
Trends of Myocarditis and Endocarditis Cases before, during, and after the First Complete COVID-19-Related Lockdown in 2020 in France

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Hospitalization Data
2.2. Myocarditis and Endocarditis
2.3. Study Design
2.4. Statistical Analysis
3. Results
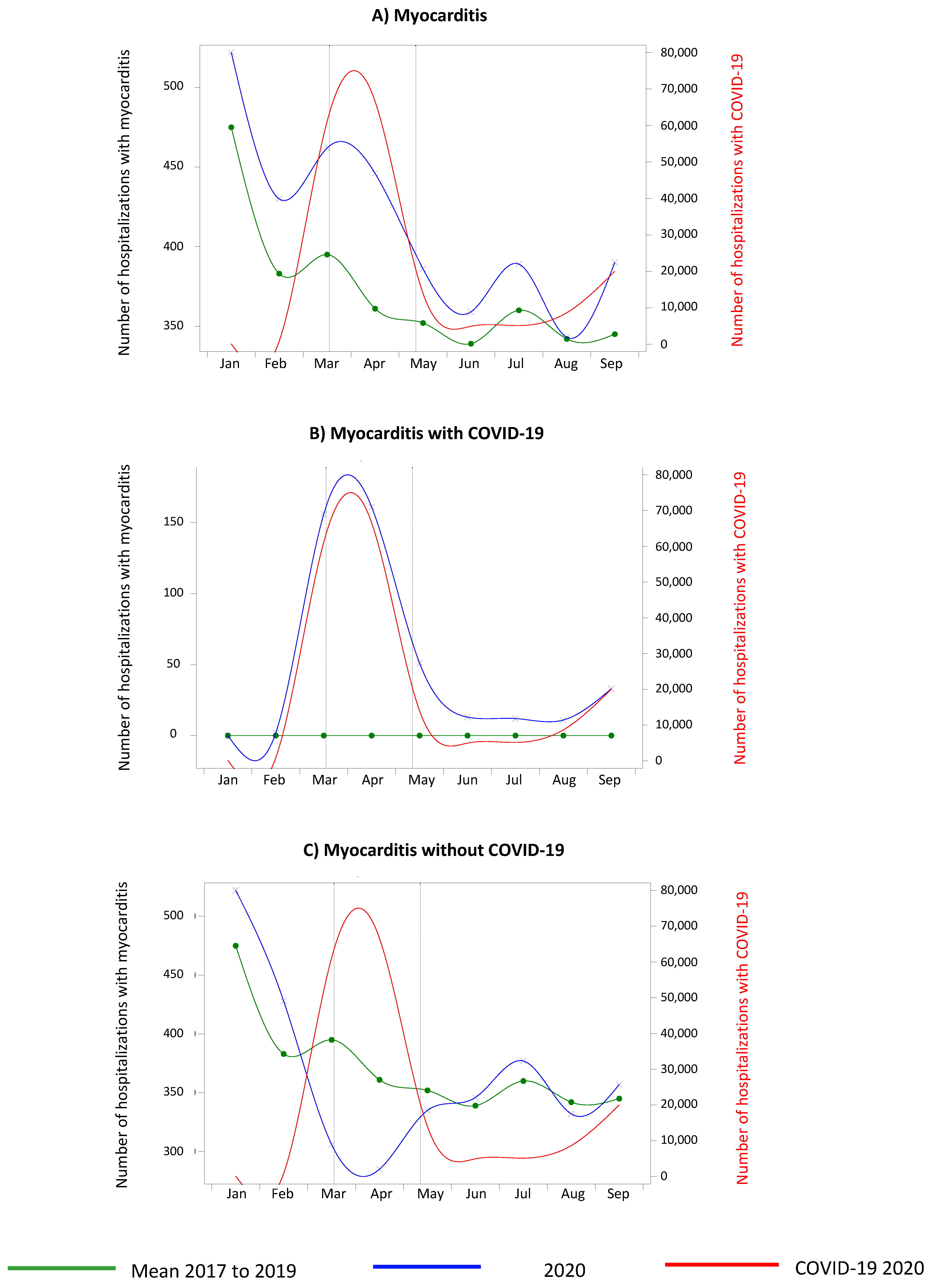
3.1. Myocarditis
3.2. Endocarditis
3.3. Clinical Characteristics of Patients According to COVID-19 Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
References
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Lond. Engl. 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Fried, J.A.; Ramasubbu, K.; Bhatt, R.; Topkara, V.K.; Clerkin, K.J.; Horn, E.; Rabbani, L.; Brodie, D.; Jain, S.S.; Kirtane, A.J.; et al. The Variety of Cardiovascular Presentations of COVID-19. Circulation 2020, 141, 1930–1936. [Google Scholar] [CrossRef] [Green Version]
- Modin, D.; Claggett, B.; Sindet-Pedersen, C.; Højbjerg Lassen, M.C.; Grundtvig Skaarup, K.; Stæhr Jensen, J.U.; Fralick, M.; Schou, M.; Lamberts, M.; Gerds, T.; et al. Acute COVID-19 and the Incidence of Ischemic Stroke and Acute Myocardial Infarction. Circulation 2020, 142, 2080–2082. [Google Scholar] [CrossRef]
- Thakkar, S.; Arora, S.; Kumar, A.; Jaswaney, R.; Faisaluddin, M.; Ud Din, M.A.; Shariff, M.; Barssoum, K.; Patel, H.P.; Nirav, A.; et al. A Systematic Review of the Cardiovascular Manifestations and Outcomes in the Setting of Coronavirus-19 Disease. Clin. Med. Insights Cardiol. 2020, 14, 1179546820977196. [Google Scholar] [CrossRef]
- O’Hearn, M.; Liu, J.; Cudhea, F.; Micha, R.; Mozaffarian, D. Coronavirus Disease 2019 Hospitalizations Attributable to Cardiometabolic Conditions in the United States: A Comparative Risk Assessment Analysis. J. Am. Heart Assoc. 2021, 10, e019259. [Google Scholar] [CrossRef]
