
A Pictorial Review of the Role of Imaging in the Detection, Management, Histopathological Correlations, and Complications of COVID-19 Pneumonia

 , , ,
, , ,
Abstract
:1. Introduction
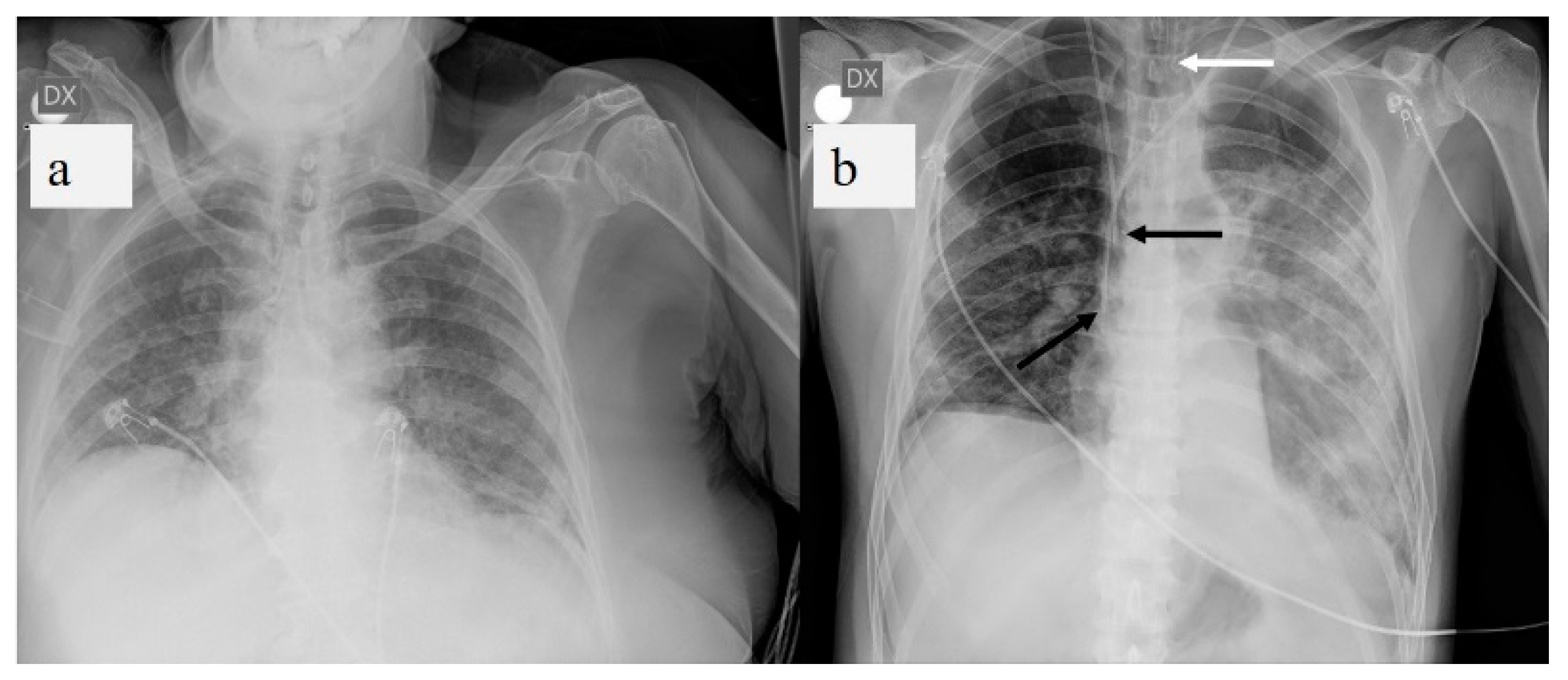
2. Chest X-ray
2.1. Chest X-ray: Role and Limitations
2.2. Chest X-ray: Protocols
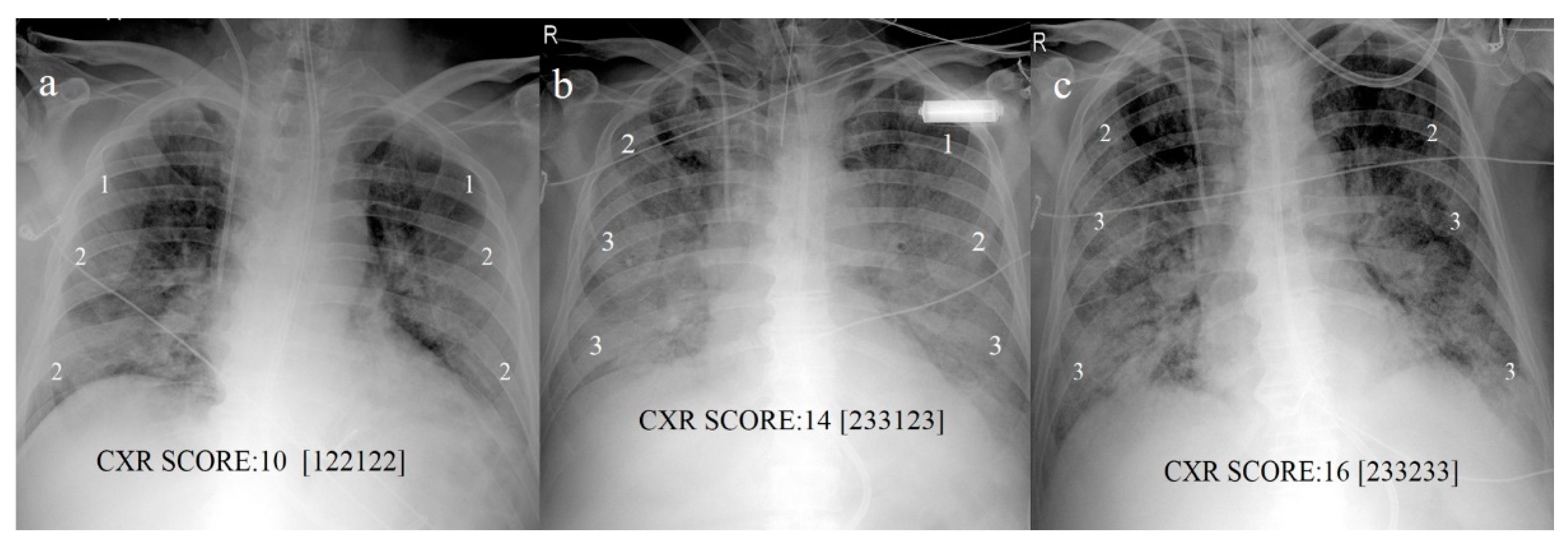
2.3. Chest X-ray: Scoring System
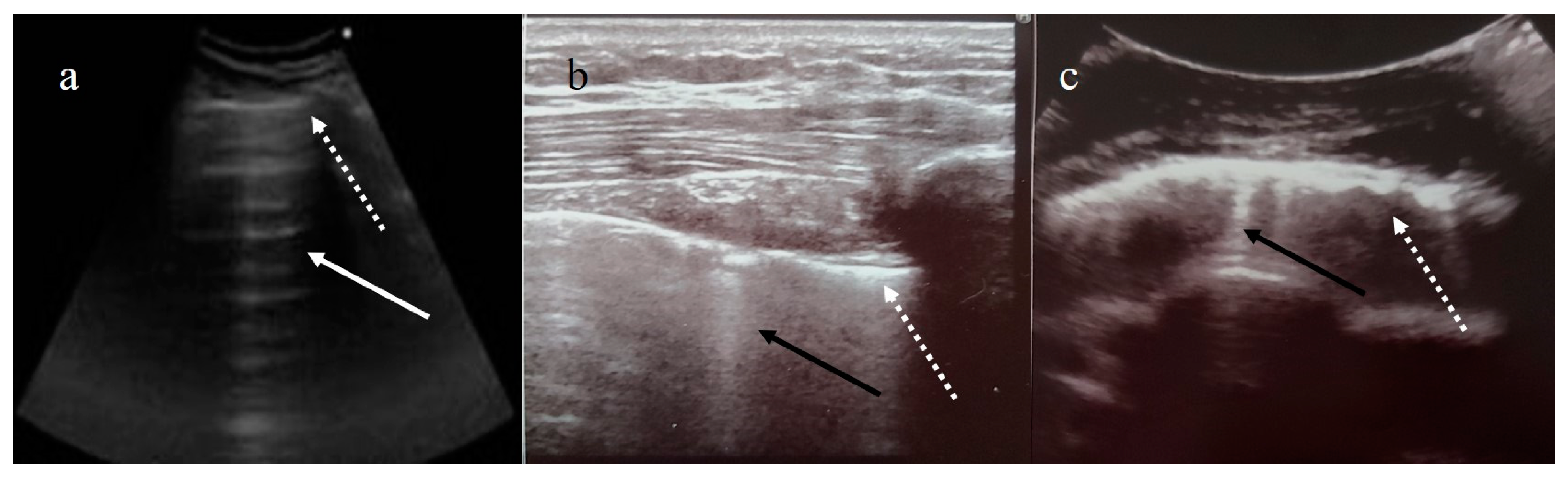
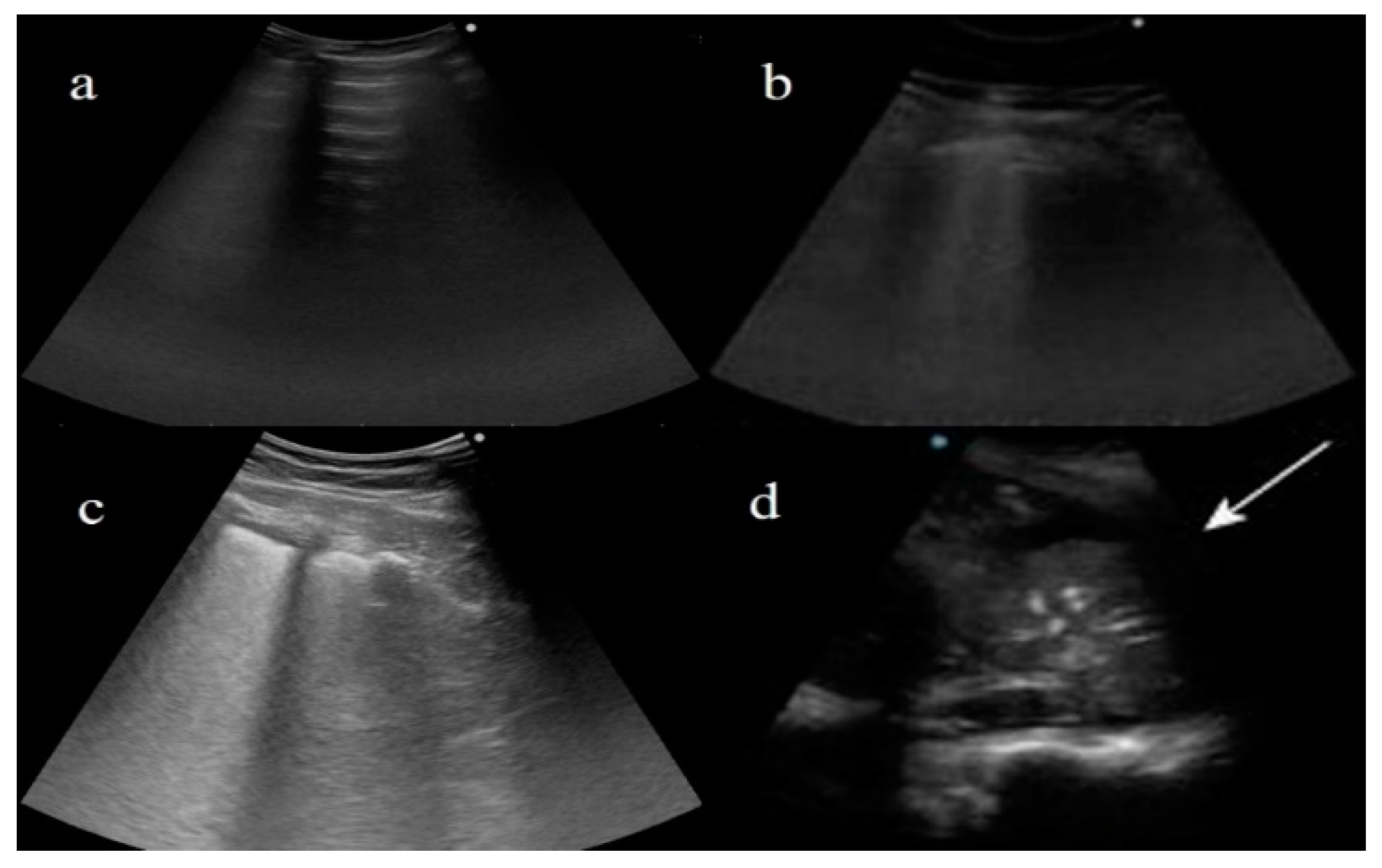
3. Lung Ultrasound
3.1. Lung Ultrasound: Role and Limitations
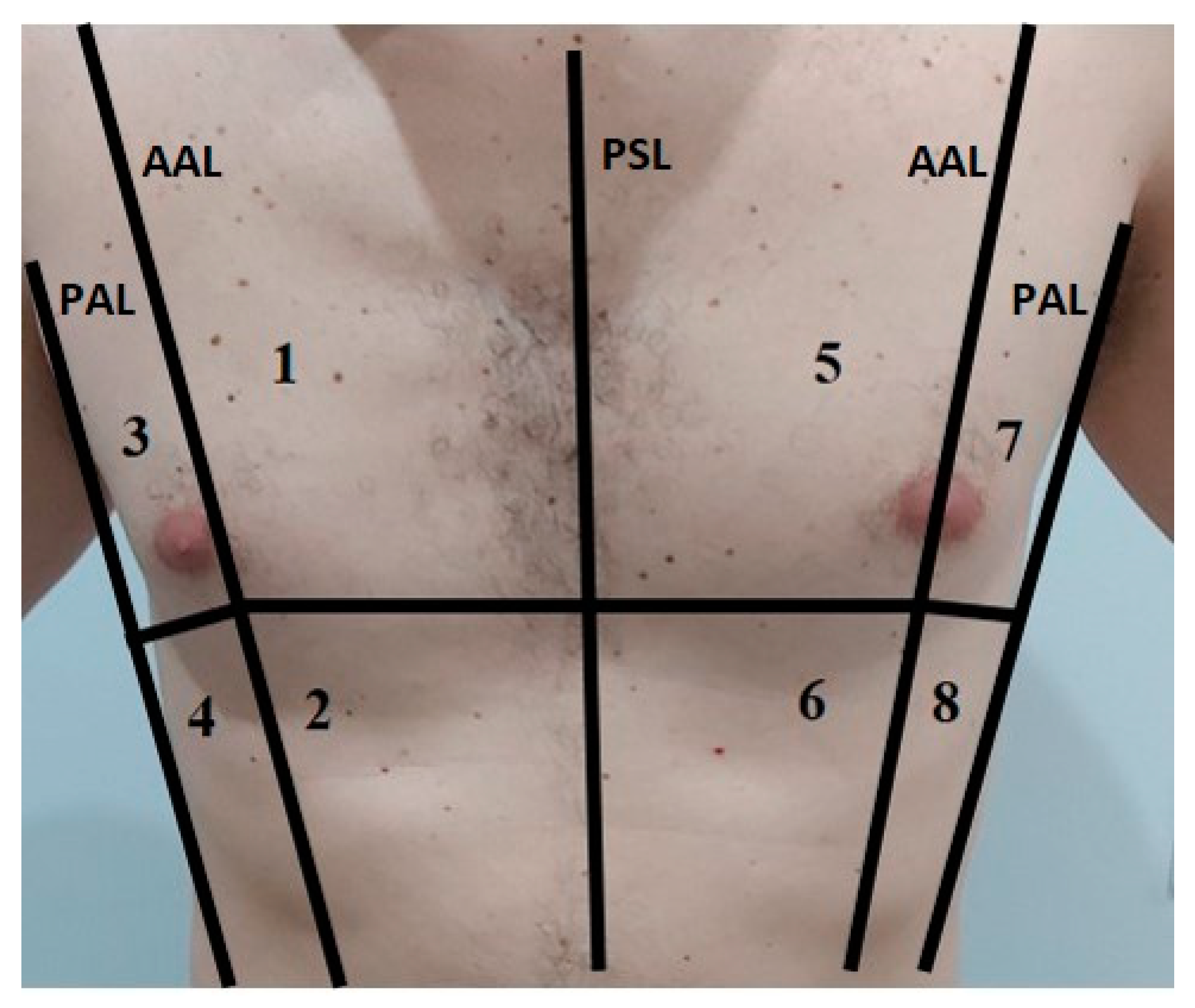
3.2. Lung Ultrasound: Protocols
3.3. Lung Ultrasound Scoring System
4. Chest CT
4.1. Chest CT: Role and Limitations
4.2. Chest CT Protocols
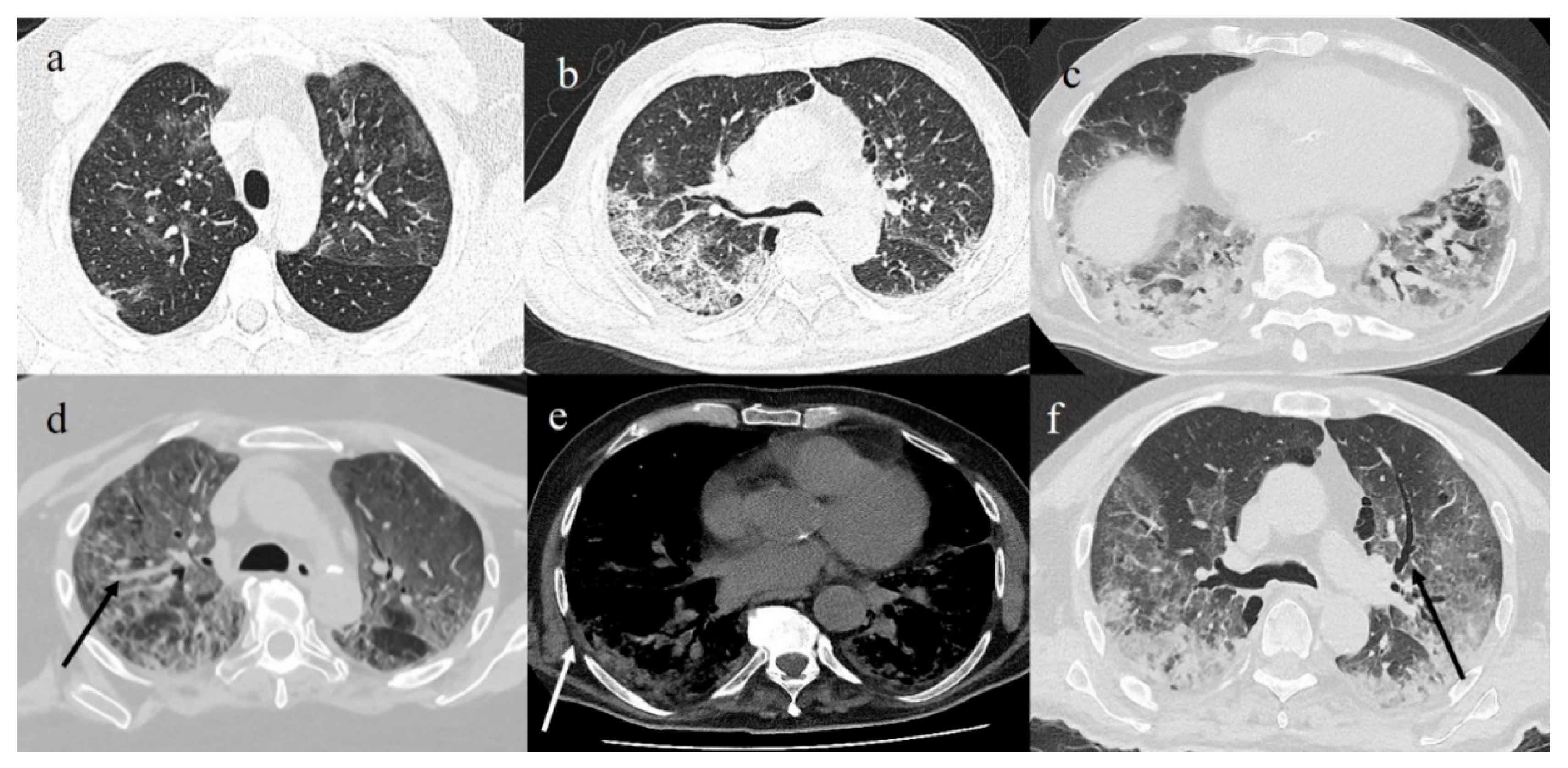
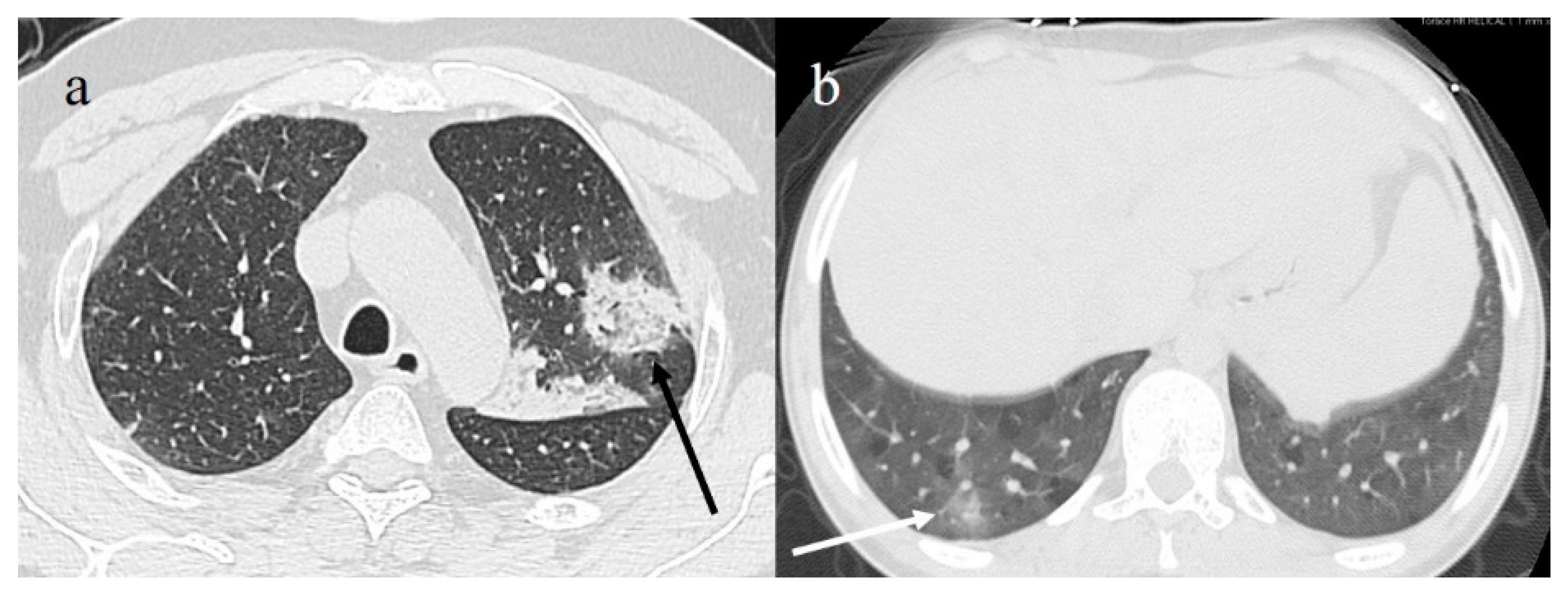
4.3. COVID-19 CT Features and Reporting System
4.4. COVID-19 Pneumonia CT Staging
4.5. CT Severity Scores as Prognostic and Predictive Indicators of Clinical Outcome
5. Imaging and Histopathological Correlations
