
“Yes, in Crisis We Pray”. The Role of Prayer in Coping with Pandemic Fears


1
Department of Social Sciences, University of Szczecin, 71-017 Szczecin, Poland
2
Department of Human Sciences, University of Economics and Innovation, 20-209 Lublin, Poland
*
Author to whom correspondence should be addressed.
Religions 2021, 12(10), 824; https://doi.org/10.3390/rel12100824
Submission received: 23 July 2021
/
Revised: 15 September 2021
/
Accepted: 22 September 2021
/
Published: 1 October 2021
(This article belongs to the Special Issue Prayer: A Psychological Perspective)
Abstract
:Based on the concepts of Huber’s centrality of religiosity as psychosocial resource, a non-experimental, moderated mediation project was designed in a group of 176 women and 84 men, who voluntarily participated in an online study, analysing the relationship between the prayer and the fears (for health, economy/finances, social life and family relations) during the COVID-19 pandemic. Multiple regression analysis was used to determine the general tendency in dependencies between variables. Among the assessed components of religiousness crucial for alleviating the fears of the COVID-19 pandemic, two forms of prayer—Private Practice and Public Practice—turned out to be the most important. Private Practice seemed to appease the fears of threats to family and social relationships of persons assessed, while Public Practice was revealed as the predictor of intensifying of the general, summed up level of fears. The areas of health (illness threat) and financial security fears were not associated neither with prayer nor any other components of religiousness. It means a selective predictive associating of prayer with the appeasing of only specific types of fears, namely those of a social nature. The results obtained point to the importance of the addressed topic in the context of searching for psycho resources in coping with difficult situations and determining their impact.
“Even though I walk through the valley of the shadow of death,I will fear no evil”(Psalm 23)
1. Introduction
If religiousness—as a phenomenon composed of various elements—comprises judgements and convictions on the supernatural and the experiences and feelings associated with them, then prayer is a certain predisposition to specific behaviour (Spilka and Ladd 2013). “Prayer is the driving force of all human efforts, of the entire spiritual life” (Łosski 2007, p. 195). What is prayer in the Bible? It is how those who believe in God talk to him. That is how they reveal their eulogies and requests. Prayer is sometimes also defined as a deeply human instinct of humanity, by which a person becomes aware of its relation to the source of life (Sadeghimoghaddam et al. 2019). Standing in prayer in the presence of God, we discover our wounds, weaknesses, and often helplessness (Werbiński 2010). Therefore, it happens both in good and bad times. The pandemic has made people search for support in dealing with the perils they experience. Google data say that the searches for the word “prayer” in 95 countries have risen up to the highest level ever recorded (Bentzen 2020). Referring to the sacred sphere in situation of uncertainty or threat, is a quite evident mechanism; psychologists of religion call attention to the fact that people often resort to prayer when their control over the situation is questioned (Cekiera 2020; Spilka and Ladd 2013).
The COVID-19 pandemic is obviously a rather shocking experience that may jeopardise the feeling of safety and the mentioned feeling of control (so it happened especially during the so-called first pandemic wave, when there was practically no expertise available on the virus and the illness it caused). In an unpredictable way it has reconfronted people from around the world with instability and chaos resulting from disastrous events (Sinding Bentzen 2019), however, of dimensions hitherto unknown. What prayer may be in the pandemic reality? The coronavirus uncertainty triggers various strategies to deal with this situation that exceeds the imagination of many, designed to recover one’s control over own life as far as possible. Offering one’s destinies to the hands of God may be one of them. In theism, what matters is humanity’s strong faith in the prospect of God’s aid in illness and its threat, and the transcendental activity of God in response to this faith. The suggested therapeutical elements of praying in a difficult time in life which certainly is the pandemic of a new, unknown and dangerous disease, are triggered by the transcendental relation of intentionality (addressing God to ask for help, the so-called prayer of petition), and may be considered a potential psycho resource, promoted by research published on this matter.
1.1. The Purpose of the Study
Published research increased the alert on serious psychological effects of the COVID-19 pandemic worldwide (Juchnowicz et al. 2021; Lakhan et al. 2020; Nguyen et al. 2020; Salari et al. 2020; Sood 2020; Torales et al. 2020; Walecka et al. 2021). Therefore, it is important to search for resources that may help to deal with the negative psychological effects more efficiently, both with the pandemic as well as the post-pandemic. Why do we think that prayer may exert a toning effect on the fears associated with the pandemic? An extensive review of respective publications points to the immunogenic meaning of this resource. It seems that prayer is not only words addressed to God, it also becomes words said by man for himself, words that are educating and supportive (Ławreszuk 2014). The presented empirical studies focus on analysing the relationship between prayer and health, suggesting its immunogenic character. Our study addressed the impact in the COVID-19 pandemic of one of the attitudes most deeply rooted in us as humans—the prayer. The main purpose of this study was to determine the relationship between prayer and intensified fear reactions caused by the COVID-19 pandemic in a sample of healthy people (Poland). The study covered dependent variables of four types (areas) of fear reactions: health fear, financial safety fear, social and family relations fear, and apart from the Private Practice (personal prayer) as the main independent variable, also four other structural elements of religiousness (Intellect, Ideology, Religious Experiences, and Public Practice), that determine the scope of Religiousness Centrality) based upon Huber’s concept. We treat this theory as a theoretical tool for predicting events. The study tested the hypothesis that prayer is a predictor of intensifying fear reactions triggered by the COVID-19 pandemic.
1.2. Background
Activity naturally complements the religious experience. Religiousness is expressed by religious practices, the fulfilling of duties stemming from convictions. Prayer is one of these activities. The word “prayer” has many meanings, as we call “prayer” also the thanksgiving, praising the glory of God, or joy of the beauty of creation. The person who expresses gratitude to God, also recognises his dependence and asks God to let him continue enjoying his goodwill (Vergote 2021, https://opoka.org.pl/biblioteka/T/TS/modlitwa_i_psychologia.html; accessed on 28 June 2021). The etymology of the word priere (prayer, but also petition) recalls this situation that determines its structure. As indicated by the word precarius, from which priere is derived, prayer expresses the situation when a person addressing his God realises the fragility of own condition. The intention that animates the prayer is awareness of absence, even when a person does not know what he lacks. The contact certainly arises from the awareness of emptiness, and the word directed to another always states the petition, if only to be listened to. The term “prayer” may be also used in the broad meaning to state concentration or meditation practised by redeeming religions, those that address their message to the personal conscience to transform it, without making man leave the community life (Vergote 2021, https://opoka.org.pl/biblioteka/T/TS/modlitwa_i_psychologia.html; accessed on 28 June 2021). Referring to the definition of prayer as concentration, it may also be said that concentration is sometimes an activity enabling man to free himself from the dispersion that alienates him from himself. Sensual impulses are removed, for example by closing the eyes, or by concentrating on a single object (Vergote 2021, https://opoka.org.pl/biblioteka/T/TS/modlitwa_i_psychologia.html; accessed on 28 June 2021). Therefore, prayer may be also so considered, more in the categories of specific tension control techniques.
Therefore, prayer is a behavioural component of religiousness that apart from the intellectual and emotional components, also develops a religious attitude (Huber 2003, 2008). According to Pargament (1999), the combination of religiousness as religious practice and convictions with the emotional reference to the sacred offers new study options, whilst prayer seems to be one of the very important elements of religious practices. Pan et al. (2012) point to the importance of the Holy Bible and of prayer in times of stress. It is consistent with published studies that show that prayer is a mechanism to cope with issues and is the most common among all religious attitudes (Hood et al. 2018; Spilka and Ladd 2013; Taylor et al. 2004). Additionally, its resilient functions are indicated to deal with the personal and social state of permanent uncertainty (Ano and Vasconcelles 2005; June and June 2021; Sinding Bentzen 2019; Meza 2020; Pargament [1997] 2001). As observed by Entwistle et al. (2018), and Tolmie and Venter (2021), the Holy Bible contains narratives that may be helpful especially in times of disasters and suffering, which are critically fearful events.
The literature on connection between religiousness and experience of fears reveals two completely different causes: (a) fear that motivates religious faith, and (b) faith that alleviates the fear. The first is associated with the feeling of helplessness in the face of imminent annihilation. Hence the answer is “effort”, “imagination”, “illusion” or “wish” that encourage to follow the concept of immortality, be it literal or symbolic. The foundations of this term are usually the affirmation of the existence of supernatural creatures, the practising of certain rituals and regulating of attitudes by moral codes. This shows that all this religious experience alleviates the anxiety triggered by the awareness of one’s own finiteness. Therefore, religious persons could enjoy a lower level of fear thanks to their rituals, norms, social relationships and system convictions (Meza 2020). Exactly the prayer is an element of practice, the basic factor of man’s religious life (Woroniecki 2018).
