
Hybrid Management of an Aortobronchial Fistula after Patch Aortoplasty for Aortic Coarctation in a Patient with SARS-CoV-2 Pneumonia: Case Report and Review of the Literature

Abstract
:1. Introduction
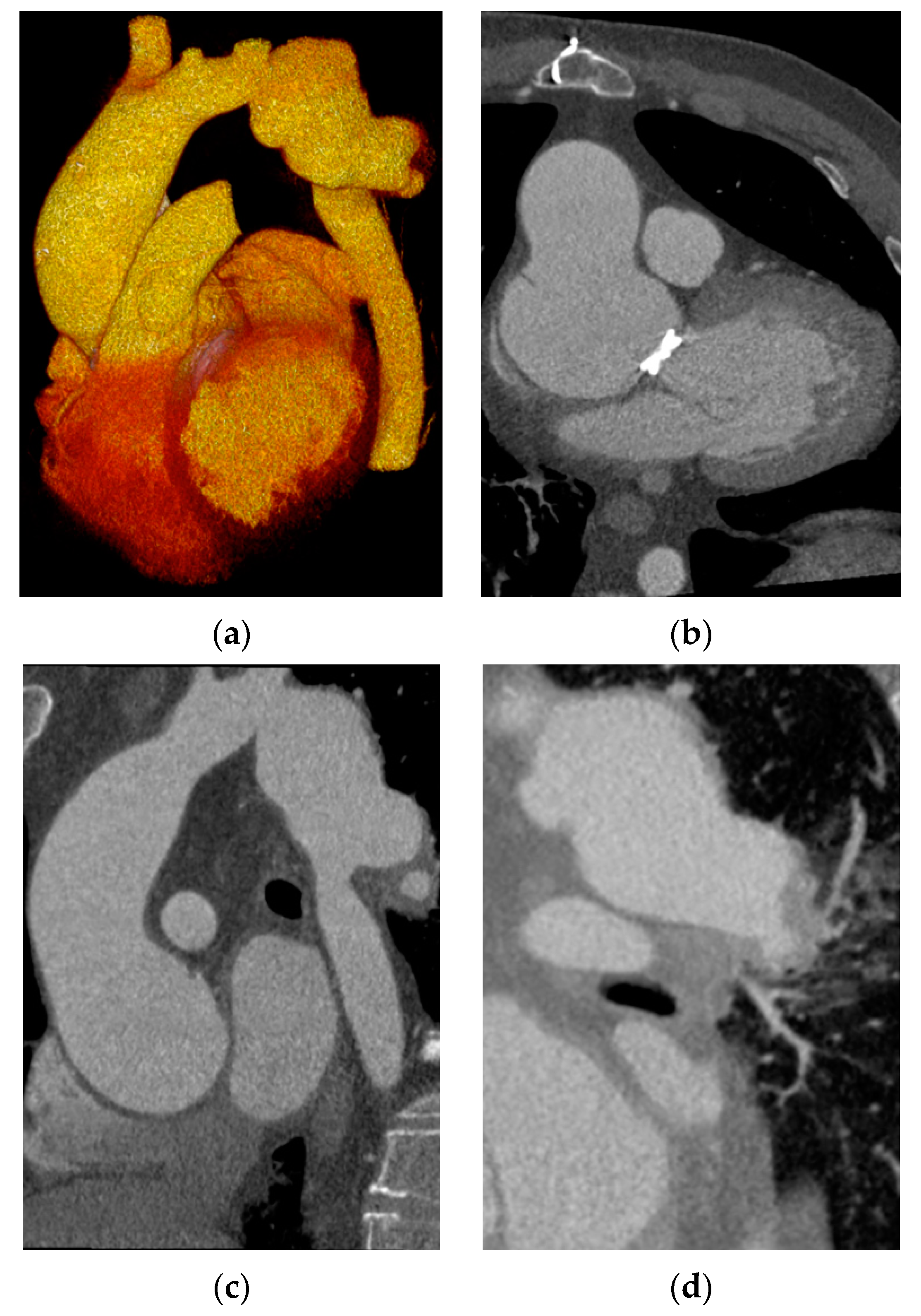
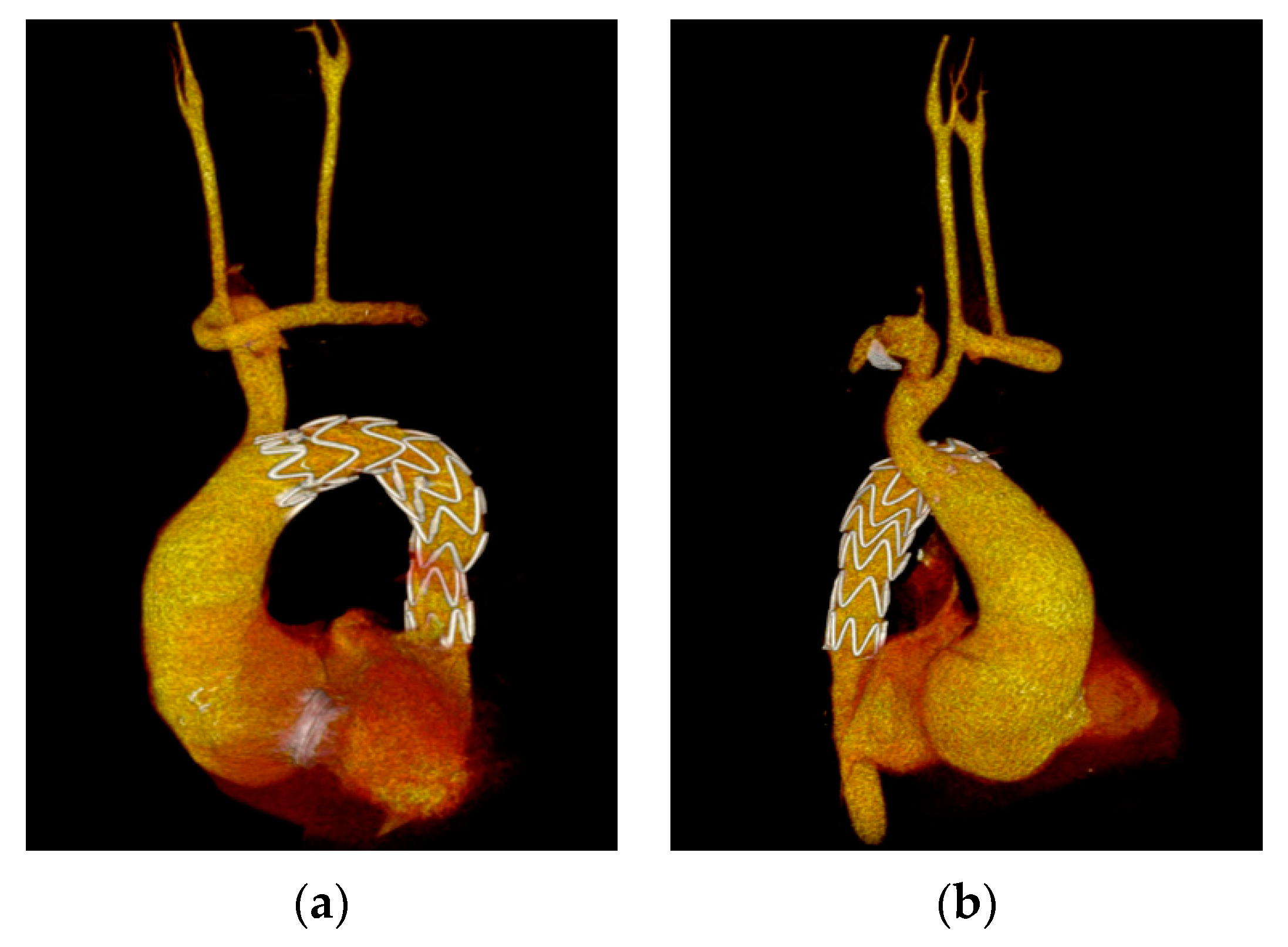
2. Case Report
3. Discussions
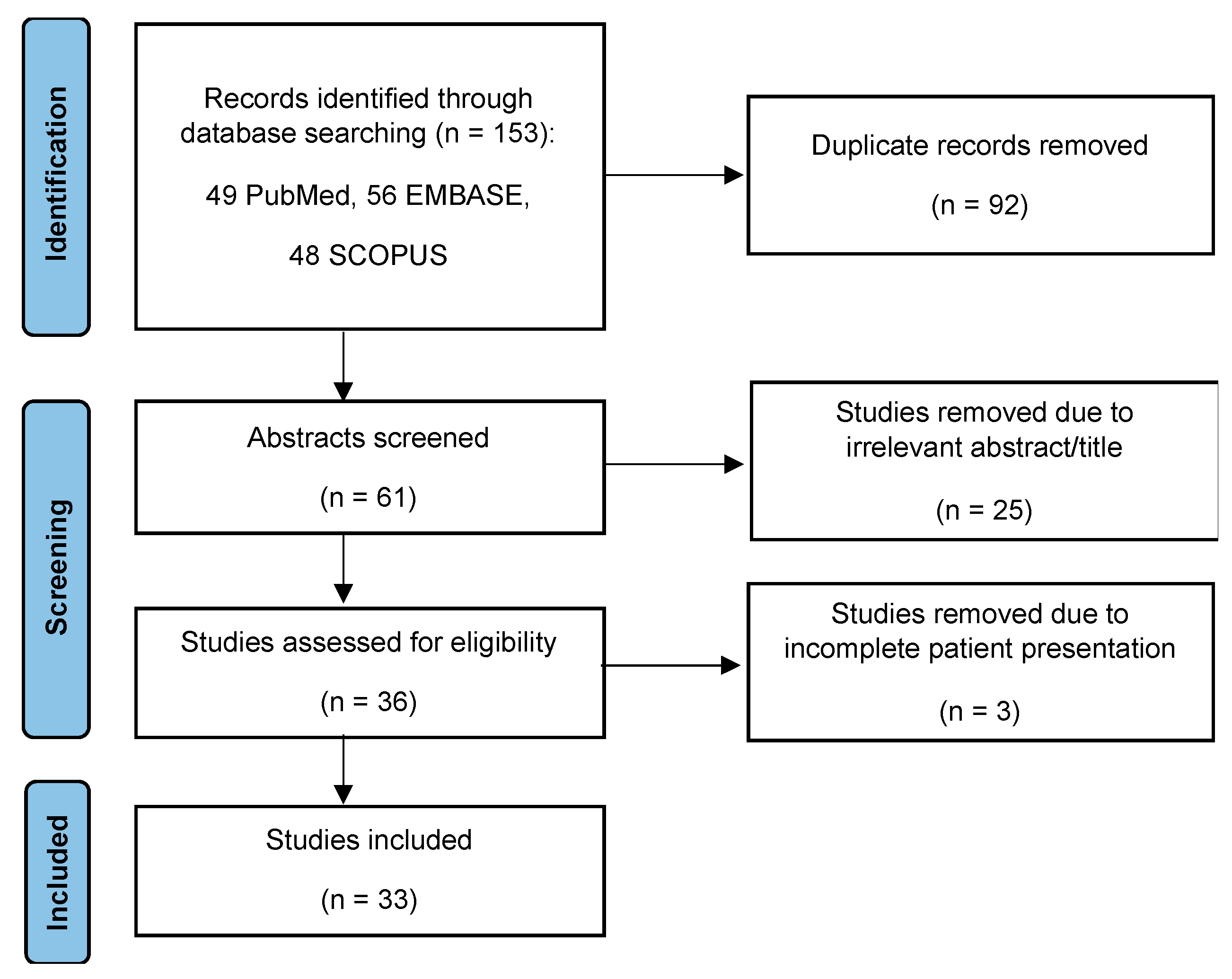
Literature Review
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernández González, A.L.; Montero, J.A.; Luna, D.; Gil, O.; Sanjuán, V.M.; Monzonís, A.M. Aortobronchial fistula secondary to chronic post-traumatic thoracic aneurysm. Tex. Heart Inst. J. 1996, 23, 174–177. [Google Scholar] [PubMed]
- Kotani, S.; Inoue, Y.; Wakatabe, M.; Yashiro, H.; Hase, M. Successful Endovascular Repair of an Aortobronchial Fistula due to Takayasu Arteritis. Ann. Vasc. Surg. 2021, 71, 533.e7–533.e10. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.S.; Stoeckel, D.A.; Kaufman, E.E.; Jacobs, D.L. Massive Hemoptysis from an Aortobronchial Fistula Secondary to BCG-Related Mycotic Thoracic Aortic Aneurysm. Ann. Thorac. Surg. 2016, 101, 350–352. [Google Scholar] [CrossRef] [PubMed]
- Posacioglu, H.; Apaydin, A.Z. Pseudoaneurysm and aortobronchial fistula after aortic coarctation repair by patch aortoplasty. Tex. Heart Inst. J. 2004, 31, 319–321. [Google Scholar] [PubMed]
- Smayra, T.; Otal, P.; Soula, P.; Chabbert, V.; Cérène, A.; Joffre, F.; Rousseau, H. Pseudoaneurysm and aortobronchial fistula after surgical bypass for aortic coarctation: Management with endovascular stent-graft. J. Endovasc. Ther. 2001, 8, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Alageel, M. Aortobronchial fistula postcoronary angiography, first reported case in the literature. Interv. Cardiol. 2020, 12, 126–128. [Google Scholar]
- Favre, J.P.; Gournier, J.P.; Adham, M.; Rosset, E.; Barral, X. Aortobronchial fistula: Report of three cases and review of the literature. Surgery 1994, 115, 264–270. [Google Scholar]
- Dorweiler, B.; Weigang, E.; Duenschede, F.; Pitton, M.B.; Dueber, C.; Vahl, C.F. Strategies for endovascular aortic repair in aortobronchial and aortoesophageal fistulas. Thorac. Cardiovasc. Surg. 2013, 61, 575–580. [Google Scholar] [CrossRef] [Green Version]
- Dake, M.D.; Miller, D.C.; Semba, C.P.; Mitchell, R.S.; Walker, P.J.; Liddell, R.P. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N. Engl. J. Med. 1994, 331, 1729–1734. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.F.; Chen, Y.C.; Lin, M.C.; Kao, C.L. Thoracic aortic aneurysm with aortobronchial fistula: A thirteen-year experience. Heart Lung 2004, 33, 119–123. [Google Scholar] [CrossRef]
- Fontana, M.; Tonelli, R.; Gozzi, F.; Castaniere, I.; Marchioni, A.; Fantini, R.; Coppi, F.; Natali, F.; Rovatti, E.; Clini, E. An Uncommon Cause of Hemoptysis: Aortobronchial Fistula. Multidiscip. Respir. Med. 2018, 13, 4–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldien, A.S.; Deo, S.; Nichols, F.C.; Greason, K.L. A Bad Experience with Endovascular Treatment of an Aortobronchial Fistula. Ann. Thorac. Surg. 2012, 93, 650–651. [Google Scholar] [CrossRef] [PubMed]
