
Healthcare Workers’ Knowledge and Perception of the SARS-CoV-2 Omicron Variant: A Multinational Cross-Sectional Study

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Content of the Survey Instrument
2.2. Validity of the Survey Tool
2.3. Sample Size
2.4. Recruitment
2.5. Scoring
2.6. Statistical Analysis
2.7. Ethical Consideration
3. Results
3.1. Overview
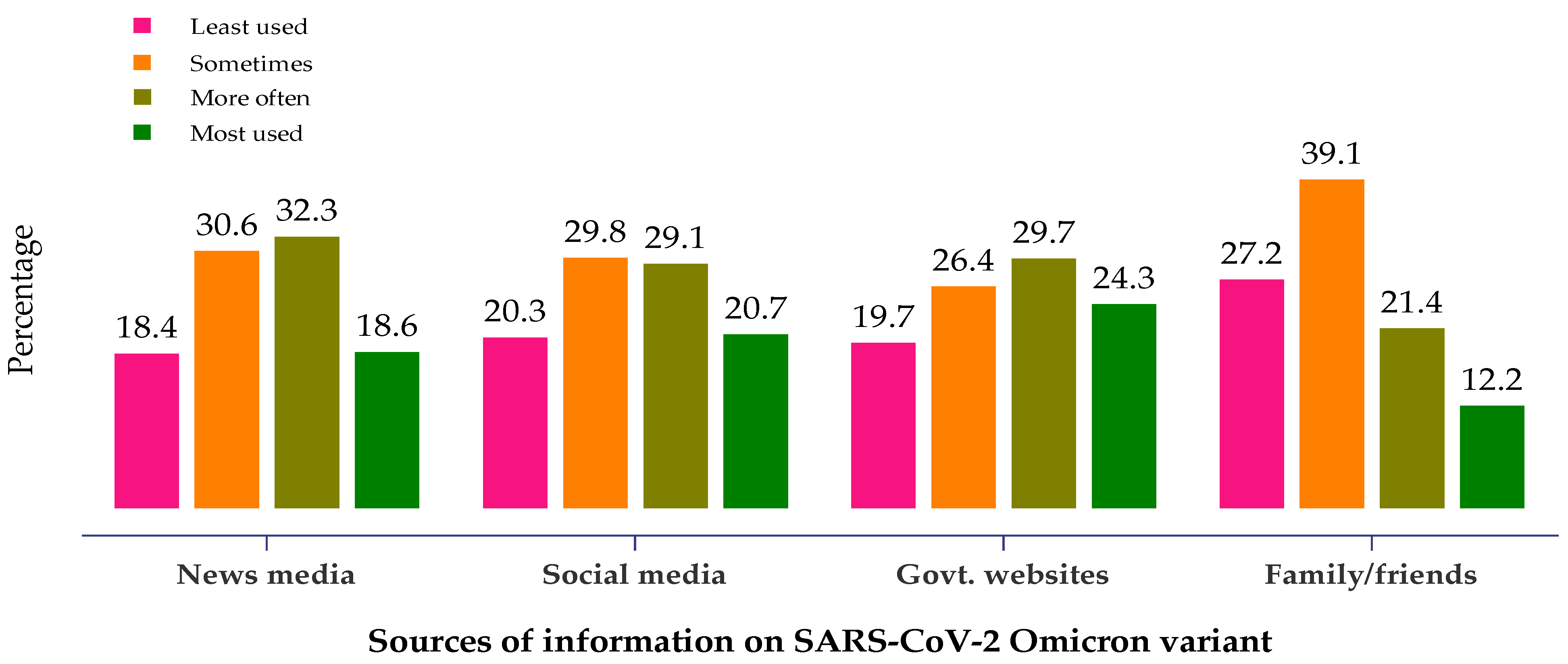
3.2. Source of Information
3.3. SARS-CoV-2 Variants of Concern
3.4. Knowledge and Perceptions about SARS-CoV-2 Omicron Variant
3.5. Comparison of HCWs’ Knowledge and Perception Scores According to Their Health Specialties
3.6. Overall Knowledge and Perception Levels
3.7. Predictors of Good Knowledge and Perception
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- John Hopkins, C. Coronavirus COVID-19 (2019-nCoV). 2020. Available online: https://www.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6 (accessed on 15 February 2022).
