
Operational Implications and Risk Assessment of COVID-19 in Dental Practices

 ,
,  ,
, 
Abstract
:1. Introduction
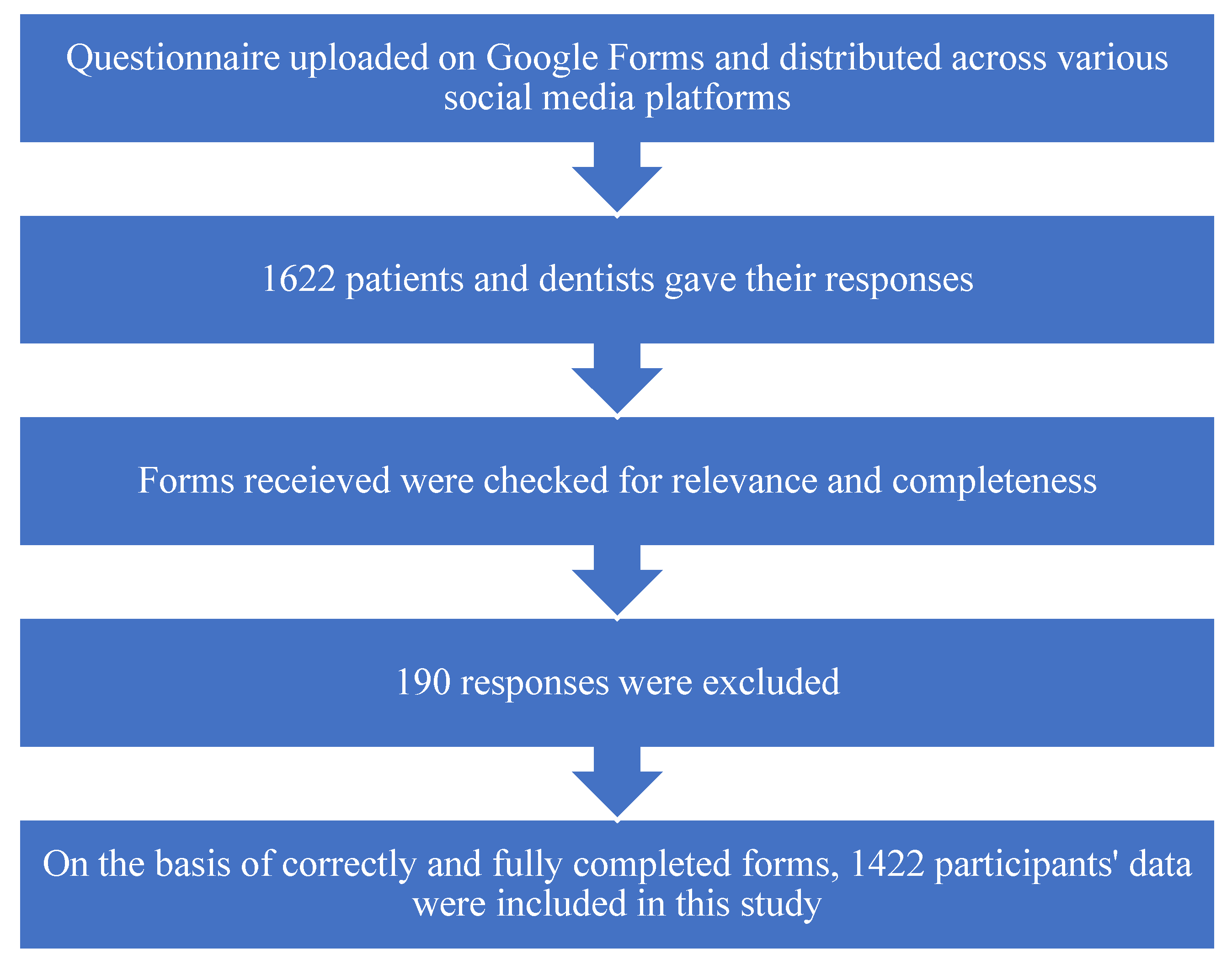
2. Materials and Methods
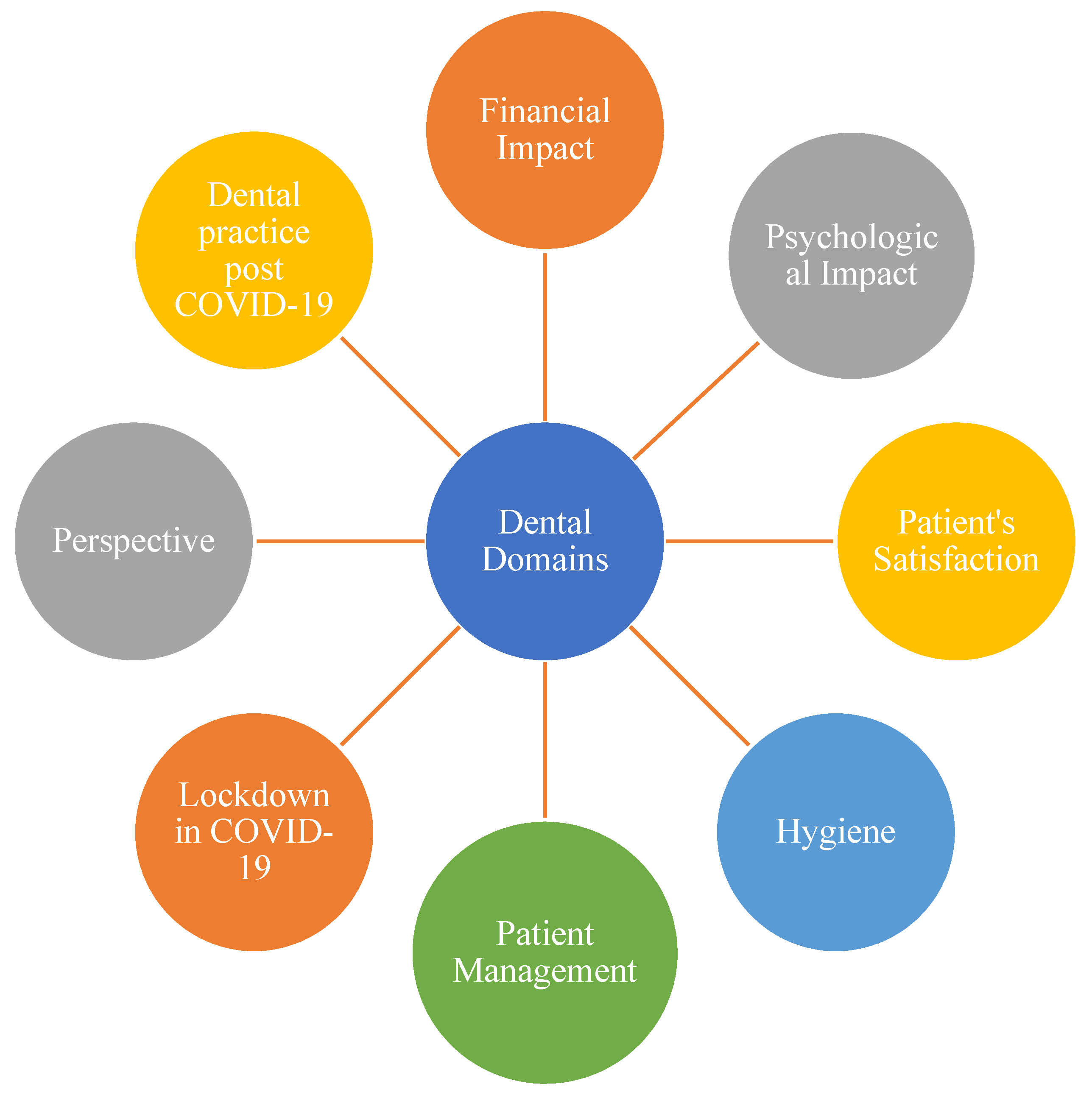
3. Results
3.1. Patients’ Satisfaction
3.2. Financial Impact
3.3. Psychological Impact
3.4. Patients’ Satisfaction
3.5. Hygiene
3.6. Patient Management
3.7. Lockdown in COVID-19 Pandemic
3.8. Dentists’ Perspective
3.9. Practicing Dentistry Post-COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Full Name/Description |
| CDC | Centre for Disease Control and Prevention |
| PPE | Personal Protective Equipment |
| COVID-19 | Novel Coronavirus Disease 2019 |
References
- Zhu, H.; Wei, L.; Niu, P. The novel coronavirus outbreak in Wuhan, China. Glob. Health Res. Policy 2020, 5, 6. Available online: https://ghrp.biomedcentral.com/articles/10.1186/s41256-020-00135-6 (accessed on 18 June 2021). [CrossRef] [PubMed] [Green Version]
- Excler, J.-L.; Saville, M.; Berkley, S.; Kim, J.H. Vaccine development for emerging infectious diseases. Nat. Med. 2021, 27, 591–600. Available online: http://www.nature.com/articles/s41591-021-01301-0 (accessed on 18 June 2021). [CrossRef] [PubMed]
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatunge, J. Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy. Environ Res. 2020, 188, 109819. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0013935120307143 (accessed on 18 June 2021). [CrossRef]