- Nodari, F.; Verrengia, A.; Di Betta, E.; Bonera, G.; Bonardelli, S. Combined Endovascular and Open Treatment to Prevent Increase in Afterload in Anastomotic Pseudoaneurysm and Aortobronchial Fistula after Surgery for Aortic Coarctation. J. Vasc. Surg. Cases Innov. Tech. 2021, 7, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Munneke, G.; Loosemore, T.; Smith, J.; Thompson, M.; Morgan, R.; Belli, A.M. Pseudoaneurysm after Aortic Coarctation Repair Presenting with an Aortobronchial Fistula Successfully Treated with an Aortic Stent Graft. Clin. Radiol. 2006, 61, 104–108. [Google Scholar] [CrossRef]
- Oliver, J.M.; Gallego, P.; Gonzalez, A.; Aroca, A.; Bret, M.; Mesa, J.M. Risk factors for aortic complications in adults with coarctation of the aorta. J. Am. Coll. Cardiol. 2004, 44, 1641–1647. [Google Scholar] [CrossRef] [Green Version]
- Radchenko, C.; Alraiyes, A.H.; Shojaee, S. A systematic approach to the management of massive hemoptysis. J. Thorac. Dis. 2017, 9, S1069–S1086. [Google Scholar] [CrossRef] [Green Version]
- Son, S.A.; Lee, D.H.; Kim, G.J. Effective strategy in the treatment of aortobronchial fistula with recurrent hemoptysis. Yeungnam Univ. J. Med. 2020, 37, 141–146. [Google Scholar] [CrossRef]
- Eren, E.; Keles, C.; Toker, M.E.; Ersahin, S.; Erentug, V.; Guler, M.; Ipek, G.; Akinci, E.; Balkanay, M.; Yakut, C. Surgical Treatment of Aortobronchial and Aortoesophageal Fistulae Due to Thoracic Aortic Aneurysm. Tex. Heart Inst. J. 2005, 32, 522–528. [Google Scholar]
- Melvan, J.N.; DeLaRosa, J.; Vasquez, J.C. Aortobronchial Fistula after Thoracic Endovascular Aortic Repair (TEVAR) for Descending Thoracic Aortic Aneurysm. Ann. Vasc. Surg. 2017, 41, 283.e1–283.e4. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Aslam, M.S.; Haddadian, B.; Bajwa, T. Percutaneous Treatment of Late-Aortic Pseudoaneurysm Resulting from Surgical Repair of Aortic Coarctation. Catheter. Cardiovasc. Interv. 2011, 78, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Bhuyan, R.R.; Rajendran, S.; Unnikrishnan, M.; Jayakumar, K. Successful Repair of Aortobronchial Fistula Using Circulatory Arrest. ANZ J. Surg. 2007, 77, 398–399. [Google Scholar] [CrossRef] [PubMed]
- Bozzani, A.; Arici, V.; Rodolico, G.; Brunetto, M.B.; Argenteri, A. Endovascular Exclusion of Aortobronchial Fistula and Distal Anastomotic Aneurysm after Extra-Anatomic Bypass for Aortic Coarctation. Tex. Heart Inst. J. 2017, 44, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Bugge, A.S.; Kvitting, J.P.E.; Sundset, A.; Birkeland, S. Lung Autotransplantation and Extra-Anatomic Bypass to Treat an Aortobronchial Fistula after Previous Surgery for Aortic Coarctation. J. Card. Surg. 2021, 36, 2924–2927. [Google Scholar] [CrossRef] [PubMed]
