu-Zaheya, L.M.; Jagbir, M.T.; Othman, A.; Ahram, M. Media use for seeking health/cancer-related information: Findings from knowledge, attitudes and practices towards cancer prevention and care survey in Jordan. Int. J. Nurs. Pract. 2014, 20, 608–615. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; et al. Acceptance of covid-19 vaccination in the elderly: A cross-sectional study in Southern Italy. Vaccines 2021, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Smith, J.; Appleton, M. Risk perception, risk management and safety assessment: What can governments do to increase public confidence in their vaccine system? Biologicals 2012, 40, 384–388. [Google Scholar] [CrossRef]
- Papagiannis, D.; Malli, F.; Raptis, D.G.; Papathanasiou, I.V. Assessment of knowledge, attitudes, and practices towards new coronavirus (SARS-CoV-2) of health care professionals in Greece before the outbreak period. Int. J. Environ. Res. Public Health 2020, 17, 4925. [Google Scholar] [CrossRef]
- Harkness, J.A.; Schoua-Glusberg, A. Questionnaires in Translation. ZUMA-Nachr. Spez. 1998, 3, 87–126. Available online: http://isites.harvard.edu/fs/docs/icb.topic506406.files/znspez3_04_Harkness_Glusberg.pdf (accessed on 22 July 2021).
- A Guide To Developing Knowledge, Attitude and Practice Surveys; WHO: Geneva, Switzerland, 2008.
- Akalu, Y.; Ayelign, B.; Molla, M.D. Knowledge, attitude and practice towards covid-19 among chronic disease patients at addis zemen hospital, Northwest Ethiopia. Infect. Drug Resist. 2020, 13, 1949–1960. [Google Scholar] [CrossRef]
- Policy, H. The Knowledge and Attitude of the Community from the Aseer Region, Saudi Arabia, Toward COVID-19 and Their Precautionary Measures Against the Disease. Risk Manag. Healthc. Policy 2020, 13, 1825. [Google Scholar]
- Goyal, L.; Zapata, M.; Ajmera, K.; Chaurasia, P.; Pandit, R.; Pandit, T. A Hitchhiker’s Guide to Worldwide COVID-19 Vaccinations: A Detailed Review of Monovalent and Bivalent Vaccine Schedules, COVID-19 Vaccine Side Effects, and Effectiveness Against Omicron and Delta Variants. Cureus 2022, 14, e29837. Available online: http://www.ncbi.nlm.nih.gov/pubmed/36204257%0Ahttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC9527088 (accessed on 31 July 2021). [CrossRef]
- Saiful Islam, M.; Siddique, A.B.; Akter, R.; Tasnim, R.; Safaet, M.; Sujan, H.; Ward, P.R.; Sikder, M.T. Knowledge, attitudes and perceptions towards COVID-19 vaccinations: A cross-sectional community survey in Bangladesh. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Fu, C.; Wei, Z.; Pei, S.; Li, S.; Sun, X.; Liu, P. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs). medRxiv 2020, 548, 2962. [Google Scholar]
- Larson, H.J.; Smith, D.M.D.; Paterson, P.; Cumming, M.; Eckersberger, E.; Freifeld, C.C.; Ghinai, I.; Jarrett, C.; Paushter, L.; Brownstein, J.S.; et al. Measuring vaccine confidence: Analysis of data obtained by a media surveillance system used to analyse public concerns about vaccines. Lancet Infect. Dis. 2013, 13, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Anwar, S.; Bustaman, A.; Radiansyah, A.; Angraini, P.; Fasli, R.; Salwiyadi, S.; Bastian, R.A.; Oktiviyari, A.; Akmal, I.; et al. Modifiable determinants of attitude towards dengue vaccination among healthy inhabitants of Aceh, Indonesia: Findings from a community-based survey. Asian Pac. J. Trop. Med. 2016, 9, 1115–1122. Available online: https://www.sciencedirect.com/science/article/pii/S1995764516303686 (accessed on 29 July 2021). [CrossRef] [PubMed]
