
COVID-19 Vaccine Hesitancy in the LGBTQ+ Population: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
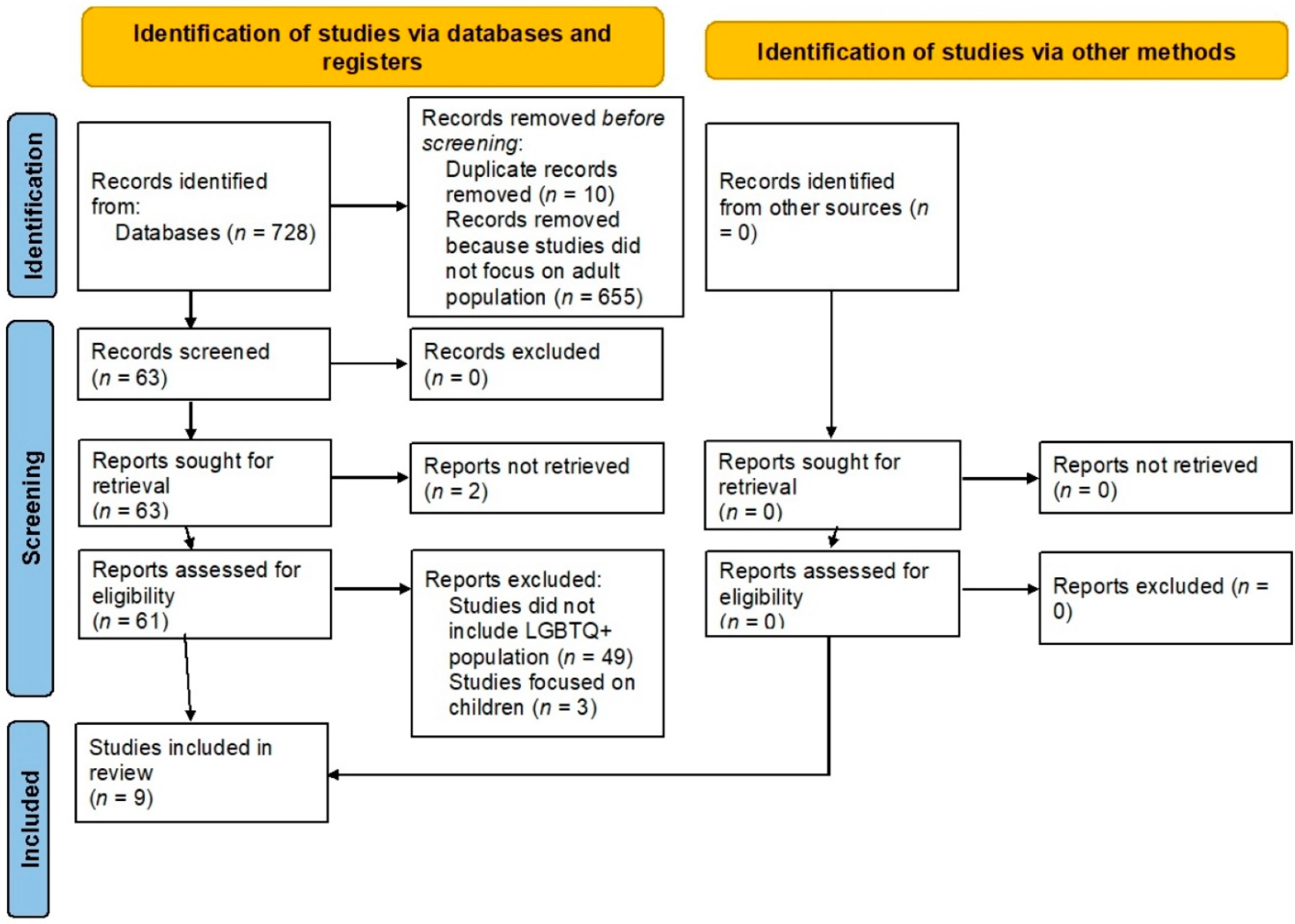
2. Methods
3. Results
4. Discussion
4.1. COVID-19 in the LGBTQ+ Population
4.2. COVID-19 Vaccines and Vaccine Hesitancy
5. Factors Influencing Vaccine Hesitancy
5.1. Environmental Factors (Health Policies, Social Factors, and Mass Media)
5.2. Agent-Related Factors (Vaccine and Disease)
5.3. Host-Related Factors (Personal Views)
6. Vaccine Hesitancy Studies in the LGBTQ+ Population
7. Strategies to Address Vaccine Hesitancy in the LGBTQ+ Population
7.1. Access to COVID-19 Vaccination
7.2. Building Trust and Addressing Misinformation
7.3. Behavior Modifiers
7.4. Patient-Centered Care
7.5. Data Collection
7.6. Public Health and Vaccine Policies
8. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, J.; Normile, D. New SARS-like virus in China triggers alarm. Science 2020, 367, 234–235. [Google Scholar] [CrossRef]
- World Health Organization. Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Available online: http://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 31 August 2021).