- Mesnier, J.; Cottin, Y.; Coste, P.; Ferrari, E.; Schiele, F.; Lemesle, G.; Thuaire, C.; Angoulvant, D.; Cayla, G.; Bouleti, C.; et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: A registry study. Lancet Public Health 2020, 5, e536–e542. [Google Scholar] [CrossRef]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Perrone Filardi, P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Solomon, M.D.; McNulty, E.J.; Rana, J.S.; Leong, T.K.; Lee, C.; Sung, S.H.; Ambrosy, A.P.; Sidney, S.; Go, A.S. The Covid-19 Pandemic and the Incidence of Acute Myocardial Infarction. N. Engl. J. Med. 2020, 383, 691–693. [Google Scholar] [CrossRef] [PubMed]
- Doolub, G.; Wong, C.; Hewitson, L.; Mohamed, A.; Todd, F.; Gogola, L.; Skyrme-Jones, A.; Aziz, S.; Sammut, E.; Dastidar, A. Impact of COVID-19 on inpatient referral of acute heart failure: A single-centre experience from the south-west of the UK. ESC Heart Fail. 2021, 8, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Rey, J.R.; Caro-Codón, J.; Rosillo, S.O.; Iniesta, A.M.; Castrejón-Castrejón, S.; Marco-Clement, I.; Martín-Polo, L.; Merino-Argos, C.; Rodríguez-Sotelo, L.; García-Veas, J.M.; et al. Heart failure in COVID-19 patients: Prevalence, incidence and prognostic implications. Eur. J. Heart Fail. 2020, 22, 2205–2215. [Google Scholar] [CrossRef] [PubMed]
- Mariet, A.S.; Giroud, M.; Benzenine, E.; Cottenet, J.; Roussot, A.; Aho-Glélé, L.S.; Tubert-Bitter, P.; Béjot, Y.; Quantin, C. Hospitalizations for stroke in France during the COVID-19 pandemic before, during and after the national lockdown. Stroke 2020, 52, 1362–1369. [Google Scholar] [CrossRef]
- Liu, R.; Zhao, J.; Zhao, M.F. The global impact of COVID-19 on acute stroke care. CNS Neurosci. Ther. 2020, 26, 1103–1105. [Google Scholar] [CrossRef] [PubMed]
- Kansagara, D.; Englander, H.; Salanitro, A.; Kagen, D.; Theobald, C.; Freeman, M.; Kripalani, S. Risk Prediction Models for Hospital Readmission: A Systematic Review; VA Evidence-based Synthesis Program Reports; Department of Veterans Affairs (US): Washington, DC, USA, 2011. Available online: http://www.ncbi.nlm.nih.gov/books/NBK82578/ (accessed on 23 March 2022).