- Klopfenstein, T.; Zahra, H.; Kadiane-Oussou, N.J.; Lepiller, Q.; Royer, P.-Y.; Toko, L.; Gendrin, V.; Zayet, S. New loss of smell and taste: Uncommon symptoms in COVID-19 patients on Nord Franche-Comte cluster, France. Int. J. Infect. Dis. 2020, 100, 117–122. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1201971220306378 (accessed on 18 June 2021). [CrossRef] [PubMed]
- Rella, S.A.; Kulikova, Y.A.; Dermitzakis, E.T.; Kondrashov, F.A. Rates of SARS-CoV-2 transmission and vaccination impact the fate of vaccine-resistant strains. Sci. Rep. 2021, 11, 15729. Available online: http://www.nature.com/articles/s41598-021-95025-3 (accessed on 18 June 2021). [CrossRef] [PubMed]
- Nijakowski, K.; Cieślik, K.; Łaganowski, K.; Gruszczyński, D.; Surdacka, A. The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures. Int. J. Environ. Res. Public Health 2021, 18, 3421. Available online: https://www.mdpi.com/1660-4601/18/7/3421 (accessed on 18 June 2021). [CrossRef]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection Control in Dental Practice During the COVID-19 Pandemic. Int. J. Environ. Res Public Health 2020, 17, 4769. Available online: https://www.mdpi.com/1660-4601/17/13/4769 (accessed on 18 June 2021). [CrossRef]
