
Designing Mobile Epidemic Prevention Medical Stations for the COVID-19 Pandemic and International Medical Aid

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
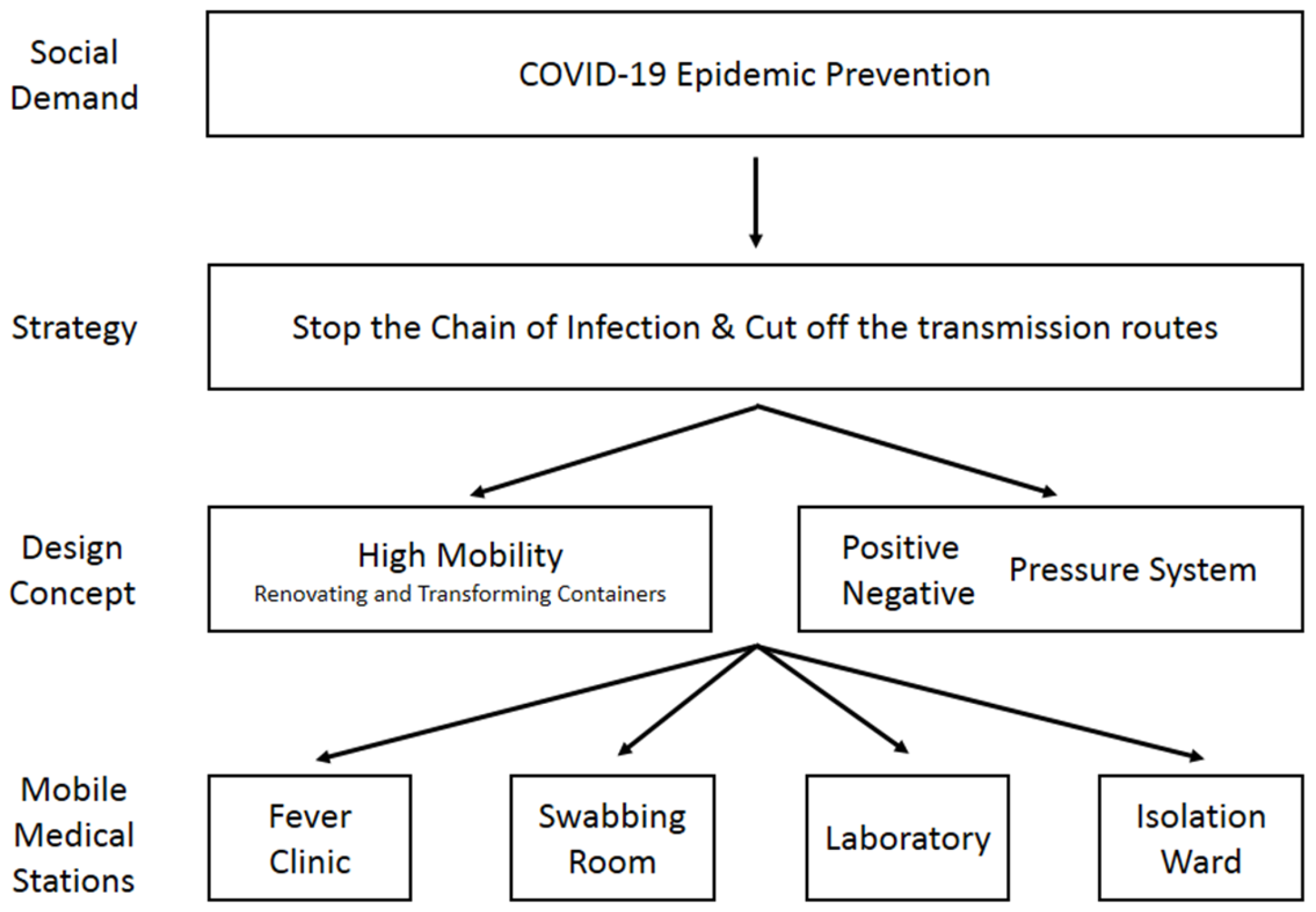
2.1. Design Concept: Mobility and Demands
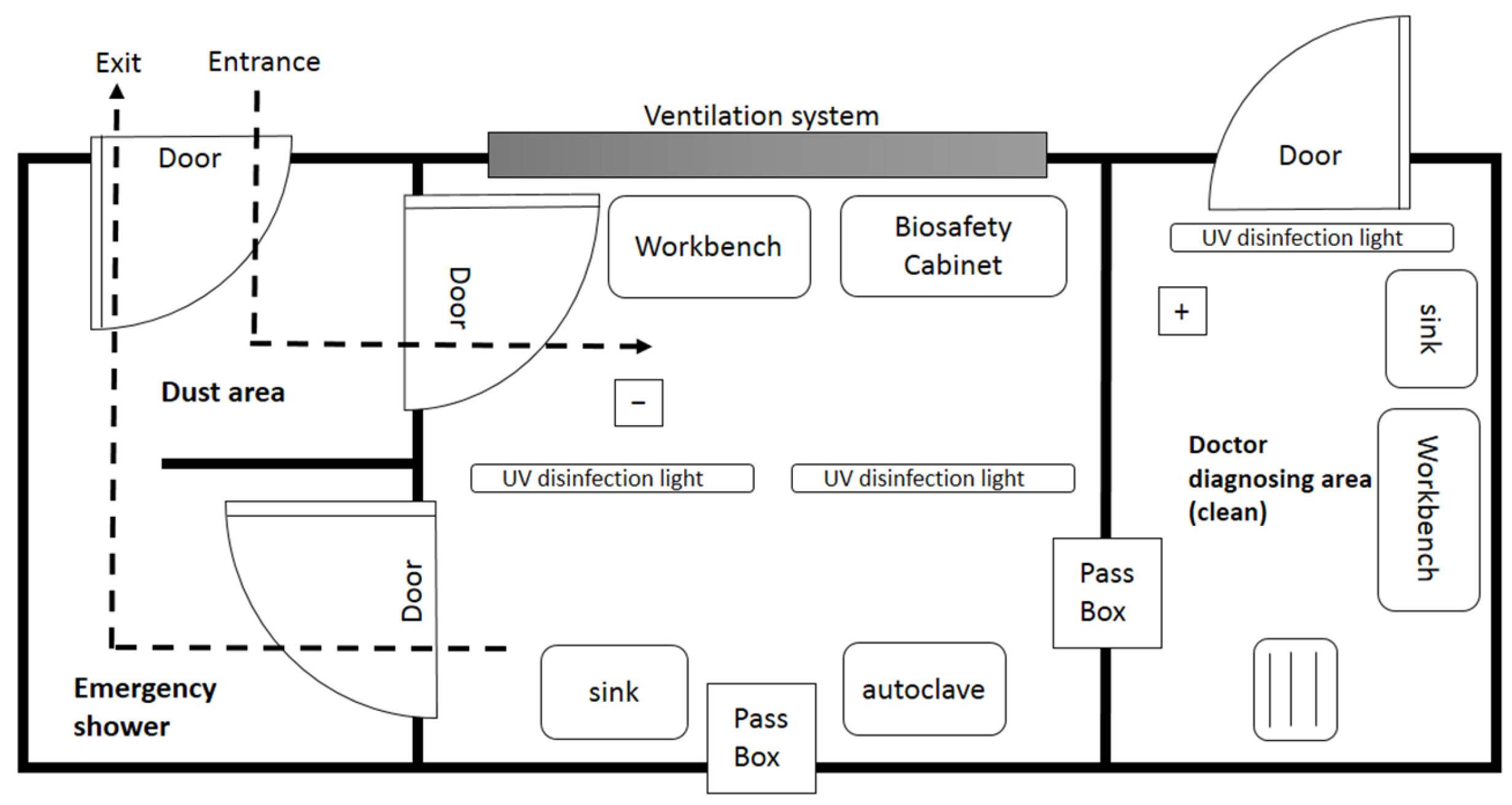
2.2. Cut off the Transmission Routes: Positive and Negative Pressure System
2.3. Specifications and Standards
- The negative pressure ventilation system must be tested by SGS (General Surveillance Society; report no. EKR2004706), and measurement results should be compliant with the Taiwan CDC (Centers for Disease Control) standard operating instructions for negative pressure isolation wards.
- The air-conditioning system must be able to switch between positive and negative pressure modes and be equipped with a HEPA (High-Efficiency Particulate Air) ventilation system. At the same time, the exhausted air must be sterilized at a high boiling temperature (100 °C).
- The medical stations must be equipped with a UV lamp and O3 ozone sterilization.
- Air-conditioning must be above 2.8 kW.
- A solar panel of 100 Ah, power 5000 VA/5000 W and lithium battery above 2750 mAh must be used with an automatic generator for continuous operation.