For the purpose of this research project we adopted Huber’s psychological concept of religiousness as a system of personal religious constructs—Ideology, Private Practice, Religious Experience, Public Practice and Intellect with special focus on the immunogenic role of prayer, together with an attempt to rationalise them empirically, made possible by Huber’s tool. The model designs an integrative, comprehensive way to collect empirical evidence by a self-report scale—the CRS.
2. Method
2.1. Participants and Procedure
Studies were conducted in the first weeks of complete lockdown during the first wave of the pandemic (Spring 2020). The tested sample of 176 women (67.7%, MAGE = 36.66, SD = 13.09) and 84 men (32.3%, MAGE = 41.23, SD = 13.9) aged from 18 to 71 was chosen via the Internet, using the snowball sampling method, which is a procedure admissible in exploratory studies (Babbie 2016). Respondents were also told, “You do not have to be religious or spiritual to answer these questions. We want to hear from people with all types of points of view”. Participants did not receive any remuneration for participating in the study. It should be emphasised that the presented study was carried out in a Polish sample, thus probably Roman Catholic. Basic sociodemographic data on the assessed group are presented in Table 1. Analysis of differences in basic social–demographic features does not differentiate male and female respondents.
2.2. Measures
For the study, a tool standardised to measure the centrality of religiousness and an own slide method were used to measure the fears due to the COVID-19 pandemic.
2.2.1. Centrality of Religiosity Scale (CRS)
The CRS Scale by Huber in its Polish adaptation by (Zarzycka 2007, 2011; Zarzycka et al. 2020) is a measure of the centrality of religiosity, i.e., the position of a system of religious constructs in human personality. It consists of five sub-scales: (1) Intellect, i.e., the frequency and importance of cognitive confrontation with religious content, without taking into account the aspect of their personal acceptance; (2) Ideology—the degree of subjectively assessed probability of the existence of transcendent reality and the intensity of openness to various forms of transcendence; (3) Private Practice—the frequency of contact with transcendent reality and the subjective meaning of that contact for an individual (personal prayer); (4) Religious Experience—the frequency with which transcendence becomes part of human experience and the extent to which the transcendent world of religious meanings is individually confirmed by the sense of communication and action; (5) Public Practice—the frequency and subjective meaning of human participation in religious services. The overall result is the sum of the subscale results and is a measure of Centrality of the system of religious meanings in an individual’s personality. The scale consists of 15 items with a Likert scale to which the respondents respond choosing between 5 and 8 possible responses. In each case the responses are transposed to the 5-point scale (the higher the score, the greater the importance/frequency of behaviour). The a-Cronbach factor for the overall score is 0.93, for Ideology 0.90, Private Practice 0.88, Religious Experience 0.86. The factor for Intellect and Public Practice is 0.82. The values of intercorrelation between items and the score in individual subscales indicate the accuracy of a separate theoretical construct, and the subscales can be considered homogeneous (Huber and Huber 2012; Zarzycka 2007).
The term Private Practice is the frequency of establishing contact with the transcendental reality, and the subjective importance of this contact for man (Zarzycka 2007; Zarzycka et al. 2020). While investigating the dimension of Private Practice we ask questions concerning the frequency of making contact with transcendent reality by the respondent, and its subjective meaning for a person. This is pursued by asking the following questions: (1). How often do you usually pray? (2). How important for you is personal prayer? (3). How often during a weekday do you direct a short prayer to God? This dimension includes an individual and personal dialogue with God, ritualistic prayer practices, and provides information about actual updating meanings of transcendental character. It also shows the intensity of using the potential of religious beliefs by an individual (Ackert et al. 2020; Huber 2003; Huber and Huber 2012; Zarzycka 2007, 2011).
We use the term Public Practice in accordance with the meaning proposed by Huber, which means the frequency and subjective importance of participation of a person in services. It provides information concerning social (communitarian) rooting of religiosity and, similar to the dimension of Private Practice, covers religious practices, expressed in various forms of worship. While investigating the dimension and role of Public Practice, questions are asked concerning the frequency and subjective importance of participation in services: (1). How often as a rule do you participate in services—also via radio or television? (2). How important for you is participation in services? and (3). How important for you is bond with the religious community? In this way information is collected concerning the social meaning and rooting of religiosity (Ackert et al. 2020; Huber 2003; Zarzycka 2007, 2011).
2.2.2. COVID-19 Fears Measure
To measure the fears of the COVID-19 pandemic we used the simple numerical method (NRS) by which the persons assessed state the intensity of fears associated with (a) fear of the risk of contracting the SarsCov2 virus (fear for health), (b) financial security fear due to the pandemic (fear for economy/finances), (c) fear of relations with distant family, friends and colleagues (fear for social life), and (d) family relations fear due to the COVID-19 pandemic, house quarantine and lockdown (fear for family relations). The respondents determined the fear intensity in a scale from 1 to 10, experienced in a given situation. Answers in all areas may be summed up (minimum 4, maximum 40), indicating the overall intensity of fears due to the pandemic.
2.2.3. Statistical Analysis
Multiple regression analysis was used to determine the general tendency in dependencies between variables. Statistical calculations were done using STATISTICA v.13 package.
3. Results
3.1. Sample Characteristic
The analysis of differences has not indicated differences between average results obtained by respondents in specific areas (Table 2), as a result of which it was decided to perform further analyses of the results of the whole study group.
3.2. Correlation Analysis
Self-reported changes in fears of social life, fear of family relations and general fear level during the pandemic were significantly correlated with all aspects of religiosity (Table 3).
There were no important connections between the tested aspects of religiousness, the health fear and the economic fear. The results show that the character of relations between religiousness and fear due to the COVID-19 pandemic creates a rather ambiguous structure of relations. Therefore, an analysis of multiple regression was carried out using the input method. Due to the lack of differences between women and men in the intensity of assessed variables, further analyses were carried out on the whole assessed group.
3.3. Multiple Regression Analysis Results
Multiple regression analysis was used to determine the general tendency in dependencies between variables (Table 4).
The analysis of results shows that Public Practice was the only predictor of a decreasing level of the overall intensity of fears due to the COVID-19 pandemic in the assessed group.
Additionally, a series of regression studies were carried out on the impact of all aspects of religiousness on the intensity of specific types of fears associated with the COVID-19 pandemic. It was stated that among the components of religiousness there were no important predictors of health and economic (financial) safety fears (Table 5, part A,B).
The results of the analysis indicate that none of the components of religiousness were effective in reducing fears for health and fears for economy/finances.
The analysis of fears in the social relations domain shows that Private Practice and Public Practice are the significant predictors (Table 5, part C). Both predictors made clear the rather approximate level of variability of the social fear, made evident by the absolute value of the Beta coefficient. In event of intensified fears associated with family relations, only Private Practice turned out to be the important predictor (Table 4, part D). These results mean that the more often the respondents prayed (indicated by the result of Private Practice sub-scale), the less fear for social life and family relations they felt. On the other hand, participation in the service (Public Practice) lowered their fear for social life.
4. Discussion
For the first time in the history of modern science, we had the opportunity to follow the attitudes in face of the anticipated annihilation or actual threat to the life and health of large social groups. It is a paradox that the global crisis of the COVID-19 pandemic has provided such opportunities to scientists around the world. Prayer is among the attitudes revealed as predictors of the areas of fear reactions and that may be crucial to preserve the well-being by reducing the level of fear due to social relations and family life, whilst for fear in general—the attitudes and experiences associated with religious practices.
There is evidence proving that prayer activities have intensified during the current pandemic (Bentzen 2020; Dein et al. 2020). However, what is their true contribution to alleviating the pandemic fears? The focus of our work is exactly an attempt to explain the functionality type of prayer activity in dealing with fears due to various aspects of functions—health (fear of illness), finances (fear that the pandemic may threaten the financial safety of respondents), social relations (fear of the vision of reduced social relationships) and family relations (fears due to worsening family relations triggered by home quarantine, the imperative to reorganise space, changing paternal responsibilities, shaken borderlines between professional and family lives triggering additional conflicts, etc. (Tuszyńska-Bogucka 2020).