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-20202020 (accessed on 31 August 2021).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 31 August 2021).
- The Washington Post. History’s Deadliest Pandemics, from Ancient Rome to Modern America. Available online: https://www.washingtonpost.com/graphics/2020/local/retropolis/coronavirus-deadliest-pandemics/ (accessed on 31 August 2021).
- Ruprecht, M.M.; Wang, X.; Johnson, A.K.; Xu, J.; Felt, D.; Ihenacho, S.; Stonehouse, P.; Curry, C.W.; DeBroux, C.; Costa, D.; et al. Evidence of Social and Structural COVID-19 Disparities by Sexual Orientation, Gender Identity, and Race/Ethnicity in an Urban Environment. J. Urban Health 2021, 98, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Peek, M.E.; Lopez, F.Y.; Williams, H.S.; Xu, L.J.; McNulty, M.C.; Acree, M.E.; Schneider, J.A. Development of a Conceptual Framework for Understanding Shared Decision making Among African-American LGBT Patients and their Clinicians. J. Gen. Intern. Med. 2016, 31, 677–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Teixeira da Silva, D.; Biello, K.; Lin, W.Y.; Valente, P.K.; Mayer, K.H.; Hightow-Weidman, L.; Bauermeister, J.A. COVID-19 Vaccine Acceptance among an Online Sample of Sexual and Gender Minority Men and Transgender Women. Vaccines 2021, 9, 204. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Kuter, B.J.; Browne, S.; Momplaisir, F.M.; Feemster, K.A.; Shen, A.K.; Green-McKenzie, J.; Faig, W.; Offit, P.A. Perspectives on the receipt of a COVID-19 vaccine: A survey of employees in two large hospitals in Philadelphia. Vaccine 2021, 39, 1693–1700. [Google Scholar] [CrossRef]
- Lin, Y.-J.; Chang, Y.-P.; Chou, W.-J.; Yen, C.-F. Explicit and Intrinsic Intention to Receive COVID-19 Vaccination among Heterosexuals and Sexual Minorities in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 7260. [Google Scholar] [CrossRef]
- Tegan and Sara Foundation. COVID-19 Vaccination and the LGBTQ+ Community. Available online: https://static1.squarespace.com/static/582601b4440243fc471a91d0/t/60c76c654a25e73bb1fc850d/1623682153103/It%27s+For+US-+COVID-19+Vaccination+and+the+LGBTQ%2B+Community.pdf (accessed on 31 August 2021).
- Bradbury-Sullivan LGBT Community Center. COVID-19 Vaccination Hesitancy and Impact Among LGBTQ+ Pennsylvanians. Available online: http://www.pa-interbranchcommission.com/_pdfs/Report-Statewide-LGBTQ-COVID-19-Survey-Results.pdf (accessed on 31 August 2021).