- There must be a differential pressure gauge and sensor.
- Available 4G Wifi.
- Firefighting installation devices must be certificated by the Taiwan Standard for Installation of Fire Safety Equipments Based on Use and Occupancy.
- A CNS (Chinese National Standards-Taiwan) 14705 certified permit must be held for the cleanroom.
- TFTA (Taiwan Food and Drug Administration) certified permits must be held for medical electric hospital beds and equipment.
- A smart water heater and medical-grade air purifier must be present.
- A Taiwan Ministry of Health and Welfare construction license for renovating containers into negative pressure isolation wards must be obtained.
- A biosafety level 3 (BSL-3; P3) standard laboratory must be used.
- The laboratory must possess a Taiwan Ministry of Economic Affairs IPO (Intellectual Property Office) patent certificate.
3. Results
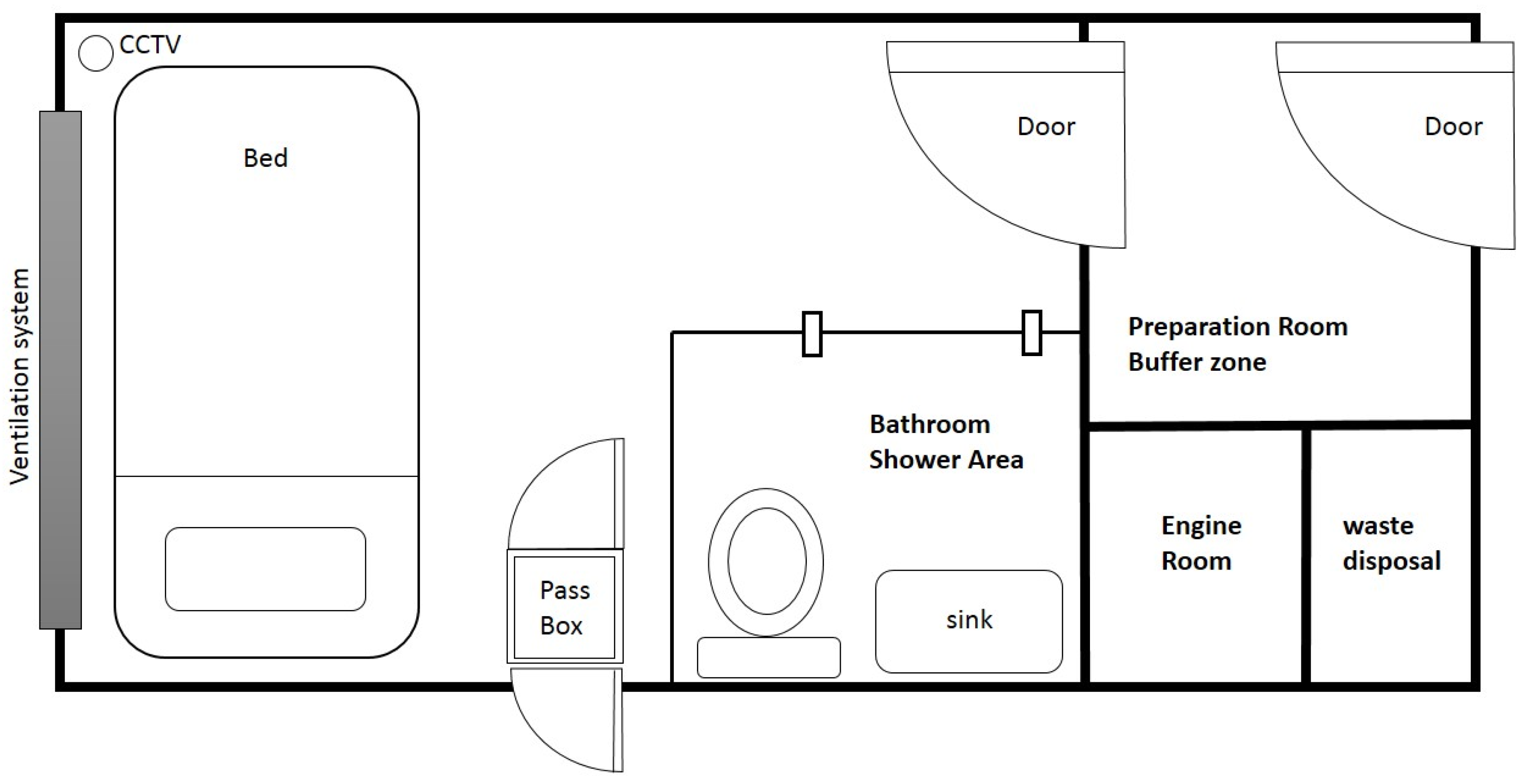
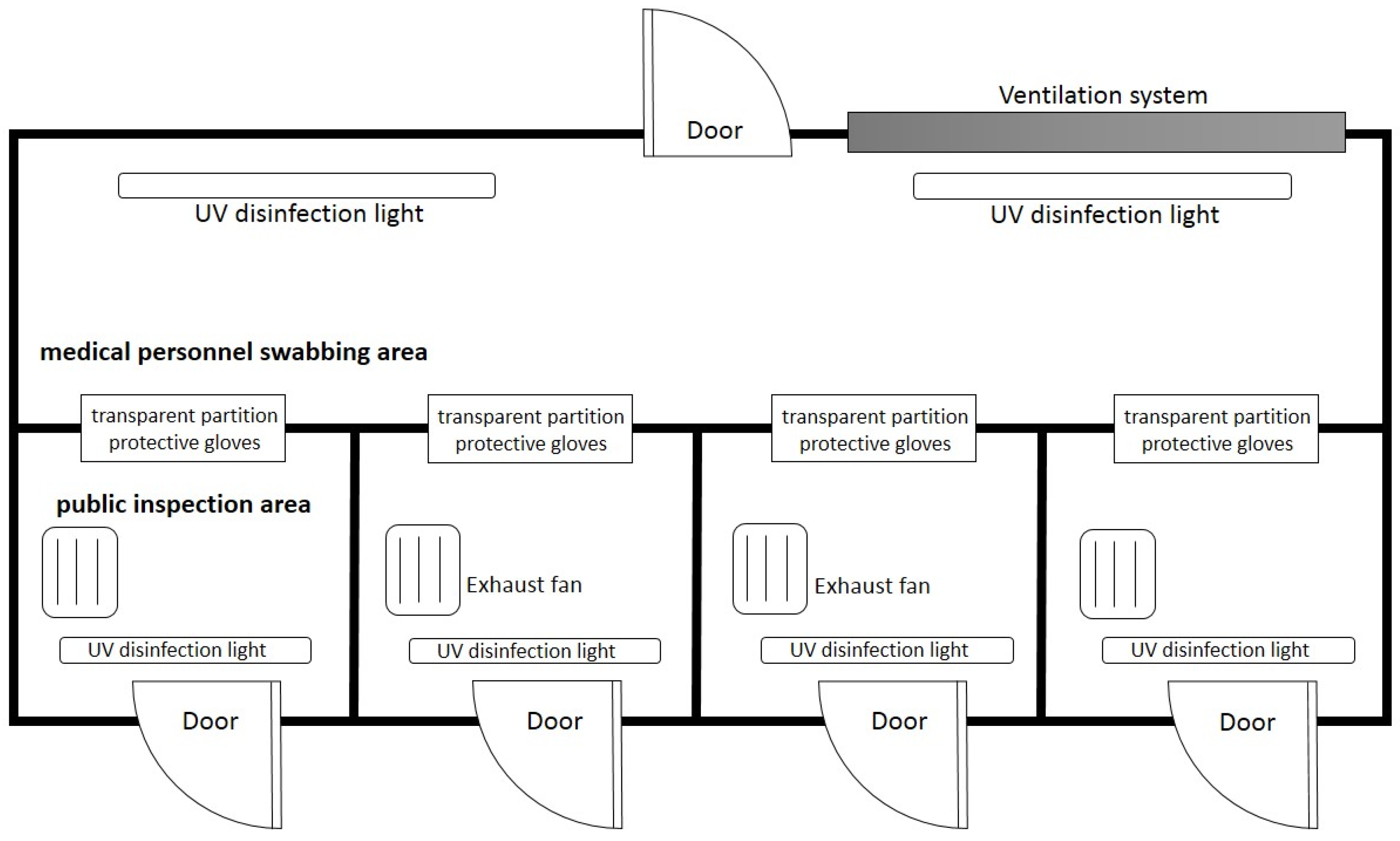
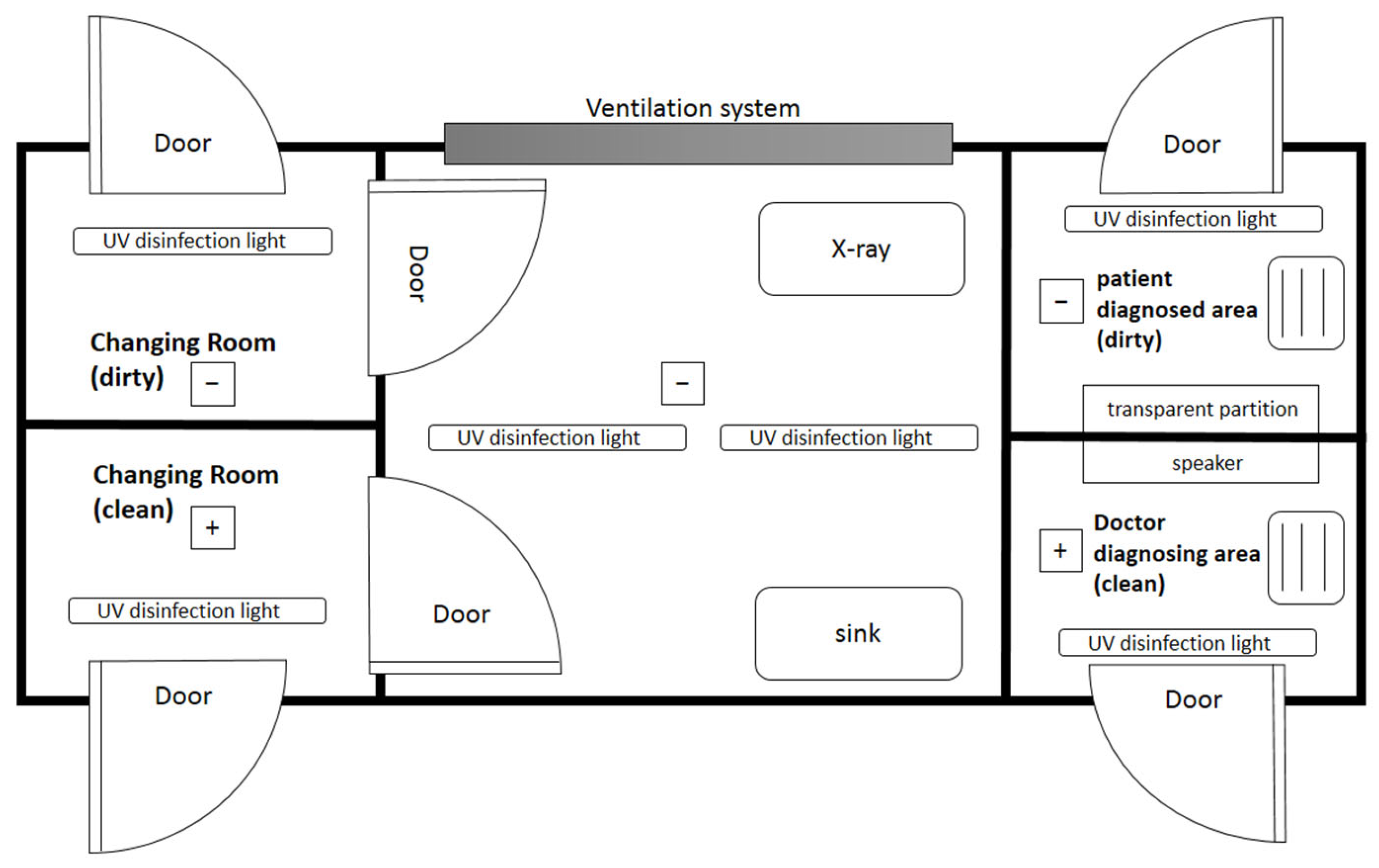
3.1. The Contents of Mobile Epidemic Prevention Medical Stations
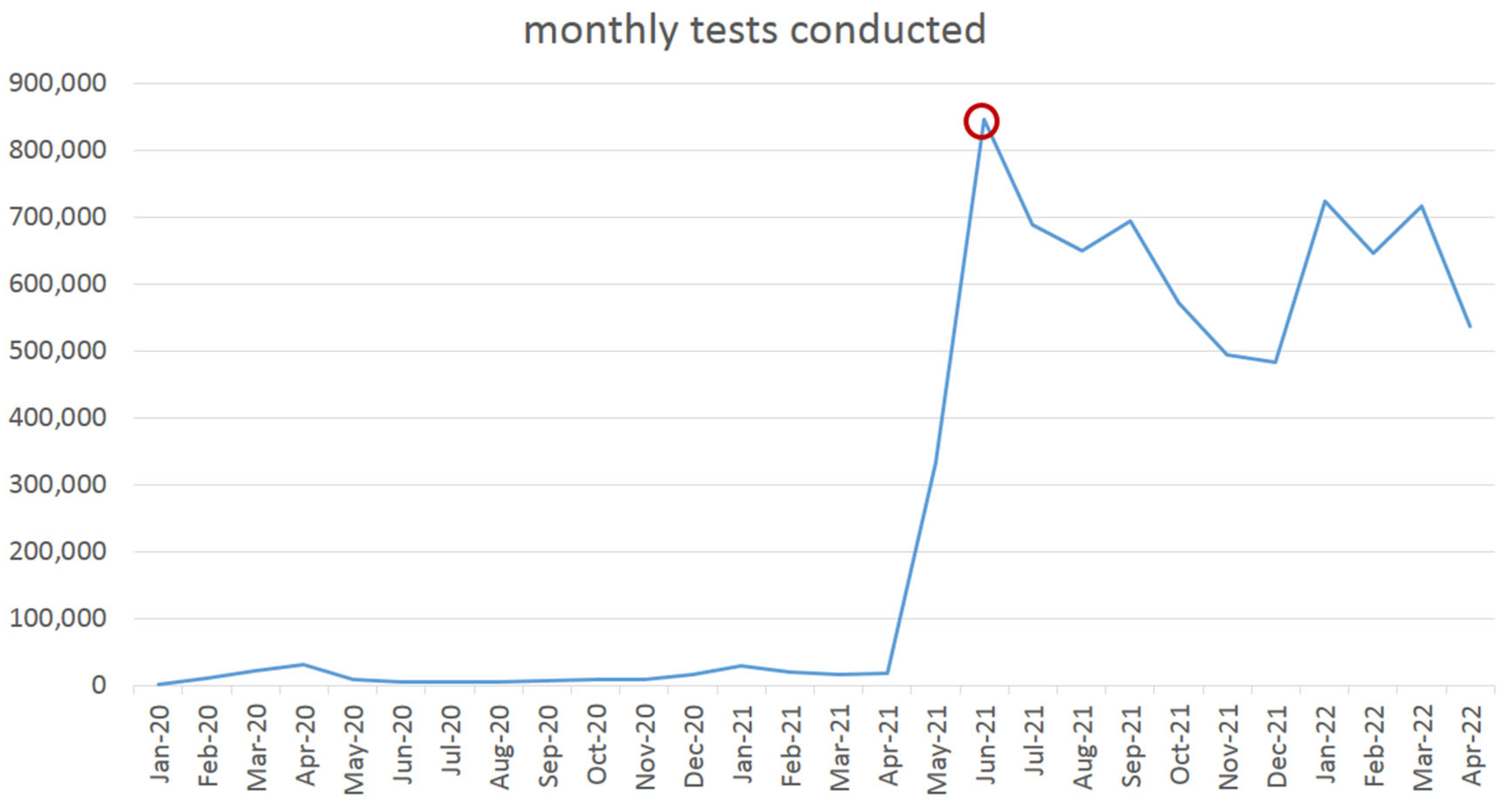