Prayer may affect the stress and ability to cope, it has been proven to be associated with happiness and a feeling of overall well-being (Francis and Robbins 2000; Francis and Lester 1997; Huber 2007; Jantos and Kiat 2007; Poloma and Pendleton 1989, 1991; Szałachowski and Tuszyńska-Bogucka 2021). As regards the role of prayer in coping with fear, it has been described in many studies. Those addressed mainly the role of prayer in time of illness (Ambs et al. 2007; Anderson and Nunnelley 2016; Boelens et al. 2009, 2012; Carvalho et al. 2014; Hollywell and Walker 2009; Jors et al. 2015; June and June 2021). We should mention that our study does not address the intercessory prayer that has a quite special position in literature.
The essence of its impact on alleviating the symptoms of illness was explained using cognitive, emotional and psychoneuroimmunological mechanisms (Andrade and Radhakrisnan 2009; Kiecold-Glaser et al. 2002; Kiecold-Glaser and Glaser 1992; Koenig 2000, 2001; Koenig and Cohen 2002; Koenig et al. 1997; Masters and Spielmans 2007). As regards the protective effect of prayer activity, the two most important and probably best known longitudinal studies should be stated. Koenig et al. (1999) during the more than six years of monitoring the effect of prayer activity, have stated that participation in mass has importantly reduced the risk of death in the assessed group of 3968 persons aged 64–101. In a similar study by Helm et al. (2000) the so-called private religious activity (namely prayer, meditation, or bible study) has ensured a protective effect against mortality during the six years of monitoring studies within the group of 3851 persons aged above 65 (provided those were persons without functional disabilities), at which it was enough that the said activity took place “several times a month” (however, the authors themselves quote their results with some caution, having observed that after considering the demographic variables, the relevance of the effect did not continue), which means that both “private” and “group” prayers (during worship) seem to suggest their immunogenic values. As studies show, prayer is used by persons of all theistic confessions, and also by those who do not belong to a specific religious tradition (Masters and Spielmans 2007). “There are men and women who consciously do not believe in God, but who in times of great existential distress still pray to the God whose existence they are denying” (Vergote 2021, https://opoka.org.pl/biblioteka/T/TS/modlitwa_i_psychologia.html; accessed on 28 June 2021).
One should return to the pandemic as a critical situation. Studies show that people tend to intensify their prayer activities having exhausted other ways to cope or when the situation looks desperate, and when these factors are taken into account, the apparently negative relation between prayer and psychological health disappears. It has also been revealed that people tend to engage more strongly in prayer when problems are acute, chronic or when other ways to cope fail (Sinding Bentzen 2019; Bentzen 2020; Ellison et al. 2001; June and June 2021).
Our study, apart from (partly) confirming the phenomena previously stated in literature, has also provided additional conclusions. Therefore, it turned out that among the assessed aspects of religiousness, two were revealed as predictors of fear (fears), namely Private Practice (personal prayer) and Public Practice (the frequency and subjective meaning of human participation in religious services). Public Practice did importantly reduce the overall level of fear associated with the pandemic experience of persons assessed. Private Practice showed a predictive impact that reduced the intensity of fears due to social and family relations of persons assessed. What is interesting and not obvious is the fact that none of the analysed aspects of religiousness were a predictor of health and financial fears. It is revealed that Private Practice did not make an effective alleviating impact on all types of fears. It interestingly contradicts the results of a study proving that among the most searched prayers in Google in March 2020 was the “coronavirus prayer”, or the prayer by which believers ask God to protect them from the coronavirus, to give them force to resist and the thanksgiving for the efforts of the health service personnel (Meza 2020).
The results obtained may point to two phenomena, namely the operability and effectiveness of prayers by persons assessed (at which we have in mind both the individual and group prayer activities, measured by the Public Practice factor). Then firstly they should be perhaps understood in categories of the prayer by the 21st century person who believes that medicine and doctors determine the state of health (let us keep in mind the specific proportion of the assessed group, dominated by persons with university degrees or students), while one should take care of his finances by himself? The specific feature of the pandemic situation is also a certain argument in this regard. Perhaps the assessed persons confined to their homes, forced to remain close to their loved ones and cut off from their broad social environments have begun feeling more strongly the hardships of such lifestyle, without being yet affected by financial problems and the threat of contracting the virus (as they remained inside the relatively safe houses)? Then the abruptly restricted physical space may have resulted troublesome, they may have also been painfully impacted by the prohibition of going outside (apart from critical situations), of contacting friends and more distant relatives. It would be consistent with Vergote’s concept of the role of prayer, by which religion is a power that frees a person, helping him to cope with harsh everyday life, touching tangible reality (Vergote, after Mach 1998). People may constitute this tangible and closest reality—important persons that are accompanying the individual all the time uninterruptedly during the lockdown, or who have vanished from the physical space quite abruptly without warning. Maybe people also want to avoid asking for physical health, fearful that God would not answer their prayers, or by surrendering to God’s will (especially Muslims—Rezaei et al. 2008, although our study is about Christians). Dein and Pargament (2012) suggest that praying for psychological, not physical changes may help people avoid a cognitive discordance and continue believing that God may, if willing to, intervene in their world. It is consistent with the Origen’s understanding of prayer, according to which petitions in prayer cannot apply to everything what man wants, and certainly not to material goods (Szram 2012).
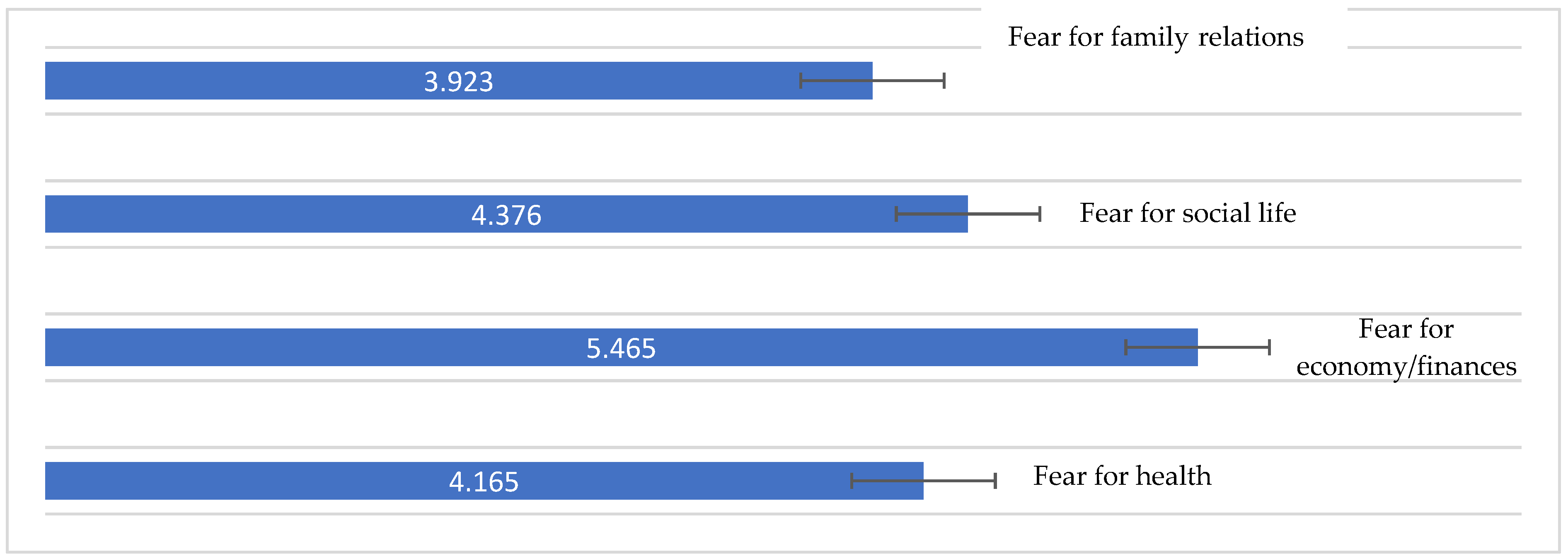
Secondly—maybe the health and economic fears were so acute that prayer (Private Practice) proved ineffective in this case? Let us observe how strong was especially the financial fear of persons assessed (Chart 1). On the other hand, the assessed group included persons relatively young and well educated who perhaps see their resources to handle the effects of the pandemic in these SES features instead of prayer? It should be emphasised that the presented study was carried out in a Polish sample. This may allow the understanding of the importance of the results in the context of the country’s politics and economic dynamics. In more wealthy economies, people who lost their jobs as a result of the pandemic received wider financial support from their government, and for this reason were less anxious about this aspect of the situation (the pandemic may even be seen as a kind of vacation). In Poland, the image of anxiety could have been entirely different due to a different economic situation of the country.