- Human Rights Campaign. The Lives and Livelihoods of Many in the LGBTQ Community Are at Risk Amidst COVID-19 Crisis. Available online: https://www.hrc.org/resources/the-lives-and-livelihoods-of-many-in-the-lgbtq-community-are-at-risk-amidst-covid-19-crisis (accessed on 31 August 2021).
- Movement Advancement Project. The Disproportionate Impacts of COVID-19 on LGBTQ. Households in the US: Results from a July/August 2020 National Poll. Available online: https://www.lgbtmap.org/file/2020-covid-lgbtq-households-report.pdf (accessed on 31 August 2021).
- Moore, S.E.; Wierenga, K.L.; Prince, D.M.; Gillani, B.; Mintz, L.J. Disproportionate Impact of the COVID-19 Pandemic on Perceived Social Support, Mental Health and Somatic Symptoms in Sexual and Gender Minority Populations. J. Homosex. 2021, 68, 577–591. [Google Scholar] [CrossRef]
- Abbas, M.; García, J.J. Comorbid Cardiovascular Diseases and HIV in LGBTQ PoC. In Heart, Brain and Mental Health Disparities for LGBTQ People of Color; Springer: New York, NY, USA, 2021; pp. 69–78. [Google Scholar]
- Cantor, A. LGBTQ Competent Obesity Prevention and Management. Lynchburg J. Med. Sci. 2021, 3, 20. [Google Scholar]
- Phillips Ii, G.; Felt, D.; Ruprecht, M.M.; Wang, X.; Xu, J.; Pérez-Bill, E.; Bagnarol, R.M.; Roth, J.; Curry, C.W.; Beach, L.B. Addressing the Disproportionate Impacts of the COVID-19 Pandemic on Sexual and Gender Minority Populations in the United States: Actions Toward Equity. LGBT Health 2020, 7, 279–282. [Google Scholar] [CrossRef]
- Rao, A.; Rucinski, K.; Ackerman, B.; Wallach, S.; Garner, A.; Santos, G.M.; Howell, S.; Beyrer, C.; Baral, S. Global interruptions in HIV prevention and treatment services as a result of the response to COVID-19: Results from a social media-based sample of men who have sex with men. J. Int. Aids Soc. 2020, 23, 181. [Google Scholar]
- Krakower, D.; Solleveld, P.; Levine, K.; Mayer, K. Impact of COVID-19 on HIV pre-exposure prophylaxis care at a Boston community health center. J. Int. Aids Soc. 2020, 23, 176–177. [Google Scholar]
- Herman, J.L.; O’Neill, K.K. Vulnerabilities to COVID-19 among Transgender Adults in the US. Available online: https://williamsinstitute.law.ucla.edu/publications/transgender-covid-19-risk/ (accessed on 31 August 2021).
- Gil, R.M.; Freeman, T.; Mathew, T.; Kullar, R.; Ovalle, A.; Nguyen, D.; Kottkamp, A.; Poon, J.; Marcelin, J.; Swartz, T.H. The LGBTQ+ communities and the COVID-19 pandemic: A call to break the cycle of structural barriers. J. Infect. Dis. 2021, jiab392. [Google Scholar] [CrossRef] [PubMed]
- True Colors United & National Homelessness Law Center. State Index on Youth Homelessness. Available online: http://nlchp.org/wp-content/uploads/2020/02/2019-State-Index.pdf (accessed on 31 August 2021).
- Center for Primary Care Harvard Medical School. LGBTQ Youth Face Unique Challenges Amidst COVID-19. Available online: http://info.primarycare.hms.harvard.edu/review/lgbtq-youth-challenges-covid-19 (accessed on 31 August 2021).
