
Association of Tocilizumab and Invasive Aspergillosis in Critically Ill Patients with Severe COVID-19 Pneumonia and Acute Respiratory Distress Syndrome


Abstract
:1. Introduction
2. Case Presentation
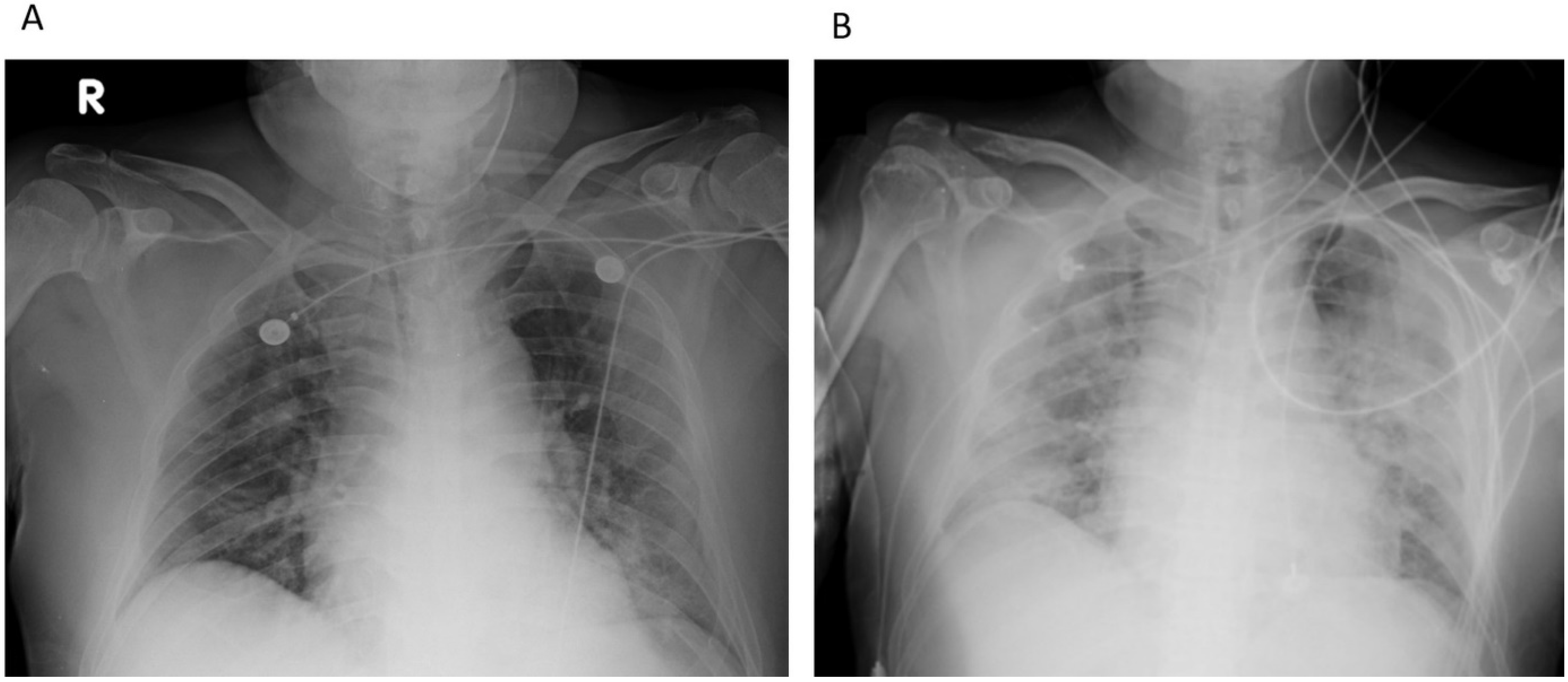
2.1. Representative Case 1 (Patient 3)
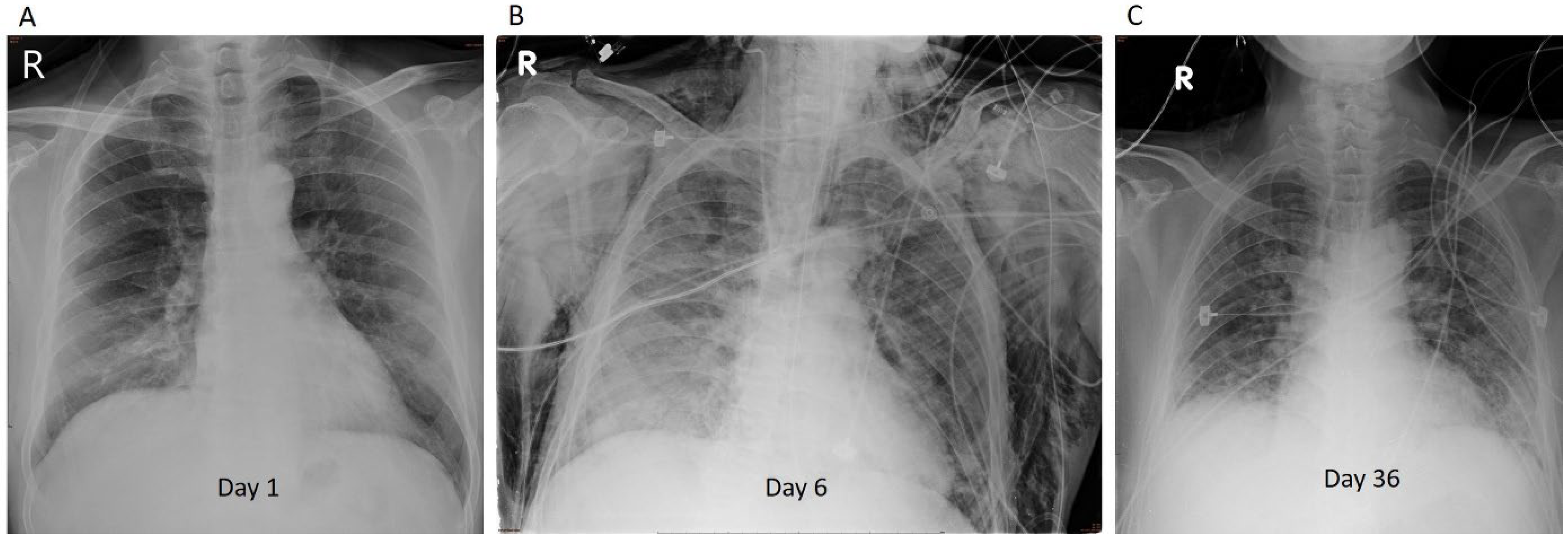
2.2. Representative Case 2 (Patient 5)
2.3. Patient Review
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: The CoDEX randomized clinical trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [PubMed]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar]
- Taiwan Centers for Disease Control. Interim Guidelines for Clinical Management of SARS-CoV-2 Infection 10th Edition. Available online: https://www.cdc.gov.tw/File/Get/G4gjnyiSWyuvWtwCU7-9kQ (accessed on 20 May 2021).
- Duarte, R.F.; Sánchez-Ortega, I.; Cuesta, I.; Arnan, M.; Patiño, B.; Fernández de Sevilla, A.; Gudiol, C.; Ayats, J.; Cuenca-Estrella, M. Serum galactomannan-based early detection of invasive aspergillosis in hematology patients receiving effective antimold prophylaxis. Clin. Infect. Dis. 2014, 59, 1696–1702. [Google Scholar] [PubMed] [Green Version]
- Nasa, P.; Singh, A.; Upadhyay, S.; Bagadia, S.; Polumuru, S.; Shrivastava, P.K.; Sankar, R.; Vijayan, L.; Soliman, M.A.; Ali, A.; et al. Tocilizumab Use in COVID-19 Cytokine-release Syndrome: Retrospective Study of Two Centers. Indian J. Crit. Care Med. Peer-Rev. 2020, 24, 771–776. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [PubMed]
- Angriman, F.; Ferreyro, B.L.; Burry, L.; Fan, E.; Ferguson, N.D.; Husain, S.; Keshavjee, S.H.; Lupia, E.; Munshi, L.; Renzi, S.; et al. Interleukin-6 receptor blockade in patients with COVID-19: Placing clinical trials into context. Lancet Respir. Med. 2021, 9, 655–664. [Google Scholar]
- Lackner, N.; Thomé, C.; Öfner, D.; Joannidis, M.; Mayerhöfer, T.; Arora, R.; Samardzic, E.; Posch, W.; Breitkopf, R.; Lass-Flörl, C. COVID-19 Associated Pulmonary Aspergillosis: Diagnostic Performance, Fungal Epidemiology and Antifungal Susceptibility. J. Fungi 2022, 8, 93. [Google Scholar] [CrossRef]
- White, P.L.; Springer, J.; Wise, M.P.; Einsele, H.; Löffler, C.; Seif, M.; Prommersberger, S.; Backx, M.; Löffler, J. A Clinical Case of COVID-19-Associated Pulmonary Aspergillosis (CAPA), Illustrating the Challenges in Diagnosis (Despite Overwhelming Mycological Evidence). J. Fungi 2022, 8, 81. [Google Scholar] [CrossRef]
