
Maternal–Neonatal Outcomes of Obstetric Deliveries Performed in Negative Pressure Isolation Rooms during the COVID-19 Omicron Variant Pandemic in Taiwan: A Retrospective Cohort Study of a Single Institution

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Definition
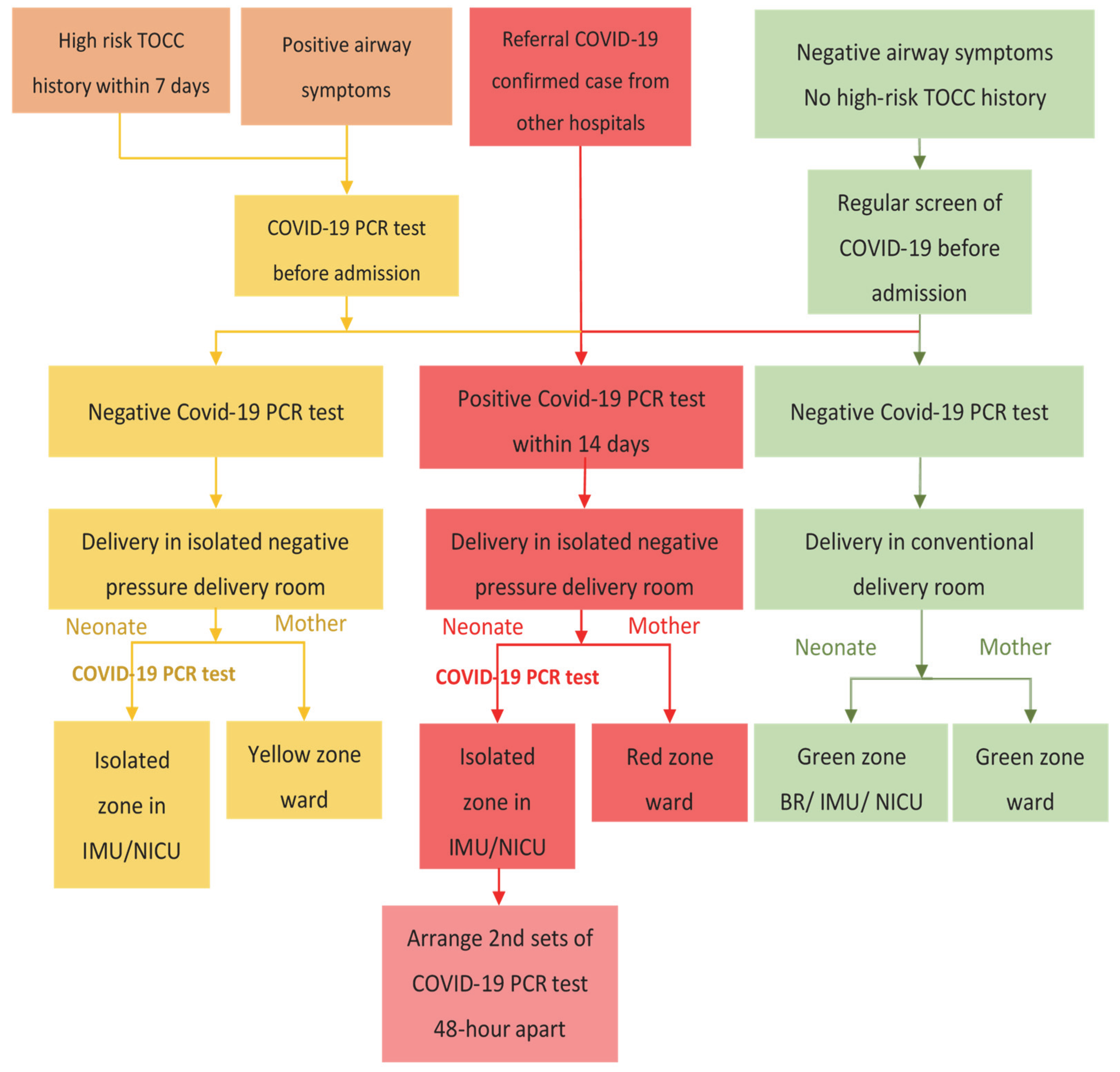
2.2. Obstetric Delivery Management Protocol
2.3. Neonatal Management Protocol
2.4. Statistics