Pargament [1997] 2001 and other analysts (McIntosh and Spilka 1990) place prayer among the health resources whose effectiveness may nevertheless depend on its style: from the postponement prayer style (actually using prayer to make God responsible and thus free oneself from his own responsibility), by the style of cooperation (by which the mover continues praying for the ways to cope with the stressor and expects God to assist in this process, but the person offering prayers also uses them to stay motivated and work to find solutions or ways to handle the problem), up to the self-directed prayer (that does not need God in principle, as the individual is capable of personally taking over control to fix or handle the situation). It is an element that may be crucially important and should be included in future studies in this area. On the other hand, Ladd and McIntosh (2008) emphasise the role of prayer in a religious environment, recommending it as a way to describe metaphysically the character of relations between divinity, other people and one’s true self.
It should be also stressed that our study is consistent with the trend relating to the prayer frequency effect (the focus of Huber’s tool is precisely on this aspect, not addressing the content of prayer in principle) on a person’s feeling (also on fear reduction). It is confirmed that the frequency of prayer is related to better health (Maltby et al. 1999; Meisenhelder and Chandler 2001). However, it should be stressed that the evidence in this area has been critically assessed by Masters and Spielmans (2007), who concluded that they differ too much in the methodology aspect (e.g., in terms of analysed populations, results and variables included in studies as controls or moderators), as to be used as basis to generalise the conclusion on the nature of relations between the frequency of prayers and the health results.
Literature indicates several hypotheses that explain the impact of frequent prayer on a person’s health and comfort: (1) intensified prayer may improve the psychological and physiological functions, which is associated with better comfort and potential health effects; (2) when people fall ill or their health and functions deteriorate or when it is threatened, they may tend more to search for divine comfort and help in dealing with illness, or even expect a cure; (3) those who pray in stressful times tend to focus on their own stress when praying, thus they are concentrated on their own problems rather than on the ways of handling them, leading to a passive and potentially harmful strategy of coping; or (4) those who pray in stressful times tend to focus on how God’s intentions and plans may help them survive the difficult situation, possibly generating a power feeling. It also seems that one should consider at this point the possible effect of the content of prayer, that is, perhaps the words and topic of prayer as such may alter the cognitive processes of the petitioning person in a positive way (Masters and Spielmans 2007). In our future studies we intend to include all stated options associated both with the content and the style of prayer activities as the psycho resource factor.
Limitations. We are aware of the fact that our studies are not free from limitations. Size and proportions of the group. More participation of women in voluntary studies on psychological effects of the COVID-19 pandemic is rather a standard, not an exception (Dębski et al. 2021; Fullana et al. 2020; Juchnowicz et al. 2021; Knolle et al. 2021; Nikolaidis et al. 2021; Padmanabhanunni and Pretorius 2021; Palgi et al. 2020; Pierce et al. 2020), not meaning that we are unaware of the limitations of conclusions caused by this situation. The number of respondents we obtained was generally low, although sufficient to test the formulated hypotheses. We did not consider it appropriate to maximize sample size at this stage of the research, which largely relies on a preliminary analysis of connections between prayer and fear. Moreover, the end of studies was forced upon by the government’s decision to end the home quarantine; further recruitment was inadvisable, as it would bring in persons in a totally different psychosocial situation.
Data collecting. Online research, although today recognised as a research standard, has its limitations (for example the lack of standard research conditions), which should be borne in mind when interpreting the results. It is important also to stress the limitations linked with the sampling method: recruitment was carried out via online where some categories (e.g., young, highly educated, and technology-proficient individuals) might be overrepresented compared to their actual frequency in the population. Moreover, variables such as experience of other stressful events were not measured, although they might have an impact on the results.
Patterns of prayer. Identifiable patterns of prayer may exist, that can be observed among people over time. Some persons may consistently demonstrate the same frequency and content of prayers regardless of circumstances, while the prayer patterns of others may be highly dependent on situation factors. Therefore, it is worthy to consider at this point the longitudinal studies, that are anyway recommended by literature (Masters and Spielmans 2007).
Multiplicity of potential intermediary variables. Self-describing studies have their limits, that are especially worthy of attention in world literature. The most basic question of the interest in the prayer issue is, “does prayer affect health?” Self-describing studies, even supported by sophisticated statistics, may only tell whether the prayer (in our case mainly its frequency) was associated with health (reducing the fear), but do not enable to draw a strong conclusion that the prayer has actually affected the psychical health of assessed persons, therefore, it is worthy to include the clinical diagnosis variable in the future. In this case, also the potential impact of other variables should be taken into consideration, such as personality, family environment, early patterns to be followed, etc. (what is also indirectly suggested by the scope of the regressions of variances explained by equations used).
Tool. Fears have been measured using a survey that we structured, that lacks the best psychometric qualities of standardised tools. However, we had no other choice, as the fear measurement questionnaire dedicated to COVID-19 developed by (Ahorsu et al. 2020) was published in Poland only in October 2020. Neither does it include the areas of fear experience of our interest, so we decided to use a tool of our own concept, developed by ourselves.
5. Conclusions
Formal proofs of truth can be made in mathematics. Scientific theories do not have binary logical value as absolute truth or absolute falsehood. Science is not a system of axioms, but models that adapt to empiricism, and thus more and more consistent with experience and explain the observed phenomena better and better. Among the assessed components of religiousness crucial for alleviating the fears of the COVID-19 pandemic, Private Practice and Public Practice turned out to be the most important. Private Practice seemed to appease the fears of threats to family and social relationships of persons assessed, while Public Practice was revealed as the predictor of intensifying of the general, summed up level of fears. The areas of health (illness threat) and financial security fears were not associated neither with Private Practice nor any other components of religiousness. It means a selective predictive associating of Private Practice with the appeasing of only specific types of fears, namely those of a social nature.
Our studies have quite relevant practical implications. Certainly, one should become aware of the psychological dimension of religious practice. Contemporary psychologists face the task to reveal and make fruitful for the modern person the rich experience of people who pray. At this point one should also address the concept according to which the online prayer may replace prayer in church. It seems that moving churches to the Internet as a “pragmatic response” (Campbell 2020a) to this cultural change does not reflect the diversity of religious practice during the pandemic (Meza 2020), because the religious experience is usually more polymorphic. Moving the churches to the Internet not only undermines the acceptance of the concept of community as a dynamic and changing process structured with various relations and determined by the personal needs and choices of its members, it also can eliminate the set of religious practices exercised by individuals in home groups or individually (Meza 2020).
One should note that a study by the Public Opinion Research Centre (Centrum Badania Opinii Społecznej) indicated that 9% of Poles have admitted physically participating in mass, even when the official limit was five persons (Boguszewski et al. 2020). Media reports in Poland (Grochot 2020) and other countries (Wildman et al. 2020) state that breaching the official limits on meetings meant to practise religious cult, is quite common. This shows just how important it is for many persons to join such gatherings, despite the looming danger. Studies reveal that in some countries even about 60% of all infections may be due to participation in mass (Bostock 2020), meaning that it is a domain of a particular safety concern. It is important data, as on one hand pointing to the importance of the possibility to join a religious service, and on the other indicating the pandemic threats it may entail. Therefore, it seems that the issues of organising a so-called safe cult should become the purpose of intensified efforts by political decision-takers. It should be noted that the lower level of concerns and anxiety of persons who attended mass more often, suggest not only the possible effects of buffering and dealing with, but also the importance of the function of social support that may be ensured by churches and religious communities (Merino 2014; Taylor et al. 2004). Therefore, maybe “The COVID-19 pandemic offers an important moment for religious institutions to re-evaluate whether or not their models of ministry truly meet people’s desires for community and connection with others”? (Campbell 2020b).
Although, prayer, both the individual and collective cannot be considered as a panacea for all problems of people in time of crisis, and “does not free a person (…) from the feeling of strangeness and solitude and from various crises of meaning, nevertheless it does offer the opportunity to include all those feelings into a credible axiological universe that somehow acquires an objective feature” (Mariański 2013, p. 158). It is important, taking into consideration that even when the COVID-19 pandemic eventually comes to an end, regrettably its consequences may be far-reaching, creating a so-called post-pandemic world, that may probably shape our environment in the coming years.
Author Contributions
Conceptualisation, W.T.-B., and R.R.S.; methodology, W.T.-B., and R.R.S.; formal analysis, W.T.-B., and R.R.S.; investigation, R.R.S., and W.T.-B.; resources, R.R.S., and W.T.-B.; writing—original draft preparation, W.T.-B., and R.R.S.; writing—review and editing, R.R.S., and W.T.-B.; visualisation, R.R.S., and W.T.-B.; supervision, R.R.S., and W.T.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the appropriate institutional research Ethics Committee and performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, or comparable ethical standards.
