
Reduced Flow-Mediated Dilatation Is Not Related to COVID-19 Severity Three Months after Hospitalization for SARS-CoV-2 Infection
 , , and
, , and
Abstract
:1. Introduction
2. Population and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
3.1. Overall Population
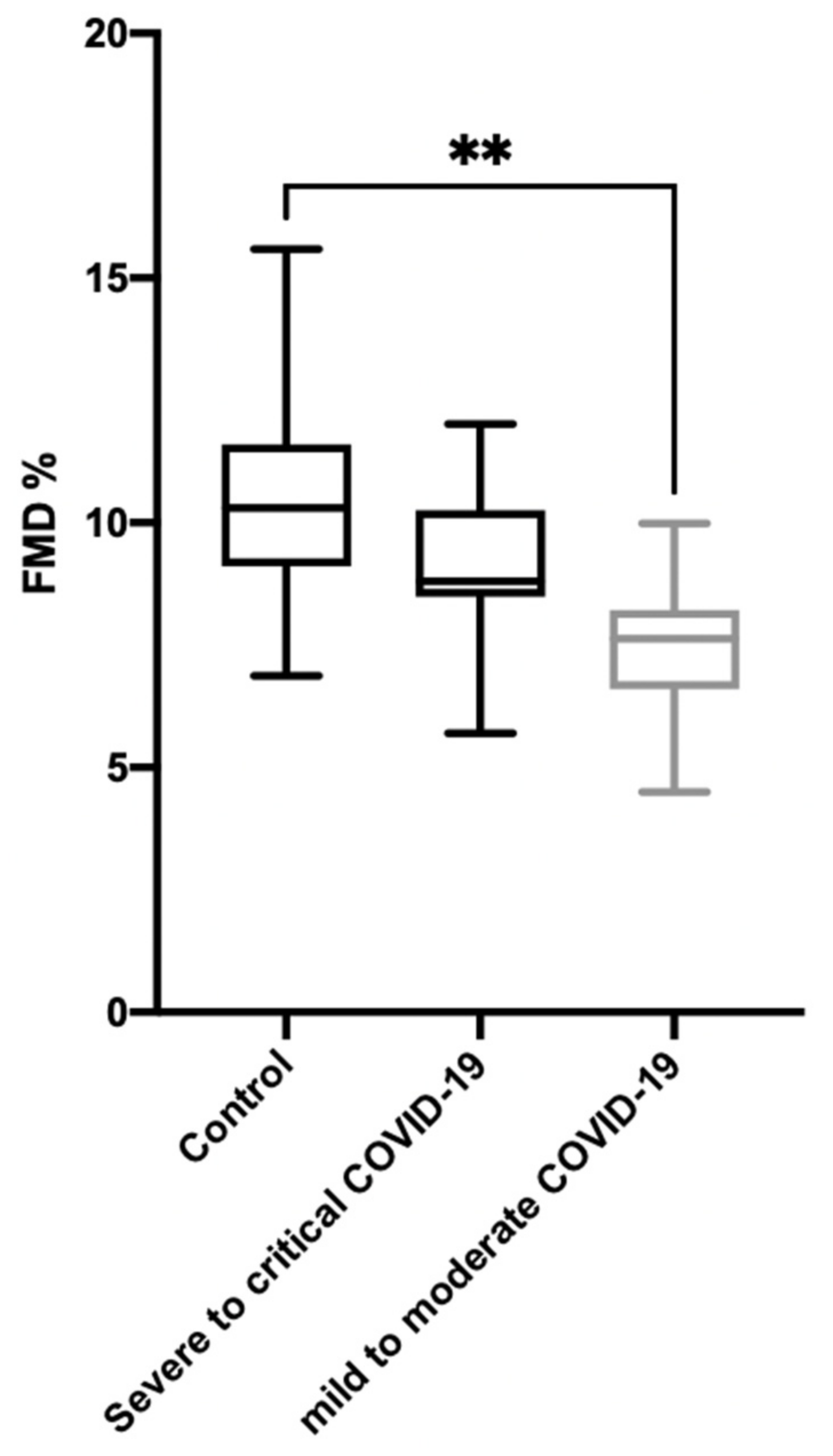
3.2. Comparison between Mild-to-Moderate and Severe or Critical Diseased Patients
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Evans, P.C.; Ed Rainger, G.; Mason, J.C.; Guzik, T.J.; Osto, E.; Stamataki, Z.; Neil, D.; Hoefer, I.E.; Fragiadaki, M.; Waltenberger, J.; et al. Endothelial Dysfunction in COVID-19: A Position Paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovasc. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert Consensus and Evidence-Based Recommendations for the Assessment of Flow-Mediated Dilation in Humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: A metaanalysis. Int. J. Cardiovasc. Imaging 2010, 26, 631–640. [Google Scholar] [CrossRef] [PubMed]
- WHO. Available online: https://www.Who.Int/Publications/i/Item/Clinical-Management-of-Covid-19 (accessed on 20 January 2021).
