
A Non-Linear Biostatistical Graphical Modeling of Preventive Actions and Healthcare Factors in Controlling COVID-19 Pandemic

 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Variable
2.2. Methods
3. Results
3.1. COVID-19 and National Preventive Action
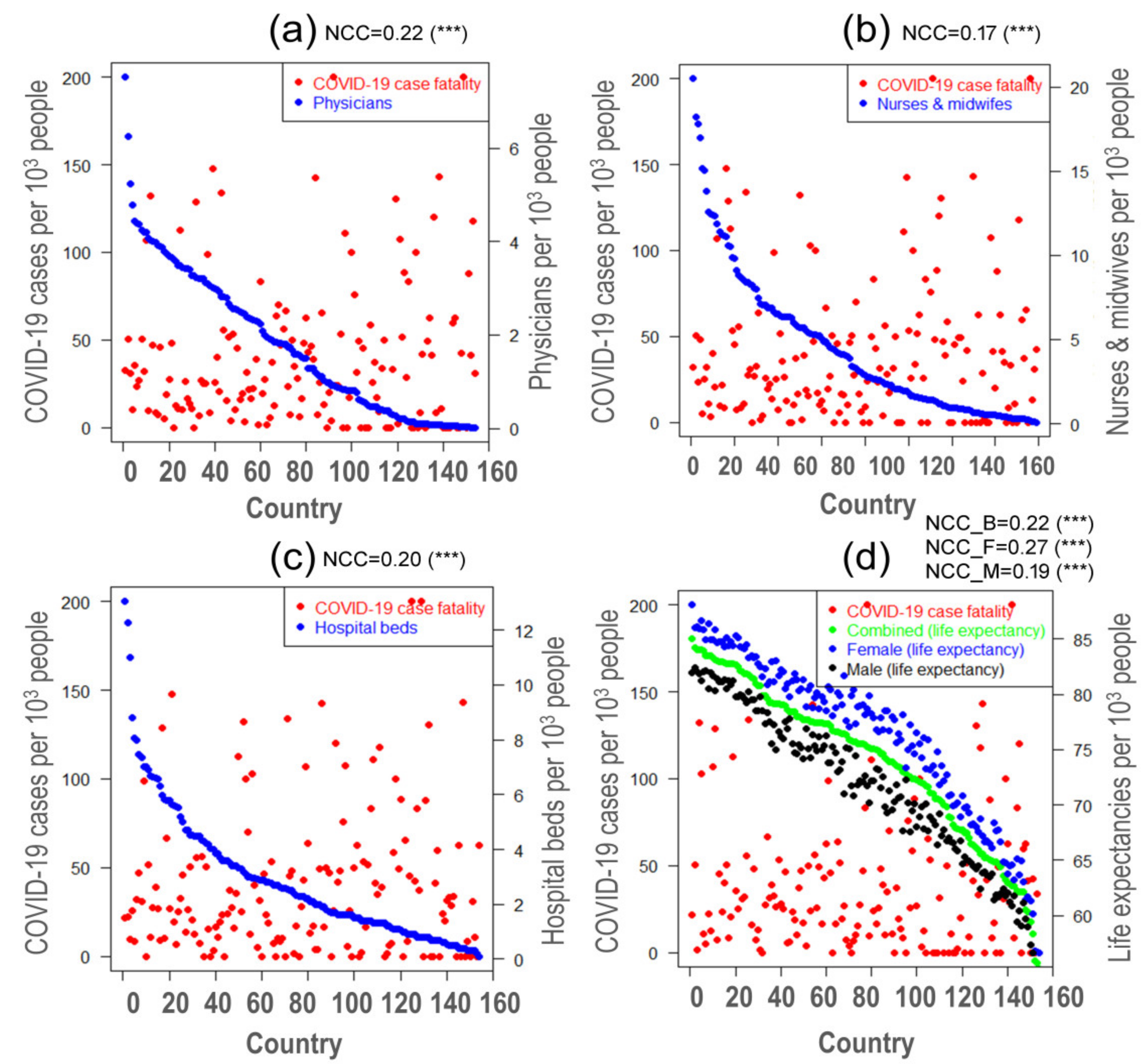
3.2. Healthcare Resources in COVID-19
3.3. Life Expectancy and COVID-19 Case Fatality
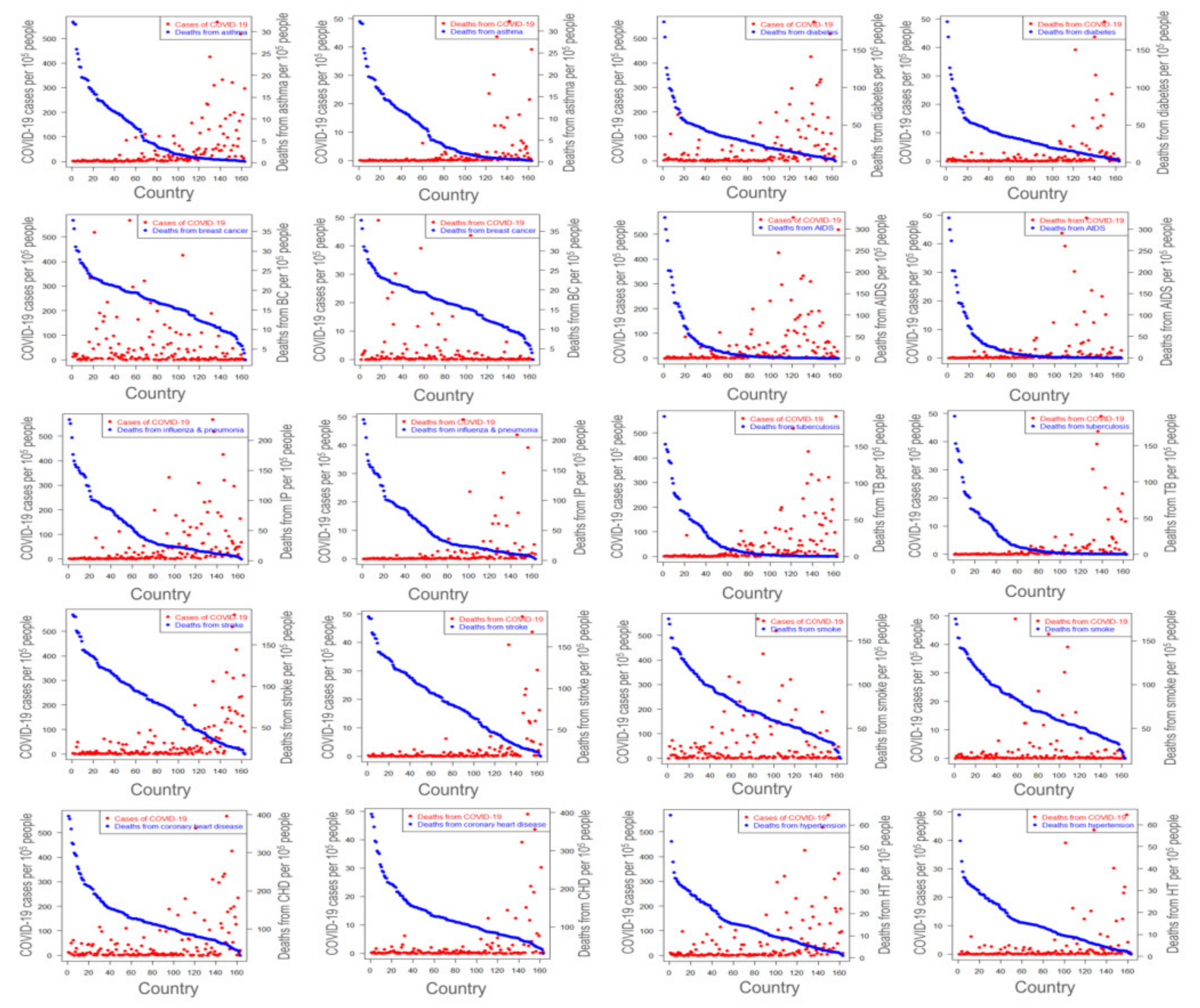
3.4. Association between COVID-19 and Comorbidities
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; De Clercq, E. Therapeutic options for the 2019 novel coronavirus (2019-nCoV). Nat. Rev. Drug Discov. 2020, 19, 149–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, Y.S.; Sircar, S.; Bhat, S.; Sharun, K.; Dhama, K.; Dadar, M.; Tiwari, R.; Chaicumpa, W. Emerging novel coronavirus (2019-nCoV)-current scenario, evolutionary perspective based on genome analysis and recent developments. Vet. Q. 2020, 40, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Hasanul, M.; Siam, B.; Md, S.; Abedin, M.; Ahmed, A.; Nishat, N.H.; Hossain, M.S.; Rahman, M.M. Pathophysiological mechanisms of disease severity in COVID-19: An update. J. Adv. Biotechnol. Exp. Ther. 2020, 3, 68–77. [Google Scholar] [CrossRef]
- Yu, H.; Sun, T.; Feng, J. Complications and Pathophysiology of COVID-19 in the Nervous System. Front. Neurol. 2020, 11, 573421. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.K.; Hall, A.; Sepiashvili, L.; Jung, B.; Steele, S.; Adeli, K. Pathophysiology of COVID-19: Mechanisms underlying disease severity and progression. Physiology 2020, 35, 288–301. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Syal, K. COVID-19: Herd Immunity and Convalescent Plasma Transfer Therapy. J. Med. Virol. 2020, 92, 1380–1382. [Google Scholar] [CrossRef] [Green Version]
- Worldometer COVID Live Update. Available online: https://www.worldometers.info/coronavirus/ (accessed on 20 April 2020).