- World Health Organization. WHO Validates Sinovac COVID-19 Vaccine for Emergency Use and Issues Interim Policy Recommendations. Available online: https://www.who.int/news/item/01-06-2021-who-validates-sinovac-covid-19-vaccine-for-emergency-use-and-issues-interim-policy-recommendations (accessed on 31 August 2021).
- World Health Organization. Coronavirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-(covid-19)-vaccines?topicsurvey=v8kj13)&gclid=EAIaIQobChMIrf75nMzb8gIVWXxvBB25MglhEAAYASAAEgI9C_D_BwE (accessed on 31 August 2021).
- Centers for Disease Control and Prevention. COVID-19 Vaccines. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html (accessed on 31 August 2021).
- US Food & Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 31 August 2021).
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Billah, M.A.; Miah, M.M.; Khan, M.N. Reproductive number of coronavirus: A systematic review and meta-analysis based on global level evidence. PLoS ONE 2020, 15, e0242128. [Google Scholar] [CrossRef] [PubMed]
- Britton, T.; Ball, F.; Trapman, P. A mathematical model reveals the influence of population heterogeneity on herd immunity to SARS-CoV-2. Science 2020, 369, 846–849. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 31 August 2021).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- World Health Organization. Report Of the Sage Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 31 August 2021).
- Wiyeh, A.B.; Cooper, S.; Jaca, A.; Mavundza, E.; Ndwandwe, D.; Wiysonge, C.S. Social media and HPV vaccination: Unsolicited public comments on a Facebook post by the Western Cape Department of Health provide insights into determinants of vaccine hesitancy in South Africa. Vaccine 2019, 37, 6317–6323. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.; Betsch, C.; Sambala, E.Z.; Mchiza, N.; Wiysonge, C.S. Vaccine hesitancy—A potential threat to the achievements of vaccination programmes in Africa. Hum. Vaccines Immunother. 2018, 14, 2355–2357. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Bach Habersaat, K.; Deshevoi, S.; Heinemeier, D.; Briko, N.; Kostenko, N.; Kocik, J.; Böhm, R.; Zettler, I.; Wiysonge, C.S.; et al. Sample study protocol for adapting and translating the 5C scale to assess the psychological antecedents of vaccination. BMJ Open 2020, 10, e034869. [Google Scholar] [CrossRef] [Green Version]
- Vickers, N.J. Animal Communication: When I’m Calling You, Will You Answer Too? Curr. Biol. 2017, 27, R713–R715. [Google Scholar] [CrossRef]
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Peng, Y.; Xu, H.; Cui, Z.; Williams, R.O. The COVID-19 Vaccine Race: Challenges and Opportunities in Vaccine Formulation. AAPS PharmSciTech 2020, 21, 225. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Pecorelli, S. Assessing COVID-19 vaccine literacy: A preliminary online survey. Hum. Vaccines Immunother. 2021, 17, 1304–1312. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological Characteristics Associated with COVID-19 Vaccine Hesitancy and Resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Willingness to Receive COVID-19 Vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef]
- Williams, L.; Flowers, P.; McLeod, J.; Young, D.; Rollins, L. Social Patterning and Stability of Intention to Accept a COVID-19 Vaccine in Scotland: Will Those Most at Risk Accept a Vaccine? Vaccines 2021, 9, 17. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Head, K.J.; Kasting, M.L.; Sturm, L.A.; Hartsock, J.A.; Zimet, G.D. A National Survey Assessing SARS-CoV-2 Vaccination Intentions: Implications for Future Public Health Communication Efforts. Sci. Commun. 2020, 42, 698–723. [Google Scholar] [CrossRef]