- Rouyer, O.; Auger, C.; Charles, A.-L.; Talha, S.; Meyer, A.; Piquard, F.; Andres, E.; Schini-Kerth, V.; Geny, B. Effects of a High Fat Meal Associated with Water, Juice, or Champagne Consumption on Endothelial Function and Markers of Oxidative Stress and Inflammation in Young, Healthy Subjects. J. Clin. Med. 2019, 8, 859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouyer, O.; Talha, S.; Di Marco, P.; Ellero, B.; Doutreleau, S.; Diemunsch, P.; Piquard, F.; Geny, B. Lack of endothelial dysfunction in patients under tacrolimus after orthotopic liver transplantation. Clin. Transplant. 2009, 23, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Gokce, N.; Keaney, J.F.J.; Hunter, L.M.; Watkins, M.T.; Nedeljkovic, Z.S.; Menzoian, J.O.; Vita, J.A. Predictive Value of Noninvasively Determined Endothelial Dysfunction for Long-Term Cardiovascular Events in Patients with Peripheral Vascular Disease. J. Am. Coll. Cardiol. 2003, 41, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Mutlu, B.; Tigen, K.; Gurel, E.; Ozben, B.; Karaahmet, T.; Basaran, Y. The Predictive Value of Flow-Mediated Dilation and Carotid Artery Intima-Media Thickness for Occult Coronary Artery Disease. Echocardiography 2011, 28, 1141–1147. [Google Scholar] [CrossRef]
- Revel, M.-P.; Parkar, A.P.; Prosch, H.; Silva, M.; Sverzellati, N.; Gleeson, F.; Brady, A. COVID-19 Patients and the Radiology Department—Advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur. Radiol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S.L. Vascular Alterations Among Young Adults with SARS-CoV-2. Am. J. Physiol. Heart Circ. Physiol. 2020. [Google Scholar] [CrossRef]
- Green, S.J. Covid-19 Accelerates Endothelial Dysfunction and Nitric Oxide Deficiency. Microbes Infect. 2020, 22, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Spiegelhalter, D.J.; Georgakopoulos, D.; Robinson, J.; Deanfield, J.E. Aging Is Associated with Endothelial Dysfunction in Healthy Men Years before the Age-Related Decline in Women. J. Am. Coll. Cardiol. 1994, 24, 471–476. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Critical COVID-19: Defined by the criteria for acute respiratory distress syndrome (ARDS), sepsis, septic shock, or other conditions that would normally require the provision of life-sustaining therapies such as mechanical ventilation (invasive or non-invasive) or vasopressor therapy. |
| Severe COVID-19: Defined by any of the following: o Oxygen saturation <90% on room air; O Respiratory rate >30 breaths/min in adults; o Signs of severe respiratory distress (accessory muscle use, inability to complete full sentences, and, in children, very severe chest wall indrawing, grunting, central cyanosis, or presence of any other general danger signs). |