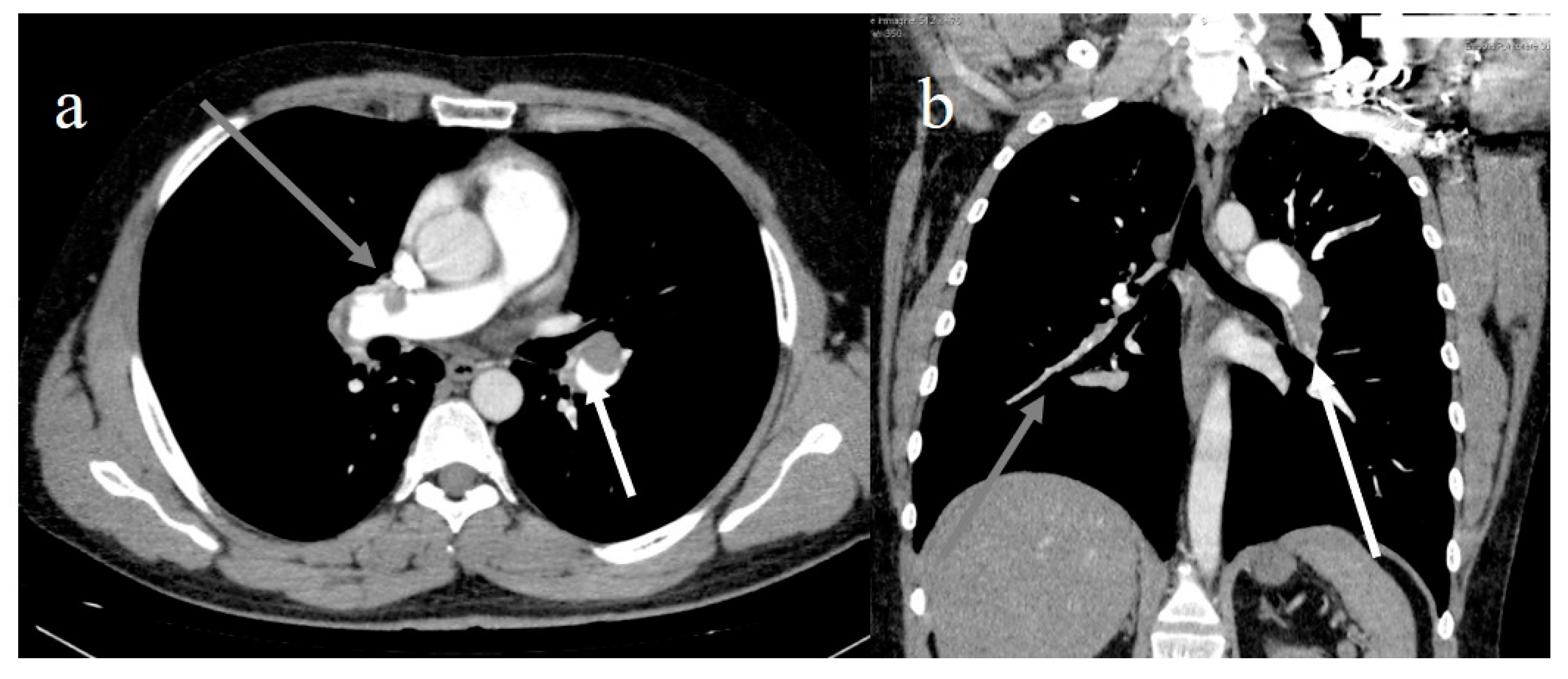
6. COVID-19 Complications
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Apolone, G.; Montomoli, E.; Manenti, A.; Boeri, M.; Sabia, F.; Hyseni, I.; Mazzini, L.; Martinuzzi, D.; Cantone, L.; Milanese, G.; et al. Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy. Tumori J. 2020. [Google Scholar] [CrossRef]
- Deslandes, A.; Berti, V.; Tandjaoui-Lambotte, Y.; Alloui, C.; Carbonnelle, E.; Zahar, J.R.; Brichlera, S.; Cohen, Y. SARS-COV-2 was already spreading in France in late December 2019. Int. J. Antimicrob. Agents 2020, 55, 106006. [Google Scholar] [CrossRef] [PubMed]
- Stawicki, S.P.; Jeanmonod, R.; Miller, A.C.; Paladino, L.; Gaieski, D.F.; Yaffee, A.Q.; De Wulf, A.; Grover, J.; Papadimos, T.J.; Bloem, C.; et al. The 2019–2020 novel coronavirus (severe acute respiratory syndrome coronavirus 2) pandemic: A joint american college of academic international medicine-world academic council of emergency medicine multidisciplinary COVID-19 working group consensus paper. J. Glob. Infect. Dis. 2020, 12, 47–93. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal–Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.; Mu, J.; Guo, J.; Lu, L.; Liu, D.; Luo, J.; Li, N.; Liu, J.; Yang, D.; Gao, H.; et al. New onset neurologic events in people with COVID-19 infection in three regions in China. Neurology 2020, 95, 1479–1487. [Google Scholar] [CrossRef]
- Wu, Y.; Guo, C.; Tang, L.; Hong, Z.; Zhou, J.; Dong, X.; Yin, H.; Xiao, Q.; Tang, Y.; Qu, X.; et al. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol. Hepatol. 2020, 5, 434–435. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Yao, L.; Li, J.; Chen, L.; Song, Y.; Cai, Z.; Yang, C. Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19. J. Med Virol. 2020, 92, 903–908. [Google Scholar] [CrossRef] [Green Version]
- The Interference Factors in Coronavirus 2 Nucleic Acid Detection 2020. Available online: https://kns.cnki.net/kcms/detail/50.1167.R.20200317.1710.002.html (accessed on 25 March 2020).
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The role of chest imaging in patient management during the COVID-19 pandemic: A multinational consensus statement from the Fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef]
- Blažić, I.; Brkljačić, B.; Frija, G. The use of imaging in COVID-19—results of a global survey by the International Society of Radiology. Eur. Radiol. 2021, 31, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.; Rodrigues, J.; Hare, S.; Edey, A.; Devaraj, A.; Jacob, J.; Johnstone, A.; McStay, R.; Denton, E.; Robinson, G. A British Society of Thoracic Imaging statement: Considerations in designing local imaging diagnostic algorithms for the COVID-19 pandemic. Clin. Radiol. 2020, 75, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Dennie, C.; Hague, C.; Lim, R.S.; Manos, D.; Memauri, B.F.; Nguyen, E.T.; Taylor, J. Canadian Society of Thoracic Radiology/Canadian Association of Radiologists Consensus Statement Regarding Chest Imaging in Suspected and Confirmed COVID-19. Can. Assoc. Radiol. J. 2020, 71, 470–481. [Google Scholar] [CrossRef]
- Neri, E.; Coppola, F.; Larici, A.R.; Sverzellati, N.; Mazzei, M.A.; Sacco, P.; Dalpiaz, G.; Feragalli, B.; Miele, V.; Grassi, R. Structured reporting of chest CT in COVID-19 pneumonia: A consensus proposal. Insights Imaging 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Fusco, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Petrillo, A.; Granata, V.; Sacco, P.; Mazzei, M.A.; et al. Coronavirus disease 2019 (COVID-19) in Italy: Features on chest computed tomography using a structured report system. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- The Royal College of Radiologists. The Role of CT in Patients Suspected with COVID-19 Infection. Available online: https://www.rcr.ac.uk/college/coronavirus-covid-19-what-rcr-doing/clinical-information/role-ct-chest/role-ct-patients (accessed on 15 June 2020).