- WHO. 2021c WHO 2nd Global Consultation on Assessing the Impact of SARS-CoV-2 Variants of Concern on Public Health Interventions. Available online: https://www.who.int/publications/m/item/2nd-global-consultation-on-assessing-theimpact-of-sars-cov-2-variants-of-concern-on-public-health-interventions (accessed on 14 January 2022).
- Dolgin, E. Omicron thwarts some of the world’s most-used COVID vaccines. Nature 2022, 601, 311. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.L.; Morris, C.P.; Betz, J.; Zhang, Y.; Bollinger, R.; Wang, N.; Thiemann, D.R.; Fall, A.; Eldesouki, R.E.; Norton, J.M.; et al. Impact of SARS-CoV-2 variants on inpatient clinical outcome. medRxiv 2022, 2022, 22270337. [Google Scholar] [CrossRef]
- Ledford, H. How severe are Omicron infections? Nature 2021, 600, 577–578. [Google Scholar] [CrossRef]
- Sheikh, A.; Kerr, S.; Woolhouse, M.; McMenamin, J.; Robertson, C. Severity of Omicron Variant of Concern and Vaccine Effectiveness against Symptomatic Disease: National Cohort with Nested Test Negative Design Study in Scotland. 2021. Available online: https://www.pure.ed.ac.uk/ws/portalfiles/portal/245818096/Severity_of_Omicron_variant_of_concern_and_vaccine_effectiveness_against_symptomatic_disease.pdf (accessed on 20 December 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. C4591001 Clinical Trial Group. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; COVE Study Group. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Khoury, D.S.; Steain, M.; Triccas, J.A.; Sigal, A.; Davenport, M.P.; Cromer, D. A meta-analysis of early results to predict vaccine efficacy against Omicron. medRxiv 2021, 12, 21267748. [Google Scholar] [CrossRef]
- Israel, A.; Merzon, E.; Schäffer, A.A.; Shenhar, Y.; Green, I.; Golan-Cohen, A.; Ruppin, E.; Magen, E.; Vinker, S. Elapsed time since BNT162b2 vaccine and risk of SARS-CoV-2 infection: Test negative design study. BMJ 2021, 375, e067873. [Google Scholar] [CrossRef]
- Callaway, E.; Ledford, H. How bad is Omicron? What scientists know so far. Nature 2021, 600, 197–199. [Google Scholar] [CrossRef]
- Pajon, R.; Doria-Rose, N.A.; Shen, X.; Schmidt, S.D.; O’Dell, S.; McDanal, C.; Feng, W.; Tong, J.; Eaton, A.; Maglinao, M.; et al. SARS-CoV-2 Omicron Variant Neutralization after mRNA-1273 Booster Vaccination. N. Engl. J. Med. 2022. [Google Scholar] [CrossRef]
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K. Knowledge and Perceptions of COVID-19 Among Health Care Workers: Cross-Sectional Study. JMIR Public Health Surveill. 2020, 6, e19160. [Google Scholar] [CrossRef] [PubMed]
- Gambhir, R.S.; Dhaliwal, J.S.; Aggarwal, A.; Anand, S.; Anand, V.; Kaur Bhangu, A. COVID-19: A survey on knowledge, awareness and hygiene practices among dental health professionals in an Indian scenario. Rocz. Panstw. Zakl. Hig. 2020, 71, 223–229. [Google Scholar] [CrossRef]
- Zhang, M.; Zhou, M.; Tang, F.; Wang, Y.; Nie, H.; Zhang, L.; You, G. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J. Hosp. Infect. 2020, 105, 183–187. [Google Scholar] [CrossRef]
- Masoud, A.T.; Zaazouee, M.S.; Elsayed, S.M.; Ragab, K.M.; Kamal, E.M.; Alnasser, Y.T.; Assar, A.; Nourelden, A.Z.; Istatiah, L.J.; KAP-COVIDGLOBAL Investigators. KAP-COVIDGLOBAL: A multinational survey of the levels and determinants of public knowledge, attitudes and practices towards COVID-19. BMJ Open 2021, 11, e043971. [Google Scholar] [CrossRef] [PubMed]