- Ferdous, M.Z.; Islam, M.S.; Sikder, M.T.; Mosaddek, A.S.M.; Zegarra-Valdivia, J.A.; Gozal, D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: An online-based cross-sectional study. PLoS ONE 2020, 15, e0239254. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Mannan, K.A.; Farhana, K.M. Knowledge, Attitude and Acceptance of a COVID-19 Vaccine: A Global Cross-Sectional Study. SSRN Electron. J. 2021, 6, 1–23. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Lombardi, A.; Bozzi, G.; Ungaro, R.; Villa, S.; Castelli, V.; Mangioni, D.; Muscatello, A.; Gori, A.; Bandera, A. Mini Review Immunological Consequences of Immunization With COVID-19 mRNA Vaccines: Preliminary Results. Front. Immunol. 2021, 12, 1–11. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Al-Zalfawi, S.M.; Rabbani, S.I.; Asdaq, S.M.B.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.A.; AlRifdah, A.H.; Almagrabe, T. Public knowledge, attitude, and perception towards COVID-19 vaccination in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 10081. [Google Scholar] [CrossRef]
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel—Implications for vaccination implementation policies. Isr. J. Health Policy Res. 2021, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jabal, K.A.; Ben-Amram, H.; Beiruti, K.; Batheesh, Y.; Sussan, C.; Zarka, S.; Edelstein, M. Impact of age, ethnicity, sex and prior infection status on immunogenicity following a single dose of the BNT162b2 MRNA COVID-19 vaccine: Real-world evidence from healthcare workers, Israel, December 2020 to January 2021. Eurosurveillance 2021, 26, 2100096. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographics | Frequency (n) | Percentages (%) | |
|---|---|---|---|
| Age | <20 | 39 | 9.7 |
| 21–40 | 218 | 54.5 | |
| 41–60 | 109 | 27.2 | |
| >61 | 34 | 8.5 | |
| Gender | Female | 186 | 46.5 |
| Male | 214 | 53.5 | |
| Marital status | Unmarried | 180 | 45 |
| Married | 220 | 55.0 | |
| Education level | High school or below | 172 | 43.2 |
| Graduate | 121 | 30.3 | |
| Postgraduate | 107 | 26.7 | |
| Employment status | Gov. employee | 81 | 20.3 |
| Non Gov. employee | 75 | 18.9 | |
| Self employed | 32 | 8.0 | |
| Student | 109 | 27.3 | |
| Retired | 36 | 9.0 | |
| Unemployed | 67 | 16.9 | |
| Residence | Urban | 281 | 70.2 |
| Rural | 119 | 29.8 | |
| Knowledge | Attitude | Perception | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Good | Fair | Poor | p Value | Good | Fair | Poor | p Value | Good | Fair | Poor | p Value | |
| Age | <20 | 4 | 25 | 7 | 0.347 | 20 | 13 | 3 | 0.001 | 8 | 10 | 18 | 0.064 |
| 21–40 | 43 | 142 | 29 | 132 | 54 | 28 | 39 | 112 | 63 | ||||
| 41–60 | 26 | 64 | 15 | 35 | 44 | 26 | 22 | 54 | 29 | ||||
| Gender | >61 | 10 | 15 | 5 | 10 | 10 | 10 | 8 | 16 | 5 | |||
| Female | 32 | 129 | 25 | 103 | 56 | 27 | 0.148 | 31 | 96 | 59 | 0.077 | ||
| Male | 51 | 129 | 30 | 96 | 74 | 40 | 54 | 100 | 55 | ||||
| Marital status | Unmarried | 40 | 115 | 24 | 0.831 | 105 | 49 | 24 | 0.005 | 37 | 80 | 62 | 0.088 |
| Married | 44 | 144 | 32 | 94 | 82 | 44 | 49 | 116 | 54 | ||||
| Education level | high school or below | 38 | 100 | 34 | 0.043 | 66 | 72 | 33 | 0.001 | 39 | 82 | 50 | 0.577 |
| graduate | 27 | 83 | 11 | 67 | 34 | 20 | 28 | 63 | 30 | ||||
| postgraduate | 19 | 75 | 11 | 66 | 24 | 15 | 19 | 50 | 36 | ||||
| Employment status | Gov. employee | 9 | 62 | 10 | 0.030 | 38 | 32 | 11 | 0.019 | 21 | 40 | 20 | 0.615 |
| non Gov. employee | 13 | 53 | 9 | 42 | 22 | 11 | 13 | 39 | 23 | ||||
| self employed | 9 | 17 | 4 | 7 | 15 | 8 | 10 | 13 | 7 | ||||
| Student | 27 | 63 | 17 | 64 | 25 | 17 | 19 | 55 | 33 | ||||
| Retired | 14 | 15 | 7 | 12 | 14 | 10 | 10 | 17 | 8 | ||||
| Unemployed | 12 | 47 | 8 | 34 | 22 | 11 | 13 | 30 | 24 | ||||
| Residence | Urban | 48 | 187 | 44 | 0.015 | 149 | 85 | 44 | 0.051 | 58 | 141 | 80 | 0.755 |
