
Hospitalized COVID-19 Patients with Severe Acute Respiratory Syndrome: A Population-Based Registry Analysis to Assess Clinical Findings, Pharmacological Treatment and Survival

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Real-World Study Details
2.2. Variables
2.3. Statistical Analysis
3. Results
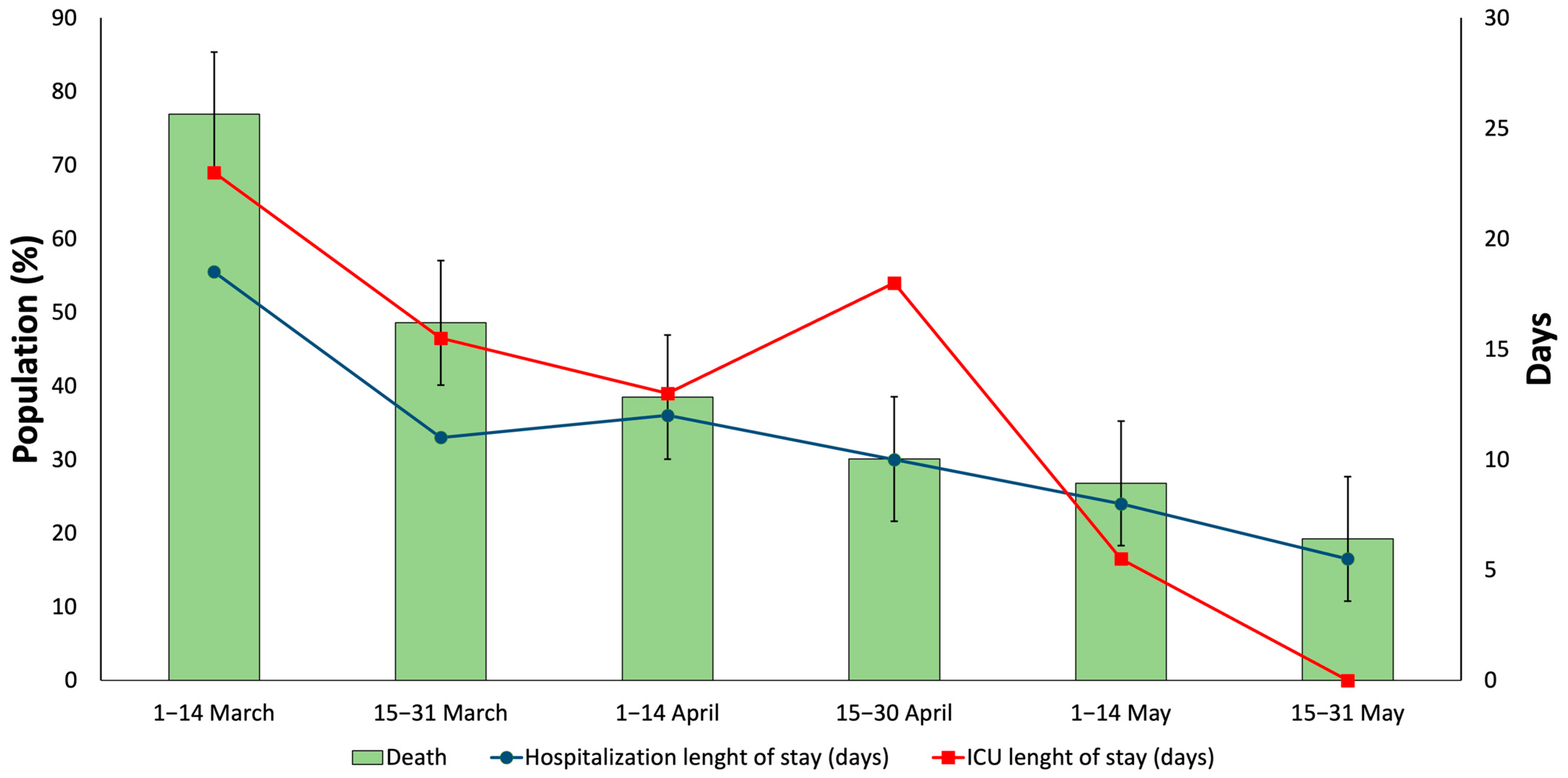
3.1. Clinical Findings
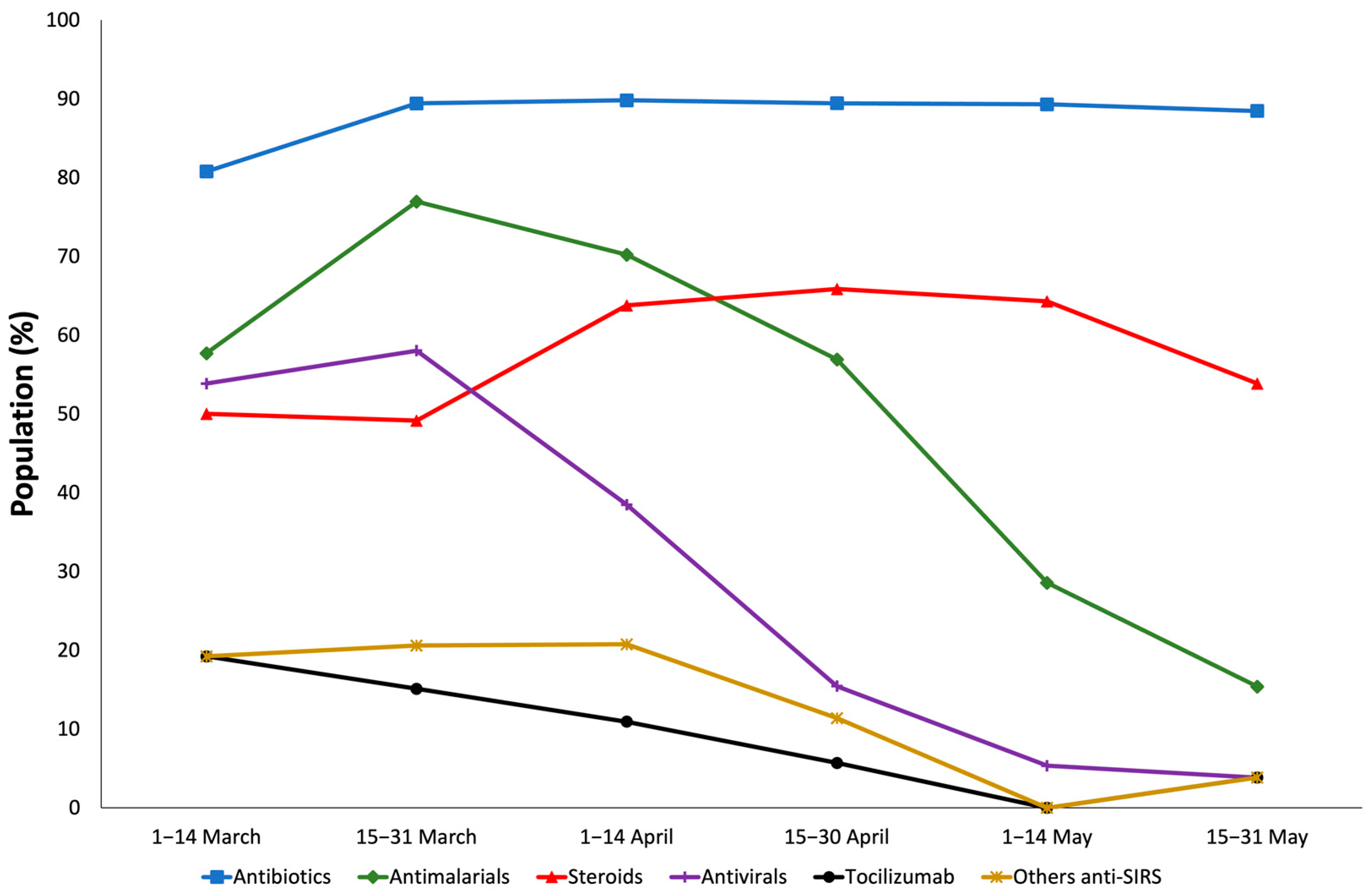
3.2. Pharmacological Treatment
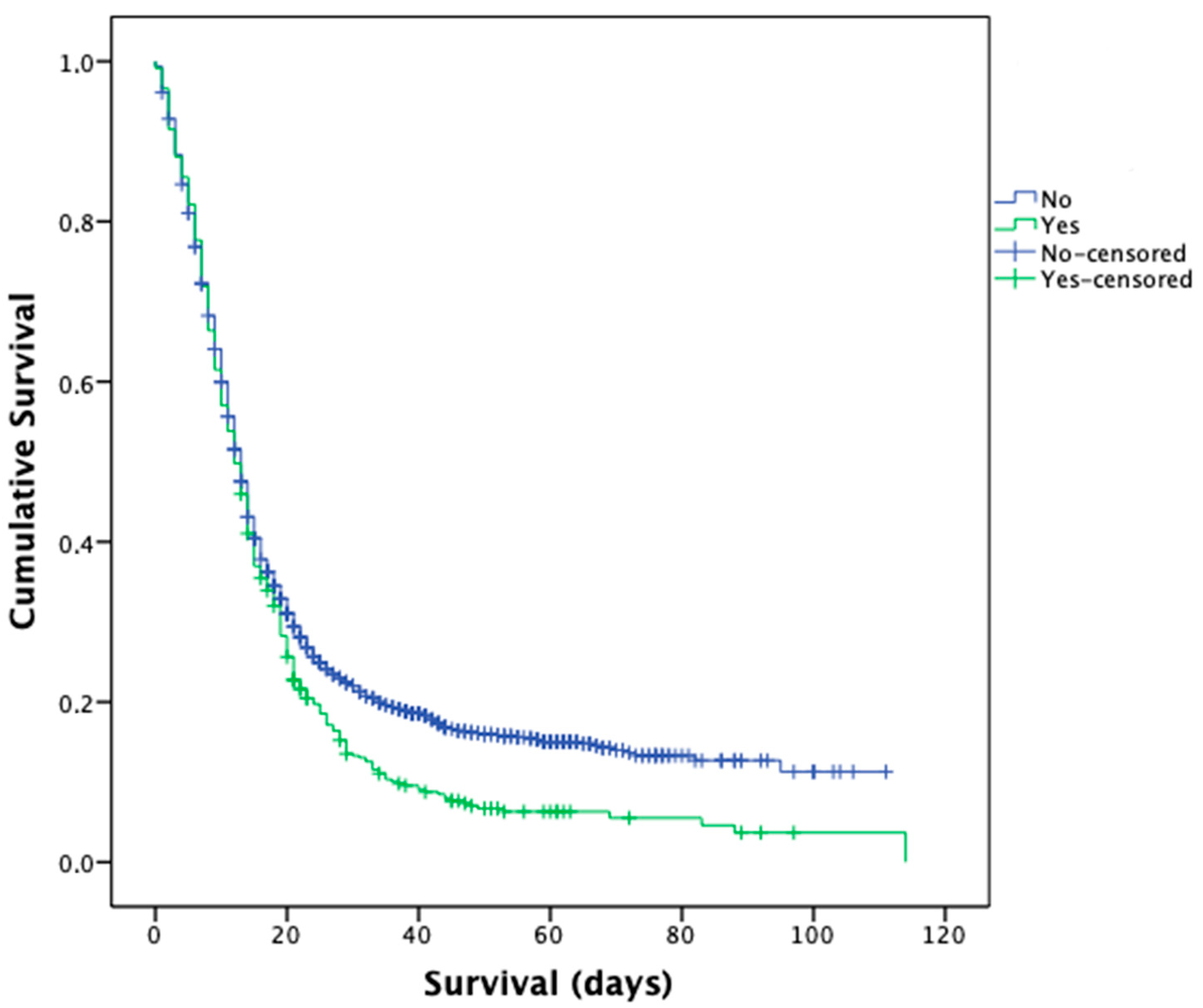
3.3. Survival and Risk Factor for Clinical Outcomes and Medication Prescribed
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berenguer, J.; Ryan, P.; Rodríguez-Baño, J.; Jarrín, I.; Carratalà, J.; Pachón, J.; Yllescas, M.; Arriba, J.R.; COVID-19@Spain Study Group; Fundación SEIMC-GESIDA; et al. Characteristics and Predictors of Death among 4035 Consecutively Hospitalized Patients with COVID-19 in Spain. Clin. Microbiol. Infect. 2020, 26, 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Casas-Rojo, J.M.; Antón-Santos, J.M.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.M.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.M.; Vargas-Núñez, J.A.; et al. Clinical Characteristics of Patients Hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clin. