
High Seroprevalence of SARS-CoV-2 in Mwanza, Northwestern Tanzania: A Population-Based Survey
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Target Population
2.2. Study Area
2.3. Sample Size Estimation and Sampling Technique
2.4. Eligibility Criteria
2.4.1. Inclusion Criteria
2.4.2. Exclusion Criteria
2.5. Sample Collection
2.6. Serological Testing
2.7. Survey Data Collection
2.8. Data Analysis
2.9. Infection Prevention Measures against SARS-CoV-2 Infection Taken during Data Collection
3. Results
3.1. Previous History of Signs and Symptoms of COVID-19
3.2. History of Chronic Illness
3.3. Seroprevalence of SARS-CoV-2 Antibodies
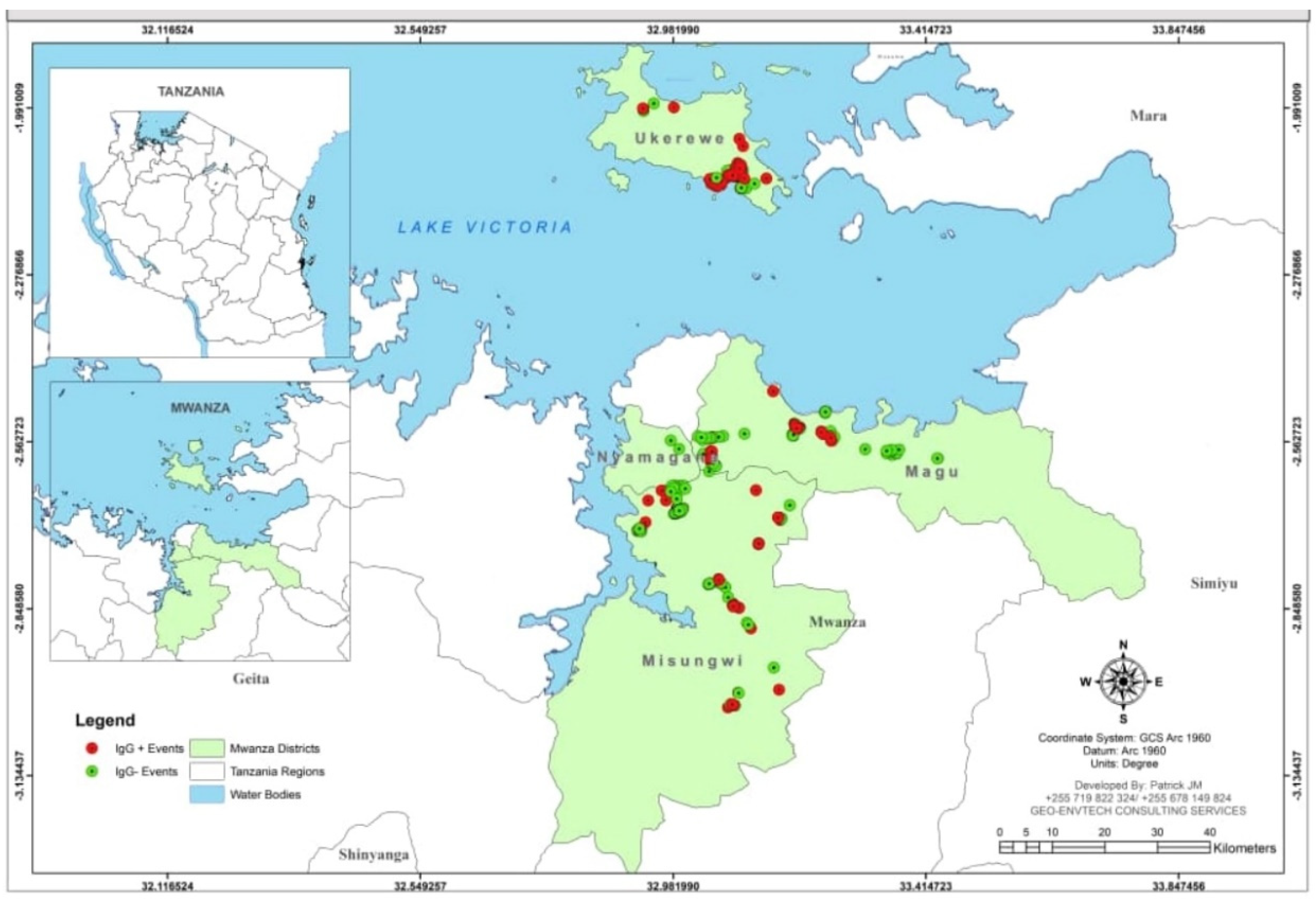
3.4. Geographical Distribution of the Participants Who Tested for IgG against SARS-CoV-2
3.5. Factors Associated with IgG Seropositivity among the Participants
3.6. Factors Associated with SARS-CoV-2 IgM Seropositivity among the Participants
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Musa, H.H.; Musa, T.H.; Musa, I.H.; Musa, I.H.; Ranciaro, A. Since January 2020 Elsevier Has Created a COVID-19 Resource Centre with Free Information in English and Mandarin on the Novel Coronavirus COVID-19. The COVID-19 Resource Centre Is Hosted on Elsevier Connect, The Company’s Public News and Information; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Gaye, B.; Khoury, S.; Cene, C.W.; Kingue, S.; N’Guetta, R.; Lassale, C.; Baldé, D.; Diop, I.B.; Dowd, J.B.; Mills, M.C.; et al. Socio-demographic and epidemiological consideration of Africa’s COVID-19 response: What is the possible pandemic course? Nat. Med. 2020, 26, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.; Hansen, K.S.; Kiragga, A.N.; Kambugu, A.; Kissa, J.; Mbonye, A.K. Predicting the impact of COVID-19 and the potential impact of the public health response on disease burden in Uganda. Am. J. Trop. Med. Hyg. 2020, 103, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Usuf, E.; Roca, A. Seroprevalence surveys in sub-Saharan Africa: What do they tell us? Lancet Glob. Health 2021, 9, e724–e725. [Google Scholar] [CrossRef]
- Tarimo, C.S.; Wu, J. The first confirmed case of COVID-19 in Tanzania: Recommendations based on lesson learned from China. Trop. Med. Health 2020, 48, 25. [Google Scholar] [CrossRef] [PubMed]
- Majiya, H.; Aliyu-Paiko, M.; Balogu, V.T.; Musa, D.A.; Salihu, I.M.; Kawu, A.A.; Bashir, Y.I.; Sani, R.A.; Baba, J.; Muhammad, A.T.; et al. Seroprevalence of COVID-19 in Niger State. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.08.04.20168112v1.abstract (accessed on 1 April 2022).
- World Bank Group. Tanzania Economic Update: Addressing the Impact of COVID-19 with a special section on the role of ICT. Afr. Reg. Macroecon. Trade Investig. Glob. Pract. 2020, 14, 82. [Google Scholar]