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.d.; Sall, A.A.; et al. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Xu, X.; Yu, C.; Qu, J.; Zhang, L.; Jiang, S.; Huang, D.; Chen, B.; Zhang, Z.; Guan, W.; Ling, Z.; et al. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1275–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Zhang, L. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, e181. [Google Scholar] [CrossRef]
- Shen, K.; Yang, Y.; Wang, T.; Zhao, D.; Jiang, Y.; Jin, R.; Zheng, Y.; Xu, B.; Xie, Z.; Lin, L.; et al. Diagnosis, treatment, and prevention of 2019 novel coronavirus infection in children: Experts’ consensus statement. World J. Pediatr. 2020, 16, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Heymann, D.L.; Shindo, N. COVID-19: What is next for public health? Lancet 2020, 395, 542–545. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Amanat, F.; Krammer, F. SARS-CoV-2 Vaccines: Status Report. Immunity 2020, 52, 583–589. [Google Scholar] [CrossRef]
- Dai, W.; Zhang, B.; Su, H.; Li, J.; Zhao, Y.; Xie, X.; Jin, Z.; Liu, F.; Li, C.; Li, Y.; et al. Structure-based design of antiviral drug candidates targeting the SARS-CoV-2 main protease. Science 2020, 368, 1331–1335. [Google Scholar] [CrossRef] [Green Version]
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation and Treatment Coronavirus (COVID-19). In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2020. [Google Scholar]
- Li, H.; Zhou, Y.; Zhang, M.; Wang, H.; Zhao, Q.; Liu, J. Updated approaches against SARS-CoV-2. Antimicrob. Agents Chemother. 2020, 64, 483–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinceti, M.; Filippini, T.; Rothman, K.J.; Ferrari, F.; Goffi, A.; Maffeis, G.; Orsini, N. Lockdown timing and efficacy in controlling COVID-19 using mobile phone tracking. EClinicalMedicine 2020, 25, 100457. [Google Scholar] [CrossRef]
- Alwashmi, M.F. The use of digital health in the detection and management of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 2906. [Google Scholar] [CrossRef]
- Yasir, A.; Hu, X.; Ahmad, M.; Rauf, A.; Shi, J.; Nasir, S.A. Modeling impact of word of mouth and E-government on online social presence during COVID-19 outbreak: A multi-mediation approach. Int. J. Environ. Res. Public Health 2020, 17, 2954. [Google Scholar] [CrossRef]