- Caes, F.; Taeymans, Y.; Van Nooten, G. Aortobronchial Fistula: A Late Complication of Coarctation Repair by Patch Aortoplasty. Thorac. Cardiovasc. Surg. 1993, 41, 80–82. [Google Scholar] [CrossRef]
- Chuter, T.A.M. Endovascular Stent-Graft Exclusion of an Aortobronchial Fistula. J. Vasc. Interv. Radiol. 1996, 7, 357–359. [Google Scholar] [CrossRef]
- Foster, C.L.; Kalbhen, C.L.; Demos, T.C.; Lonchyna, V.A. Aortobronchial fistula occurring after coarctation repair: Findings on aortography, helical CT, and CT angiography. AJR Am. J. Roentgenol. 1998, 171, 401–402. [Google Scholar] [CrossRef] [Green Version]
- Garniek, A.; Morag, B.; Schmahmann, S.; Rubinstein, Z.J. Aortobronchial fistula as a complication of surgery for correction of congenital aortic anomalies. Radiology 1990, 175, 347–348. [Google Scholar] [CrossRef]
- Hamilton, M.C.K.; Holemans, J.A.; Entwisle, J. Aortobronchopulmonary Fistula after Repair of Aortic Coarctation. Clin. Radiol. 2004, 59, 1044–1047. [Google Scholar] [CrossRef]
- Hayat, J. Aortobronchial Fistula after Coarctation Repair Treated with Extra-Anatomic Graft. Rawal Med. J. 2010, 35, 253–254. [Google Scholar]
- Kakos, G.S.; Kataria, Y.P.; Vasko, J.S. Occult Hemoptysis: Iatrogenic Aortobronchial Fistula. Arch. Surg. 1975, 110, 352. [Google Scholar] [CrossRef] [PubMed]
- Kalkat, M.S.; Bonser, R.S. Management of Aortobronchial Fistula Following Coarctation Repair. Eur. J. Cardio-Thorac. Surg. 2003, 23, 116–118. [Google Scholar] [CrossRef] [Green Version]
- Kamler, M.; Tuengerthal, S.; Rauch, H.; Hagl, S.; Jakob, H. Near-Fatal Hemoptysis and Emergency Surgical Repair after Aortic Patch-Plasty. Thorac. Cardiovasc. Surg. 2001, 49, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Kansal, V.; Nagpal, S. Delayed Diagnosis of Hemoptysis in the Case of Prior Aortic Coarctation Repair: A Case Report of Aortobronchial Fistula. Respir. Med. Case Rep. 2015, 16, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, W.A.; Kern, J.A.; Tribble, C.G. Repair of Aortobronchial Fistula Using Extraanatomic Grafts and Hypothermic Arrest. Ann. Thorac. Surg. 1997, 63, 1158–1160. [Google Scholar] [CrossRef]
- Manganas, C.; Iliopoulos, J.; Chard, R.B.; Nunn, G.R. Reoperation and Coarctation of the Aorta: The Need for Lifelong Surveillance. Ann. Thorac. Surg. 2001, 72, 1222–1224. [Google Scholar] [CrossRef]
- Marcheix, B.; Lamarche, Y.; Perrault, P.; Cartier, R.; Bouchard, D.; Carrier, M.; Perrault, L.P.; Demers, P. Endovascular Management of Pseudo-Aneurysms after Previous Surgical Repair of Congenital Aortic Coarctation. Eur. J. Cardio-Thorac. Surg. 2007, 31, 1004–1007. [Google Scholar] [CrossRef]
- Milano, A.; De Carlo, M.; Mussi, A.; Falaschi, F.; Bortolotti, U. Aortobronchial Fistula after Coarctation Repair and Blunt Chest Trauma. Ann. Thorac. Surg. 1999, 67, 539–541. [Google Scholar] [CrossRef]