- Mercadante, A.R.; Law, A.V. Will They, or Won’t They? Examining Patients’ Vaccine Intention for Flu and COVID-19 Using the Health Belief Model. Res. Soc. Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 Vaccine Demand and Hesitancy: A Nationwide Online Survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once We Have It, Will We Use It? A European Survey on Willingness to Be Vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for COVID-19 vaccines: A rapid systematic review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Pomares, T.D.; Buttenheim, A.M.; Amin, A.B.; Joyce, C.M.; Porter, R.M.; Bednarczyk, R.A.; Omer, S.B. Association of cognitive biases with human papillomavirus vaccine hesitancy: A cross-sectional study. Hum. Vaccines Immunother. 2020, 16, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Browne, M.; Thomson, P.; Rockloff, M.J.; Pennycook, G. Going against the Herd: Psychological and Cultural Factors Underlying the “Vaccination Confidence Gap”. PLoS ONE 2015, 10, e0132562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The Psychological Roots of Anti-Vaccination Attitudes: A 24-Nation Investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef]
- Gowda, C.; Dempsey, A.F. The Rise (and Fall?) Of Parental Vaccine Hesitancy. Hum. Vaccines Immunother. 2013, 9, 1755–1762. [Google Scholar] [CrossRef] [Green Version]
- Salmon, D.; Dudley, M.; Glanz, J.; Omer, S. Vaccine Hesitancy: Causes, Consequences, and a Call to Action. Vaccine 2015, 33, D66–D71. [Google Scholar] [CrossRef]
- Daley, M.F.; Narwaney, K.J.; Shoup, J.A.; Wagner, N.M.; Glanz, J.M. Addressing Parents’ Vaccine Concerns: A Randomized Trial of a Social Media Intervention. Am. J. Prev. Med. 2018, 55, 44–54. [Google Scholar] [CrossRef]
- Arede, M.; Bravo-Araya, M.; Bouchard, É.; Singh Gill, G.; Plajer, V.; Shehraj, A.; Shuaib, Y.A. Combating Vaccine Hesitancy: Teaching the Next Generation to Navigate Through the Post Truth Era. Front. Public Health 2018, 6, 381. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the Vaccine Confidence Gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Olson, O.; Berry, C.; Kumar, N. Addressing parental vaccine hesitancy towards childhood vaccines in the United States: A systematic literature review of communication interventions and strategies. Vaccines 2020, 8, 590. [Google Scholar] [CrossRef] [PubMed]
- Karafillakis, E.; Larson, H.J. The benefit of the doubt or doubts over benefits? A systematic literature review of perceived risks of vaccines in European populations. Vaccine 2017, 35, 4840–4850. [Google Scholar] [CrossRef] [PubMed]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1–2. [Google Scholar] [CrossRef]
- Allen, J.D.; Feng, W.; Corlin, L.; Porteny, T.; Acevedo, A.; Schildkraut, D.; King, E.; Ladin, K.; Fu, Q.; Stopka, T.J. Why are some people reluctant to be vaccinated for COVID-19? A cross-sectional survey among U.S. Adults in May–June 2020. Prev. Med. Rep. 2021, 24, 101494. [Google Scholar] [CrossRef]
- Arvanitis, M.; Opsasnick, L.; O’Conor, R.; Curtis, L.M.; Vuyyuru, C.; Yoshino Benavente, J.; Bailey, S.C.; Jean-Jacques, M.; Wolf, M.S. Factors associated with COVID-19 vaccine trust and hesitancy among adults with chronic conditions. Prev. Med. Rep. 2021, 24, 101484. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef]
- Pelčić, G.; Karačić, S.; Mikirtichan, G.L.; Kubar, O.I.; Leavitt, F.J.; Cheng-Tek Tai, M.; Morishita, N.; Vuletić, S.; Tomašević, L. Religious exception for vaccination or religious excuses for avoiding vaccination. Croat. Med. J. 2016, 57, 516–521. [Google Scholar] [CrossRef] [Green Version]
- Wielders, C.C.; van Binnendijk, R.S.; Snijders, B.E.; Tipples, G.A.; Cremer, J.; Fanoy, E.; Dolman, S.; Ruijs, W.; Boot, H.J.; de Melker, H.E.; et al. Mumps epidemic in orthodox religious low-vaccination communities in the Netherlands and Canada, 2007 to 2009. Eurosurveillance 2011, 16, 19989. [Google Scholar] [CrossRef]
- Nature. Test Behavioural Nudges to Boost COVID Immunization. Available online: https://www.nature.com/articles/d41586-021-00329-z (accessed on 31 August 2021).