| Non-severe (mild-to-moderate) COVID-19: Defined as absence of any criteria for severe or critical COVID-19. |
| Total Population (n = 27) | Mild to Moderate Disease (n = 16) | Severe to Critical Disease (n = 11) | p | |
|---|---|---|---|---|
| FMD (%) | 8.1 (7.2–8.9) | 7.6 (6.6–8.2) | 8.8 (8.5–10.2) | 0.016 |
| Clinical characteristics | ||||
| Age (years) | 57 (49–66) | 57 (51–66) | 51 (46–73) | 0.84 |
| Male (n/%) | 17/63% | 9 (56%) | 8 (73%) | 0.38 |
| BMI (Kg/m2) | 29 (26.2–34) | 29.5 (26.4–34.1) | 27.1 (25.6–32.1) | 0.33 |
| Systolic blood pressure (mmHg) | 134 (128–140) | 137 (129–153) | 132 (124–137) | 0.12 |
| Diastolic blood pressure (mmHg) | 84 (77–93) | 85 (81–98) | 78 (75–91) | 0.19 |
| Hypertension (n/%) | 13/48% | 6/37% | 7/64% | 0.18 |
| Diabetes (n/%) | 7/26% | 5/31% | 2/18% | 0.44 |
| Sleep apnea syndrome (n/%) | 6/22% | 3/19% | 3/27% | 0.60 |
| Chronic heart failure (n/%) | 0 | 0 | 0 | - |
| Former or active smokers (n/%) | 6/22% | 4/25% | 2/18% | 0.68 |
| Charlson Comorbidity Index Score | 2 (0–3) | 2 (1–3) | 2 (0–4) | 0.91 |
| Total Population (n = 27) | Mild-to-Moderate Disease (n = 16) | Severe-to-Critical Disease (n = 11) | p | |
|---|---|---|---|---|
| FMD (%) | 8.1 (7.2–8.9) | 7.6 (6.6–8.2) | 8.8 (8.5–10.2) | 0.016 |
| Hospitalization characteristics | ||||
| Total hospitalization duration (days) | 14 (8–42) | 12 (7–15) | 42 (21–53) | <0.001 |
| ICU hospitalization (Yes, n/%) | 11/41% | 0 | 11/100% | <0.001 |
| Chest CT on admission with severe/critical (>50%) abnormal lung parenchyma (Yes, n/%) | 9/33% | 0 | 8/73% | <0.001 |
| Pulmonary embolism during hospitalization | 4/15% | 0 | 4/36% | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riou, M.; Oulehri, W.; Momas, C.; Rouyer, O.; Lebourg, F.; Meyer, A.; Enache, I.; Pistea, C.; Charloux, A.; Marcot, C.; et al. Reduced Flow-Mediated Dilatation Is Not Related to COVID-19 Severity Three Months after Hospitalization for SARS-CoV-2 Infection. J. Clin. Med. 2021, 10, 1318. https://doi.org/10.3390/jcm10061318
Riou M, Oulehri W, Momas C, Rouyer O, Lebourg F, Meyer A, Enache I, Pistea C, Charloux A, Marcot C, et al. Reduced Flow-Mediated Dilatation Is Not Related to COVID-19 Severity Three Months after Hospitalization for SARS-CoV-2 Infection. Journal of Clinical Medicine. 2021; 10(6):1318. https://doi.org/10.3390/jcm10061318
Chicago/Turabian StyleRiou, Marianne, Walid Oulehri, Cedric Momas, Olivier Rouyer, Fabienne Lebourg, Alain Meyer, Irina Enache, Cristina Pistea, Anne Charloux, Christophe Marcot, and et al. 2021. "Reduced Flow-Mediated Dilatation Is Not Related to COVID-19 Severity Three Months after Hospitalization for SARS-CoV-2 Infection" Journal of Clinical Medicine 10, no. 6: 1318. https://doi.org/10.3390/jcm10061318