- Siddiquea, B.N.; Shetty, A.; Bhattacharya, O.; Afroz, A.; Billah, B. Global epidemiology of COVID-19 knowledge, attitude and practice: A systematic review and meta-analysis. BMJ Open 2021, 11, e051447. [Google Scholar] [CrossRef]
- WHO. Coronavirus Update 70: Update on SARS-CoV-2 Variant of Concern Omicron. Available online: https://www.who.int/docs/default-source/coronaviruse/risk-comms-updates/update70_omicron.pdf?sfvrsn=eaf76988_5 (accessed on 10 December 2021).
- CDC. Update on Omicron Variant. Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-12-16/06-COVID-Scobie-508.pdf (accessed on 17 December 2021).
- CDC. Science Brief: Omicron (B.1.1.529) Variant. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/scientific-brief-omicron-variant.html (accessed on 12 December 2021).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, P.; Bloom’s Taxonomy. Vanderbilt University Center for Teaching. Available online: https://cft.vanderbilt.edu/guides-sub-pages/blooms-taxonomy.htm (accessed on 15 December 2021).
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Murray, C.J.L. COVID-19 will continue but the end of the pandemic is near. Lancet 2022, 399, 417–419. [Google Scholar] [CrossRef]
- Hoffmann, M.; Krüger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2022, 185, 447–456.e11. [Google Scholar] [CrossRef] [PubMed]
- OECD Policy Responses to Coronavirus (COVID-19). Transparency, Communication and Trust: The Role of Public Communication in Responding to the Wave of Disinformation about the New Coronavirus. Available online: https://www.oecd.org/coronavirus/policy-responses/transparency-communication-and-trust-the-role-of-public-communication-in-responding-to-the-wave-of-disinformation-about-the-new-coronavirus-bef7ad6e/ (accessed on 19 January 2022).
- World Health Organization (WHO). Pandemic Fatigue—Reinvigorating the Public to Prevent COVID-19. Policy Framework for Supporting Pandemic Prevention and Management; WHO Regional Office for Europe: Copenhagen, Denmark, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf (accessed on 19 February 2022).
- World Health Organization. Coronavirus Disease (COVID-19) Training: Online Training. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/training/online-training (accessed on 19 February 2022).
- United Nations. Sharpen Your Skills during Lockdown with UN e-Learning Courses. Available online: https://unric.org/en/sharpen-your-skills-during-lockdown-with-united-nations-e-learning-courses/ (accessed on 19 February 2022).
- Mutambudzi, M.; Niedwiedz, C.; Macdonald, E.B.; Leyland, A.; Mair, F.; Anderson, J.; Celis-Morales, C.; Cleland, J.; Forbes, J.; Gill, J.; et al. Occupation and risk of severe COVID-19: Prospective cohort study of 120 075 UK Biobank participants. Occup. Environ. Med. 2020, 78, 307–314. [Google Scholar] [CrossRef]
- World Health Organization (Europe). The Omicron Variant: Sorting Fact from Myth. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/pages/news/news/2022/01/the-omicron-variant-sorting-fact-from-myth (accessed on 20 January 2022).