3.2. Practical Experience of Mobile Epidemic Prevention Medical Stations in Taiwan
3.3. International Medical Aid in Palau
4. Discussion
4.1. Maximizing the Use of Medical Resources with Flexibility
4.2. Comparison with Other Mobile Facilities: Advantages and Disadvantages
4.3. Economic Value
4.4. Difficulty and Future Possibility
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atzrodt, C.L.; Maknojia, I.; McCarthy, R.D.P.; Oldfield, T.M.; Po, J.; Ta, K.T.L.; Stepp, H.E.; Clements, T.P. A Guide to COVID-19: A global pandemic caused by the novel coronavirus SARS-CoV-2. FEBS J. 2020, 287, 3633–3650. [Google Scholar] [CrossRef]
- Sharma, A.; Ahmad Farouk, I.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef]
- Salian, V.S.; Wright, J.A.; Vedell, P.T.; Nair, S.; Li, C.; Kandimalla, M.; Tang, X.; Porquera, E.M.C.; Kalari, K.R.; Kandimalla, K.K. COVID-19 Transmission, Current Treatment, and Future Therapeutic Strategies. Mol. Pharm. 2021, 18, 754–771. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus (COVID-19) Dashboard Overview; WHO: Geneva, Switzerland, 2022; Available online: https://covid19.who.int (accessed on 16 February 2022).