- Dutta, A.; Fischer, H.W. The local governance of COVID-19: Disease prevention and social security in rural India. World Dev. 2021, 138, 105234. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.; Malik, M.; Raees, V.; Anwar, A. Role of Mass Media and Public Health Communications in the COVID-19 Pandemic. Cureus 2020, 12, e10453. [Google Scholar] [CrossRef]
- Liu, L.; Xie, J.; Li, K.; Ji, S. Exploring how media influence preventive behavior and excessive preventive intention during the COVID-19 pandemic in China. Int. J. Environ. Res. Public Health 2020, 17, 7990. [Google Scholar] [CrossRef] [PubMed]
- Heydari, S.T.; Zarei, L.; Sadati, A.K.; Moradi, N.; Akbari, M.; Mehralian, G.; Lankarani, K.B. The effect of risk communication on preventive and protective Behaviours during the COVID-19 outbreak: Mediating role of risk perception. BMC Public Health 2021, 21, 54. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Pizzol, D.; Marotta, C.; Antunes, M.; Racalbuto, V.; Veronese, N.; Smith, L. Coronavirus diseases (COVID-19) current status and future perspectives: A narrative review. Int. J. Environ. Res. Public Health 2020, 17, 2690. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.; Gozde, Y.; Fareed, Z.; Shahzad, F.; Ahmad, M. Impact of novel coronavirus (COVID-19) on daily routines and air environment: Evidence from Turkey. Air Qual. Atmos. Health 2021, 14, 381–387. [Google Scholar] [CrossRef]
- Mersha, A.; Shibiru, S.; Girma, M.; Ayele, G.; Bante, A.; Kassa, M.; Abebe, S.; Shewangizaw, M. Perceived barriers to the practice of preventive measures for COVID-19 pandemic among health professionals in public health facilities of the Gamo zone, southern Ethiopia: A phenomenological study. BMC Public Health 2021, 21, 199. [Google Scholar] [CrossRef]
- Khader, Y.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S.; AlShurman, B.A. Dentists’ awareness, perception, and attitude regarding COVID-19 and infection control: Cross-sectional study among Jordanian dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef]