- Lu, D.-E.; Hung, S.-H.; Su, Y.-S.; Lee, W.-S. Analysis of Fungal and Bacterial Co-Infections in Mortality Cases among Hospitalized Patients with COVID-19 in Taipei, Taiwan. J. Fungi 2022, 8, 91. [Google Scholar] [CrossRef]
- Deana, C.; Vetrugno, L.; Bassi, F.; De Monte, A. Tocilizumab administration in COVID-19 patients: Water on the fire or gasoline? Med. Mycol. Case Rep. 2021, 31, 32–34. [Google Scholar] [PubMed]
- Sun, K.S.; Tsai, C.F.; Chen, S.C.C.; Huang, W.C. Clinical outcome and prognostic factors associated with invasive pulmonary aspergillosis: An 11-year follow-up report from Taiwan. PLoS ONE 2017, 12, e0186422. [Google Scholar]
- Marta, G.-C.; Lorena, F.-E.; Laura, M.-V.; Angela, L.-M.; Blanca, L.-G.; Rodrigo, A.-A.; Marta, S.-G.; Santiago, M.-G.; Liliana, P.-M.; Maria Luisa, S.-N.; et al. COVID-19-Associated Pulmonary Aspergillosis in a Tertiary Hospital. J. Fungi 2022, 8, 97. [Google Scholar] [CrossRef]
- Aubry, A.; Porcher, R.; Bottero, J.; Touratier, S.; Leblanc, T.; Brethon, B.; Rousselot, P.; Raffoux, E.; Menotti, J.; Derouin, F.; et al. Occurrence and kinetics of false-positive Aspergillus galactomannan test results following treatment with beta-lactam antibiotics in patients with hematological disorders. J. Clin. Microbiol. 2006, 44, 389–394. [Google Scholar]
- Morena, V.; Milazzo, L.; Oreni, L.; Bestetti, G.; Fossali, T.; Bassoli, C.; Torre, A.; Cossu, M.V.; Minari, C.; Ballone, E.; et al. Off-label use of tocilizumab for the treatment of SARS-CoV-2 pneumonia in Milan, Italy. Eur. J. Intern. Med. 2020, 76, 36–42. [Google Scholar]
- Quartuccio, L.; Sonaglia, A.; McGonagle, D.; Fabris, M.; Peghin, M.; Pecori, D.; De Monte, A.; Bove, T.; Curcio, F.; Bassi, F.; et al. Profiling COVID-19 pneumonia progressing into the cytokine storm syndrome: Results from a single Italian Centre study on tocilizumab versus standard of care. J. Clin. Virol. 2020, 129, 104444. [Google Scholar]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar]