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Abejón, E.; Tamayo, E.; Martín-García, D.; Álvarez, F.J.; Herrera-Gómez, F. Clinical Profile, Treatment and Predictors during the First COVID-19 Wave: A Population-Based Registry Analysis from Castile and Leon Hospitals. Int. J. Environ. Res. Public. Health 2020, 17, E9360. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 Acute Respiratory Distress Syndrome (ARDS): Clinical Features and Differences from Typical Pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef] [PubMed]
- Parsons, P.E.; Eisner, M.D.; Thompson, B.T.; Matthay, M.A.; Ancukiewicz, M.; Bernard, G.R.; Wheeler, A.P.; NHLBI Acute Respiratory Distress Syndrome Clinical Trials Network. Lower Tidal Volume Ventilation and Plasma Cytokine Markers of Inflammation in Patients with Acute Lung Injury. Crit. Care Med. 2005, 33, 1–6. [Google Scholar] [CrossRef]
- Iebba, V.; Zanotta, N.; Campisciano, G.; Zerbato, V.; Di Bella, S.; Cason, C.; Luzzati, R.; Confalonieri, M.; Palamara, A.T.; Comar, M. Profiling of Oral Microbiota and Cytokines in COVID-19 Patients. Front. Microbiol. 2021, 12, 671813. [Google Scholar] [CrossRef]