Informed Consent Statement
Patient written consent was waived due to instant anonymization of the results (obtained via Internet without personal data - inability to identify. Consent expressed in the online form).
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors have no conflicts of interests to declare.
References
- Ackert, Michael, Erekle Maglakelidze, Irina Badurashvili, and Stefan Huber. 2020. Validation of the Short Forms of the Centrality of Religiosity Scale in Georgia. Religions 11: 57. [Google Scholar] [CrossRef] [Green Version]
- Ahorsu, Daniel Kwasi, Chung-Ying Lin, Vida Imani, Mohsen Saffari, and Mark D. Griffiths. 2020. The fear of COVID-19 scale: Development and initial validation. International Journal of Mental Health and Addiction 27: 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, James W., and Paige A. Nunnelley. 2016. Private prayer associations with depression, anxiety and other health conditions: An analytical review of clinical studies. Postgraduate Medicine 128: 635–41. [Google Scholar] [CrossRef] [PubMed]
- Andrade, Chittaranjan, and Rajiv Radhakrishnan. 2009. Prayer and healing: A medical and scientific perspective on randomized controlled trials. Indian Journal of Psychiatry 51: 247–53. [Google Scholar] [CrossRef]
- Anita, H. Ambs, Melissa F. Miller, Ashley W. Smith, Michael S. Goldstein, An-Fu Hsiao, and Rachel Ballard-Barbash. 2007. Religious and spiritual practices and identification among individuals living with cancer and other chronic disease. Journal of the Society for Integrative Oncology 5: 53–60. [Google Scholar] [CrossRef]
- Ano, Gene G., and Erin B. Vasconcelles. 2005. Religious coping and psychological adjustment to stress: A meta-analysis. Journal of Clinical Psychology 61: 461–80. [Google Scholar] [CrossRef] [PubMed]
- Babbie, Earl. 2016. The Practice of Social Research, 14th ed. Boston: Cengage Learning. [Google Scholar]
- Bentzen, Jeanet. 2020. In Crisis, We Pray: Religiosity and the COVID-19 Pandemic. CEPR: Public Economics (Topic): N. pag. Available online: https://cepr.org/active/publications/discussion_papers/dp.php?dpno=14824 (accessed on 23 May 2021).
- Boelens, Peter A., Roy R. Reeves, William H. Replogle, and Harold G. Koenig. 2009. A randomized trial of the effect of prayer on depression and anxiety. International Journal of Psychiatry in Medicine 39: 377–92. [Google Scholar] [CrossRef]
- Boelens, Peter A., Roy R. Reeves, William H. Replogle, and Harold G. Koenig. 2012. The effect of prayer on depression and anxiety: Maintenance of positive influence one year after prayer intervention. International Journal of Psychiatry in Medicine 43: 85–98. [Google Scholar] [CrossRef]
- Boguszewski, Rafał, Marta Makowska, Marta Bożewicz, and Monika Podkowińska. 2020. The COVID-19 Pandemic’s Impact on Religiosity in Poland. Religions 11: 646. [Google Scholar] [CrossRef]
- Bostock, Bill. 2020. South Korea is testing 200,000 members of a doomsday church linked to more than 60% of its coronavirus cases. Business Insider. February 25. Available online: https://www.businessinsider.com/south-korea-tests-every-shincheonji-cult-member-coronavirus-outbreak-2020-2?r=USandIR=T (accessed on 7 May 2021).
- Campbell, Heidi A. 2020a. Religion embracing and resisting cultural change in a time of social distancing. Religion in Quarantine: The Future of Religion in a Post-Pandemic World. Edited by Heidi A. Campbell. Network for New Media. College Station: Religion and Digital Culture Studies. pp. 9–14. Available online: https://hdl.handle.net/1969.1/188004 (accessed on 15 May 2021).
- Campbell, Heidi A. 2020b. Distancing Religion Online: Lessons from the Pandemic Prompted Religious Move Online. Available online: https://contendingmodernities.nd.edu/global-currents/distancing-religion-online-lessons-from-the-pandemic-prompted-religious-move-online/ (accessed on 27 June 2021).
- Carvalho, Camila Csizmar, Erika de Cássia Lopes Chaves, Denise Hollanda Iunes, Talita Prado Simão, Cristiane da Silva Marciano Grasselli, and Cristiane Giffoni Braga. 2014. A efetividade da prece na redução da ansiedade em pacientes com câncer [Effectiveness of prayer in reducing anxiety in cancer patients]. Revista da Escola de Enfermagem da U S P 48: 683–89. [Google Scholar]
- Cekiera, Rafał. 2020. “Ocal ludzkość przed koronawirusem!” Analiza internetowych intencji modlitewnych w czasie pandemii [“Save the mankind from the coronavirus!”. Analysis of internet prayer intentions during the times of pandemic]. LUD 4: 213–33. [Google Scholar] [CrossRef]
- Dębski, Paweł, Szymon Florek, Magdalena Piegza, Robert Pudlo, and Piotr Gorczyca. 2021. Is it good to be resilient during the COVID-19 period? The role of ego-resiliency in the intensity of symptoms of anxiety, alcohol use and aggression among Polish people. International Journal of Occupational Medicine and Environmental Health 34: 289–300. [Google Scholar] [CrossRef] [PubMed]
- Dein, Simon, and Keith I. Pargament. 2012. On not praying for the return of an amputated limb: Conserving a relationship with God as the primary function of prayer. Bulletin of the Menninger Clinic 76: 235–59. [Google Scholar] [CrossRef] [PubMed]
- Dein, Simon, Kate Loewenthal, Christopher Alan Lewis, and Kenneth I. Pargament. 2020. COVID-19, mental health and religion: An agenda for future research. Mental Health Religion and Culture 23: 1–9. [Google Scholar] [CrossRef]
- Ellison, Christopher G., Jason D. Boardman, David R. Williams, and James S. Jackson. 2001. Religious involvement, stress, and mental health: Findings from the 1995 Detroit Area Study. Social Forces 80: 215–49. [Google Scholar] [CrossRef] [Green Version]
- Entwistle, David N., Stephen K. Moroney, and Jamie Aten. 2018. Integrative reflections on disasters, suffering, and the practice of spiritual and emotional care. Journal of Psychology and Theology 46: 67–81. [Google Scholar] [CrossRef]
- Francis, Leslie J., and David Lester. 1997. Religion, personality and happiness. Journal of Contemporary Religion 12: 81–86. [Google Scholar] [CrossRef]
- Francis, Leslie J., and Mandy Robbins. 2000. Religion and happiness: A study in empirical theology. Transpersonal Psychology Review 4: 17–22. [Google Scholar]
- Fullana, Miguel A., Diego Hidalgo-Mazzei, Eduard Vieta, and Joaquim Radua. 2020. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. Journal of Affective Disorders 275: 80–81. [Google Scholar] [CrossRef]
- Grochot, Arkadiusz. 2020. Część Księży nie Przestrzega Obostrzeń i Wpuszcza do Kościoła Kilkadziesiąt Osób [Some Priests are Disobeying the Restrictions and Allowing Several Dozen People into Churches]. Available online: https://www.rmf24.pl/raporty/raport-koronawirus-z-chin/polska/news-czesc-ksiezy-nie-przestrzega-obostrzen-i-wpuszcza-do-kosciol,nId,4426635 (accessed on 13 July 2021).
- Helm, Hughes M., Judith C. Hays, Elizabeth P. Flint, Harold G. Koenig, and Dan G. Blazer. 2000. Does private religious activity prolong survival? A six-year follow-up study of 3,851 older adults. Journal of Gerontology 55: 400–5. [Google Scholar] [CrossRef]
- Hollywell, Claire, and Jan Walker. 2009. Private prayer as a suitable intervention for hospitalised patients: A critical review of the literature. Journal of Clinical Nursing 18: 637–51. [Google Scholar] [CrossRef] [PubMed]
- Hood, Ralph W., Jr., Peter C. Hill, and Bernard Spilka. 2018. The Psychology of Religion: An Empirical Approach, 5th ed. New York & London: Guilford Press. [Google Scholar]
- Huber, Stefan. 2003. Zentralität und Inhalt. Ein neues multidimensionales Modell der Religiosität. Opladen: Leske + Budrich. [Google Scholar]
- Huber, Stefan. 2007. Are religious beliefs relevant in daily life? In Religion Inside and Outside Traditional Institutions. Edited by Heinz Streib. Lieden: Brill Academic Publishers, pp. 211–30. [Google Scholar]
- Huber, Stefan. 2008. Kerndimensionen, Zentralität und Inhalt. Ein interdisciplinäres Modell der Religiosität. Journal für Psychologie. 16. Available online: http://www.journal-fuer-psychologie.de/jfp-3-2008-05.html (accessed on 20 December 2020).