- Guidance for Dental Settings-Interim Infection Prevention and Control Guidance for Dental Settings During the Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html (accessed on 18 June 2021).
- Lal, A.; Sanaullah, A.M.; Saleem, M.K.; Ahmed, N.; Maqsood, A.; Ahmed, N. Psychological Distress among Adults in Home Confinement in the Midst of COVID-19 Outbreak. Eur. J. Dent. 2020, 14, 27–33. Available online: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0040-1718644 (accessed on 18 June 2021). [CrossRef]
- Ghai, S. Teledentistry during COVID-19 pandemic. Diabetes Metab Syndr. Clin Res. Rev. 2020, 14, 933–935. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1871402120301983 (accessed on 18 June 2021). [CrossRef]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Saleem, M.K.M.; Lal, A. Knowledge, Attitude, and Practice Towards COVID-19 Among General Population of Karachi South: A Cross-Sectional Survey. J. Dow. Univ. Health Sci. 2020, 14, 77–82. Available online: http://www.jduhs.com/index.php/jduhs/article/view/991 (accessed on 18 June 2021). [CrossRef]
- Chitaladze, T.; Kazakhashvili, N. Knowledge, Attitudes and Perception Among Patients Towards Cross-Infection Control Measures in Dental Clinics in Georgia Before The Covid-19 Pandemic. Georgian Med. News 2020, 161–166. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33526748 (accessed on 18 June 2021).