- Irfan, M.; Ahmad, M.; Fareed, Z.; Iqbal, N.; Sharif, A.; Wu, H. On the indirect environmental outcomes of COVID-19: Short-term revival with futuristic long-term implications. Int. J. Environ. Health Res. 2021. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.A.; Sheikh, F.N.; Jamal, S.; Ezeh, J.K.; Akhtar, A. Coronavirus (COVID-19): A Review of Clinical Features, Diagnosis, and Treatment. Cureus 2020, 12, e7355. [Google Scholar] [CrossRef] [Green Version]
- Raoult, D.; Zumla, A.; Locatelli, F.; Ippolito, G.; Kroemer, G. Coronavirus infections: Epidemiological, clinical and immunological features and hypotheses. Cell Stress 2020, 4, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, N.; Peterman, A.; Potts, A.; O’Donnell, M.; Thompson, K.; Shah, N.; Oertelt-Prigione, S. Gender and COVID-19 working group COVID-19: Reducing the risk of infection might increase the risk of intimate partner violence. Lancet EClinicalMed. 2020, 21, 100348. [Google Scholar] [CrossRef]
- Horton, R. Offline: COVID-19-a reckoning. Lancet 2020, 395, 935. [Google Scholar] [CrossRef]
- Armitage, R.; Nellums, L.B. COVID-19 and the consequences of isolating the elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef] [Green Version]
- Gerst-Emerson, K.; Jayawardhana, J. Loneliness as a Public Health Issue: The Impact of Loneliness on Health Care Utilization Among Older Adults. Am. J. Public Health 2015, 105, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Santini, Z.I.; Jose, P.E.; York Cornwell, E.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef] [Green Version]
- Kwok, K.O.; Lai, F.; Wei, W.I.; Wong, S.Y.S.; Tang, J.W.T. Herd immunity—Estimating the level required to halt the COVID-19 epidemics in affected countries. J. Infect. 2020, S0163-4453, 30154–30157. [Google Scholar] [CrossRef]
- Tang, X.; Wu, C.; Li, X.; Song, Y.; Yao, X.; Wu, X.; Duan, Y.; Zhang, H.; Wang, Y.; Qian, Z.; et al. On the origin and continuing evolution of SARS-CoV-2. Natl. Sci. Rev. 2020, 7, 1012–1023. [Google Scholar] [CrossRef] [Green Version]
- Humanitarian Data Exchange Humanitarian Data Exchange. Available online: https://data.humdata.org/ (accessed on 20 April 2020).