- Kannan, S.; Ali, P.S.S.; Sheeza, A. Omicron (B.1.1.529)—Variant of concern—Molecular profile and epidemiology: A mini review. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 8019–8022. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Frequency (%) |
|---|---|
| Sex | |
| Male | 539 (57.3) |
| Female | 401 (42.7) |
| Age (mean ± SD) | 31.2 ± 11.2 years |
| 18-29 | 530 (56.4) |
| 30-39 | 194 (20.6) |
| ≥40 | 216 (23) |
| Participant’s Location | |
| Asia | 604 (64.3) |
| Africa | 137 (14.6) |
| Europe | 125 (13.3) |
| South America | 39 (4.1) |
| North America | 28 (3.0) |
| Oceanic | 7 (0.7) |
| Profession | |
| Doctors | 430 (45.7) |
| Medical students | 225 (23.9) |
| Pharmacists | 120 (12.8) |
| Nurses | 60 (6.4) |
| Allied health | 105 (11.2) |
| I Heard of SARS-CoV-2 Omicron | 940 (100) |
| I Attended Lectures/Dissions About Omicron | 341 (36.3) |
| Survey Completion Time (mean ± SD) | 5.9 ± 3.9 min |
| Items Related to the SARS-CoV-2 Omicron Variant | Correct Response (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Knowledge | Doctors | Medical Students | Nurses | Pharmacists | Allied Health | Variance | p-Values (Male vs. Female) | p-Value (Doctors vs. Others) | p-Value (Attended vs. Did Not Attend Lectures) | p-Value (Developed vs. Developing Country) |
| n = 430 | n = 225 | n = 60 | n = 120 | n = 105 | ||||||
| The Omicron variant was first reported to the World health organization from South Africa | 328 (76.3) | 132 (58.7) | 46 (76.7) | 73 (60.8) | 69 (65.7) | 0.002 | <0.001 | 0.001 | 0.010 | <0.001 |
| Skin rash is not a symptom of Omicron | 341 (79.3) | 163 (72.4) | 45 (75) | 83 (77.5) | 73 (69.5) | 0.315 | 0.767 | 0.048 | 0.952 | 0.060 |
| Omicron can be transmited to all age groups | 402 (93.5) | 197 (87.6) | 57 (95) | 112 (93.3) | 91 (86.7) | 0.051 | 0.021 | 0.033 | 0.434 | 0.080 |
| Wearing a face mask, hand hygiene, social distancing, indoor ventilation, avoiding crowded places, and COVID-19 vaccination can protect from Omicron | 403 (93.5) | 208 (92.4) | 57 (95) | 112 (93.3) | 93 (88.6) | 0.693 | 0.991 | 0.458 | 0.443 | 0.590 |
| Taking two doses of COVID-19 vaccination is important | 394 (91.6) | 194 (86.2) | 52 (86.7) | 108 (90.0) | 90 (85.7) | 0.167 | 0.243 | 0.025 | 0.009 | 0.295 |
| Perceptions | ||||||||||
| Currently available COVID-19 vaccines offer protection against Omicron | 140 (32.6) | 74 (32.9) | 17 (28.3) | 41 (34.2) | 34 (32.4) | 0.888 | 0.177 | 0.978 | 0.855 | 0.326 |
| A COVID-19 booster dose offers protection against Omicron | 173 (40.2) | 92 (40.9) | 18 (30.0) | 53 (44.2) | 39 (37.1) | 0.331 | 0.149 | 0.606 | 0.269 | 0.906 |