- Nathwani, S.; Rahman, N. The 3 P’s model enhancing patient safety during the COVID-19 pandemic. Oral Surg. 2021, 14, 246–254. Available online: https://onlinelibrary.wiley.com/doi/10.1111/ors.12607 (accessed on 18 June 2021). [CrossRef] [PubMed]
- Nazir, M.; Almulhim, K.S.; Al-Daamah, Z.; Bubshait, S.; Sallout, M.; Al-Ghamdi, S. Dental Fear and Patient Preference for Emergency Dental Treatment Among Adults in COVID-19 Quarantine Centers in Dammam, Saudi Arabia. Patient Prefer. Adherence 2021, 15, 1707. Available online: https://www.dovepress.com/dental-fear-and-patient-preference-for-emergency-dental-treatment-amon-peer-reviewed-fulltext-article-PPA (accessed on 18 June 2021). [CrossRef] [PubMed]
- Kim, D.; Ko, J.-H.; Peck, K.R.; Baek, J.Y.; Moon, H.-W.; Ki, H.K. A COVID-19 Exposure at a Dental Clinic Where Healthcare Workers Routinely Use Particulate Filtering Respirators. Int. J. Environ. Res. Public Health 2021, 18, 6481. Available online: https://www.mdpi.com/1660-4601/18/12/6481 (accessed on 18 June 2021). [CrossRef] [PubMed]
- Lo, N.G.; Bizzoca, M.E.; Lo, M.L.; Campisi, G. The Management of Dental Practices in the Post-COVID 19 Era: An Economic and Operational Perspective. Int. J. Environ. Res. Public Health 2020, 17, 8905. Available online: https://www.mdpi.com/1660-4601/17/23/8905 (accessed on 18 June 2021).
- Uhlen, M.M.; Ansteinsson, V.E.; Stangvaltaite-Mouhat, L.; Korzeniewska, L.; Skudutyte-Rysstad, R.; Shabestari, M. Psychological impact of the COVID-19 pandemic on dental health personnel in Norway. BMC Health Serv. Res. 2021, 21, 420. Available online: https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-021-06443-y (accessed on 18 June 2021). [CrossRef] [PubMed]
- Sinjari, B.; Rexhepi, I.; Santilli, M.; D′Addazio, G.; Chiacchiaretta, P.; Di Carlo, P.; Caputi, S. The Impact of COVID-19 Related Lockdown on Dental Practice in Central Italy—Outcomes of A Survey. Int. J. Environ. Res. Public Health 2020, 17, 5780. Available online: https://www.mdpi.com/1660-4601/17/16/5780 (accessed on 18 June 2021). [CrossRef]
- Al-Khalifa, K.S.; Al-Sheikh, R.; Al-Swuailem, A.S.; Alkhalifa, M.S.; Al-Johani, M.H.; Al-Moumen, S.A. Pandemic preparedness of dentists against coronavirus disease: A Saudi Arabian experience. PLoS ONE 2020, 15, 0237630. Available online: https://dx.plos.org/10.1371/journal.pone.0237630 (accessed on 18 June 2021).