- Salton, F.; Confalonieri, P.; Campisciano, G.; Cifaldi, R.; Rizzardi, C.; Generali, D.; Pozzan, R.; Tavano, S.; Bozzi, C.; Lapadula, G.; et al. Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS. J. Clin. Med. 2022, 11, 2951. [Google Scholar] [CrossRef]
- Bogoch, I.I.; Watts, A.; Thomas-Bachli, A.; Huber, C.; Kraemer, M.U.G.; Khan, K. Potential for Global Spread of a Novel Coronavirus from China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Asakura, H.; Ogawa, H. COVID-19-Associated Coagulopathy and Disseminated Intravascular Coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef]
- Tzotzos, S.J.; Fischer, B.; Fischer, H.; Zeitlinger, M. Incidence of ARDS and Outcomes in Hospitalized Patients with COVID-19: A Global Literature Survey. Crit. Care Lond. Engl. 2020, 24, 516. [Google Scholar] [CrossRef]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 Diagnosis and Management: A Comprehensive Review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Del Sole, F.; Farcomeni, A.; Loffredo, L.; Carnevale, R.; Menichelli, D.; Vicario, T.; Pignatelli, P.; Pastori, D. Features of Severe COVID-19: A Systematic Review and Meta-Analysis. Eur. J. Clin. Investig. 2020, 50, e13378. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Abejón, E.; Martín-García, D.; Tamayo, E.; Álvarez, F.J.; Herrera-Gómez, F. Clinical Profile, Pharmacological Treatment, and Predictors of Death Among Hospitalized COVID-19 Patients With Acute Kidney Injury: A Population-Based Registry Analysis. Front. Med. 2021, 8, 657977. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Abejón, E.; Herrera-Gómez, F.; Martín-García, D.; Tamayo, E.; Álvarez, F.J. A Population-Based Registry Analysis on Hospitalized COVID-19 Patients with Previous Cardiovascular Disease: Clinical Profile, Treatment, and Predictors of Death. J. Cardiovasc. Dev. Dis. 2021, 8, 167. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. RECORD Working Committee The REporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) Statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Spanish Agency for Medicine and Health Products Available Treatments for the Management of Respiratory Infection by SARS-CoV-2. Available online: https://www.aemps.gob.es/laAEMPS/docs/medicamentos-disponibles-SARS-CoV-2-22-5-2020.pdf?x57200 (accessed on 6 May 2021).
- Spanish Ministry of Health Clinical Management of COVID-19. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Protocolo_manejo_clinico_ah_COVID-19.pdf (accessed on 6 May 2021).