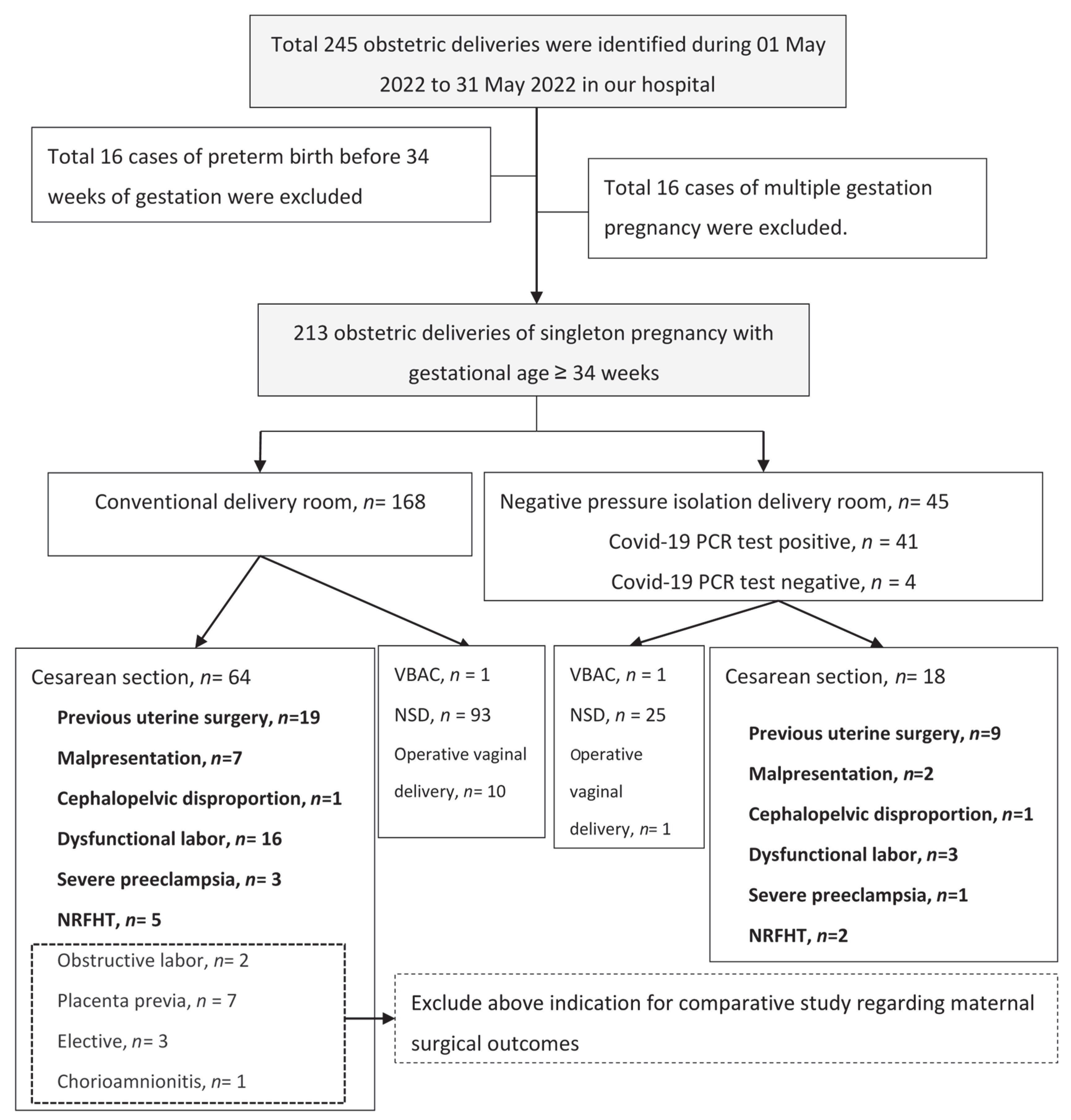
3. Results
3.1. Patient Characteristics
3.2. Maternal Surgical Outcomes
3.3. Perinatal Outcomes
3.4. Efforts on Control of COVID-19 In-Hospital Transmission
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. COVID-19 Dashboard; World Health Organization: Geneva, Switzerland, 2020; Available online: https://covid19.who.int/ (accessed on 3 July 2022).