- Burke, R.M.; Midgley, C.M.; Dratch, A.; Fenstersheib, M.; Haupt, T.; Holshue, M.; Ghinai, I.; Jarashow, M.C.; Lo, J.; McPherson, T.D.; et al. Active Monitoring of Persons Exposed to Patients with Confirmed COVID-19—United States, January–February 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 245–246. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Lf, A.-M.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [CrossRef]
- Rezaei, M.; Netz, R.R. Airborne virus transmission via respiratory droplets: Effects of droplet evaporation and sedimentation. Curr. Opin. Colloid Interface Sci. 2021, 55, 101471. [Google Scholar] [CrossRef]
- WHO. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations [Scientific Brief]; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions (accessed on 16 February 2022).
- Hsieh, C.-W.; Wang, M.; Wong, N.W.; Ho, L.K.-k. A whole-of-nation approach to COVID-19: Taiwan’s National Epidemic Prevention Team. Int. Political Sci. Rev. 2021, 42, 300–315. [Google Scholar] [CrossRef]
- Singh, D.; Kumar, V.; Kaur, M. Densely connected convolutional networks-based COVID-19 screening model. Appl. Intell. 2021, 51, 3044–3051. [Google Scholar] [CrossRef]
- Baker, C.M.; Chades, I.; McVernon, J.; Robinson, A.P.; Bondell, H. Optimal allocation of PCR tests to minimise disease transmission through contact tracing and quarantine. Epidemics 2021, 37, 100503. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, J.H.; Lee, H.; Moon, S.J.; Nam, E.W. COVID-19 screening center models in South Korea. J. Public Health Policy 2021, 42, 15–26. [Google Scholar] [CrossRef]
- Doerner, K.; Focke, A.; Gutjahr, W.J. Multicriteria tour planning for mobile healthcare facilities in a developing country. Eur. J. Oper. Res. 2007, 179, 1078–1096. [Google Scholar] [CrossRef]
- Malone, N.C.; Williams, M.M.; Smith Fawzi, M.C.; Bennet, J.; Hill, C.; Katz, J.N.; Oriol, N.E. Mobile health clinics in the United States. Int. J. Equity Health 2020, 19, 40. [Google Scholar] [CrossRef]
- Attipoe-Dorcoo, S.; Delgado, R.; Gupta, A.; Bennet, J.; Oriol, N.E.; Jain, S.H. Mobile health clinic model in the COVID-19 pandemic: Lessons learned and opportunities for policy changes and innovation. Int. J. Equity Health 2020, 19, 73. [Google Scholar] [CrossRef]
- Chen, X.; Lu, L.; Shi, J.; Zhang, X.; Fan, H.; Fan, B.; Qu, B.; Lv, Q.; Hou, S. Application and Prospect of a Mobile Hospital in Disaster Response. Disaster Med. Public Health Prep. 2020, 14, 377–383. [Google Scholar] [CrossRef]
- Labiris, G.; Fanariotis, M.; Christoulakis, C.; Petounis, A.; Kitsos, G.; Aspiotis, M.; Psillas, K. Tele-ophthalmology and conventional ophthalmology using a mobile medical unit in remote Greece. J. Telemed Telecare 2003, 9, 296–299. [Google Scholar] [CrossRef]
- WHO. COVID-19: Occupational Health and Safety for Health Workers [Interim Guidance]; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Wang, F.; Chaerasari, C.; Rakshit, D.; Permana, I.; Kusnandar. Performance Improvement of a Negative-Pressurized Isolation Room for Infection Control. Healthcare 2021, 9, 1081. [Google Scholar] [CrossRef]
- Al-Benna, S. Negative pressure rooms and COVID-19. J. Perioper. Pract. 2021, 31, 18–23. [Google Scholar] [CrossRef]
- Wang, H.; Mo, P.; Li, G.; Chen, P.; Liu, J.; Wang, F.; Zhang, Y.; Zhao, Q. Environmental virus surveillance in the isolation ward of COVID-19. J. Hosp. Infect. 2020, 105, 373–374. [Google Scholar] [CrossRef]
- Yeo, S.; Hosein, I.; McGregor-Davies, L. Use of HEPA filters to reduce the risk of nosocomial spread of SARS-CoV-2 via operating theatre ventilation systems. Br. J. Anaesth. 2020, 125, e361–e363. [Google Scholar] [CrossRef]