- Wolfe, R.M.; Sharp, L.K.; Lipsky, M.S. Content and design attributes of anti-vaccination web sites. JAMA 2002, 287, 3245–3248. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, R.K.; Wolfe, R.M.; Fox, D.E.; Fox, J.R.; Nowalk, M.P.; Troy, J.A.; Sharp, L.K. Vaccine Criticism on the World Wide Web. J. Med. Internet Res. 2005, 7, e17. [Google Scholar] [CrossRef] [Green Version]
- Harmsen, I.A.; Mollema, L.; Ruiter, R.A.C.; Paulussen, T.G.W.; de Melker, H.E.; Kok, G. Why Parents Refuse Childhood Vaccination: A Qualitative Study Using Online Focus Groups. BMC Public Health 2013, 13, 1183. [Google Scholar] [CrossRef] [Green Version]
- Davies, P.; Chapman, S.; Leask, J. Antivaccination activists on the world wide web. Arch. Dis. Child. 2002, 87, 22–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betsch, C.; Brewer, N.T.; Brocard, P.; Davies, P.; Gaissmaier, W.; Haase, N.; Leask, J.; Renkewitz, F.; Renner, B.; Reyna, V.F.; et al. Opportunities and Challenges of Web 2.0 for Vaccination Decisions. Vaccine 2012, 30, 3727–3733. [Google Scholar] [CrossRef] [Green Version]
- Munn, L. Angry by design: Toxic communication and technical architectures. Humanit. Soc. Sci. Commun. 2020, 7, 1–11. [Google Scholar] [CrossRef]
- Scullard, P.; Peacock, C.; Davies, P. Googling children’s health: Reliability of medical advice on the internet. Arch. Dis. Child. 2010, 95, 580–582. [Google Scholar] [CrossRef]
- Betsch, C.; Renkewitz, F.; Betsch, T.; Ulshöfer, C. The Influence of Vaccine-Critical Websites on Perceiving Vaccination Risks. J. Health Psychol. 2010, 15, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Vaccines and Immunizations. Available online: https://www.cdc.gov/vaccines/vac-gen/evalwebs.htm (accessed on 31 August 2021).
- Centers for Disease Control and Prevention. COVID-19 Vaccines for Moderately to Severely Immunocompromised People. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html (accessed on 31 August 2021).
- The Harvard Gazette. Turn Voting into a Celebration, Not a Chore. Available online: https://news.harvard.edu/gazette/story/2018/10/harvard-panel-shares-strategies-to-increase-voter-turnout/ (accessed on 31 August 2021).
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [Green Version]
- Iten, A.; Bonfillon, C.; Bouvard, T.; Siegrist, C.-A.; Pittet, D. P037: Nosocomial Influenza Prevention Using Multi-Modal Intervention Strategies; 20-Years of Experience. Antimicrob. Resist. Infect. Control 2013, 2, P37. [Google Scholar] [CrossRef] [Green Version]
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 4, CD001431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gay and Lesbian Medical Association. Guidelines for Care of Lesbian, Gay, Bisexual, and Transgender Patients. Available online: http://www.glma.org/_data/n_0001/resources/live/Welcoming%20Environment.pdf (accessed on 31 August 2021).
- Vanjani, R.; Martino, S.; Reiger, S.F.; Lawless, J.; Kelly, C.; Mariano, V.J.; Trimbur, M.C. Physician-Public Defender Collaboration—A New Medical-Legal Partnership. N. Engl. J. Med. 2020, 383, 2083–2086. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO/UNICEF Joint Reporting Process. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/who-unicef-joint-reporting-process (accessed on 31 August 2021).