- Seak, C.J.; Liu, Y.T.; Ng, C.J. Rapid responses in the emergency department of Linkou Chang Gung Memorial Hospital, Taiwan effectively prevent spread of COVID-19 among healthcare workers of emergency department during outbreak: Lessons learnt from SARS. Biomed. J. 2020, 43, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Chu, S.M.; Hsu, J.F.; Hsu, C.C.; Chang, Y.L.; Lien, R.; Cheng, S.W.; Chiang, M.C. Delivery management of suspected or confirmed COVID-19 positive mothers. Pediatr. Neonatol. 2021, 62, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, F.; Oros, D.; Gunier, R.B.; Deantoni, S.; Rauch, S.; Casale, R.; Nieto, R.; Bertino, E.; Rego, A.; Menis, C.; et al. Effects of prenatal exposure to maternal COVID-19 and perinatal care on neonatal outcome: Results from the INTERCOVID Multinational Cohort Study. Am. J. Obs. Gynecol. 2022, 227, 488.e1–488.e17. [Google Scholar] [CrossRef]
- Vimercati, A.; De Nola, R.; Trerotoli, P.; Metta, M.E.; Cazzato, G.; Resta, L.; Malvasi, A.; Lepera, A.; Ricci, I.; Capozza, M.; et al. COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes-A Monocentric, Single-Cohort Study. Vaccines 2022, 10, 166. [Google Scholar] [CrossRef] [PubMed]
- De Medeiros, K.S.; Sarmento, A.C.A.; Costa, A.P.F.; Macedo, L.T.A.; da Silva, L.A.S.; de Freitas, C.L.; Simoes, A.C.Z.; Goncalves, A.K. Consequences and implications of the coronavirus disease (COVID-19) on pregnancy and newborns: A comprehensive systematic review and meta-analysis. Int. J. Gynaecol. Obs. 2022, 156, 394–405. [Google Scholar] [CrossRef]
- Chi, J.; Gong, W.; Gao, Q. Clinical characteristics and outcomes of pregnant women with COVID-19 and the risk of vertical transmission: A systematic review. Arch. Gynecol. Obs. 2021, 303, 337–345. [Google Scholar] [CrossRef]
- Wang, L.M.; Lai, S.P.; Liang, S.J.; Yang, S.T.; Liu, C.H.; Wang, P.H. Maternal and fetal outcomes of the pregnant woman with COVID-19: The first case report in Taiwan. Taiwan J. Obs. Gynecol. 2021, 60, 942–944. [Google Scholar] [CrossRef]
- Chang, W.H. COVID-19 pandemic’s effects on the quality of pregnant women’s emergency treatment: Review of two cases from a medical center in northern Taiwan. Taiwan J. Obs. Gynecol. 2020, 59, 795–800. [Google Scholar] [CrossRef]
- Yang, S.T.; Yeh, C.C.; Lee, W.L.; Lee, F.K.; Chang, C.C.; Wang, P.H. A symptomatic near-term pregnant woman recovered from SARS-CoV-2 infection. Taiwan J. Obs. Gynecol. 2021, 60, 945–948. [Google Scholar] [CrossRef]
- Wang, C.-L.; Liu, Y.-Y.; Wu, C.-H.; Wang, C.-Y.; Wang, C.-H.; Long, C.-Y. Impact of COVID-19 on Pregnancy. Int. J. Med. Sci. 2021, 18, 763–767. [Google Scholar] [CrossRef]
- Pramanik, A.K.; Rangaswamy, N.; Gates, T. Neonatal respiratory distress: A practical approach to its diagnosis and management. Pediatr. Clin. N. Am. 2015, 62, 453–469. [Google Scholar] [CrossRef] [PubMed]