- Our World in Data Our World in Data. Available online: https://ourworldindata.org/ (accessed on 20 April 2020).
- World Life Expectancy World Life Expectancy. Available online: https://www.worldlifeexpectancy.com/ (accessed on 20 April 2020).
- Ranjan, C. nlcor: Compute Nonlinear Correlations; ProcessMiner Inc.: Atlanta, GA, USA, 2020. [Google Scholar]
- Wang, Q.; Shen, Y.; Zhang, J.Q. A nonlinear correlation measure for multivariable data set. Phys. D Nonlinear Phenom. 2005, 200, 287–295. [Google Scholar] [CrossRef]
- Anderson, A. COVID-19 Outbreak Highlights Critical Gaps in School Emergency Preparedness; Brookings Institution: Washington, DC, USA, 2020. [Google Scholar]
- Cao, Y.; Li, Q.; Chen, J.; Guo, X.; Miao, C.; Yang, H.; Chen, Z.; Li, C.; Li, L. Hospital Emergency Management Plan During the COVID-19 Epidemic. Acad. Emerg. Med. 2020, 27, 309–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. CDC in Action: Preparing First Responders, Healthcare Providers, and Health Systems; CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- UNICEF; WHO; IFRC. Interim Guidance for COVID-19 Prevention and Control in Schools; IASC: New York, NY, USA, 2020. [Google Scholar]
- CDC. Interim Guidance for Businesses and Employers to Plan and Respond to Coronavirus Disease 2019 (COVID-19); CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- Kandel, N.; Chungong, S.; Omaar, A.; Xing, J. Health security capacities in the context of COVID-19 outbreak: An analysis of International Health Regulations annual report data from 182 countries. Lancet 2007, 395, 1047–1053. [Google Scholar] [CrossRef]
- Lau, L.S.; Samari, G.; Moresky, R.T.; Casey, S.E.; Kachur, S.P.; Roberts, L.F.; Zard, M. COVID-19 in humanitarian settings and lessons learned from past epidemics. Nat. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- The Social Science in Humanitarian Action Platform Key considerations: Quarantine in the Context of COVID-19 (February 2020) . 2020. Available online: https://www.socialscienceinaction.org/resources/february-2020-social-science-humanitarian-action-platform/ (accessed on 20 April 2020).
- Qualls, N.; Levitt, A.; Kanade, N.; Wright-Jegede, N.; Dopson, S.; Biggerstaff, M.; Reed, C.; Uzicanin, A. Community Mitigation Guidelines to Prevent Pandemic Influenza—United States, 2017. MMWR Recomm. Rep. 2017, 66, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Torok, M.E. Taking the right measures to control COVID-19. Lancet Infect. Dis. 2020, 20, 523–524. [Google Scholar] [CrossRef] [Green Version]
- Plümper, T.; Neumayer, E. Lockdown policies and the dynamics of the first wave of the Sars-CoV-2 pandemic in Europe. J. Eur. Public Policy 2020. [Google Scholar] [CrossRef]
- Ji, Y.; Ma, Z.; Peppelenbosch, M.P.; Pan, Q. Potential association between COVID-19 mortality and health-care resource availability. Lancet Glob. Health 2020, 8, e480. [Google Scholar] [CrossRef] [Green Version]
- Farahani, M.; Price, N.; El-Halabi, S.; Mlaudzi, N.; Keapoletswe, K.; Lebelonyane, R.; FetogangR, E.B.; Chebani, T.; Kebaabetswe, P.; Masupe, T.; et al. Impact of health system inputs on health outcome: A multilevel longitudinal analysis of Botswana national antiretroviral program (2002–2013). PLoS ONE 2016, 11, e0160206. [Google Scholar] [CrossRef] [PubMed]
- Drayi, F. The Impact Of Hospital Bed And Beddings On Patients: The Ghanaian Healthcare Consumer Perspectives. Int. J. Innov. Res. Adv. Stud. 2019, 6, 138–145. [Google Scholar]
- Kruk, M.E.; Gage, A.D.; Joseph, N.T.; Danaei, G.; García-Saisó, S.; Salomon, J.A. Mortality due to low-quality health systems in the universal health coverage era: A systematic analysis of amenable deaths in 137 countries. Lancet 2018, 392, 2203–2212. [Google Scholar] [CrossRef] [Green Version]