- Alkurt, G.; Murt, A.; Aydin, Z.; Tatli, O.; Agaoglu, N.B.; Irvem, A.; Aydin, M.; Karaali, R.; Gunes, M.; Yesilyurt, B.; et al. Seroprevalence of coronavirus disease 2019 (COVID-19) among health care workers from three pandemic hospitals of Turkey. PLoS ONE 2021, 16, e0247865. [Google Scholar] [CrossRef] [PubMed]
- Majiya, H.; Aliyu-Paiko, M.; Balogu, V.T. Seroprevalence of SARS-CoV-2 in Niger State: A Pilot Cross Sectional Study. medRxiv 2021. [Google Scholar] [CrossRef]
- Mulenga, L.B.; Hines, J.Z.; Fwoloshi, S.; Chirwa, L.; Siwingwa, M.; Yingst, S.; Wolkon, A.; Barradas, D.T.; Favaloro, J.; Zulu, J.E.; et al. Prevalence of SARS-CoV-2 in six districts in Zambia in July, 2020: A cross-sectional cluster sample survey. Lancet Glob. Health 2021, 9, e773–e781. [Google Scholar] [CrossRef]
- Chitungo, I.; Dzobo, M.; Hlongwa, M.; Dzinamarira, T. COVID-19: Unpacking the low number of cases in Africa. Public Health Pract. 2020, 1, 100038. [Google Scholar] [CrossRef] [PubMed]
- Wiens, K.E.; Mawien, P.N.; Rumunu, J.; Slater, D.; Jones, F.K.; Moheed, S.; Caflish, A.; Bior, B.K.; Jacob, I.A.; Lako, R.L.L.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Juba, South Sudan: A population-based study. medRxiv Prepr. Serv. Health Sci. 2021, 1–28. [Google Scholar] [CrossRef]
- Africa CDC. Generic Protocol for a Population-Based, Age and Gender-Stratified Sero-Survey Studyf SARS-CoV-2; Africa CDC: Addis Ababa, Ethiopia, 2020. [Google Scholar]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and COVID-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Salum, S.S.; Sheikh, M.A.; Hebestreit, A.; Kelm, S. Anti SARS-CoV2 seroprevalence in Zanzibar in 2021 before the Omicron wave. medRxiv 2022. [Google Scholar] [CrossRef]
- Lobaloba Ingoba, L.; Djontu, J.C.; Mfoutou Mapanguy, C.C.; Mouzinga, F.; Diafouka Kietela, S.; Vouvoungui, C.; Kuisma, E.; Nguimbi, E.; Ntoumi, F. Seroprevalence of anti-SARS-CoV-2 antibodies in a population living in Bomassa village, Republic of Congo. IJID Reg. 2022, 2, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Adetifa, I.M.O.; Uyoga, S.; Gitonga, J.N.; Mugo, D.; Otiende, M.; Nyagwange, J.; Karanja, H.K.; Tuju, J.; Wanjiku, P.; Aman, R.; et al. Temporal trends of SARS-CoV-2 seroprevalence during the first wave of the COVID-19 epidemic in Kenya. Nat. Commun. 2021, 12, 3966. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID-19: GPs urge government to clear up confusion over symptoms. BMJ 2021, 373, n1654. [Google Scholar] [CrossRef] [PubMed]