- Cooper, S.; Okeibunor, J.C.; Wiyeh, A.; Wiysonge, C.S. Knowledge Advances and Gaps on the Demand Side of Vaccination. Lancet Infect. Dis. 2019, 19, 13–15. [Google Scholar] [CrossRef]
- Artiga, S.; Ndugga, N.; Pham, O. Immigrant Access to COVID-19 Vaccines: Key Issues to Consider. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/immigrant-access-to-covid-19-vaccines-key-issues-to-consider/ (accessed on 31 August 2021).
- Heffernan, O. Misinformation Is Harming Trust in the COVID Vaccine Among Latinos in New York. Available online: https://documentedny.com/2020/12/18/misinformation-is-harming-trust-in-the-covid-vaccine-among-latinos-in-new-york/ (accessed on 31 August 2021).
- Visram, T. How Will Undocumented Immigrants Get the COVID-19 Vaccine? Available online: https://www.fastcompany.com/90595912/how-will-undocumented-immigrants-get-the-covid-vaccine (accessed on 31 August 2021).
- Sember, R.; Gere, D. “Let the Record Show...”: Art Activism and the AIDS Epidemic. Am. J. Public Health 2006, 96, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Fox, D.M. AIDS and the American health polity: The history and prospects of a crisis of authority. Milbank Q. 1986, 64 (Suppl. 1), 7–33. [Google Scholar] [CrossRef]
- Parker, C.M.; Hirsch, J.S.; Philbin, M.M.; Parker, R.G. The Urgent Need for Research and Interventions to Address Family-Based Stigma and Discrimination Against Lesbian, Gay, Bisexual, Transgender, and Queer Youth. J. Adolesc. Health 2018, 63, 383–393. [Google Scholar] [CrossRef]
- Robert Wood Johnson Foundation. Discrimination in America. Available online: https://www.rwjf.org/en/library/research/2017/10/discrimination-in-america--experiences-and-views.html (accessed on 31 August 2021).
- Human Rights Campaign. The Economic Impact of COVID-19 on the LGBTQ Community. Available online: https://www.hrc.org/resources/the-economic-impact-of-covid-19-on-the-lgbtq-community (accessed on 31 August 2021).


{kind=link}
| Author | Year | Country | Total Population | NB Gender Present | Number of NB Participants | Overall Gender Distribution | Overall Acceptance Rate (%) | Acceptance Rate in NB Participants (%) |
|---|---|---|---|---|---|---|---|---|
| Freeman et al. [9] | 2020 | UK | 5114 | Yes | 20 | M = 2574, F = 2515 | 71.71% | - |
| Lazarus et al. [10] | 2021 | China | 712 | Yes | 0 | M = 360, F = 351 | 88.62% | - |
| Lazarus et al. [10] | 2021 | Brazil | 717 | Yes | 4 | M = 276, F = 436 | 85.36% | - |
| Lazarus et al. [10] | 2021 | Canada | 707 | Yes | 6 | M = 307, F = 392 | 68.74% | - |
| Lazarus et al. [10] | 2021 | Ecuador | 741 | Yes | 10 | M = 323, F = 407 | 71.93% | - |
| Lazarus et al. [10] | 2021 | France | 669 | Yes | 2 | M = 334, F = 333 | 58.89% | - |
| Lazarus et al. [10] | 2021 | Germany | 722 | Yes | 2 | M = 298, F = 417 | 68.42% | - |
| Lazarus et al. [10] | 2021 | India | 742 | Yes | 6 | M = 243, F = 485 | 74.53% | - |