- D’Anna, L.; Brown, M.; Oishi, S.; Ellis, N.; Brown, Z.; Bentley, P.; Drumm, B.; Halse, O.; Jamil, S.; Jenkins, H.; et al. Impact of National Lockdown on the Hyperacute Stroke Care and Rapid Transient Ischaemic Attack Outpatient Service in a Comprehensive Tertiary Stroke Centre During the COVID-19 Pandemic. Front. Neurol. 2021, 12, 627493. [Google Scholar] [CrossRef]
- Zhao, J.; Li, H.; Kung, D.; Fisher, M.; Shen, Y.; Liu, R. Impact of the COVID-19 Epidemic on Stroke Care and Potential Solutions. Stroke 2020, 51, 1996–2001. [Google Scholar] [CrossRef]
- Bader, F.; Manla, Y.; Atallah, B.; Starling, R. Heart failure and COVID-19. Heart Fail. Rev. 2021, 26, 1–10. [Google Scholar] [CrossRef]
- Dong, N.; Cai, J.; Zhou, Y.; Liu, J.; Li, F. End-Stage Heart Failure with COVID-19: Strong Evidence of Myocardial Injury by 2019-nCoV. JACC Heart Fail. 2020, 8, 515–517. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Lindner, D.; Fitzek, A.; Bracminger, H. Association of cardiac infection with SARS-Cov-2 in confirmed COVID-19 autopsy cases. JAMA Cardiol. 2020, 5, 1281–1285. [Google Scholar] [CrossRef]
- Giustino, G.; Pinney, S.P.; Lala, A.; Reddy, V.Y.; Johnston-Cox, H.A.; Mechanick, J.I.; Halperin, J.L.; Fuster, V. Coronavirus and Cardiovascular Disease, Myocardial Injury, and Arrhythmia: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 76, 2011–2023. [Google Scholar] [CrossRef] [PubMed]
- Bonow, R.O.; Fonarow, G.C.; O’Gara, P.T.; Yancy, C.W. Association of coronavirus disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. 2020, 7, 751–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, I.C.; Kim, J.Y.; Kim, H.A.; Han, S. COVID-19 related myocarditis in a 21-year-old female patient. Eur. Heart J. 2020, 41, 1859. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Lupi, L.; Zaccone, G. Cardiac involvement in a patIent with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef] [Green Version]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Wenzel, P.; Kopp, S.; Gobel Swenzel, P.; Kopp, S.; Gobel, S.; Jansen, T.; Geyer, M.; Hahn, F.; Kreitner, K.; Escher, F.; et al. Evidence of SARS-Cov-2 mRNA in endomyocardial biopsies of patiens wih clinically suspected myocarditis tested negative for COVID-19 in nasopharyngeal swab. Cardiovasc. Res. 2020, 116, 1661–1663. [Google Scholar] [CrossRef]
- Escher, F.; Pietsch, H.; Aleshcheva, G.; Bock, T.; Baumeier, C.; Elsaesser, A.; Wenzel, P.; Hamm, C.; Westenfeld, R.; Schultheiss, M.; et al. Detection of viral SARS-Cov-2 genomes and histopathological changes in endomyocardial biopsies. ESC Heart Fail. 2020, 7, 2440–2447. [Google Scholar] [CrossRef]