- Huber, Stefan, and Odilo W. Huber. 2012. The Centrality of Religiosity Scale (CRS). Religions 3: 710–24. [Google Scholar] [CrossRef]
- Jantos, Marek, and Hosen Kiat. 2007. Prayer as medicine: How much have we learned? The Medical Journal of Australia 186: 51–53. [Google Scholar] [CrossRef]
- Jors, Karin, Arndt Büssing, Niels Christian Hvidt, and Klaus Baumann. 2015. Personal prayer in patients dealing with chronic illness: A review of the research literature. Evidence-Based Complementary and Alternative Medicine 2015: 927973. [Google Scholar] [CrossRef]
- Juchnowicz, Dariusz, Jacek Baj, Alicja Forma, Kaja Karakuła, Elżbieta Sitarz, Jacek Bogucki, and Hanna Karakula-Juchnowicz. 2021. The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown. Journal of Clinical Medicine 10: 944. [Google Scholar] [CrossRef]
- June, Lee N., and Shirley A. June. 2021. Initial Real Time Coping by African American Christians During the Coronavirus Pandemic (COVID-19). Journal of Pastoral Care and Counseling, 1–9. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, Janice K., and Ronald Glaser. 1992. Psychoneuroimmunology: Can psychological intervention modulate immunity? Journal of Consulting and Clinical Psychology 60: 569–75. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, Janice K., Lynanne McGuire, Theodore F. Robles, and Ronald Glaser. 2002. Emotions, morbidity, and mortality: New perspectives from psychoneuroimmunology. Annual Review of Psychology 53: 83–107. [Google Scholar] [CrossRef] [Green Version]
- Knolle, Franziska, Lisa Ronan, and Graham K. Murray. 2021. The impact of the COVID-19 pandemic on mental health in the general population: A comparison between Germany and the UK. BMC Psychology 9: 60. [Google Scholar] [CrossRef]
- Koenig, Harold G. 2000. Psychoneuroimmunology and the faith factor. The Journal of Gender-Specific Medicine: JGSM: The Official Journal of the Partnership for Women’s Health at Columbia 3: 37–44. [Google Scholar]
- Koenig, Harold G. 2001. Religion and medicine III: Developing a theoretical model. International Journal of Psychiatry in Medicine 31: 199–216. [Google Scholar] [CrossRef] [Green Version]
- Koenig, Harold G., and Harvey J. Cohen. 2002. The Link between Religion and Health: Psychoneuroimmunology and the Faith Factor. Oxford: Oxford University Press. [Google Scholar] [CrossRef]
- Koenig, Harold G, Harvey J. Cohen, Linda K. George, Judith G. Hays, David B. Larson, and Dan G. Blazer. 1997. Attendance at religious services, interleukin-6, and other biological parameters of immune function in older adults. International Journal of Psychiatry in Medicine 27: 233–50. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Harold G., Hays Judith, Larson David, George Linda, Cohen Hezekiah Joseph, Mccullough Michael, Meador Keith, and Blazer Dan. 1999. Does Religious Attendance Prolong Survival? A Six-Year Follow-Up Study of 3968 Older Adults. The Journals Of Gerontology. Series A, Biological Sciences and Medical Sciences 54: M370-6. [Google Scholar] [CrossRef]
- Ladd, Kevin L., and Daniel N. McIntosh. 2008. Meaning, god, and prayer: Physical and metaphysical aspects of social support. Mental Health, Religion and Culture 11: 23–38. [Google Scholar] [CrossRef] [Green Version]
- Lakhan, Ram, Amit Agrawal, and Manoj Sharma. 2020. Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. Journal of Neuroscience in Rural Practice 11: 519–25. [Google Scholar] [CrossRef]
- Ławreszuk, Marek. 2014. Modlitwa wspólnoty. Historyczny rozwój prawosławnej tradycji liturgicznej [Community Prayer. Historical Development of the Orthodox Liturgical Tradition]. Białystok: Wydawnictwo Uniwersytetu w Białymstoku. [Google Scholar]
- Łosski, Włodzimierz. 2007. Teologia mistyczna Kościoła Wschodniego [Mystical Theology of the Eastern Church]. Kraków: Uniwersytetu Jagiellońskiego. [Google Scholar]
- Mach, Joanna. 1998. Patologia psychiczna a religijność w ujęciu Antoine Vergote’a [Mental pathology and religiosity according to Antoine Vergote]. Roczniki Psychologiczne 1: 147–65. [Google Scholar]
- Maltby, John, Christopher Allan Lewis, and Liza Day. 1999. Religious orientation and psychological well-being: The role of the frequency of personal prayer. British Journal of Health Psychology 4: 363–78. [Google Scholar] [CrossRef]
- Mariański, Janusz. 2013. Sens życia, wartości, religia. Studium socjologiczne. [The Meaning of Life, Values, Religion. A Sociological Study]. Lublin: Wydawnictwo KUL. [Google Scholar]
- Masters, Kevin S., and Glen I. Spielmans. 2007. Prayer and health: Review, meta-analysis, and research agenda. Journal of Behavioral Medicine 30: 329–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIntosh, Daniel N., and Bernard Spilka. 1990. Religion and physical health: The role of personal faith and control beliefs. Research in the Social Scientific Study of Religion 2: 167–94. [Google Scholar]
- Meisenhelder, Janice Bell, and Emily N. Chandler. 2001. Frequency of prayer and functional health in Presbyterian pastors. Journal for the Scientific Study of Religion 40: 323–29. [Google Scholar] [CrossRef]
- Merino, Stephen M. 2014. Social support and the religious dimensions of close ties. Journal for the Scientific Study of Religion 53: 595–612. Available online: www.jstor.org/stable/24644229 (accessed on 15 July 2021).
- Meza, Diego. 2020. In a Pandemic Are We More Religious? Traditional Practices of Catholics and the COVID-19 in Southwestern Colombia. International Journal of Latin American Religions 2020: 1–17. [Google Scholar] [CrossRef]
- Nguyen, Hoang C., Minh H. Nguyen, Binh N. Do, Cuong Q. Tran, Thao T. P. Nguyen, Khue M. Pham, Linh V. Pham, Khanh V. Tran, Trang T. Duong, Tien V. Tran, and et al. 2020. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. Journal of Clinical Medicine 9: 965. [Google Scholar] [CrossRef] [Green Version]
- Nikolaidis, Aki, Diana Paksarian, Lindsay Alexander, Jacob Derosa, Julia Dunn, Dylan M. Nielson, Irene Droney, Minji Kang, Ioanna Douka, Evelyn Bromet, and et al. 2021. The Coronavirus Health and Impact Survey (CRISIS) reveals reproducible correlates of pandemic-related mood states across the Atlantic. Scientific Reports 11: 8139. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhanunni, Anita, and Tyrone Pretorius. 2021. The Loneliness–Life Satisfaction Relationship: The Paralleland Serial Mediating Role of Hopelessness, Depression and Ego-Resilience among Young Adults in South Africa during COVID-19. International Journal of Environmental Research and Public Health 8: 3613. [Google Scholar] [CrossRef] [PubMed]
- Palgi, Yuval, Amit Shrira, Lia Ring, Ehud Bodner, Sharon Avidor, Yoav Bergman, Sara Cohen-Fridel, Shoshi Keisari, and Yaakov Hoffman. 2020. The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. Journal of Affective Disorders 275: 109–11. [Google Scholar] [CrossRef] [PubMed]
- Pan, Jen Der Peter, Ching-Yieh Lee, Shih-Hua Chang, and Jye-Ru Karen Jiang. 2012. Using prayer and scripture in a Christian-based stress-coping support group for church attendances: Implications for professionals. Journal of Pastoral Care and Counseling 66: 4. [Google Scholar] [PubMed]
- Pargament, Kenneth I. 1999. The psychology of religion and spirituality? Yes and no. International Journal for the Psychology of Religion 9: 3–16. [Google Scholar] [CrossRef]
- Pargament, Kenneth I. 2001. The Psychology of Religion and Coping: Theory, Research, Practice. New York: Guilford Press. First published in 1997. [Google Scholar]
- Pierce, Matthias, Holly Hope, Tamsin Ford, Stephani Hatch, Matthew Hotopf, Ann John, Evangelos Kontopantelis, Roger Webb, Simon Wessely, Sally McManus, and et al. 2020. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. The Lancet Psychiatry 7: 883–92. [Google Scholar] [CrossRef]
- Poloma, Margaret M., and Brian F. Pendleton. 1989. Exploring types of prayer and quality of life: A research note. Review of Religious Research 31: 46–53. [Google Scholar] [CrossRef]
- Poloma, Margaret M., and Brian F. Pendleton. 1991. The effects of prayer and prayer experiences on measures of general well-being. Journal of Psychology and Theology 19: 71–83. [Google Scholar] [CrossRef]
- Rezaei, Mahboubeh, Mohsen Adib-Hajbaghery, Naima Seyedfatemi, and Fatemeh Hoseini. 2008. Prayer in Iranian cancer patients undergoing chemotherapy. Complementary Therapies in Clinical Practice 14: 90–97. [Google Scholar] [CrossRef]
- Sadeghimoghaddam, Soudabeh, Mousa Alavi, Tayebeh Mehrabi, and AmirHosein Bankpoor-fard. 2019. The Effect of Two Methods of Relaxation and Prayer Therapy on Anxiety and Hope in Patients with Coronary Artery Disease: A Quasi-Experimental Study. Iranian Journal of Nursing and Midwifery Research 24: 102–7. [Google Scholar] [CrossRef]
- Salari, Nader, Amin Hosseinian-Far, Rostam Jalali, Aliakbar Vaisi-Raygani, Shna Rasoulpoor, Masoud Mohammadi, Shabnam Rasoulpoor, and Behnam Khaledi-Paveh. 2020. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Global Health 16: 57. [Google Scholar] [CrossRef] [PubMed]
- Sinding Bentzen, Jeanet. 2019. Acts of God? Religiosity and Natural Disasters across Subnational World Districts. The Economic Journal 129: 2295–321. [Google Scholar] [CrossRef]
- Sood, Sadhika. 2020. Psychological effects of the coronavirus disease-2019 pandemic. Research and Humanities in Medical Education 7: 23–26. Available online: https://www.rhime.in/ojs/index.php/rhime/article/view/264 (accessed on 16 July 2021).