- De la Cuesta, R.M.R.; Del Villar Guerra, P.; Villanueva, A.M.; Alaport, V.M.; Norniella, C.M.; Albistegui, M.J.B.; Gonzalez, V.G. CPAP vs oxygen therapy in infants being transported due to acute respiratory failure. Pediatr. Engl. Ed. 2020, 93, 152–160. [Google Scholar] [CrossRef]
- Justicia-Grande, A.J.; Pardo-Seco, J.; Cebey-Lopez, M.; Vilanova-Trillo, L.; Gomez-Carballa, A.; Rivero-Calle, I.; Puente-Puig, M.; Curros-Novo, C.; Gomez-Rial, J.; Salas, A.; et al. Development and Validation of a New Clinical Scale for Infants with Acute Respiratory Infection: The ReSVinet Scale. PLoS ONE 2016, 11, e0157665. [Google Scholar] [CrossRef]
- Landoas, A.; Cazzorla, F.; Gallouche, M.; Larrat, S.; Nemoz, B.; Giner, C.; Le Marechal, M.; Pavese, P.; Epaulard, O.; Morand, P.; et al. SARS-CoV-2 nosocomial infection acquired in a French university hospital during the 1st wave of the COVID-19 pandemic, a prospective study. Antimicrob. Resist. Infect. Control 2021, 10, 114. [Google Scholar] [CrossRef]
- Du, Q.; Zhang, D.; Hu, W.; Li, X.; Xia, Q.; Wen, T.; Jia, H. Nosocomial infection of COVID-19: A new challenge for healthcare professionals (Review). Int. J. Mol. Med. 2021, 47, 31. [Google Scholar] [CrossRef] [PubMed]
- Di Toro, F.; Gjoka, M.; Di Lorenzo, G.; De Santo, D.; De Seta, F.; Maso, G.; Risso, F.M.; Romano, F.; Wiesenfeld, U.; Levi-D’Ancona, R.; et al. Impact of COVID-19 on maternal and neonatal outcomes: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women With and Without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatrics 2021, 175, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, D.J.; Rasmussen, S.A. An update on COVID-19 and pregnancy. Am. J. Obs. Gynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef]
- Allotey, J.; Fernandez, S.; Bonet, M.; Stallings, E.; Yap, M.; Kew, T.; Zhou, D.; Coomar, D.; Sheikh, J.; Lawson, H.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and COVID-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Lee, B.; Choi, Y.Y.; Um, J.; Lee, K.S.; Sung, H.K.; Kim, Y.; Park, J.S.; Lee, M.; Jang, H.C.; et al. Clinical Characteristics of 40 Patients Infected With the SARS-CoV-2 Omicron Variant in Korea. J. Korean Med. Sci. 2022, 37, e31. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.O.; Kotecha, S.J.; Kotecha, S. Respiratory Distress of the Term Newborn Infant. Paediatr. Respir. Rev. 2013, 14, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.U.; Wilkins, I.; Sun, L.; Gregory, K.; Haberman, S.; Hoffman, M.; Kominiarek, M.A.; Reddy, U.; Bailit, J. Respiratory morbidity in late preterm births. JAMA 2010, 304, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Moser, C.; Baack, M. Respiratory Distress in the Newborn. Pediatr. Rev. 2014, 35, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Monen, L.; Hasaart, T.H.; Kuppens, S.M. The aetiology of meconium-stained amniotic fluid: Pathologic hypoxia or physiologic foetal ripening? (Review). Early Hum. Dev. 2014, 90, 325–328. [Google Scholar] [CrossRef]