- Bizzoca, M.E.; Campisi, G.; Lo, M.L. Covid-19 Pandemic: What Changes for Dentists and Oral Medicine Experts? A Narrative Review and Novel Approaches to Infection Containment. Int. J. Environ. Res. Public Health 2020, 17, 3793. Available online: https://www.mdpi.com/1660-4601/17/11/3793 (accessed on 18 June 2021). [CrossRef]
- Kamran, R.; Saba, K.; Azam, S. Impact of COVID-19 on Pakistani dentists: A nationwide cross sectional study. BMC Oral Health 2021, 21, 59. Available online: https://bmcoralhealth.biomedcentral.com/articles/10.1186/s12903-021-01413-6 (accessed on 18 June 2021). [CrossRef]
- Rahman, N.; Nathwani, S.; Kandiah, T. Teledentistry from a patient perspective during the coronavirus pandemic. Br. Dent. J. 2020. Available online: https://www.nature.com/articles/s41415-020-1919-6 (accessed on 18 June 2021). [CrossRef]
- Maqsood, A.; Sadiq, M.S.K.; Mirza, D.; Ahmed, N.; Lal, A.; Halim, M.S. The Teledentistry, Impact, Current Trends, and Application in Dentistry: A Global Study. Biomed. Res. Int. 2021, 2021, 5437237. Available online: https://www.hindawi.com/journals/bmri/2021/5437237/ (accessed on 18 June 2021). [CrossRef]
- Ge, Z.; Yang, L.; Xia, J.; Fu, X.; Zhang, Y. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J. Zhejiang Univ. B 2020, 21, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jungo, S.; Moreau, N.; Mazevet, M.E.; Ejeil, A.-L.; Biosse Duplan, M.; Salmon, B. Prevalence and risk indicators of first-wave COVID-19 among oral health-care workers: A French epidemiological survey. PLoS ONE 2021, 16, e0246586. [Google Scholar] [CrossRef]
- Ammar, N.; Aly, N.M.; Folayan, M.O.; Khader, Y.; Virtanen, J.I.; Al-Batayneh, O.B. Behavior change due to COVID-19 among dental academics—The theory of planned behavior: Stresses, worries, training, and pandemic severity. PLoS ONE 2020, 15, e0239961. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | N | % | |
|---|---|---|---|
| Age | 10–25 25–35 35–45 45–55 55–65 65–75 | 80 197 134 132 95 73 | 11.3 27.7 18.8 18.6 13.4 10.3 |
| Gender | Male Female | 380 331 | 53.4 46.6 |
| Education | Educated Non-educated | 359 352 | 50.5 49.5 |
| Questions | Responses | |
|---|---|---|
| Yes | No | |
| Was the clinic’s security wearing mask? | 584 | 127 |
| Did you receive preventive measures at the clinic’s entrance? | 453 | 258 |
| Was proper social distancing practiced at the clinic? | 591 | 120 |
| Did you arrive at the clinic with Dental emergency? | 547 | 164 |
| Was PPE provided to you for your safety? | 147 | 564 |
| Was the dental assistant wearing proper PPE? | 463 | 248 |
| Was the dentist wearing proper PPE? | 553 | 158 |
| Was proper medical history taken? | 605 | 106 |
| Were infection control measures performed in the waiting area? | 410 | 301 |
| Are you satisfied with the services provided to you? | 530 | 181 |
| Variables | Unstandardized Coefficients | Standardized Coefficients | t | p-Value | 95.0% Confidence Interval for B | Collinearity Statistics | |||
|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | Tolerance | VIF | |||
| Age | −0.005 | 0.005 | −0.039 | −1.064 | 0.288 | −0.014 | 0.004 | 0.997 | 1.003 |
| Gender | −0.076 | 0.014 | −0.203 | −5.506 | ** 0.001 | −0.104 | −0.049 | 0.994 | 1.006 |