| COVID-19 mutations could alter the response to vaccines, treatment, and transmissibility | 264 (61.4) | 112 (49.8) | 38 (63.3) | 67 (55.8) | 60 (57.1) | 0.044 | 0.516 | 0.030 | 0.244 | 0.954 |
| Both vaccinated and unvaccinated people are vulnerable to Omicron | 388 (90.2) | 196 (87.1) | 56 (93.3) | 104 (86.7) | 89 (84.8) | 0.294 | 0.335 | 0.152 | 0.125 | 0.989 |
| Travel bans cannot limit the global spread of Omicron | 111 (25.8) | 48 (21.3) | 18 (30) | 18 (15) | 26 (24.8) | 0.085 | 0.004 | 0.126 | 0.324 | <0.001 |
| Older people and people with comorbidities should postpone travel | 396 (92.1) | 211 (93.8) | 54 (90) | 109 (90.8) | 95 (90.5) | 0.764 | 0.807 | 0.941 | 0.193 | 0.314 |
| Steroids are not effective against severe Omicron | 200 (46.5) | 114 (50.7) | 33 (55) | 69 (57.5) | 72 (68.6) | <0.001 | 0.009 | 0.002 | 0.413 | 0.678 |
| A COVID-19 rapid antigen test is not reliable to detect the Omicron | 174 (40.5) | 100 (44.4) | 25 (41.7) | 54 (45) | 44 (41.9) | 0.847 | 0.475 | 0.314 | 0.998 | 0.060 |
| Face masks offer protection against all SARS-CoV-2 variants | 370 (86) | 191 (84.9) | 46 (76.7) | 104 (86.7) | 82 (78.1) | 0.122 | 0.501 | 0.192 | 0.419 | 0.125 |
| Countries should accelerate the COVID-19 vaccination program | 405 (94.2) | 206 (91.6) | 54 (90) | 109 (90.8) | 96 (91.4) | 0.516 | 0.472 | 0.080 | 0.381 | 0.179 |
| Specialty | Frequency | Median (Range) | F | df | p-Value | |
|---|---|---|---|---|---|---|
| Knowledge score | Doctors | 430 | 14 (0–20) | 3.82 | 4 | 0.004 |
| Medical students | 225 | 12 (4–20) | ||||
| Nurses | 60 | 12 (6–20) | ||||
| Pharmacists | 120 | 12 (2–20) | ||||
| Allied Health | 105 | 12 (2–20) | ||||
| Perception score | Doctors | 430 | 13 (5–18) | 0.374 | 4 | 0.827 |
| Medical students | 225 | 12 (6–20) | ||||
| Nurses | 60 | 12 (6–18) | ||||
| Pharmacists | 120 | 12 (6–20) | ||||
| Allied Health | 105 | 12 (4–18) |
| Subgroup | Knowledge | p-Value | Perception | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Good | Moderate | Poor | Good | Neutral | Misperceptions | ||||
| Scores | 16–20 | 12–15 | <12 | 16–20 | 12–15 | <12 | |||
| Total | N= 940 | 228 (24.3) | 409 (43.5) | 303 (32.2) | <0.001 | 194 (20.6) | 492 (52.3) | 254 (27) | 0.001 |
| Sex | 0.624 | 0.913 | |||||||
| Male | 132 (14) | 240 (25.5) | 167 (17.8) | 109 (11.6) | 285 (30.3) | 145 (15.4) | |||
| Female | 96 (10.2) | 169 (18) | 136 (14.5) | 85 (9) | 207 (22) | 109 (11.6) | |||
| Age (years) | 0.002 | 0.132 | |||||||
| <30 | 118 (12.6) | 216 (23) | 196 (20.9) | 97 (10.3) | 286 (30.4) | 147 (15.6) | |||
| ≥30 | 110 (11.7) | 193 (20.5) | 107 (11.4) | 97 (10.3) | 206 (21.9) | 107 (11.4) | |||
| Countries | <0.001 | 0.369 | |||||||
| Developing | 178 (18.9) | 312 (33.3) | 266 (28.3) | 43 (4.6) | 98 (10.4) | 43 (4.6) | |||