- Ahmad, M.; Vismara, L. The Psychological Impact of COVID-19 Pandemic on Women’s Mental Health during Pregnancy: A Rapid Evidence Review. Int. J. Env. Res. Public Health 2021, 18, 7112. [Google Scholar] [CrossRef]
- Boekhorst, M.; Muskens, L.; Hulsbosch, L.P.; Van Deun, K.; Bergink, V.; Pop, V.J.M.; van den Heuvel, M.I. The COVID-19 outbreak increases maternal stress during pregnancy, but not the risk for postpartum depression. Arch. Womens Ment. Health 2021, 24, 1037–1043. [Google Scholar] [CrossRef]
- Mayopoulos, G.A.; Ein-Dor, T.; Li, K.G.; Chan, S.J.; Dekel, S. COVID-19 positivity associated with traumatic stress response to childbirth and no visitors and infant separation in the hospital. Sci. Rep. 2021, 11, 13535. [Google Scholar] [CrossRef]
- Preis, H.; Mahaffey, B.; Pati, S.; Heiselman, C.; Lobel, M. Adverse Perinatal Outcomes Predicted by Prenatal Maternal Stress Among U.S. Women at the COVID-19 Pandemic Onset. Ann. Behav Med. 2021, 55, 179–191. [Google Scholar] [CrossRef]
- Puertas-Gonzalez, J.A.; Marino-Narvaez, C.; Peralta-Ramirez, M.I.; Romero-Gonzalez, B. The psychological impact of the COVID-19 pandemic on pregnant women. Psychiatry Res. 2021, 301, 113978. [Google Scholar] [CrossRef] [PubMed]
- Schou, T.M.; Joca, S.; Wegener, G.; Bay-Richter, C. Psychiatric and neuropsychiatric sequelae of COVID-19—A systematic review. Brain Behav. Immun. 2021, 97, 328–348. [Google Scholar] [CrossRef] [PubMed]
- Khan, D.S.A.; Hamid, L.R.; Ali, A.; Salam, R.A.; Zuberi, N.; Lassi, Z.S.; Das, J.K. Differences in pregnancy and perinatal outcomes among symptomatic versus asymptomatic COVID-19-infected pregnant women: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2021, 21, 801. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Perez, O.; Vouga, M.; Cruz Melguizo, S.; Forcen Acebal, L.; Panchaud, A.; Muñoz-Chápuli, M.; Baud, D. Association Between Mode of Delivery Among Pregnant Women With COVID-19 and Maternal and Neonatal Outcomes in Spain. JAMA 2020, 324, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Juan, J.; Gil, M.M.; Rong, Z.; Zhang, Y.; Yang, H.; Poon, L.C. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: Systematic review. Ultrasound Obs. Gynecol. 2020, 56, 15–27. [Google Scholar] [CrossRef]
- Arslan, B.; Bicer, I.G.; Sahin, T.; Vay, M.; Dilek, O.; Destegul, E. Clinical characteristics and hematological parameters associated with disease severity in COVID-19 positive pregnant women undergoing cesarean section: A single-center experience. J. Obs. Gynaecol. Res. 2022, 48, 402–410. [Google Scholar] [CrossRef]