| Rural | 35 | 69 | 13 | 47 | 46 | 24 | 27 | 54 | 35 | ||||
| Mean Knowledge | Mean Attitude | Mean Perception | ||||
|---|---|---|---|---|---|---|
| Variables | Mean (S.D) | p Value | Mean (S.D) | p Value | Mean (S.D) | p Value |
| Age | 0.5602 (0.165) 0.5964 (0.19568) 0.3759 (0.26572) 0.1944 (0.19615) | 0.009 | 1.5556 (0.28730) 1.5736 (0.37016) 1.4029 (0.34624) 1.3375 (0.39000) | 0.001 | 0.6111 (0.24960) 0.6752 (0.21860) 0.4762 (0.29114) 0.3750 (0.29906) | 0.001 |
| <20 21–40 41–60 >61 | ||||||
| Gender | 0.5658 (0.20926) 0.4525 (0.26746) | 0.001 | 1.5390 (0.36552) 1.4705 (0.37266) | 0.066 | 0.6452 (0.23052) 0.5226 (0.30705) | 0.017 |
| Female Male | ||||||
| Marital Status | 0.6134 (0.19448) 0.4188 (0.25468) | 0.012 | 1.5475(0.37851) 1.4662(0.36106) | 0.029 | 0.6508 (0.23912) 0.5239 (0.29792) | 0.002 |
| Unmarried Married | ||||||
| Education Level | 0.3777 (0.25744) 0.6074 (0.19467) 0.5997 (0.19107) | 0.001 | 1.4523 (0.33256) 1.5289 (0.38587) 1.5560 (0.40541) | 0.051 | 0.4753 (0.29452) 0.6426(0.26581) 0.6810 (0.20655) | 0.001 |
| High school or below Graduate Postgraduate | ||||||
| Employment Status | 0.5251 (0.20190) 0.5431 (0.23216) 0.2889 (0.25496) 0.6184(0.19018) 0.2269 (0.23622) 0.5075 (0.24521) | 0.001 | 1.5231 (0.29981) 1.5724 (0.33364) 1.2750 (0.40921) 1.5339 (0.39624) 1.3819 (0.31756) 1.5037 (0.41342) | 0.002 | 0.5494 (0.30726) 0.5967 (0.25959) 0.5250 (0.33701) 0.6752 (0.21504) 0.3750 (0.29580) 0.5821 (0.26610) | 0.001 |
| Gov. employee Non Gov. employee Self employed Student Retired Unemployed | ||||||
| Residence | 0.5446 (0.21737) 0.4074 (0.29152) | 0.019 | 1.5302 (0.35036) 1.4306 (0.41015) | 0.015 | 0.6246 (0.26132) 0.4722 (0.29503) | 0.026 |
| Urban Rural | ||||||
| Independent Variable | Knowledge | Attitude | Perception | ||||||
|---|---|---|---|---|---|---|---|---|---|
| R Square | 0.316 | R Square | 0.063 | R Square | 0.224 | ||||
| Adjusted R Square | 0.293 | Adjusted R Square | 0.031 | Adjusted R Square | 0.198 | ||||
| Durbin Watson | 1.657 | Durbin Watson | 1.938 | Durbin Watson | 1.718 | ||||
| B | SE | p-Value | B | SE | p-Value | B | SE | p-Value | |
| (Constant) | 0.622 | 0.057 | 0.000 | 1.641 | 0.090 | 0.000 | 0.678 | 0.066 | 0.000 |
| Age | −0.070 | 0.028 | 0.013 | −0.073 | 0.045 | 0.106 | −0.069 | 0.033 | 0.036 |
| Gender | 0.007 | 0.040 | 0.869 | 0.024 | 0.063 | 0.704 | −0.033 | 0.046 | 0.471 |
| Marital status | 0.076 | 0.047 | 0.110 | −0.053 | 0.076 | 0.483 | 0.054 | 0.055 | 0.329 |
| Education level | 0.077 | 0.025 | 0.002 | 0.013 | 0.040 | 0.751 | 0.076 | 0.029 | 0.009 |
| Employment status | −0.028 | 0.010 | 0.006 | −0.015 | 0.016 | 0.349 | −0.021 | 0.012 | 0.067 |
| Residence | −0.075 | 0.034 | 0.030 | −0.034 | 0.055 | 0.533 | −0.140 | 0.040 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bibi, A.; Abbas, S.; Mushtaq, S.; Mansoor, A.; Green, I.R.; Mallhi, T.H.; Khan, Y.H.; Khan, A. Knowledge, Attitudes and Perceptions towards COVID-19 Vaccinations: A Cross-Sectional Survey in Pakistan. Medicina 2023, 59, 272. https://doi.org/10.3390/medicina59020272
Bibi A, Abbas S, Mushtaq S, Mansoor A, Green IR, Mallhi TH, Khan YH, Khan A. Knowledge, Attitudes and Perceptions towards COVID-19 Vaccinations: A Cross-Sectional Survey in Pakistan. Medicina. 2023; 59(2):272. https://doi.org/10.3390/medicina59020272
Chicago/Turabian StyleBibi, Asima, Sameen Abbas, Saima Mushtaq, Atika Mansoor, Ivan R. Green, Tauqeer Hussain Mallhi, Yusra Habib Khan, and Amjad Khan. 2023. "Knowledge, Attitudes and Perceptions towards COVID-19 Vaccinations: A Cross-Sectional Survey in Pakistan" Medicina 59, no. 2: 272. https://doi.org/10.3390/medicina59020272