- Russell, B.; Moss, C.; Rigg, A.; Hopkins, C.; Papa, S.; Van Hemelrijck, M. Anosmia and ageusia are emerging as symptoms in patients with COVID-19: What does the current evidence say? Ecancermedicalscience 2020, 14, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; Lugova, H.; Dhingra, S.; Sharma, P.; Islam, S.; et al. Surveillance of antimicrobial resistance in low- and middle-income countries: A scattered picture. Antimicrob. Resist. Infect. Control 2021, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Haldrup, M.; Johansen, M.I.; Fjaeldstad, A.W. Anosmia and ageusia as primary symptoms of COVID-19. Ugeskr. Laeger 2020, 182, V04200205. [Google Scholar] [PubMed]
- Mermelstein, S. Acute anosmia from COVID-19 infection. Pract. Neurol. 2020, 20, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Biadsee, A.; Biadsee, A.; Kassem, F.; Dagan, O.; Masarwa, S.; Ormianer, Z. Olfactory and Oral Manifestations of COVID-19: Sex-Related Symptoms—A Potential Pathway to Early Diagnosis. Otolaryngol. Head Neck Surg. 2020, 163, 722–728. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Frequencies (n) | Percentages (%)/Median/IQR |
|---|---|---|
| Age(years) | 805 | 35 (IQR: 26–47) |
| Sex | ||
| Male | 458 | 56.9 |
| Female | 347 | 43.1 |
| District of residence | ||
| Magu | 249 | 30.9 |
| Misungwi | 297 | 36.9 |
| Ukerewe | 259 | 32.2 |
| Occupation | ||
| Business | 145 | 18.0 |
| Employed | 56 | 07.0 |
| Farmers | 448 | 55.7 |
| * Others | 156 | 19.3 |
| Variables | Frequencies | Percentages (%) |
|---|---|---|
| History of fever | ||
| Yes | 252 | 31.3 |
| No | 553 | 68.7 |
| History of fatigue | ||
| Yes | 265 | 32.9 |
| No | 540 | 67.1 |
| History of sore throat | ||
| Yes | 93 | 11.6 |
| No | 712 | 88.4 |
| History of cough | ||
| Yes | 585 | 27.3 |
| No | 220 | 72.7 |
| History of runny nose | ||
| Yes | 275 | 34.2 |
| No | 530 | 65.8 |
| History of shortness of breath(SOB) | ||
| Yes | 52 | 6.5 |
| No | 753 | 93.5 |
| History of wheezing | ||
| Yes | 49 | 6.1 |
| No | 756 | 93.9 |
| History of chest pain | ||
| Yes | 32 | 4.0 |
| No | 773 | 96.0 |
| History of other respiratory symptoms | ||
| Yes | 11 | 1.4 |
| No | 794 | 98.6 |
| History of headache | ||
| Yes | 259 | 32.2 |
| No | 546 | 67.78 |
| History of smell loss | ||
| Yes | 64 | 7.9 |
| No | 741 | 92.1 |
| History of taste loss | ||
| Yes | 82 | 10.2 |
| No | 723 | 88.8 |
| History of diarrhea | ||
| Yes | 71 | 8.8 |
| No | 734 | 91.2 |
| Variable | Frequency (n) | Percentage (%) |
|---|---|---|
| History of diabetes | ||
| Yes | 30 | 3.7 |
| No | 775 | 96.3 |
| History of lung diseases | ||
| Yes | 19 | 2.4 |
| No | 786 | 97.6 |
| History of blood pressure | ||
| Yes | 36 | 4.5 |
| No | 769 | 95.5 |
| History of renal diseases | ||
| Yes | 7 | 1 |
| No | 798 | 99 |
| History HIV/AIDs | ||