- Ma, K.L.; Liu, Z.H.; Cao, C.; Liu, M.; Liao, J.; Zou, J.; Kong, L.; Wan, K.; Zhang, J.; Wang, Q.; et al. COVID-19 myocarditis and severity factors: An adult cohort study. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Zhao, J.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac involvement in patients recovered from COVID-19, identified using magnetic resonance imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered from Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Starekova, J.; Bluemke, D.A.; Bradham, X.S.; Eckhardt, L.; Grist, T.M.; Kusmirek, J.A.; Purtell, C.S.; Schiebler, M.L.; Reeder, S.B. Evaluation for myocarditis in competitive student athletes recovering from coronavirus disease 2019 with cardiac magnetic resonance imaging. JAMA Cardiol. 2021, 6, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomasoni, D.; Italia, L.; Adamo, M.; Inciardi, R.M.; Lombardi, C.M.; Solomon, S.D.; Metra, M. COVID-19 and heart failure: From infection to inflammation and angiotension II stimulation. Searching for evidence from a new disease. Eur. Soc. Cardiol. 2020, 22, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhou, Y.; Wang, D.W. SARS-CoV-2: A potential novel etiology of fulminant myocarditis. Herz 2020, 45, 230–232. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.; Shao, F.; Bao, B.; Ma, X.; Xu, Z.; You, J.; Zhao, P.; Liu, Y.; Ng, M.; Cui, H.; et al. Clinical Manifestation and Neonatal Outcomes of Pregnant Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. Open Forum Infect. Dis. 2020, 7, a283. [Google Scholar] [CrossRef]
- Deng, Q.; Hu, B.; Zhang, Y.; Wang, H.; Zhou, X.; Hu, W.; Cheng, Y.; Yan, J.; Ping, H.; Zhou, Q. Suspected myocardial injury in patients with COVID-19: Evidence from front-line clinical observation in Wuhan, China. Int. J. Cardiol. 2020, 311, 116–121. [Google Scholar] [CrossRef]
- Knight, D.S.; Kotecha, T.; Razvi, Y.; Chacko, L.; Brown, J.T.; Jeetley, P.S.; Goldring, J.; Jacobs, M.; Lamb, L.E.; Negus, R.; et al. COVID-19: Myocardial injury in survivors. Circulation 2020, 142, 1120–1122. [Google Scholar] [CrossRef]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T.; Chahal, C.A.A. Recognizing COVID-19-related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm. 2020, 17, 1463–1471. [Google Scholar] [CrossRef]
- Kumanayaka, D.; Mutyala, M.; Reddy, D.V.; Slim, J. Coronavirus Disease 2019 Infection as a Risk Factor for Infective Endocarditis. Cureus 2021, 13, e14813. [Google Scholar] [CrossRef]
- Siepmann, T.; Sedghi, A.; Simon, E.; Winzer, S.; Barlinn, J.; de With, K.; Mirow, L.; Wolz, M.; Gruenewald, T.; Schroettner, P.; et al. Increased risk of acute stroke among patients with severe COVID-19: A multicenter study and meta-analysis. Eur. J. Neurol. 2021, 28, 238–347. [Google Scholar] [CrossRef]