- Khedmat, L.; Mohaghegh, P.; Veysizadeh, M.; Hosseinkhani, A.; Fayazi, S.; Mirzadeh, M. Pregnant women and infants against the infection risk of COVID-19: A review of prenatal and postnatal symptoms, clinical diagnosis, adverse maternal and neonatal outcomes, and available treatments. Arch. Gynecol. Obs. 2021, 306, 323–335. [Google Scholar] [CrossRef]
- Cuerva, M.J.; Carbonell, M.; Martin Palumbo, G.; Lopez Magallon, S.; De La Calle, M.; Bartha, J.L. Personal Protective Equipment during the COVID-19 pandemic and operative time in cesarean section: Retrospective cohort study. J. Matern.-Fetal Neonatal Med. 2022, 35, 2976–2979. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obs. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef]
- Ciapponi, A.; Bardach, A.; Comande, D.; Berrueta, M.; Argento, F.J.; Rodriguez Cairoli, F.; Zamora, N.; Santa Maria, V.; Xiong, X.; Zaraa, S.; et al. COVID-19 and pregnancy: An umbrella review of clinical presentation, vertical transmission, and maternal and perinatal outcomes. PLoS ONE 2021, 16, e0253974. [Google Scholar] [CrossRef]
- Tolu, L.B.; Ezeh, A.; Feyissa, G.T. Vertical transmission of Severe Acute Respiratory Syndrome Coronavirus 2: A scoping review. PLoS ONE 2021, 16, e0250196. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Delivery Room (n = 168) | Isolated Negative Pressure Room (n = 45) | p-Value | |||
|---|---|---|---|---|---|
| Age (median) | 32 (19–44) | 30 (18–44) | 0.082 † | ||
| BMI(median) | 26.6 (17.9–47.6) | 27.5 (19.6–43.6) | 0.218 † | ||
| Gravida (median) | 2 (1–6) | 2 (1–8) | 0.022 † | ||
| Primi-gravida | 98 (58.3%) | 17 (37.8%) | 0.014 * | ||
| Gestational age by weeks (median) | 38 3/7 (34 3/7–40 6/7) | 38 4/7 (34 4/7–40 2/7) | 0.305 † | ||
| GDM | 19 (11.3%) | 4 (8.9%) | 0.791 ◊ | ||
| PIH | 6 (3.6%) | 4 (8.9%) | 0.224 ◊ | ||
| Preeclampsia | 7 (4.2%) | 2 (4.4%) | 1.000 ◊ | ||
| IUGR | 3 (1.8%) | 0 | 1.000 ◊ | ||
| Medical diseases | 21 (12.5%) | 2 (4.4%) | 0.176 ◊ | ||
| COVID-19 PCR test results | Negative | 168 | Negative | 4 | - |
| Positive | 0 | Positive | 41 | - | |
| Delivery Mode | |||||
| Vaginal delivery | 93 (55.4%) | 25 (55.6%) | 0.981 * | ||
| Operative vaginal delivery | 10 (6.0%) | 1 (2.2%) | 0.464 ◊ | ||
| VBAC | 1 (0.6%) | 1 (2.2%) | 0.379 ◊ | ||
| Cesarean section | 64 (38.1%) | 18 (40.0%) | 0.816 * | ||
| Primary CS | 38 (22.6%) | 7 (15.6%) | 0.304 * | ||
| Emergent CS | 16 (9.5%) | 9 (20.0%) | 0.053 * | ||
| Total CS rate | 38.1% | 40.0% | 0.816 * | ||
| Primary CS rate | 38/(38 + 93 + 10) = 26.8% | 7/(25 + 1 + 7) = 21.2% | 0.312 * | ||
| COVID-19 Confirmed Case, n = 41 | Close Contact with Confirmed Case, n = 4 | |
|---|---|---|
| COVID-19 PCR test | Positive = 41 | Positive = 0 |
| Referral cases | 29 | 3 |