- Royal Australia and New Zealand College of Radiologists (2020) Guidelines for CT chest and Chest Radiograph Reporting in Patients with Suspected COVID-19 Infection. Available online: www.ranzcr.com/college/document-library/guidelines-for-ct-chest-and-chestradio-graph-reporting-in-patients-with-suspected-covid-19-infection (accessed on 15 June 2020).
- Revel, M.P.; Parkar, A.P.; Prosch, H.; Silva, M.; Sverzellati, N.; Gleeson, F.; Brady, A. COVID-19 patients and the radiology department – advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur. Radiol. 2020, 30, 4903–4909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akl, E.A.; Blažić, I.; Yaacoub, S.; Frija, G.; Chou, R.; Appiah, J.A.; Fatehi, M.; Flor, N.; Hitti, E.; Jafri, H.; et al. Use of Chest Imaging in the Diagnosis and Management of COVID-19: A WHO Rapid Advice Guide. Radiology 2021, 298, E63–E69. [Google Scholar] [CrossRef]
- Chinese Society of Radiology. Radiological diagnosis of new coronavirus infected pneumonitis: Expert recommendation from the Chinese Society of Radiology (First Edition). Chin. J. Radiol. 2020, 54, 1. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interim Clinical Guidance for Management of Patients with Confirmed Coro-navirus Disease (COVID-19). Available online: Managementpatients.html (accessed on 16 April 2020).
- ACR Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. Available online: https://www.acr.org/Advocacy-and-Economics/ACR-PositionStatements/Recommendations-for-Chest-Radiography-and-CTfor-Suspected-COVID19-Infection (accessed on 16 April 2020).
- Brogna, B.; Bignardi, E.; Brogna, C.; Alberigo, M.; Grappone, M.; Megliola, A.; Salvatore, P.; Fontanella, G.; Mazza, E.; Musto, L. Typical CT findings of COVID-19 pneumonia in patients presenting with repetitive negative RT-PCR. Radiography 2020. [Google Scholar] [CrossRef]
- Vespro, V.; Andrisani, M.C.; Fusco, S.; Di Meglio, L.; Plensich, G.; Scarabelli, A.; Stellato, E.; Ierardi, A.M.; Scudeller, L.; Coppola, A.; et al. Chest X-ray findings in a large cohort of 1117 patients with SARS-CoV-2 infection: A multicenter study during COVID-19 outbreak in Italy. Intern. Emerg. Med. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Jung, H.K.; Kim, J.Y.; Lee, M.S.; Lee, J.Y.; Park, J.S.; Hyun, M.; Kim, H.A.; Kwon, Y.S.; Choi, S.-W.; Moon, S.M.; et al. Characteristics of COVID-19 Patients Who Progress to Pneumonia on Follow-Up Chest Radiograph: 236 Patients from a Single Isolated Cohort in Daegu, South Korea. Korean J. Radiol. 2020, 21, 1265. [Google Scholar] [CrossRef] [PubMed]
- Maroldi, R.; Rondi, P.; Agazzi, G.M.; Ravanelli, M.; Borghesi, A.; Farina, D. Which role for chest x-ray score in predicting the outcome in COVID-19 pneumonia? Eur. Radiol. 2020, 2, 1–7. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Xia, L. Coronavirus Disease 2019 (COVID-19): Role of Chest CT in Diagnosis and Management. Am. J. Roentgenol. 2020, 214, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, A.; Schiaffino, S.; Arpaia, F.; Della Pepa, G.; Tritella, S.; Bertolotti, P.; Menicagli, L.; Monaco, C.G.; Carbonaro, L.A.; Spairani, R.; et al. Chest x-ray in the COVID-19 pandemic: Radiologists’ real-world reader performance. Eur. J. Radiol. 2020, 132, 109272. [Google Scholar] [CrossRef]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Weinstock, M.B.; Echenique, A.; Russell, J.W.; Leib, A.; Miller, J.A.; Cohen, D.Y.; Waite, S.; Frye, A.; Illuzzi, F.A. Chest X-ray findings in 636 ambula-tory patients with COVID-19 presenting to an urgent care center: A normal chest x-ray is no guarantee. J. Urgent. Care. Med. 2020, 14, 13–18. Available online: www.jucm.com (accessed on 1 May 2020).
- Schiaffino, S.; Tritella, S.; Cozzi, A.; Carriero, S.; Blandi, L.; Ferraris, L.; Sardanelli, F. Diagnostic Performance of Chest X-Ray for COVID-19 Pneumonia During the SARS-CoV-2 Pandemic in Lombardy, Italy. J. Thorac. Imaging 2020, 35, W105–W106. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Lee, K.H.; Kim, J.Y.; Lee, Y.K.; Ko, H.; Kim, K.H.; Park, C.M.; Kim, Y.-H. Chest Radiographic and CT Findings of the 2019 Novel Coronavirus Disease (COVID-19): Analysis of Nine Patients Treated in Korea. Korean J. Radiol. 2020, 21, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.; Leung, S.T.; Chin, T.W.; Lo, C.S.Y.; Lui, M.M.-S.; Lee, J.C.Y.; Chiu, K.W.-H.; Chung, T.W.-H.; et al. Frequency and distribution of chest radio-graphic findings in COVID-19 positive patients. Radiology 2020, 296, 72–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martino, A.; Fiore, E.; Mazza, E.M.; Minichiello, S.; Brogna, B.; Petronilla, S.; Megliola, A.; Musto, L. CT features of coronavirus disease 2019 (COVID-19) pneumonia: Experience of a single center in Southern Italy. Infez. Med. 2020, 28, 104–110. [Google Scholar] [PubMed]
- Gatti, M.; Calandri, M.; Barba, M.; Biondo, A.; Geninatti, C.; Gentile, S.; Greco, M.; Morrone, V.; Piatti, C.; Santonocito, A.; et al. Baseline chest X-ray in coronavirus disease 19 (COVID-19) patients: Association with clinical and laboratory data. Radiol. Med. 2020, 125, 1271–1279. [Google Scholar] [CrossRef]
- Intersociety Recommendations for Reporting Dose Class. Italian Society of Medical and Interventional Radiology (SIRM). Available online: https://www.sirm.org/ (accessed on 1 December 2020).