- Kimmig, L.M.; Wu, D.; Gold, M.; Pettit, N.N.; Pitrak, D.; Mueller, J.; Husain, A.N.; Mutlu, E.A.; Mutlu, G.M. IL-6 inhibition in critically ill COVID-19 patients is associated with increased secondary infections. Front. Med. 2020, 7, 583897. [Google Scholar]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Shankar-Hari, M.; Vale, C.L.; Godolphin, P.J.; Fisher, D.; Higgins, J.P.T.; Spiga, F.; Savovic, J.; Tierney, J.; Baron, G.; et al. Association between administration of IL-6 antagonists and mortality among patients hospitalized for COVID-19: A meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar]
- Cai, S.; Sun, W.; Li, M.; Dong, L. A complex COVID-19 case with rheumatoid arthritis treated with tocilizumab. Clin. Rheumatol. 2020, 39, 2797–2802. [Google Scholar] [CrossRef]
- Burger, B.J.; Epps, S.M.; Cardenas, V.M.; Jagana, R.; Atchley, W.T. Tocilizumab Is Associated with Increased Risk of Fungal Infections among Critically Ill Patients with COVID-19 and Acute Renal Failure: An Observational Cohort Study; American Thoracic Society: New York, NY, USA, 2021; p. A2635. [Google Scholar]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; COVID-19 Study Group; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [PubMed]
- Mughal, M.S.; Kaur, I.; Kakadia, M.; Wang, C.; Alhashemi, R.; Salloum, R.; Ricca, A.; Granet, K. Is there any additional benefit of multiple doses of tocilizumab in COVID-19 patients? Cureus 2020, 12, e12214. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | |
|---|---|---|---|---|---|---|
| Age | 72 | 53 | 61 | 63 | 61 | 77 |
| Sex | Male | Male | Male | Male | Male | Female |
| Weight (kg) | 77 | 73 | 70 | 53 | 64 | 66 |
| Tobacco exposure | Current smoker | Never smoked | Current smoker | Never smoked | Former smoker | Never smoked |
| Comorbidities | DM, HbA1c: 6.6% Wegner granulomatosis | DM, HbA1c: 9.2% | DM, HbA1c: 11% HTN | DM, HbA1c: 9.4% HTN | COPD | DM, HbA1c: 6.4% |
| COVID-19 symptoms | Dyspnea, cough | Cough, myalgia | Cough, fever, dyspnea | Cough, fever, diarrhea | Fever, dyspnea, cough | Cough, dyspnea |
| Time from symptom onset to diagnosis (day(s)) | 3 | 2 | 4 | 1 | 1 | 1 |
| APACHE II scores | 23 | 11 | 13 | 26 | 18 | 31 |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | |
|---|---|---|---|---|---|---|
| First tocilizumab dose | 5.2 mg/kg | 11 mg/kg | 4 mg/kg | 7.5 mg/kg | 6.25 mg/kg | 6 mg/kg |
| Second tocilizumab dose | 5.2 mg/kg | n/a | 4 mg/kg | 7.5 mg/kg | 3.1 mg/kg | 6 mg/kg |
| Days between 1ST and 2nd tocilizumab dose | 3 | n/a | 4 | 6 | 8 | 11 |
| Total cumulative tocilizumab dose | 10.4 mg/kg | 11 mg/kg | 8 mg/kg | 15 mg/kg | 9.38 mg/kg | 12.12 mg/kg |