- Spilka, Bernard, and Kevin L. Ladd. 2013. The Psychology of Prayer: A Scientific Approach. New York: Guilford Press. [Google Scholar]
- Szałachowski, Roman, and Wioletta Tuszyńska-Bogucka. 2021. “Dies Irae?” The Role of Religiosity in Dealing with Psychological Problems Caused by the COVID-19 Pandemic—Studies on a Polish Sample. Religions 12: 267. [Google Scholar] [CrossRef]
- Szram, Mariusz. 2012. Koncepcja modlitwy integralnej według Orygenesa [The concept of integral prayer according to Origen]. Verbum Vitae 22: 185–201. [Google Scholar]
- Taylor, Robert Joseph, Linda Marie Chatters, and Jeff Levin. 2004. Religion in the Lives of African Americans: Social, Psychological, and Health Perspectives. London: SAGE Publishing. [Google Scholar]
- Tolmie, Francois, and Rian Venter. 2021. Making sense of the COVID-19 pandemic from the Bible—Some perspectives. HTS Teologiese Studies/Theological Studies 77: a6493. [Google Scholar] [CrossRef]
- Torales, Julio, Marcelo O’Higgins, João Mauricio Castaldelli-Maia, and Antonio Ventriglio. 2020. The outbreak of COVID-19 coronavirus and its impact on global mental health. The International Journal of Social Psychiatry 66: 317–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuszyńska-Bogucka, Wioletta. 2020. “Rodzina covidowa”? Zagrożenia i zadania rodzinne w czasie epidemii COVID-19 ["The covid family"? Threats and family tasks during the COVID-19 epidemic]. In Medycyna spersonalizowana [Personalised Medicine]. Edited by Anna Bogucka-Kocka and Janusz Kocki. Lublin: Polihymnia, pp. 31–41. [Google Scholar]
- Vergote, Antoine. 2021. Modlitwa i psychologia. [Psychology and Prayer]. Available online: https://opoka.org.pl/biblioteka/T/TS/modlitwa_i_psychologia.html (accessed on 10 June 2021).
- Walecka, Irena, Piotr Ciechanowicz, Klaudia Dopytalska, Agata Mikucka-Wituszyńska, Elżbieta Szymańska, Jacek Bogucki, Janusz Kock, Karolina Kułakowska, and Wioletta Tuszyńska-Bogucka. 2021. Psychological consequences of hospital isolation during the COVID-19 pandemic—research on the sample of polish firefighting academy students. Current Psychology 2021: 1–10. [Google Scholar] [CrossRef]
- Werbiński, Ireneusz. 2010. Modlitwa—dialog człowieka z Bogiem [Prayer—man’s dialogue with God]. Paedagogia Christiana 2: 135–47. [Google Scholar] [CrossRef]
- Wildman, Wesley J., Bulbulia Joseph, Sosis Richard, and Schjoedt Uffe. 2020. Religion and the COVID-19 pandemic. Religion, Brain and Behavior 10: 115–17. [Google Scholar] [CrossRef] [Green Version]
- Woroniecki, Jacek. 2018. Pełnia modlitwy [The Fullness of Prayer]. Warszawa: deReggio. [Google Scholar]
- Zarzycka, Beata. 2007. Skala Centralności Religijności Stefana Hubera [The Polish Version of S. Huber’s Centrality of Religiosity Scale]. Roczniki Psychologiczne 10: 133–57. [Google Scholar]
- Zarzycka, Beata. 2011. Polska adaptacja Skali Centralności Religijności S. Hubera. In Psychologiczny pomiar religijności [The Polish Version of S. Huber’s Centrality of Religiosity Scale]. Edited by M. Jarosz. Lublin: Wydawnictwo KUL. [Google Scholar]
- Zarzycka, Beata, Rafał P. Bartczuk, and Radosław Rybarski. 2020. Centrality of Religiosity Scale in Polish Research: A Curvilinear Mechanism that Explains the Categories of Centrality of Religiosity. Religions 11: 64. [Google Scholar] [CrossRef] [Green Version]
Chart 1.
Average intensity of fears in the assessed group.


{kind=link}
Table 1.
Sociodemographic data differences between females and males by Pearson’s Chi-square test.
| Females | Males | p | Females | Males | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | % | n | % | ||||
| Place of residence | 0.657 | Marital status | 0.165 | ||||||||
| village | 21 | 11.9 | 14 | 16.7 | single | 90 | 51.1 | 33 | 39.3 | ||
| town of up to 25,000 thousand | 18 | 10.2 | 8 | 9.5 | married | 77 | 43.8 | 44 | 52.4 | ||
| small town of 25–50 thousand | 14 | 8 | 8 | 9.5 | divorced | 9 | 5.1 | 6 | 7.1 | ||
| average city of 50–300 thousand | 29 | 16.5 | 9 | 10.7 | separated | - | - | - | - | ||
| large city of more than 300 thousand | 84 | 53.4 | 45 | 53.6 | widowed | - | - | 1 | 0.4 | ||
| Education | 0.506 | Having children | 0.162 | ||||||||
| primary education | 2 | 1.1 | 2 | 2.4 | yes no | 78 98 | 44.3 55.7 | 45 39 | 53.6 46.4 | ||
| secondary education | 19 | 10.8 | 15 | 17.9 | |||||||
| secondary education and studying | 39 | 22.2 | 16 | 19 | |||||||
| higher education | 91 | 51.7 | 39 | 46.4 | |||||||
| higher education and studying | 25 | 14.2 | 12 | 14.3 | |||||||
| Assessment of material status | 0.511 | Assessment of health status | 0.843 | ||||||||
| very poor | 1 | 0.6 | 1 | 1.2 | very poor | 1 | 0.6 | - | - | ||
| poor | 7 | 4 | 4 | 4.8 | poor | 8 | 4.5 | 5 | 6 | ||
| average | 66 | 37.5 | 23 | 27.4 | average | 27 | 15.3 | 14 | 16.7 | ||
| good | 77 | 43.8 | 45 | 53.6 | good | 94 | 53.4 | 40 | 47.6 | ||
| very good | 25 | 14.2 | 11 | 13.1 | very good | 46 | 26.1 | 25 | 29.8 | ||
Table 2.
Descriptive statistics and the significance of differences in the intensity of studied variables in men and women (df = 158).
Table 2.