- Rodríguez, A.; Moreno, G.; Gómez, J.; Carbonell, R.; Picó-Plana, E.; Benavent Bofill, C.; Sánchez Parrilla, R.; Trefler, S.; Esteve Pitarch, E.; Canadell, L.; et al. Severe Infection Due to the SARS-CoV-2 Coronavirus: Experience of a Tertiary Hospital with COVID-19 Patients during the 2020 Pandemic. Med. Intensiva 2020, 44, 525–533. [Google Scholar] [CrossRef]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus Disease 2019 (COVID-19): A Literature Review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, Laboratory and Imaging Features of COVID-19: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Torres Acosta, M.A.; Singer, B.D. Pathogenesis of COVID-19-Induced ARDS: Implications for an Ageing Population. Eur. Respir. J. 2020, 56, 2002049. [Google Scholar] [CrossRef]
- Huppert, L.A.; Matthay, M.A.; Ware, L.B. Pathogenesis of Acute Respiratory Distress Syndrome. Semin. Respir. Crit. Care Med. 2019, 40, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamb, Y.N. Remdesivir: First Approval. Drugs 2020, 80, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, L.; Shen, A.; Chen, Y.; Qi, Z. Rational Use of Tocilizumab in the Treatment of Novel Coronavirus Pneumonia. Clin. Drug Investig. 2020, 40, 511–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.-C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. 2020, 27. [Google Scholar] [CrossRef]
- Guaraldi, G.; Banchelli, F.; Milic, J.; Dolci, G.; Massari, M.; Corsini, R.; Meschiari, M.; Girardis, M.; Busani, S.; Cossarizza, A.; et al. Methylprednisolone as Rescue Therapy after Tocilizumab Failure in Patients with Severe COVID-19 Pneumonia. Clin. Exp. Rheumatol. 2021, 39, 1141. [Google Scholar]
- Salton, F.; Confalonieri, P.; Meduri, G.U.; Santus, P.; Harari, S.; Scala, R.; Lanini, S.; Vertui, V.; Oggionni, T.; Caminati, A.; et al. Prolonged Low-Dose Methylprednisolone in Patients With Severe COVID-19 Pneumonia. Open Forum Infect. Dis. 2020, 7, ofaa421. [Google Scholar] [CrossRef]
- Rizk, J.G.; Kalantar-Zadeh, K.; Mehra, M.R.; Lavie, C.J.; Rizk, Y.; Forthal, D.N. Pharmaco-Immunomodulatory Therapy in COVID-19. Drugs 2020, 80, 1267–1292. [Google Scholar] [CrossRef]
- Du, R.-H.; Liang, L.-R.; Yang, C.-Q.; Wang, W.; Cao, T.-Z.; Li, M.; Guo, G.-Y.; Du, J.; Zheng, C.-L.; Zhu, Q.; et al. Predictors of Mortality for Patients with COVID-19 Pneumonia Caused by SARS-CoV-2: A Prospective Cohort Study. Eur. Respir. J. 2020, 55, 2000524. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| SARS |
|
| TOTAL | MALE | FEMALE | p | ||
|---|---|---|---|---|---|
| N | 1025 | 650 | 375 | 0.004 | |
| Age (median and IQR) | 78 (66–86) | 76 (66–85) | 81 (68–88) | 0.004 | |
| Age < 65 (95% CI) | 78.54 (76.02–81.05) | 77.54 (74.33–80.75) | 80.27 (76.24–84.29) | 0.305 | |
| Age ≥ 65 (95% CI) | 21.46 (18.95–23.98) | 22.46 (19.25–25.67) | 19.73 (15.71–23.76) | 0.305 | |