| Symptoms of COVID-19 infection | ||
| Fever | 9 | 0 |
| Cough | 18 | 0 |
| Sore throat | 16 | 0 |
| Muscle or body aches | 4 | 0 |
| Congestion or rhinorrhea | 3 | 0 |
| Shortness of breath | 0 | 0 |
| Asymptomatic | 9 | 4 |
| Delivery Room, n = 104 | Isolated Negative Pressure Room, n = 27 | p-Value | |
|---|---|---|---|
| Age (median) | 31.5 (19–43) | 30 (20–41) | 0.109 † |
| BMI (median) | 25.50 (17.9–47.6) | 27.34 (19.6–35.5) | 0.276 † |
| Gravida (median) | 2 (1–6) | 2 (1–8) | 0.021 † |
| Primigravida | 60 (57.7%) | 10 (37.0%) | 0.056 * |
| Gestational age by weeks (median) | 38 4/7 (34 1/7–40 6/7) | 38 5/7 (34 3/7–40 2/7) | 0.393 † |
| GBS colonization | 23 (22.1%) | 6 (22.2%) | 0.839 ◊ |
| GDM | 11 (10.6%) | 2 (7.4%) | 1.000 ◊ |
| PIH | 2 (1.9%) | 1 (3.7%) | 0.503 ◊ |
| Preeclampsia | 4 (3.7%) | 0 (0.0%) | 0.583 ◊ |
| IUGR | 3 (3.9%) | 0 (0.0%) | 1.000 ◊ |
| Medical diseases | 10 (9.6%) | 1 (3.7%) | 0.459 ◊ |
| Delivery Mode | |||
| NSD | 93 (89.4%) | 25 (92.6%) | 0.625 * |
| Operative vaginal delivery | 10 (9.6%) | 1 (3.7%) | 0.459 ◊ |
| VBAC | 1 (1.00%) | 1 (3.7%) | 0.371 ◊ |
| Trial of Labor | |||
| Rupture of membrane | 12 (11.5%) | 5 (18.5%) | 0.409 ◊ |
| In labor | 26 (25.0%) | 18 (66.7%) | <0.001 * |
| Induction of labor | 66 (63.5%) | 4 (14.8%) | <0.001 ◊ |
| Maternal Surgical Outcome | |||
| Change to CS (%) | 16 (15.4%) | 0 (0.0%) | <0.001 † |
| 1st stage of labo(min) | 242.5 (15–1050) | 160 (30–930) | 0.005 † |
| 2nd stage of labor (min) | 48 (6–217) | 27 (4–108) | 0.009 † |
| 3rd stage of labor (min) | 1 (1–13) | 1 (1–6) | 0.416 † |
| Total labor (min) | 300.5 (35–1077) | 190 (35–978) | 0.003 † |
| Time of stay in delivery unit (min) | 1119.5 (148–3967) | 547 (133–1843) | 0.001 † |
| Epidural analgesia (%) | 94 (90.4%) | 0 (0.0%) | <0.001 ◊ |
| Blood loss (mL) | 200 (100–400) | 200 (200–850) | 0.102 † |
| Operative time (min) | 24 (12–54) | 25 (19–54) | 0.080 † |
| 3rd- to 4th-degree lacerations (%) | 15 (14.4%) | 2 (7.4%) | 0.522 ◊ |
| Re-admission in 14 days | 1 (1.0%) | 1 (3.7%) | 0.369 ◊ |
| Delivery Room, n = 51 | Isolated Negative Pressure Room, n = 18 | p-Value | |
|---|---|---|---|
| Age (median) | 34 (23–44) | 32 (18–44) | 0.377 † |
| BMI (median) | 27.5 (21.3–38.1) | 28.4 (22.2–43.6) | 0.280 † |
| Gravida (median) | 2 (1–5) | 2 (1–6) | 0.348 † |
| Para (median) | 1 (1–4) | 2 (1–4) | 0.358 † |
| Abortus (median) | 0 (0–4) | 0 (0–4) | 0.694 † |
| Gestational age by weeks (median) | 38 1/7 (34 2/7–40 1/7) | 38 1.5/7 (35 3/7–40) | 0.722 † |
| GDM | 6 (11.8%) | 2 (11.1%) | 1.000 ◊ |
| PIH | 2 (3.9%) | 3 (16.7%) | 0.107 ◊ |
| Preeclampsia | 2 (3.9%) | 2 (11.1%) | 0.277 ◊ |
| IUGR | 0 | 0 | - |
| Medical diseases | 6 (11.8%) | 1 (5.6%) | 0.665 ◊ |
| Emergent cesarean section | 15 (29.4%) | 9 (50.0%) | 0.118 |
| Cesarean Section Indications | |||