| Education | 0.010 | 0.014 | 0.026 | 0.718 | 0.473 | −0.017 | 0.037 | 0.997 | 1.003 |
| Variables | N | % | |
|---|---|---|---|
| Age | 20–25 25–35 35–45 45–55 55–65 | 218 297 102 32 62 | 30.7 41.8 14.3 4.5 8.7 |
| Gender | Male Female | 347 364 | 48.8 51.2 |
| Experience | 0–5 years 5–10 years 10–15 years 15–20 years 20–25 years 25–30 years Above 30 years | 241 115 142 88 56 63 3 | 33.9 16.2 20.0 12.4 7.9 8.9 0.8 |
| Qualification | General Dentist Specialist Consultant | 332 286 93 | 46.7 40.2 13.1 |
| Variables | Df | Mean Square | p-Value |
|---|---|---|---|
| Financial Impact | 1 | 6.903 | 0.001 |
| Psychological Impact | 1 | 6.357 | 0.001 |
| Patient’s Satisfaction | 1 | 0.611 | 0.001 |
| Hygiene | 1 | 0.434 | 0.001 |
| Patient Management | 1 | 0.245 | 0.013 |
| Lockdown | 1 | 1.038 | 0.001 |
| Perspective | 1 | 0.411 | 0.010 |
| Post-COVID-19 | 1 | 0.039 | 0.564 |
| Variables | Df | Mean Square | p-Value |
|---|---|---|---|
| Financial Impact | 4 | 9.939 | 0.001 |
| Psychological Impact | 4 | 1.875 | 0.001 |
| Patient’s Satisfaction | 4 | 0.086 | 0.001 |
| Hygiene | 4 | 0.639 | 0.001 |
| Patient Management | 4 | 0.926 | 0.001 |
| Lockdown | 4 | 0.342 | 0.001 |
| Perspective | 4 | 0.099 | 0.168 |
| Post-COVID-19 | 4 | 3.560 | 0.001 |
| Variables | Df | Mean Square | p-Value |
|---|---|---|---|
| Financial Impact | 2 | 14.568 | 0.001 |
| Psychological Impact | 2 | 4.239 | 0.001 |
| Patient’s Satisfaction | 2 | 0.142 | 0.001 |
| Hygiene | 2 | 0.273 | 0.001 |
| Patient Management | 2 | 0.101 | 0.077 |
| Lockdown | 2 | 1.231 | 0.001 |
| Perspective | 2 | 0.376 | 0.002 |
| Post-COVID-19 | 2 | 2.940 | 0.001 |
| Variables | Df | Mean Square | p-Value |
|---|---|---|---|
| Financial Impact | 6 | 5.038 | 0.001 |
| Psychological Impact | 6 | 2.360 | 0.001 |
| Patient’s Satisfaction | 6 | 0.035 | 0.001 |
| Hygiene | 6 | 0.031 | 0.028 |
| Patient Management | 6 | 0.211 | 0.001 |
| Lockdown | 6 | 0.907 | 0.001 |
| Perspective | 6 | 0.378 | 0.001 |
| Post-COVID-19 | 6 | 0.473 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wajeeh, S.; Lal, A.; Ahmed, N.; Khalil, M.I.; Maqsood, A.; Alshammari, A.M.M.; Alshammari, A.Z.; Alsharari, M.M.M.; Alrushaydan, A.H.; Alruwaili, A.F.; et al. Operational Implications and Risk Assessment of COVID-19 in Dental Practices. Int. J. Environ. Res. Public Health 2021, 18, 12244. https://doi.org/10.3390/ijerph182212244
Wajeeh S, Lal A, Ahmed N, Khalil MI, Maqsood A, Alshammari AMM, Alshammari AZ, Alsharari MMM, Alrushaydan AH, Alruwaili AF, et al. Operational Implications and Risk Assessment of COVID-19 in Dental Practices. International Journal of Environmental Research and Public Health. 2021; 18(22):12244. https://doi.org/10.3390/ijerph182212244
Chicago/Turabian StyleWajeeh, Saba, Abhishek Lal, Naseer Ahmed, Md. Ibrahim Khalil, Afsheen Maqsood, Akram Mojidea M Alshammari, Abdulelah Zaid Alshammari, Meshari Musallam Mohammed Alsharari, Abdulelah Hamdan Alrushaydan, Abdulaziz Fandi Alruwaili, and et al. 2021. "Operational Implications and Risk Assessment of COVID-19 in Dental Practices" International Journal of Environmental Research and Public Health 18, no. 22: 12244. https://doi.org/10.3390/ijerph182212244