| Chronic Diseases (95% CI) | |||||
| Hypertension | 48.98 (45.92–52.04) | 46.92 (43.09–50.76) | 52.53 (47.48–57.59) | 0.084 | |
| Cardiovascular disease | 39.61 (36.62–42.6) | 43.23 (39.42–47.04) | 33.33 (28.56–38.1) | 0.002 | |
| Diabetes | 21.56 (19.04–24.08) | 21.23 (18.09–24.37) | 22.13 (17.93–26.34) | 0.735 | |
| Chronic respiratory disease | 16.49 (14.22–18.76) | 18.15 (15.19–21.12) | 13.6 (10.13–17.07) | 0.058 | |
| Neoplasia | 10.73 (8.84–12.63) | 12.15 (9.64–14.67) | 8.27 (5.48–11.05) | 0.053 | |
| Autoimmune disease | 7.9 (6.25–9.55) | 9.08 (6.87–11.29) | 5.87 (3.49–8.25) | 0.066 | |
| Chronic Kidney disease | 7.12 (5.55–8.7) | 7.85 (5.78–9.91) | 5.87 (3.49–8.25) | 0.235 | |
| Treatment | |||||
| Oxygen delivery and ventilation (95% CI) | |||||
| IMV | 16.68 (14.4–18.97) | 20.15 (17.07–23.24) | 10.67 (7.54–13.79) | 0.001 | |
| Oxygen delivery | 4.78 (3.47–6.09) | 5.54 (3.78–7.3) | 3.47 (1.62–5.32) | 0.134 | |
| NIPPV | 3.41 (2.3–4.53) | 3.38 (1.99–4.77) | 3.47 (1.62–5.32) | 0.994 | |
| Medicines (95% CI) | |||||
| Antibiotics | 89.27 (87.37–91.16) | 88.31 (85.84–90.78) | 90.93 (88.03–93.84) | 0.191 | |
| Antimalarial | 68.1 (65.24–70.95) | 69.69 (66.16–73.23) | 65.33 (60.52–70.15) | 0.149 | |
| Steroids | 55.9 (52.86–58.94) | 58.31 (54.52–62.1) | 51.73 (46.68–56.79) | 0.041 | |
| Antivirals | 43.51 (40.48–46.55) | 47.08 (43.24–50.91) | 37.33 (32.44–42.23) | 0.002 | |
| Tocilizumab | 17.95 (15.6–20.3) | 21.23 (18.09–24.37) | 12.27 (8.95–15.59) | 0.001 | |
| Other anti-SIRS * | 11.9 (9.92–13.88) | 15.23 (12.47–17.99) | 6.13 (3.7–8.56) | 0.001 | |
| Clinical Outcomes | |||||
| Hospital LoS (median and IQR) | 11 (6–19) | 12 (6–21) | 9 (5–16) | 0.002 | |
| ICU LoS | (median and IQR) | 15 (9–25) | 15 (9–27) | 15 (8–24) | 0.403 |
| N | 99 | 79 | 20 | ||
| Death (95% CI) | 42.54 (39.51–45.56) | 44.62 (40.79–48.44) | 38.93 (34–43.87) | 0.076 | |
| AKI (95% CI) | 18.73 (16.34–21.12) | 19.38 (16.35–22.42) | 17.6 (13.75–21.45) | 0.481 | |
| Fungal superinfection (95% CI) | 5.37 (3.99–6.75) | 6 (4.17–7.83) | 4.27 (2.22–6.31) | 0.236 | |
| Bacterial superinfection (95% CI) | 4.39 (3.14–5.64) | 5.23 (3.52–6.94) | 2.93 (1.23–4.64) | 0.084 | |
| SIRS (95% CI) | 3.9 (2.72–5.09) | 4.62 (3–6.23) | 2.67 (1.04–4.3) | 0.121 | |
| Cardiomyopathy (95% CI) | 1.85 (1.03–2.68) | 2.62 (1.39–3.84) | 0.53 (0.2–1.27) | 0.017 | |
| DIC (95% CI) | 0.68 (0.18–1.19) | 0.92 (0.19–1.66) | 0.27 (0.06–0.59) | 0.219 | |
| Medicines | Total (95% CI) | Death (95% CI) | No-Death (95% CI) | p |
|---|---|---|---|---|
| N = 1025 | N = 589 | N = 436 | ||
| Antibiotics | 89.27 (87.37–91.16) | 88.62 (86.06–91.19) | 90.14 (87.34–92.94) | 0.439 |
| Ceftriaxone | 67.51 (64.65–70.38) | 66.38 (62.57–70.2) | 69.04 (64.7–73.38) | 0.37 |
| Azithromycin | 65.37 (62.45–68.28) | 69.61 (65.9–73.32) | 59.63 (55.03–64.24) | 0.001 |