- Moore, J.; Cheng, A.M.; Leary, P. Recurrent Hemoptysis Leading to Cardiac Arrest Due to Aortobronchial Fistula. Am. J. Respir. Crit. Care Med. 2018, 197, A3439. [Google Scholar]
- Neves, A.A.G.; de Oliveira, A.G.N.M.; Beck, R.T.; dos Santos, R.V.; Moreira, F.C.P.; Amato, A.C.M. Tratamento Endovascular de Pseudoaneurisma de Aorta Torácica Com Fístula Aorto-Brônquica Em Pós-Operatório Tardio de Cirurgia de Correção de Coarctação de Aorta. J. Vasc. Bras. 2011, 10, 64–67. [Google Scholar] [CrossRef]
- O’Sullivan, K.E.; Bolster, F.; Lawler, L.P.; Hurley, J. Endovascular Management of an Acquired Aortobronchial Fistula Following Aortic Bypass for Coarctation. Interact. Cardiovasc. Thorac. Surg. 2014, 18, 131–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana, A.L.; Aguilar, E.M.; Heredero, A.F.; Riambau, V.; Paul, L.; Acín, F. Aortobronchial Fistula after Aortic Coartactation. J. Thorac. Cardiovasc. Surg. 2006, 131, 240–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Caulo, E.A.; Velázquez, C.J.; Barquero, J.M.; García-Borbolla, M. Atypical Chest Pain and Hemoptysis 27 Years After Aortic Coarctation Surgery: Aortobronchial Fistula, Management and Endovascular Treatment. Rev. Española Cardiol. 2011, 64, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Saunders, S.; Young, C. An Unusual Epistaxis. Postgrad. Med. J. 2002, 78, 619–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinelnikov, Y.S.; Kornilov, I.A.; Soynov, I.A. Pseudoaneurysm and Aorto-Bronchial Fistula Following Balloon Dilation of Recoarctation. Cardiol. Young 2016, 26, 596–598. [Google Scholar] [CrossRef]
- Verma, H.; Hiremath, N.; Maiya, S.; George, R.K.; Tripathi, R.K. Endovascular Exclusion of Complex Postsurgical Aortic Arch Pseudoaneurysm Using Vascular Plug Devices and a Review of Vascular Plugs. Perspect. Vasc. Surg. Endovasc. Ther. 2012, 24, 193–197. [Google Scholar] [CrossRef]
- Knyshov, G.V.; Sitar, L.L.; Glagola, M.D.; Atamanyuk, M.Y. Aortic aneurysms at the site of the repair of coarctation of the aorta: A review of 48 patients. Ann. Thorac. Surg. 1996, 61, 935–939. [Google Scholar] [CrossRef]
- Becker, R.C. COVID-19 update: Covid-19-associated coagulopathy. J. Thromb. Thrombolysis 2020, 50, 54–67. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Patients | Age, Sex | Symptoms | Age at Culprit Intervention | Type(s) of Surgery | Complication Responsible for ABF | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Aslam et al., 2011 [21] | 1 | 28, F | Hemoptysis | 16 | Resection of the native DTA, graft replacement of the DTA with proximal and distal end-to-side anastomoses | PSA proximal anastomosis | Replacement of DTA synthetic graft + wedge resection lung | 38-years- old: new PSA at the caudal end of the graft treated with coil embolization and Amplatzer vascular plug, uneventful at 1 month |
| Bhuyan et al., 2007 [22] | 1 | 45, M | Recurrent, massive haemoptysis | 25 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft | No follow-up data |