| Status of capa $ | Probable | Probable | Probable | Probable | Probable | Probable |
| Usage of penicillin before diagnosis | No | No | Yes, piperacillin/tazobactam | Yes, piperacillin/tazobactam | No | No |
| Blood Aspergillus AG titer while IA diagnosed | 0.69 | 0.61 | 0.73 | 1.82 | 0.76 | 1.09 |
| The highest blood ASPERGILLUS AG titer | 1.60 | 6.62 | 1.14 | 3.17 | 2.26 | 4.71 |
| The highest BAL ASPERGILLUS AG titer | 7.09 | 0.89 | 0.36 | 0.76 | 0.26 | 0.41 |
| Imagine evidence of aspergillosis in chest CT | N/A | Nonspecific findings | N/A | Clusters of fluffy nodules | Diffuse ground glass opacity with reticulations | Diffuse ground glass opacity with consolidations |
| Days after COVID-19 symptom onset to IA diagnosed | 32 | 32 | 15 | 21 | 20 | 27 |
| Days after ICU admission to IA diagnosed | 28 | 19 | 6 | 18 | 11 | 10 |
| Days after 1ST tocilizumab dose to IA diagnosed | 28 | 26 | 9 | 13 | 11 | 21 |
| Days after 2nd tocilizumab dose to IA diagnosed | 25 | n/a | 5 | 7 | 3 | 10 |
| Antifungal agent | Voriconazole | Voriconazole + caspofungin, switched to posaconazole | Voriconazole | Voriconazole, add-on caspofungin | Voriconazole + micafungin, switched to posaconazole | Voriconazole, add-on caspofungin |
| Outcomes | Death on Day 51 | Death on Day 168 | Discharged on Day 28 | Discharged on Day 76 | Discharged on Day 61 | Discharged on Day 151 (respiratory care ward) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, K.-L.; Chang, C.-Y.; Sung, H.-Y.; Hu, T.-Y.; Kuo, L.-K. Association of Tocilizumab and Invasive Aspergillosis in Critically Ill Patients with Severe COVID-19 Pneumonia and Acute Respiratory Distress Syndrome. J. Fungi 2022, 8, 339. https://doi.org/10.3390/jof8040339
Wu K-L, Chang C-Y, Sung H-Y, Hu T-Y, Kuo L-K. Association of Tocilizumab and Invasive Aspergillosis in Critically Ill Patients with Severe COVID-19 Pneumonia and Acute Respiratory Distress Syndrome. Journal of Fungi. 2022; 8(4):339. https://doi.org/10.3390/jof8040339
Chicago/Turabian StyleWu, Kuo-Lun, Chia-Yuan Chang, Heng-You Sung, Ting-Yu Hu, and Li-Kuo Kuo. 2022. "Association of Tocilizumab and Invasive Aspergillosis in Critically Ill Patients with Severe COVID-19 Pneumonia and Acute Respiratory Distress Syndrome" Journal of Fungi 8, no. 4: 339. https://doi.org/10.3390/jof8040339