| Levofloxacin | 22.34 (19.79–24.89) | 19.19 (16.01–22.36) | 26.61 (22.46–30.75) | 0.005 |
| Teicoplanine | 1.27 (0.58–1.95) | 1.19 (0.31–2.06) | 1.38 (0.28–2.47) | 0.791 |
| Cefditoren | 4.68 (3.39–5.98) | 5.77 (3.89–7.66) | 3.21 (1.56–4.87) | 0.055 |
| Clarithromycin | 0.78 (0.24–1.32) | 0.68 (0.02–1.34) | 0.92 (0.02–1.81) | 0.668 |
| Moxifloxacin | 0.2 (0.08–0.39) | 0 (0–0) | 0.46 (0.18–0.85) | 0.1 |
| Cefotaxime | 0.2 (0.08–0.39) | 0.17 (0.06–0.41) | 0.23 (0.02–0.56) | 0.831 |
| Ceftaroline | 0 (0–0) | 0 (0–0) | 0 (0–0) | - |
| Antimalarials | 68.1 (65.24–70.95) | 66.55 (62.74–70.36) | 70.18 (65.89–74.48) | 0.218 |
| Hydroxychloroquine | 63.8 (60.86–66.75) | 63.5 (59.61–67.39) | 64.22 (59.72–68.72) | 0.812 |
| Chloroquine | 5.27 (3.9–6.64) | 3.74 (2.2–5.27) | 7.34 (4.89–9.79) | 0.011 |
| Steroids | 55.9 (52.86–58.94) | 58.91 (54.94–62.89) | 51.83 (47.14–56.52) | 0.024 |
| Methylprednisolone | 54.05 (51–57.1) | 56.54 (52.53–60.54) | 50.69 (46–55.38) | 0.063 |
| Prednisone | 10.83 (8.93–12.73) | 13.58 (10.82–16.35) | 7.11 (4.7–9.52) | 0.001 |
| Antivirals | 43.51 (40.48–46.55) | 41.94 (37.95–45.92) | 45.64 (40.97–50.32) | 0.237 |
| Lopinavir-Ritonavir | 43.41 (40.38–46.45) | 41.94 (37.95–45.92) | 45.41 (40.74–50.09) | 0.267 |
| Remdesevir | 0.29 (0.04–0.54) | 0.17 (0.06–0.41) | 0.46 (0.18–0.85) | 0.397 |
| Tocilizumab | 17.95 (15.6–20.3) | 23.26 (19.85–26.67) | 10.78 (7.87–13.69) | 0.001 |
| Other anti-SIRS | 11.9 (9.92–13.88) | 10.02 (7.59–12.44) | 14.45 (11.15–17.75) | 0.03 |
| Interferon Beta | 8.98 (7.23–10.73) | 7.3 (5.2–9.4) | 11.24 (8.27–14.2) | 0.029 |
| Anakinra | 2.54 (1.57–3.5) | 2.72 (1.4–4.03) | 2.29 (0.89–3.7) | 0.67 |
| Ruxolitinib | 0.1 (0.09–0.12) | 0 (0–0) | 0.23 (0.02–0.56) | 0.245 |
| Baricitinib | 0.59 (0.12–1.05) | 0.51 (0.07–0.92) | 0.69 (0.09–1.35) | 0.711 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Abejón, E.; Herrera-Gómez, F.; Pedrosa-Naudín, M.A.; Tamayo, E.; Álvarez, F.J. Hospitalized COVID-19 Patients with Severe Acute Respiratory Syndrome: A Population-Based Registry Analysis to Assess Clinical Findings, Pharmacological Treatment and Survival. Medicina 2022, 58, 829. https://doi.org/10.3390/medicina58060829
Gutiérrez-Abejón E, Herrera-Gómez F, Pedrosa-Naudín MA, Tamayo E, Álvarez FJ. Hospitalized COVID-19 Patients with Severe Acute Respiratory Syndrome: A Population-Based Registry Analysis to Assess Clinical Findings, Pharmacological Treatment and Survival. Medicina. 2022; 58(6):829. https://doi.org/10.3390/medicina58060829
Chicago/Turabian StyleGutiérrez-Abejón, Eduardo, Francisco Herrera-Gómez, M. Aránzazu Pedrosa-Naudín, Eduardo Tamayo, and F. Javier Álvarez. 2022. "Hospitalized COVID-19 Patients with Severe Acute Respiratory Syndrome: A Population-Based Registry Analysis to Assess Clinical Findings, Pharmacological Treatment and Survival" Medicina 58, no. 6: 829. https://doi.org/10.3390/medicina58060829