| Bozzani et al., 2017 [23] | 1 | 65, M | Hemoptysis | 48 | Extra-anatomic bypass distal arch-DTA | PSA distal anastomosis | TEVAR between extra-anatomic bypass and distal DTA + Amplatzer occlusion of the proximal DTA at the level of the coarctation | Uneventful 15 months |
| Bugge et al., 2021 [24] | 1 | 43, M | Dry cough, recurrent hemoptysis | 32 | 1. 10-years-old: patch augmentation complicated with PSA 2. 15-years-old: new patch augmentation complicated with infection 3. 32-years-old: interposition of a synthetic graft | PSA distal anastomosis | TEVAR | New ABF after 2 months secondary to left main bronchus compression by the graft, treated with extra-anatomic bypass AA-DTA + left pulmonary hilum dissection with excision of the portion of the bronchus containing the fistula + lung autotransplantation, uneventful 6 months |
| Caes et al., 1993 [25] | 1 | 24, M | Irritative cough, recurrent hemoptysis | 11 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft + closure of the pulmonary side of the ABF with running suture | Postoperative MSOF, discharged after 48 days, uneventful 1 year |
| Chuter et al., 1996 [26] | 1 | 56, M | Massive hemoptysis | 35 | Interventions 1 and 2—unknown age and surgical technique, complicated with re-coarctation and PSA 3. 35-years-old: interposition of a synthetic graft | PSA distal anastomosis | TEVAR | Uneventful 7 months |
| Eldien et al., 2011 [12] | 1 | 35, F | Hemoptysis | 35 | Interposition of a synthetic graft | Unspecified complication at distal anastomosis | Hybrid: TEVAR + left subclavian–to–left carotid bypass graft | Graft infection after 1 month treated with open surgical repair—extra-anatomic bypass AA—DTA + removal of the infected graft + lung decortication. Postoperative ECMO support for 13 days and MSOF, discharged after 62 days, uneventful 3 months |
| Eren et al., 2005 [18] | 1 | 42, M | Recurrent hemoptysis | 25 | Synthetic patch aortoplasty | PSA aortoplasty site | Synthetic patch aortoplasty + debridement and suture of lung parenchima | No follow-up data |
| Fontana et al., 2018 [11] | 1 | 46, M | Recurrent hemoptysis | 18 | Unspecificed surgical repair | PSA | TEVAR | Uneventful 30 days |
| Foster et al., 1998 [27] | 1 | 62, M | Recurrent, massive hemoptysis | 48 | 1. 18-years-old: resection of the coarctation and replacement with a homograft complicated with aneurysm formation 2. 44-years-old: interposition of a synthetic graft | PSA distal anastomosis | Interposition of a synthetic graft | Uneventful 4 years |
| Garniek et al., 1990 [28] | 1 | 5, M | Recurrent hemoptysis | 5 months | 1. Unknown correction of PDA and coarctation in the neonatal period, complicated with occlusion of the subclavian graft at the age of 5 months 2. Extra-anatomic bypass AA-DTA | PSA distal anastomosis | - | Exitus—uncontrollable intrabronchial hemorrhage |