- Radiological Procedures and Prevention of the Spread of COVID-19 in the Radiology Departments. Italian Society of Medi-cal and Interventional Radiology (SIRM). Available online: https://www.sirm.org/wp-con-tent/uploads/2020/03/Procedure-covid19_cotugno.pdf (accessed on 1 March 2020).
- Xiang, C.; Huang, L.; Xia, L. Mobile chest X-ray manifestations of 54 deceased patients with coronavirus disease 2019. Medicine 2020, 99, e23167. [Google Scholar] [CrossRef]
- Mollura, D.J.; Palmore, T.N.; Folio, L.R.; Bluemke, D.A. Radiology Preparedness in Ebola Virus Disease: Guidelines and Challenges for Disinfection of Medical Imaging Equipment for the Protection of Staff and Patients. Radiology 2015, 275, 538–544. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Ding, N.; Chen, H.; Liu, X.-J.; He, W.-J.; Dai, W.-C.; Zhou, Z.-G.; Lin, F.; Pu, Z.-H.; Li, D.-F.; et al. Infection Control against COVID-19 in Departments of Radiology. Acad. Radiol. 2020, 27, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.; Shivers Investigation On Behalf of the SHIVERS Investigation Team; Haven, K.; Reed, P.; Bissielo, A.; Harvey, D.; McArthur, C.; Bringans, C.; Freundlich, S.; Ingram, R.J.H.; et al. A chest radiograph scoring system in patients with severe acute respiratory infection: A validation study. BMC Med. Imaging 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Warren, M.A.; Zhao, Z.; Koyama, T.; Bastarache, J.A.; Shaver, C.M.; Semler, M.W.; Rice, T.W.; Matthay, M.A.; Calfee, C.S.; Ware, L.B. Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS. Thorax 2018, 73, 840–846. [Google Scholar] [CrossRef]
- Toussie, D.; Voutsinas, N.; Finkelstein, M.; Cedillo, M.A.; Manna, S.; Maron, S.Z.; Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C.; et al. Clinical and Chest Radiography Features Determine Patient Outcomes In Young and Middle Age Adults with COVID-19. Radiology 2020, 297, E197–E206. [Google Scholar] [CrossRef] [PubMed]
- Yates, A.; Dempsey, P.J.; Vencken, S.; MacMahon, P.J.; Hutchinson, B.D. Structured reporting in portable chest radiographs: An essential tool in the diagnosis of COVID-19. Eur. J. Radiol. 2021, 134, 109414. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Albanesi, M.; Cavigli, E.; Moroni, C.; Bindi, A.; Luvarà, S.; Lucarini, S.; Busoni, S.; Mazzoni, L.N.; Miele, V. Chest X-ray in new Coronavirus Disease 2019 (COVID-19) infection: Findings and correlation with clinical outcome. La Radiol. Med. 2020, 125, 730–737. [Google Scholar] [CrossRef]
- Murphy, K.; Smits, H.; Knoops, A.J.G.; Korst, M.B.J.M.; Samson, T.; Scholten, E.T.; Schalekamp, S.; Schaefer-Prokop, C.M.; Philipsen, R.H.H.M.; Meijers, A.; et al. COVID-19 on Chest Radiographs: A Multireader Evaluation of an Artificial Intelligence System. Radiology 2020, 296, E166–E172. [Google Scholar] [CrossRef] [PubMed]
- Haak, S.L.; Renken, I.J.; Jager, L.C.; Lameijer, H.; van der Kolk, B.B.Y. Diagnostic accuracy of point-of-care lung ultrasound in COVID-19. Emerg. Med. J. 2021, 38, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID -19. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yassa, M.; Yirmibes, C.; Cavusoglu, G.; Eksi, H.; Dogu, C.; Usta, C.; Mutlu, M.; Birol, P.; Gulumser, C. Outcomes of universal SARS-CoV-2 testing pro-gram in pregnant women admitted to hospital and the adjuvant role of lung ultrasound in screening: A prospective cohort study. J. Matern. Fetal. Neonatal. Med. 2020, 33, 3820–3826. [Google Scholar] [CrossRef]
- Giorno, E.P.C.; De Paulis, M.; Sameshima, Y.T.; Weerdenburg, K.; Savoia, P.; Nanbu, D.Y.; Couto, T.B.; Sa, F.V.M.; Farhat, S.C.L.; Carvalho, W.B.; et al. Point-of-care lung ultrasound imaging in pediatric COVID-19. Ultrasound J. 2020, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Iodice, V.; Pisaturo, M.; Fusco, F.M.; Tambaro, O.; Parrella, G.; Bignardi, E.; Viglietti, R.; Pisapia, R.; Palmiero, G.; Bignardi, E.; et al. Use of lung ultrasound in COVID-19: Com-parison with ultra-high-resolution computed tomography among 29 patients at “D. Cotugno” hospital, Naples, Italy. Infez. Med. 2020, 28, 346–350. [Google Scholar] [PubMed]
- Marino, F.; Martorano, C.; Tripepi, R.; Bellantoni, M.; Tripepi, G.; Mallamaci, F.; Zoccali, C. Subclinical pulmonary congestion is prevalent in nephrotic syndrome. Kidney Int. 2016, 89, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Q.-Y.; Chinese Critical Care Ultrasound Study Group (CCUSG); Wang, X.-T.; Zhang, L.-N. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensiv. Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lomoro, P.; Verde, F.; Zerboni, F.; Simonetti, I.; Borghi, C.; Fachinetti, C.; Natalizi, A.; Martegani, A. COVID-19 pneumonia manifestations at the admission on chest ultrasound, radiographs, and CT: Single-center study and comprehensive radiologic literature review. Eur. J. Radiol. Open 2020, 7, 100231. [Google Scholar] [CrossRef]