- Sadighi Akha, A.A. Aging and the immune system: An overview. J. Immunol. Methods 2018, 463, 21–26. [Google Scholar] [CrossRef]
- Franceschi, C.; Garagnani, P.; Morsiani, C.; Conte, M.; Santoro, A.; Grignolio, A.; Monti, D.; Capri, M.; Salvioli, S. The continuum of aging and age-related diseases: Common mechanisms but different rates. Front. Med. 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Niccoli, T.; Partridge, L. Ageing as a risk factor for disease. Curr. Biol. 2012, 22, R741–R752. [Google Scholar] [CrossRef] [Green Version]
- MacNee, W.; Rabinovich, R.A.; Choudhury, G. Ageing and the border between health and Disease. Eur. Respir. J. 2014, 44, 1332–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goronzy, J.J.; Weyand, C.M. Immune aging and autoimmunity. Cell. Mol. Life Sci. 2012, 69, 1615–1623. [Google Scholar] [CrossRef] [Green Version]
- WHO Bangladesh. COVID-19 Morbidity and Mortality Weekly Update (MMWU); WHO Bangladesh: Decca, Bangladesh, 2020; Volume 18. [Google Scholar]
- Glynn, J.R. Protecting workers aged 60–69 years from COVID-19. Lancet Infect. Dis. 2020, 3099, 30311. [Google Scholar] [CrossRef]
- Kurotani, K.; Akter, S.; Kashino, I.; Goto, A.; Mizoue, T.; Noda, M.; Sasazuki, S.; Sawada, N.; Tsugane, S. Quality of diet and mortality among Japanese men and women: Japan Public Health Center based prospective study. BMJ 2016, 352, i1209. [Google Scholar] [CrossRef] [Green Version]
- Hale, M.W.; Spencer, S.J.; Conti, B.; Jasoni, C.L.; Kent, S.; Radler, M.E.; Reyes, T.M.; Sominsky, L. Diet, behavior and immunity across the lifespan. Neurosci. Biobehav. Rev. 2015, 58, 46–62. [Google Scholar] [CrossRef]
- Kalache, A.; de Hoogh, A.I.; Howlett, S.E.; Kennedy, B.; Eggersdorfer, M.; Marsman, D.S.; Shao, A.; Griffiths, J.C. Nutrition interventions for healthy ageing across the lifespan: A conference report. Eur. J. Nutr. 2019, 58, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Meydani, S.N.; Leka, L.S.; Fine, B.C.; Dallal, G.E.; Keusch, G.T.; Singh, M.F.; Hamer, D.H. Vitamin E and Respiratory Tract Infections in Elderly Nursing Home ResidentsA Randomized Controlled Trial. JAMA 2004, 292, 828–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abood, R.A.; Hasson, H.M.; Khalaf, A.A.; Saleh, E.M. Impact of Comorbidities on Survival Among Patients with Chronic Myeloid Leukaemia Using the Charlson Comorbidity Index: Retrospective study from Basra, Iraq. Sultan Qaboos Univ. Med. J. 2019, 19, e236–e241. [Google Scholar] [CrossRef]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Kmietowicz, Z. Covid-19: Highest risk patients are asked to stay at home for 12 weeks. BMJ 2020, 368, m1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdulla, F.; Nain, Z.; Karimuzzaman, M.; Hossain, M.M.; Rahman, A. A Non-Linear Biostatistical Graphical Modeling of Preventive Actions and Healthcare Factors in Controlling COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4491. https://doi.org/10.3390/ijerph18094491
Abdulla F, Nain Z, Karimuzzaman M, Hossain MM, Rahman A. A Non-Linear Biostatistical Graphical Modeling of Preventive Actions and Healthcare Factors in Controlling COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(9):4491. https://doi.org/10.3390/ijerph18094491
Chicago/Turabian StyleAbdulla, Faruq, Zulkar Nain, Md. Karimuzzaman, Md. Moyazzem Hossain, and Azizur Rahman. 2021. "A Non-Linear Biostatistical Graphical Modeling of Preventive Actions and Healthcare Factors in Controlling COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 9: 4491. https://doi.org/10.3390/ijerph18094491