| Hamilton et al., 2004 [29] | 3 | 28, F | Massive hemoptysis + dyspnea | 7 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft + fistula closure | No follow-up data |
| 37, F | Massive hemoptysis | 20 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft | No follow-up data | ||
| 57, F | Massive hemoptysis | 24 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft | No follow-up data | ||
| Hayat J, 2010 [30] | 2 | 30, F | Massive hemoptysis | 24 | Synthetic patch aortoplasty | PSA aortoplasty site | Extra-anatomic bypass AA-DTA + ABF closure covered with pleura | Postoperative hemotorax, no follow-up |
| 46, M | Hemoptysis | 38 | Synthetic patch aortoplasty complicated with massive hemorrhage + paraplegia | PSA aortoplasty site | Interposition of a synthetic graft + ABF closure | No follow-up data | ||
| Kakos et al., 1975 [31] | 1 | 56, M | Hemoptysis | 49 | Not mentioned | Not mentioned | Direct closure of the aorta | Uneventful 12 months |
| Kalkat et al., 2003 [32] | 2 | 54, M | Recurrent hemoptysis + left sided chest pain | 43 | Synthetic patch aortoplasty complicated with massive hemorrhage + paraplegia | PSA aortoplasty site | Extra-anatomic bypass AA-DTA + resection of the involved aorta and PSA + bronchus repair | Uneventful 10 years |
| 52, M | Massive hemoptysis | 22 | 2 interventions—synthetic patch aortoplasty at the age of 13 and 22 years complicated with paraparesis and transient cortical blindness | PSA aortoplasty site | Interposition of a synthetic graft | Uneventful 3 years | ||
| Kamler et al., 2001 [33] | 1 | 38, M | Massive hemoptysis | 28 | 1. 15-years-old: synthetic patch aortoplasty complicated with re-coarctation 2. 28-years-old: synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft + left pneumonectomy | Uneventful 3 years |
| Kansal et al., 2015 [34] | 1 | 46, M | Recurrent hemoptysis | 17 | Unknown open surgical repair | PSA | TEVAR | No follow-up data |
| Lawrence et al., 1997 [35] | 1 | 23, F | Massive hemoptysis | 15 | Interventions 1 and 2—unknown age, surgical technique and complications. 3. 15-years-old: interposition of a synthetic graft | PSA | Extra-anatomic bypass AA-DTA+ removal of the old graft and PSA + bypass using a synthetic graft between the extra-anatomic conduit and the left axillary artery | No follow-up data |
| Manganas et al., 2001 [36] | 1 | 29, F | Massive hemoptysis | 24 | 1. 3-years-old: resection of the coarctation and end-to-end anastomosis complicated with re-coarctation 2. 9-years-old: synthetic patch aortoplasty complicated with recoarctation 3. 24-years-old: extra-anatomic bypass AA-DTA | PSA distal anastomosis | Unspecified surgical repair | No follow-up data |
| Marcheix et al., 2007 [37] | 1 | 32, M | Massive hemoptysis | 29 | 1. 4-years-old: synthetic patch aortoplasty, complication not mentioned 2. 29-years-old: interposition of a synthetic graft | PSA distal anastomosis | TEVAR | Uneventful 12.9 months |