| Yes | 20 | 2.5 |
| No | 785 | 97.5 |
| On ART | ||
| Yes | 16 | 80 |
| No | 4 | 20 |
| Sickle cell disease | ||
| Yes | 5 | 0.6 |
| No | 800 | 99.4 |
| Cancer | ||
| Yes | 8 | 1.0 |
| No | 797 | 99.0 |
| Variable | Total | IgG Seropositivity (n, %) | Bivariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|---|
| cOR | 95%CI | p-Value | aOR | 95%CI | p-Value | |||
| Age (years) | 805 | * 34 (IQR: 26–47) | 0.994 | 0.985–1.00 | 0.260 | |||
| Sex | ||||||||
| Male | 458 | (223, 48.69) | 1 | |||||
| Female | 347 | (174, 50.14) | 1.08 | 0.63–1.85 | 0.782 | |||
| District | ||||||||
| Magu | 249 | (112, 44.98) | 1 | |||||
| Misungwi | 297 | (135, 45.45) | 1.01 | 0.73–1.42 | 0.912 | |||
| Ukerewe | 259 | (150, 57.92) | 1.68 | 1.19–2.39 | 0.004 | 1.29 | 1.08–1.54 | 0.004 |
| Occupation | ||||||||
| Business | 145 | (82, 56.55) | 1.05 | 0.72–1.51 | 0.603 | |||
| Employed | 56 | (27, 48.21) | 1.06 | 0.57–1.95 | 0.488 | 0.99 | 0.54–1.85 | 0.993 |
| Farmer | 448 | (215, 47.99) | 1.48 | 0.94–2.33 | 0.972 | |||
| Others | 156 | (73, 46.79) | 1 | |||||
| History of fever | ||||||||
| Yes | 252 | (127, 50.39) | 1.16 | 0.79–1.43 | 0.679 | |||
| No | 553 | (270, 48.82) | 1 | |||||
| History of fatigue | ||||||||
| Yes | 265 | (133, 50.18) | 1.05 | 0.56–1.12 | 0.193 | |||
| No | 540 | (264, 48.89) | 1 | |||||
| History of sore throat | ||||||||
| Yes | 93 | (45, 48.39) | 0.96 | 0.62–1.48 | 0.849 | |||
| No | 712 | (352, 49.4) | 1 | |||||
| History of cough | ||||||||
| Yes | 220 | (97, 44.09) | 0.75 | 0.55–1.02 | 0.069 | |||
| No | 585 | (300, 51.28) | 1 | |||||
| History of runny nose | ||||||||
| Yes | 275 | (139, 50.54) | 1.08 | 0.81–1.44 | 0.616 | |||
| No | 530 | (258, 48.68) | 1 | |||||
| History of SOB | ||||||||
| Yes | 52 | (24, 46.15) | 0.87 | 0.49–1.53 | 0.637 | |||
| No | 753 | (373, 49.52) | 1 | |||||
| History of chest pain | ||||||||
| Yes | 32 | (15, 46.88) | 0.90 | 0.44–1.83 | 0.778 | |||
| No | 773 | (382, 49.42) | 1 | |||||
| History of smell loss | ||||||||
| Yes | 64 | (35, 54.69) | 1.26 | 0.76–2.11 | 0.371 | 1.15 | 0.67–1.98 | 0.601 |
| No | 741 | (362, 48.85) | 1 | |||||
| History of taste loss | ||||||||
| Yes | 82 | (45, 54.87) | 1.28 | 0.81–2.03 | 0.289 | 1.27 | 0.78–2.06 | 0.331 |
| No | 723 | (352, 48.69) | 1 | |||||
| Variable | Total | IgM Seropositivity (n, %) | Bivariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|---|
| cOR | 95%CI | p-Value | aOR | 95%CI | p-Value | |||
| Age(years) | 805 | * 32.5 (IQR: 25–45) | 0.994 | 0.976–1.01 | 0.594 | |||
| Sex | ||||||||
| Male | 347 | (26,7.52) | 1.08 | 0.63–1.85 | 0.783 | 1.19 | 0.68–2.06 | 0.528 |
| Female | 458 | (32,6.90) | 1 | |||||
| District | ||||||||