Descriptive statistics and the significance of differences in the intensity of studied variables in men and women (df = 158).
| Sex | M | SD | SEM | U | p | M | SD | SEM | U | p | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intellect | W | 176 | 9.35 | 4.01 | 6823.5 | n.s. | Fear for health | 4.23 | 2.49 | 0.18 | 7211.5 | n.s. |
| M | 84 | 8.86 | 3.97 | 4.01 | 2.11 | 0.23 | ||||||
| Ideology | W | 12.15 | 3.86 | 0.29 | 6592.5 | n.s. | Fear for economy/finances | 5.25 | 2.68 | 0.20 | 6373.0 | n.s. |
| M | 11.05 | 4.68 | 0.51 | 5.91 | 2.72 | 0.29 | ||||||
| Private Practice | W | 10.49 | 4.42 | 0.33 | 7155.0 | n.s. | Fear for social life | 4.20 | 2.50 | 0.18 | 6528.5 | n.s. |
| M | 10.12 | 4.79 | 0.52 | 4.73 | 2.65 | 0.28 | ||||||
| Religious Experience | W | 9.60 | 4.68 | 0.35 | 7383.5 | n.s. | Fear for family relations | 3.77 | 2.59 | 0.19 | 6527.0 | n.s. |
| M | 9.49 | 4.89 | 0.53 | 4.23 | 2.50 | 0.27 | ||||||
| Public Practice | W | 9.42 | 3.94 | 0.29 | 7173.0 | n.s. | Fears (general) | 17.46 | 6.62 | 0.49 | 6524.0 | n.s. |
| M | 9.64 | 4.11 | 0.44 | 18.90 | 6.98 | 0.76 | ||||||
| Centrality of religiosity | W | 51.02 | 19.04 | 1.43 | 6984.5 | n.s. | ||||||
Table 3.
Correlates of increased COVID-19 fears during the pandemic as measured by responses expressing level of fear from 1 to 10.
Table 3.
Correlates of increased COVID-19 fears during the pandemic as measured by responses expressing level of fear from 1 to 10.
| Fear for Health | Fear for Economy/Finances | Fear for Social Life | Fear for Family Relations | COVID-19 Fear (General) | |
|---|---|---|---|---|---|
| Intellect | −0.075 | 0.026 | −0.409 ** | −0.385 ** | −0.317 ** |
| Ideology | −0.040 | 0.074 | −0.381 ** | −0.399 ** | −0.280 ** |
| Private Practice | −0.076 | 0.052 | −0.474 ** | −0.459 ** | −0.360 ** |
| Religious Experience | −0.072 | 0.024 | −0.421 ** | −0.392 ** | −0.324 ** |
| Public Practice | −0.089 | 0.001 | −0.470 ** | −0.393 ** | −0.358 ** |
| Centrality of religiosity | −0.077 | 0.039 | −0.474 ** | −0.446 ** | −0.361 ** |
Legend: ** p < 0.01.
Table 4.
Summary of a multiple regression analysis predicting level of COVID-19 fear (general).
| B | SE B | Beta | t | p | CI 95% B | ||
|---|---|---|---|---|---|---|---|
| Min | Max | ||||||
| Intellect | −0.064 | 0.195 | −0.038 | −0.328 | n.s. | −0.449 | 0.321 |
| Ideology | 0.119 | 0.165 | 0.073 | 0.723 | n.s. | −0.205 | 0.443 |
| Private Practice | −0.324 | 0.227 | −0.217 | −1.428 | n.s. | −0.770 | 0.123 |
| Religious Experience | 0.002 | 0.192 | 0.001 | 0.010 | n.s. | −0.377 | 0.381 |
| Public Practice | −0.361 | 0.170 | −0.213 | −2.127 | 0.034 | −0.696 | −0.027 |
| Constants | 23.882 | 1.235 | 19.339 | 0.000 | 21.450 | 26.314 | |
| R = 0.381; R2 = 0.145; Corr. R2 = 0.128; F(5,254) = 8.650; p < 0.00000; SEE: 6.314 | |||||||
Table 5.
Summary of a multiple regression analysis predicting level of types of COVID-19 fears.
| B | SE B | Beta | t | p | CI 95% B | ||
|---|---|---|---|---|---|---|---|
| Min | Max | ||||||
| A. Fear for health | |||||||
| Intellect | −0.022 | −0.002 | 0.080 | 0.760 | n.s. | 0.144 | 0.124 |
| Ideology | 0.050 | −0.001 | 0.057 | 0.382 | n.s. | 0.160 | 0.173 |
| Private Practice | −0.010 | −0.003 | 0.083 | 0.891 | n.s. | 0.142 | 0.159 |
| Religious Experience | −0.010 | 0.004 | 0.074 | 0.893 | n.s. | 0.148 | 0.069 |
| Public Practice | −0.058 | 0.001 | 0.061 | 0.345 | n.s. | 0.072 | 0.133 |
| Constants | 4.526 | 0.014 | 0.422 | 0.001 | n.s. | 5.391 | 5.446 |
| R = 0.103; R2 = 0.011; Corr.R2 = -; F(5,254) = 0.554; p < 0.734; SEE: 2.387 | |||||||
| B. Fear for economy/finances | |||||||
| Intellect | −0.027 | 0.084 | −0.040 | −0.322 | n.s. | −0.192 | 0.138 |
| Ideology | 0.097 | 0.071 | 0.149 | 1.368 | n.s. | −0.043 | 0.236 |
| Private Practice | 0.101 | 0.097 | 0.170 | 1.039 | n.s. | −0.091 | 0.293 |
| Religious Experience | −0.060 | 0.083 | −0.105 | −0.723 | n.s. | −0.223 | 0.103 |
| Public Practice | −0.093 | 0.073 | −0.137 | −1.276 | n.s. | −0.237 | 0.051 |
| Constants | 4.978 | 0.531 | 9.375 | 0.000 | 3.932 | 6.024 | |
| R = 0.127; R2 = 0.016; Corr.R2 = -; F(5,254) = 0.834; p < 0.526; SEE: 2.714 | |||||||
| C. Fear for social life | |||||||
| Intellect | −0.013 | 0.069 | −0.021 | −0.192 | n.s. | −0.150 | 0.123 |
| Ideology | 0.033 | 0.058 | 0.053 | 0.560 | n.s. | −0.082 | 0.148 |
| Private Practice | −0.176 | 0.080 | −0.313 | −2.193 | 0.029 | −0.335 | −0.018 |
| Religious Experience | 0.016 | 0.068 | 0.030 | 0.237 | n.s. | −0.118 | 0.151 |
| Public Practice | −0.171 | 0.060 | −0.267 | −2.844 | 0.005 | −0.290 | −0.053 |
| Constants | 7.415 | 0.438 | 16.917 | 0.000 | 6.551 | 8.278 | |
| R = 0.499; R2 = 0.249; Corr.R2 = 0.234; F(5,254) = 16,866; p < 0.00000; SEE: 2.241 | |||||||
| D. Fear for family relations | |||||||
| Intellect | −0.002 | 0.071 | −0.003 | −0.028 | n.s. | −0.142 | 0.138 |
| Ideology | −0.060 | 0.060 | −0.098 | −1.008 | n.s. | −0.178 | 0.058 |
| Private Practice | −0.238 | 0.082 | −0.421 | −2.890 | 0.004 | −0.401 | −0.076 |
| Religious Experience | 0.055 | 0.070 | 0.102 | 0.790 | n.s. | −0.083 | 0.193 |
| Public Practice | −0.039 | 0.062 | −0.060 | −0.625 | n.s. | −0.160 | 0.083 |
| Constants | 6.964 | 0.449 | 15.493 | 0.000 | 6.078 | 7.849 | |
| R = 0.465; R2 = 0.216; Corr. R2 = 0.201; F(5,254) = 14.051; p < 0.00000; SSE: 2.298 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Szałachowski, R.R.; Tuszyńska-Bogucka, W. “Yes, in Crisis We Pray”. The Role of Prayer in Coping with Pandemic Fears. Religions 2021, 12, 824. https://doi.org/10.3390/rel12100824
AMA Style
Szałachowski RR, Tuszyńska-Bogucka W. “Yes, in Crisis We Pray”. The Role of Prayer in Coping with Pandemic Fears. Religions. 2021; 12(10):824. https://doi.org/10.3390/rel12100824
Chicago/Turabian StyleSzałachowski, Roman Ryszard, and Wioletta Tuszyńska-Bogucka. 2021. "“Yes, in Crisis We Pray”. The Role of Prayer in Coping with Pandemic Fears" Religions 12, no. 10: 824. https://doi.org/10.3390/rel12100824
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.