| Milano et al., 1999 [38] | 1 | 34, M | Recurrent hemoptysis + dysphonia | 17 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft + partial removal of the upper lobe of the left lung | Uneventful 8 months |
| Moore et al., 2018 [39] | 1 | 67, F | Massive hemoptysis | Not mentioned | Unknown open surgical repair | PSA distal anastomosis | TEVAR | No follow-up data |
| Munneke et al., 2005 [14] | 1 | 53, F | Recurrent hemoptysis | 27 | Synthetic patch aortoplasty | PSA aortoplasty site | TEVAR covering the origin of the left subclavian artery with retrograde flow through the left vertebral artery | No follow-up data |
| Neves et al., 2017 [40] | 1 | 38, F | Massive hemoptysis + precordial pain | 16 | Extra-anatomic bypass AA-DTA | PSA distal anastomosis | TEVAR | Uneventful 3 months |
| Nodari et al., 2021 [13] | 1 | 78, F | Recurrent hemoptysis | 41 | Extra-anatomic bypass left subclavian artery-DTA | PSA distal anastomosis | Hybrid approach: Exclusion of the extra-anatomic bypass with an Amplatzer plug + coil exclusion of the PSA + TEVAR of the native aorta + left axillo-femoral bypass to relieve pressure in the pre-coarctation aortic arch | Uneventful 4 months |
| O’Sullivan et al., 2014 [41] | 1 | 46, M | Massive hemoptysis | 13 | 1. Neonatal period: unknown correction 2. 13-years-old: extra-anatomic bypass distal arch-DTA with reimplantation of the left subclavian artery into the proximal end of the bypass graft | PSA left subclavian artery reimplantation site | Occlusion of the left subclavian artery with an Amplatzer plug + TEVAR exclusion of the extra-anatomic bypass | No follow-up data |
| Posacioglu et al., 2004 [4] | 1 | 26, M | Massive hemoptysis | 10 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft + suture ligature of the pulmonary lesion | No follow-up data |
| Quintana et al., 2006 [42] | 1 | 47, M | Massive hemoptysis | 32 | Unknown open surgical repair | PSA | TEVAR | Hemoptysis in the 5th postoperative day secondary to type 2B endoleak treated with coil embolization, uneventful at 12 months |
| Rodriguez-Caulo et al., 2011 [43] | 1 | 39, M | Hemoptysis + atypical chest pain | 12 | Synthetic patch aortoplasty | PSA aortoplasty site | TEVAR | Proximal Type 1A endoleak the 3rd postoperative day: hybrid management with a secondary TEVAR + left carotid-left subclavian artery bypass, uneventful at 12 months |
| Saunders et al., 2002 [44] | 1 | 37, M | Epistaxis + hemoptysis | 19 | Synthetic patch aortoplasty | PSA aortoplasty site | Interposition of a synthetic graft | Minor stroke in the postoperative period, no follow up |
| Sinelnikov et al., 2015 [45] | 1 | 6, F | Hemoptysis + dyspnea | 5 | 1. 5-years-old: interposition of a synthetic graft complicated with re-coarctation 2. 3 months after the 1rst intervention: balloon dilatation of the re-coarctation | PSA proximal anastomosis | Replacement of the interposed synthetic graft + repair of the left lower lobe bronchus | Uneventful 6 months |