| Lazaus et al. [10] | 2021 | Italy | 736 | Yes | 1 | M = 323, F = 412 | 70.79% | - |
| Lazarus et al. [10] | 2021 | Mexico | 699 | Yes | 2 | M = 332, F = 364 | 76.25% | - |
| Lazarus et al. [10] | 2021 | Nigeria | 670 | Yes | 22 | M = 275, F = 373 | 65.22% | - |
| Lazarus et al. [10] | 2021 | Poland | 666 | Yes | 0 | M = 362, F = 302 | 56.31% | - |
| Lazarus et al. [10] | 2021 | Russia | 680 | Yes | 6 | M = 328, F = 346 | 54.85% | - |
| Lazarus et al. [10] | 2021 | Singapore | 655 | Yes | 3 | M = 342, F = 310 | 67.94% | - |
| Lazarus et al. [10] | 2021 | South Africa | 619 | Yes | 3 | M = 321, F = 294 | 81.58% | - |
| Lazarus et al. [10] | 2021 | South Korea | 752 | Yes | 0 | M = 357, F = 392 | 79.79% | - |
| Lazarus et al. [10] | 2021 | Spain | 748 | Yes | 2 | M = 345, F = 401 | 74.33% | - |
| Lazarus et al. [10] | 2021 | Sweden | 650 | Yes | 2 | M = 322, F = 326 | 65.23% | - |
| Lazarus et al. [10] | 2021 | UK | 768 | Yes | 14 | M = 344, F = 408 | 71.48% | - |
| Lazarus et al. [10] | 2021 | USA | 773 | Yes | 9 | M = 337, F = 423 | 75.42% | - |
| Reiter et al. [11] | 2020 | USA | 2006 | Yes | 16 | M = 868, F = 1122 | 68.50% | 56.25% |
| Salali et al. [12] | 2020 | UK | 1088 | Yes | 31 | M = 322, F = 735 | 82.00% | - |
| Salali et al. [12] | 2020 | Turkey | 3936 | Yes | 18 | M = 1474, F = 2462 | 67.00% | - |
| Shekhar et al. [13] | 2020 | USA | 3479 | Yes | 7 | M = 864, F = 2598 | 36.00% | 43.00% |
| Teixeira da Silva et al. [14] | 2021 | USA | 1350 | Yes | 1262 | Not reported | Not reported; study focused on predictors of vaccine acceptance | Not reported; study focused on predictors of vaccine acceptance |
| Bendau et al. [15] | 2021 | Germany | 1779 | Yes | 10 | M = 389, F = 1380 | 64.50% | - |
| Kuter et al. [16] | 2021 | USA | 12034 | Yes | 878 | M = 5658, F = 1241 | 63.70% | 28.90% |
| Lin et al. [17] | 2021 | Taiwan | 1047 | Yes | 171 | M-430, F-617 | Sexual minority individuals had higher levels of explicit and intrinsic intention to receive COVID-19 vaccination relative to heterosexual individuals. | Not reported; multiple regression models were used |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garg, I.; Hanif, H.; Javed, N.; Abbas, R.; Mirza, S.; Javaid, M.A.; Pal, S.; Shekhar, R.; Sheikh, A.B. COVID-19 Vaccine Hesitancy in the LGBTQ+ Population: A Systematic Review. Infect. Dis. Rep. 2021, 13, 872-887. https://doi.org/10.3390/idr13040079
Garg I, Hanif H, Javed N, Abbas R, Mirza S, Javaid MA, Pal S, Shekhar R, Sheikh AB. COVID-19 Vaccine Hesitancy in the LGBTQ+ Population: A Systematic Review. Infectious Disease Reports. 2021; 13(4):872-887. https://doi.org/10.3390/idr13040079
Chicago/Turabian StyleGarg, Ishan, Hamza Hanif, Nismat Javed, Ramsha Abbas, Samir Mirza, Muhammad Ali Javaid, Suman Pal, Rahul Shekhar, and Abu Baker Sheikh. 2021. "COVID-19 Vaccine Hesitancy in the LGBTQ+ Population: A Systematic Review" Infectious Disease Reports 13, no. 4: 872-887. https://doi.org/10.3390/idr13040079