- Wang, Y.; Qiang, W.M.; Wang, C.; Wu, P.P.; Li, M.M.; Kong, Q.Q.; Yu, L.; Chen, L. Nursing management at a Chinese fever clinic during the COVID-19 pandemic. Int. Nurs. Rev. 2021, 68, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Artika, I.M.; Ma’roef, C.N. Laboratory biosafety for handling emerging viruses. Asian Pac. J. Trop. Biomed. 2017, 7, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, Y.; Liu, J.; Bailey, A.L.; Plante, K.S.; Plante, J.A.; Zou, J.; Xia, H.; Bopp, N.E.; Aguilar, P.V.; et al. A trans-complementation system for SARS-CoV-2 recapitulates authentic viral replication without virulence. Cell 2021, 184, 2229–2238.e13. [Google Scholar] [CrossRef] [PubMed]
- Nolte, K.B.; Muller, T.B.; Denmark, A.M.; Burstein, R.; Villalobos, Y.A. Design and Construction of a Biosafety Level 3 Autopsy Laboratory. Arch. Pathol. Lab. Med. 2020, 145, 407–414. [Google Scholar] [CrossRef]
- TCDC. COVID-19 Total Tests Conducted; Taiwan Centers for Disease Control: Taipei, China, 2022. Available online: https://sites.google.com/cdc.gov.tw/2019-ncov/taiwan (accessed on 16 February 2022).
- Paulmann, J. Conjunctures in the History of International Humanitarian Aid during the Twentieth Century. Humanit. Int. J. Hum. Rights Humanit. Dev. 2013, 4, 215–238. [Google Scholar] [CrossRef]
- Craig, A.T.; Heywood, A.E.; Hall, J. Risk of COVID-19 importation to the Pacific islands through global air travel. Epidemiol. Infect. 2020, 148, e71. [Google Scholar] [CrossRef]
- Ikerdeu, E.; Lyman, A.; Koshiba, C.; Tutii, I.; Whipps, V.; Ngirmang, K.; Osarch, S. Lessons from the Field: Interventions to Improve Health and Quality of Life to Address the NCD Crisis in Palau—Fostering Collaboration Across Sectors within the Government and Civil Society. Hawaii J. Health Soc. Welf. 2020, 79, 19–23. [Google Scholar]
- Shearer, F.M.; Walker, J.; Tellioglu, N.; McCaw, J.M.; McVernon, J.; Black, A.; Geard, N. Rapid assessment of the risk of SARS-CoV-2 importation: Case study and lessons learned. Epidemics 2021, 38, 100549. [Google Scholar] [CrossRef]
- Petrova, E.; Farinholt, T.; Joshi, T.P.; Moreno, H.; Al Mohajer, M.; Patel, S.M.; Petrosino, J.; Anandasabapathy, S. A Community-Based Management of COVID-19 in a Mobile Container Unit. Vaccines 2021, 9, 1362. [Google Scholar] [CrossRef]
- McMaster, D.; Clare, G. Designing a Mobile Eye Hospital to Support Health Systems in Resource-Scarce Environments. Disaster Med. Public Health Prep. 2021, 16, 1–5. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, M.-Z.; Chou, Y.-H.; Chang, Y.-Z.; Pai, J.-Y.; Bair, H.; Pai, S.; Yu, N.-C. Designing Mobile Epidemic Prevention Medical Stations for the COVID-19 Pandemic and International Medical Aid. Int. J. Environ. Res. Public Health 2022, 19, 9959. https://doi.org/10.3390/ijerph19169959
Gao M-Z, Chou Y-H, Chang Y-Z, Pai J-Y, Bair H, Pai S, Yu N-C. Designing Mobile Epidemic Prevention Medical Stations for the COVID-19 Pandemic and International Medical Aid. International Journal of Environmental Research and Public Health. 2022; 19(16):9959. https://doi.org/10.3390/ijerph19169959
Chicago/Turabian StyleGao, Mi-Zuo, Ying-Hsiang Chou, Yan-Zin Chang, Jar-Yuan Pai, Henry Bair, Sharon Pai, and Nai-Chi Yu. 2022. "Designing Mobile Epidemic Prevention Medical Stations for the COVID-19 Pandemic and International Medical Aid" International Journal of Environmental Research and Public Health 19, no. 16: 9959. https://doi.org/10.3390/ijerph19169959