| Smayra et al., 2001 [5] | 1 | 61, M | Recurrent hemoptysis | 43 | Extra-anatomic bypass distal arch-DTA | PSA distal anastomosis | TEVAR between extra-anatomic bypass and distal DTA | Injury to the iliac artery while manipulating the catheter: iliofemoral bypass, uneventful 2 years |
| Verma et al., 2012 [46] | 1 | 36, M | Recurrent hemoptysis + dysphonia | 32 | 1. 23-years-old: synthetic patch aortoplasty complicated with ruptured PSA at aortoplasty site 2. 32-years-old: extra-anatomic bypass AA-DTA with ligation of the aortic arch distal to the left common carotid artery and of the distal descending thoracic aorta after the PSA complicated with persistent flow in the PSA and ABF | PSA aortoplasty site | Endovascular occlusion of the distal aortic arch with Amplatzer plug 2, of the aortic coarctation with Amender PDA closure device and of the distal leak site with Amender PDA closure device | Uneventful 6 months |
| Intervention (No. of Cases) | Complications (No. of Cases) |
|---|---|
| Replacement of the synthetic graft (1 case) | PSA (after 10 years) (1 case) |
| Interposition of a synthetic graft (12 cases) | MSOF (postoperative) (1 case) Minor stroke (postoperative) (1 case) |
| Synthetic patch aortoplasty (1 case) | - |
| Extra-anatomic bypass (3 cases) | Hemothorax (postoperative) (1 case) |
| Direct closure (1 case) | - |
| Unfinished intervention (1 case) | Exitus (intraoperative) (1 case) |
| Unspecified (1 case) | - |
| Endovascular (14 cases) | ABF (after 2 months) (1 case) Endoleak (Type 1A and 2B, postoperative) (2 cases) Iliac artery injury (intraoperative) (1 case) |
| Hybrid (2 cases) | Graft infection (after 1 month) (1 case) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tinica, G.; Tarus, A.; Bacusca, A.; Chistol, R.O.; Rusu, A.C.; Todosia, M.T.; Furnica, C. Hybrid Management of an Aortobronchial Fistula after Patch Aortoplasty for Aortic Coarctation in a Patient with SARS-CoV-2 Pneumonia: Case Report and Review of the Literature. Medicina 2022, 58, 1385. https://doi.org/10.3390/medicina58101385
Tinica G, Tarus A, Bacusca A, Chistol RO, Rusu AC, Todosia MT, Furnica C. Hybrid Management of an Aortobronchial Fistula after Patch Aortoplasty for Aortic Coarctation in a Patient with SARS-CoV-2 Pneumonia: Case Report and Review of the Literature. Medicina. 2022; 58(10):1385. https://doi.org/10.3390/medicina58101385
Chicago/Turabian StyleTinica, Grigore, Andrei Tarus, Alberto Bacusca, Raluca Ozana Chistol, Alexandra Cristina Rusu, Mihaela Tomaziu Todosia, and Cristina Furnica. 2022. "Hybrid Management of an Aortobronchial Fistula after Patch Aortoplasty for Aortic Coarctation in a Patient with SARS-CoV-2 Pneumonia: Case Report and Review of the Literature" Medicina 58, no. 10: 1385. https://doi.org/10.3390/medicina58101385