| Developed | 50 (5.3) | 97 (10.3) | 37 (3.9) | 151 (16.1) | 394 (41.9) | 211 (22.4) | |||
| Profession | 0.001 | 0.496 | |||||||
| Doctors | 121 (12.9) | 203 (21.6) | 106 (11.3) | 94 (10) | 227 (24.1) | 109 (11.6) | |||
| Medical students | 42 (4.5) | 87 (9.3) | 96 (10.2) | 46 (4.9) | 109 (11.6) | 70 (7.4) | |||
| Nurses | 15 (1.6) | 27 (2.9) | 18 (1.9) | 12 (1.3) | 36 (3.8) | 12 (1.3) | |||
| Pharmacists | 27 (2.9) | 50 (5.3) | 43 (4.6) | 18 (1.9) | 68 (7.2) | 32 (3.6) | |||
| Allied health | 23 (2.4) | 42 (4.5) | 40 (4.3) | 24 (2.6) | 52 (5.5) | 29 (3.1) | |||
| Odds Ratio (95% Confidence Intervals) | ||||
|---|---|---|---|---|
| Categories | Good Knowledge | Good Perception | Both | |
| Sex | Female | 1 | 1 | 1 |
| Male | 0.93 (0.68–1.27) | 0.89 (0.64–1.24) | 0.85 (0.49–1.47) | |
| Age | Years | 1.07 (0.99–1.02) | 1.01 (1.00–1.03) * | 1.01 (0.99–1.04) |
| Location | Asia | 1 | 1 | 1 |
| Africa | 0.48 (0.26–78) ** | 0.55 (0.31–0.95) * | 0.21 (0.05–0.92) * | |
| Europe | 1.18 (0.76–1.84) | 1.14 (0.70–1.84) | 1.33 (0.66–2.68) | |
| South America | 1.23 (0.53–2.86) | 2.69 (1.21–6.00) * | 1.37 (0.37–5.00) | |
| North America | 0.53 (0.06–4.52) | 2.84 (0.62–12.91) | - | |
| Oceanic | 0.73 (0.33–1.63) | 2.04 (1.00–4.16) * | 0.90 (0.25–3.22) | |
| Profession | Doctors | 1 | 1 | 1 |
| Medical students | 0.67 (0.43–1.04) | 1.15 (0.70–1.76) | 0.85 (0.37–1.94) | |
| Pharmacists | 0.91 (0.48–1.72) | 0.86 (0.43–1.70) | 1.08 (0.40–2.96) | |
| Nurses | 0.85 (0.51–1.42) | 0.72 (0.40–1.30) | 0.59 (0.19–1.81) | |
| Allied health | 0.77 (0.46–1.29) | 1.07 (0.64–1.80) | 0.78 (0.31–1.95) | |
| Engaged in Omicron-related training/discussions | No | 1 | 1 | 1 |
| Yes | 1.72 (1.27–2.38) ** | 0.98 (0.70–1.38) | 1.80 (1.04–3.11) ** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhagavathula, A.S.; Mahabadi, M.A.; Tesfaye, W.; Nayar, K.R.; Chattu, V.K. Healthcare Workers’ Knowledge and Perception of the SARS-CoV-2 Omicron Variant: A Multinational Cross-Sectional Study. Healthcare 2022, 10, 438. https://doi.org/10.3390/healthcare10030438
Bhagavathula AS, Mahabadi MA, Tesfaye W, Nayar KR, Chattu VK. Healthcare Workers’ Knowledge and Perception of the SARS-CoV-2 Omicron Variant: A Multinational Cross-Sectional Study. Healthcare. 2022; 10(3):438. https://doi.org/10.3390/healthcare10030438
Chicago/Turabian StyleBhagavathula, Akshaya Srikanth, Mohammadjavad Ashrafi Mahabadi, Wubshet Tesfaye, Kesavan Rajasekharan Nayar, and Vijay Kumar Chattu. 2022. "Healthcare Workers’ Knowledge and Perception of the SARS-CoV-2 Omicron Variant: A Multinational Cross-Sectional Study" Healthcare 10, no. 3: 438. https://doi.org/10.3390/healthcare10030438