| Previous uterine surgery | 19 (37.3%) | 9 (50.0%) | 0.347 * |
| Malpresentation | 7 (13.7%) | 2 (5.6%) | 1.000 ◊ |
| Cephalopelvic disproportion | 1 (2.0%) | 1 (5.6%) | 0.457 ◊ |
| Dysfunctional labor | 16 (31.4%) | 3 (11.1%) | 0.358 ◊ |
| Severe preeclampsia | 3 (5.9%) | 1 (5.6%) | 1.000 ◊ |
| NRFHT | 5 (9.8%) | 2 (11.1%) | 1.000 ◊ |
| Maternal Outcome Paired with Indications of Cesarean Deliveries | |||
| Blood loss (mL) | 500 (300–1800) | 425 (200–1100) | 0.365 † |
| Postpartum hemorrhage (%) | 6 (11.8%) | 2 (11.1%) | 1.000 ◊ |
| Operative time (min) | 81 (39–126) | 91 (64–127) | 0.111 † |
| Delivery Room, n = 168 | Isolated Negative Pressure Room, n = 45 | p-Value | |
|---|---|---|---|
| Birth weight (gm) | 3040 (1765–3825) | 3090 (2006–4010) | 0.215 † |
| MSAF | 7 (4.2%) | 10 (22.2%) | <0.001 * |
| Apgar score’1 < 7 | 3 (1.8%) | 0 | 1.000 ◊ |
| Apgar score’5 < 7 | 0 | 0 | - |
| NICU admission | 14 (8.3%) | 25 (55.6%) | <0.001 * |
| Neonatal respiratory distress | 18 (10.7%) | 18 (40.0%) | <0.001 * |
| Oxygen therapy | 16 (9.5%) | 12 (26.7%) | 0.003 * |
| Median Downes’ score | 4 (2–5) | 3 (2–5) | 0.209 † |
| Downes’ score < 4 | 5 (27.8%) | 9 (52.9%) | 0.176 ◊ |
| Downes’ score 4–7 | 13 (72.2%) | 8 (47.2%) | 0.134 * |
| Downes’ score > 7 | 0 | 0 | - |
| Neonatal fever | 10 (6.0%) | 1 (2.2%) | 0.464 ◊ |
| Antibiotic use | 26 (15.5%) | 17 (37.8%) | 0.001 * |
| Median hospitalization (days) | 4 (3–19) | 5 (3–12) | <0.001 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, Y.-C.; Wu, P.-C.; Chiu, L.-C.; Chueh, H.-Y.; Chen, Y.-N.; Lee, Y.-C.; Li, W.-F.; Chiang, C.-Y.; Hsu, C.-C.; Peng, H.-H.; et al. Maternal–Neonatal Outcomes of Obstetric Deliveries Performed in Negative Pressure Isolation Rooms during the COVID-19 Omicron Variant Pandemic in Taiwan: A Retrospective Cohort Study of a Single Institution. J. Clin. Med. 2022, 11, 5441. https://doi.org/10.3390/jcm11185441
Liao Y-C, Wu P-C, Chiu L-C, Chueh H-Y, Chen Y-N, Lee Y-C, Li W-F, Chiang C-Y, Hsu C-C, Peng H-H, et al. Maternal–Neonatal Outcomes of Obstetric Deliveries Performed in Negative Pressure Isolation Rooms during the COVID-19 Omicron Variant Pandemic in Taiwan: A Retrospective Cohort Study of a Single Institution. Journal of Clinical Medicine. 2022; 11(18):5441. https://doi.org/10.3390/jcm11185441
Chicago/Turabian StyleLiao, Yi-Chiao, Ping-Chung Wu, Li-Chun Chiu, Ho-Yen Chueh, Yu-Ning Chen, Yen-Chang Lee, Wen-Fang Li, Chi-Yuan Chiang, Chin-Chieh Hsu, Hsiu-Huei Peng, and et al. 2022. "Maternal–Neonatal Outcomes of Obstetric Deliveries Performed in Negative Pressure Isolation Rooms during the COVID-19 Omicron Variant Pandemic in Taiwan: A Retrospective Cohort Study of a Single Institution" Journal of Clinical Medicine 11, no. 18: 5441. https://doi.org/10.3390/jcm11185441