- Abbasi, J. Researchers Investigate What COVID-19 Does to the Heart. JAMA 2021, 325, 808–811. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Garcia, J.; Jaladanki, S.; Rivas-Lasarte, M.; Cagliostro, M.; Gapta, A.; Joshi, A.; Ting, P.; Mitter, S.S.; Bagiella, E.; Mancini, D.; et al. New heart failure diagnoses among patients hospitalized for COVID-19. JACC 2021, 77517, 2258–2262. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Fonarow, G.C. Coronavirus disease 2019 (COVID-19) and the heart. Is heart failure the next chapter ? JAMA Cardiol. 2020, 5, 1216–1217. [Google Scholar] [CrossRef] [PubMed]
- Block, J.P.; Boehmer, T.K.; Forrest, C.B.; Carton, T.W.; Lee, G.M.; Ajani, U.A.; Christakis, D.A.; Cowell, L.G.; Draper, C.; Ghildayal, N.; et al. Cardiac Complications After SARS-CoV-2 Infection and mRNA COVID-19 Vaccination-PCORnet, United States, January 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 517–523. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| COVID-19 + N (%) | COVID-19 − N (%) | p-Value | |
|---|---|---|---|
| Myocarditis (n = 836) | 322 | 514 | |
| Age, years | |||
| Mean (SD) | 61.1 (19.9) | 50.2 (20.4) | <10−4 |
| Sex | 0.0068 | ||
| Women | 104 (32.3) | 214 (41.6) | |
| Men | 218 (67.7) | 300 (58.4) | |
| Hypertension | 115 (35.7) | 101 (19.7) | <10−4 |
| Diabetes | 75 (23.3) | 38 (7.4) | <10−4 |
| Obesity | 57 (17.7) | 53 (10.3) | 0.0021 |
| Atrial fibrillation | 62 (19.3) | 61 (11.9) | 0.0033 |
| In-hospital mortality | 76 (23.6) | 26 (5.1) | <10−4 |
| Endocarditis (n = 1473) | 136 | 1337 | |
| Age, years | |||
| Mean (SD) | 69.8 (15.2) | 71.0 (14.3) | 0.32 |
| Sex | 0.079 | ||
| Women | 33 (24.3) | 422 (31.6) | |
| Men | 103 (75.7) | 915 (68.5) | |
| Hypertension | 72 (52.9) | 573 (42.9) | 0.024 |
| Diabetes | 39 (28.7) | 348 (26.0) | 0.50 |
| Obesity | 21 (15.4) | 157 (11.7) | 0.21 |
| Atrial fibrillation | 43 (31.6) | 484 (36.2) | 0.29 |
| In-hospital mortality | 43 (31.6) | 214 (16.0) | <10−4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pommier, T.; Benzenine, E.; Bernard, C.; Mariet, A.-S.; Béjot, Y.; Giroud, M.; Morgant, M.-C.; Steinmetz, E.; Guenancia, C.; Bouchot, O.; et al. Trends of Myocarditis and Endocarditis Cases before, during, and after the First Complete COVID-19-Related Lockdown in 2020 in France. Biomedicines 2022, 10, 1231. https://doi.org/10.3390/biomedicines10061231
Pommier T, Benzenine E, Bernard C, Mariet A-S, Béjot Y, Giroud M, Morgant M-C, Steinmetz E, Guenancia C, Bouchot O, et al. Trends of Myocarditis and Endocarditis Cases before, during, and after the First Complete COVID-19-Related Lockdown in 2020 in France. Biomedicines. 2022; 10(6):1231. https://doi.org/10.3390/biomedicines10061231
Chicago/Turabian StylePommier, Thibaut, Eric Benzenine, Chloé Bernard, Anne-Sophie Mariet, Yannick Béjot, Maurice Giroud, Marie-Catherine Morgant, Eric Steinmetz, Charles Guenancia, Olivier Bouchot, and et al. 2022. "Trends of Myocarditis and Endocarditis Cases before, during, and after the First Complete COVID-19-Related Lockdown in 2020 in France" Biomedicines 10, no. 6: 1231. https://doi.org/10.3390/biomedicines10061231