| Misungwi | 297 | (11, 3.70) | 1 | |||||
| Magu | 249 | (21, 8.43) | 2.39 | 1.13–5.06 | 0.022 | 2.89 | 1.34–6.25 | 0.007 |
| Ukerewe | 259 | (26, 10.03) | 2.9 | 1.40–5.99 | 0.004 | 3.55 | 1.68–7.47 | 0.001 |
| Occupation | ||||||||
| Business | 145 | (11, 7.58) | 0.83 | 0.41–1.67 | 0.603 | |||
| Employed | 56 | (6, 10.71) | 1.44 | 0.51–4.03 | 0.48 | |||
| Farmer | 448 | (29, 6.47) | 0.99 | 0.42–2.31 | 0.97 | |||
| Others | 156 | (12,7.69) | 1 | |||||
| History of fever | ||||||||
| Yes | 252 | (20, 7.94) | 1.6 | 0.67–2.05 | 0.588 | |||
| No | 553 | (38, 6.87) | 1 | |||||
| History of fatigue | ||||||||
| Yes | 265 | (24, 9.05) | 1.48 | 0.86–2.55 | 0.157 | |||
| No | 540 | (34, 6.29) | 1 | |||||
| History of sore throat | ||||||||
| Yes | 93 | (6, 6.45) | 0.88 | 0.37–2.09 | 0.765 | |||
| No | 712 | (52, 7.30) | 1 | |||||
| History of cough | ||||||||
| Yes | 220 | (15, 6.81) | 0.92 | 0.50–1.69 | 0.795 | |||
| No | 585 | (43, 7.35) | 1 | |||||
| History of runny nose | ||||||||
| Yes | 275 | (28,10.18) | 1.89 | 1.11–3.23 | 0.123 | 1.84 | 1.03–3.51 | 0.036 |
| No | 530 | (30,5.67) | 1 | |||||
| History of SOB | ||||||||
| Yes | 52 | (6, 11.54) | 1.76 | 0.72–4.31 | 0.217 | |||
| No | 753 | (52, 6.90) | 1 | |||||
| History of chest pain | ||||||||
| Yes | 32 | (1, 3.12) | 0.41 | 0.05–3.02 | 0.378 | |||
| No | 773 | (57, 7.37) | 1 | |||||
| History of smell loss | ||||||||
| Yes | 64 | (6, 9.38) | 1.37 | 0.56–3.33 | 0.486 | |||
| No | 741 | (52, 7.02) | 1 | |||||
| History of taste loss | ||||||||
| Yes | 82 | (12,14.63) | 2.52 | 1.28–4.99 | 0.008 | 1.84 | 1.12–4.48 | 0.023 |
| No | 723 | (46, 6.36) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nyawale, H.A.; Moremi, N.; Mohamed, M.; Njwalila, J.; Silago, V.; Krone, M.; Konje, E.T.; Mirambo, M.M.; Mshana, S.E. High Seroprevalence of SARS-CoV-2 in Mwanza, Northwestern Tanzania: A Population-Based Survey. Int. J. Environ. Res. Public Health 2022, 19, 11664. https://doi.org/10.3390/ijerph191811664
Nyawale HA, Moremi N, Mohamed M, Njwalila J, Silago V, Krone M, Konje ET, Mirambo MM, Mshana SE. High Seroprevalence of SARS-CoV-2 in Mwanza, Northwestern Tanzania: A Population-Based Survey. International Journal of Environmental Research and Public Health. 2022; 19(18):11664. https://doi.org/10.3390/ijerph191811664
Chicago/Turabian StyleNyawale, Helmut A., Nyambura Moremi, Mohamed Mohamed, Johnson Njwalila, Vitus Silago, Manuel Krone, Eveline T. Konje, Mariam M. Mirambo, and Stephen E. Mshana. 2022. "High Seroprevalence of SARS-CoV-2 in Mwanza, Northwestern Tanzania: A Population-Based Survey" International Journal of Environmental Research and Public Health 19, no. 18: 11664. https://doi.org/10.3390/ijerph191811664