- Sperandeo, M.; Filabozzi, P.; Carnevale, V. Ultrasound Diagnosis of Ventilator-Associated Pneumonia. Chest 2016, 149, 1350–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinti, M.G.; Quarato, C.M.I.; Sperandeo, M. Transthoracic Ultrasound in Pneumothorax. Ann. Thorac. Surg. 2020, 109, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrer, L.; Donini, E.; Marinelli, D.; Zanetti, M.; Mento, F.; Torri, E.; Smargiassi, A.; Inchingolo, R.; Soldati, G.; Demi, L.; et al. Automatic Pleural Line Extraction and COVID-19 Scoring From Lung Ultrasound Data. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2020, 67, 2207–2217. [Google Scholar] [CrossRef]
- Bonadia, N.; Carnicelli, A.; Piano, A.; Buonsenso, D.; Gilardi, E.; Kadhim, C.; Torelli, E.; Petrucci, M.; Di Maurizio, L.; Biasucci, D.G.; et al. Lung Ultrasound Findings Are Associated with Mortality and Need for Intensive Care Admission in COVID-19 Patients Evaluated in the Emergency Department. Ultrasound Med. Biol. 2020, 46, 2927–2937. [Google Scholar] [CrossRef] [PubMed]
- Dargent, A.; Chatelain, E.; Kreitmann, L.; Quenot, J.-P.; Cour, M.; Argaud, L.; The COVID-LUS Study Group. Lung ultrasound score to monitor COVID-19 pneumonia progression in patients with ARDS. PLOS ONE 2020, 15, e0236312. [Google Scholar] [CrossRef]
- Mongodi, S.; Orlando, A.; Arisi, E.; Tavazzi, G.; Santangelo, E.; Caneva, L.; Pozzi, M.; Pariani, E.; Bettini, G.; Maggio, G.; et al. Lung Ultrasound in Patients with Acute Respiratory Failure Reduces Conventional Imaging and Health Care Provider Exposure to COVID-19. Ultrasound Med. Biol. 2020, 46, 2090–2093. [Google Scholar] [CrossRef]
- Brahier, T.; Meuwly, J.-Y.; Pantet, O.; Vez, M.-J.B.; Donnet, H.G.; Hartley, M.-A.; Hugli, O.; Boillat-Blanco, N. Lung ultrasonography for risk stratification in patients with COVID-19: A prospective observational cohort study. Clin. Infect. Dis. 2020, 17, 1408. [Google Scholar] [CrossRef] [PubMed]
- Pacileo, M.; Giallauria, F.; Savarese, C.; Cirillo, T.; Crescibene, F.; Di Lorenzo, A.; Ferrillo, M.; Calabrese, M.G.; Vigorito, C.; D’Andrea, A. The role of echocardiography in SARS-CoV-2 pandemic: A compromise among appropriateness, safety and clinical impact. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef] [PubMed]
- Tung-Chen, Y.; de Gracia, M.M.; Díez-Tascón, A.; Alonso-González, R.; Agudo-Fernández, S.; Parra-Gordo, M.L.; Ossaba-Vélez, S.; Rodríguez-Fuertes, P.; Llamas-Fuentes, R. Correlation between Chest Computed Tomography and Lung Ultrasonography in Patients with Coronavirus Disease 2019 (COVID-19). Ultrasound Med. Biol. 2020, 46, 2918–2926. [Google Scholar] [CrossRef] [PubMed]
- Tsai, N.W.; Ngai, C.W.; Mok, K.L.; Tsung, J.W. Lung ultrasound imaging in avian influenza A (H7N9) respiratory failure. Crit. Ultrasound J. 2014, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperandeo, M.; Rotondo, A.; Guglielmi, G.; Catalano, D.; Feragalli, B.; Trovato, G.M. Transthoracic ultrasound in the as-sessment of pleural and pulmonary diseases: Use and limitations. Radiol. Med. 2014, 119, 729–740. [Google Scholar] [CrossRef]
- Sperandeo, M.; Varriale, A.; Bianco, M.; Piattelli, M.; Bizzarri, M.; Ghittoni, G.; Copetti, M.; Vendemiale, G.; Sperandeo, G. Characterization of the normal pulmonary surface and pneumonectomy space by reflected ultrasound. J. Ultrasound 2011, 14, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.R.; Burns, P.N.; Wilkinson, L.M.; Simpson, D.H.; Muradali, D. Gas at Abdominal US: Appearance, Relevance, and Analysis of Artifacts. Radiology 1999, 210, 113–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogra, V.; Rubens, D.J. Ultrasound Secrets; Hanley & Belfus: Philadelphia, PA, USA, 2004; pp. 8–13. [Google Scholar]
- Sperandeo, M.; Trovato, G. Lung Ultrasound in COVID-19 Patients – More Shadows Than Information – Letter to the Editor on the Article “W. LU et al. Ultraschall in Med. 2020 Apr 15.”. Ultraschall Der Med.-Eur. J. Ultrasound 2020, 41, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Trovato, G.M.; Sperandeo, M. Usefulness of lung ultrasound imaging in COVID-19 pneumonia: The persisting need of safety and evidences. Echocardiography 2020, 37, 1138–1139. [Google Scholar] [CrossRef]
- Sperandeo, M.; Quarato, C.M.I.; Rea, G. Diagnosis of coronavirus disease 2019 pneumonia in pregnant women: Can we rely on lung ultrasound? Am. J. Obstet. Gynecol. 2020, 223, 615. [Google Scholar] [CrossRef]
- Tinti, M.G.; Rea, G.; Frongillo, E.; Saponara, A.; Sperandeo, M. The pathologic patterns detectable by transthoracic ultraso-nography are only the pleural and subpleural ones and are not specific: Why compare them with high-resolution computed tomography? J. Ultrasound Med. 2018, 37, 1847–1848. [Google Scholar] [CrossRef] [PubMed]
- Sperandeo, M.; Carnevale, V.; Varriale, A. Response to Pleuro-Pulmonary US Examination Artifacts: “Error in Images”. Ultrasound Med. Biol. 2010, 36, 357. [Google Scholar] [CrossRef]
- Quarato, C.M.I.; Venuti, M.; Sperandeo, M. Diagnosis of Coronavirus Disease (COVID-19) Pneumonia: Is Lung Ultrasound the Better Choice? Am. J. Roentgenol. 2021, 216, W5. [Google Scholar] [CrossRef]
- Quarato, C.M.I.; Venuti, M.; Lacedonia, D.; Simeone, A.; Dimitri, L.M.C.; Rea, G.; Ferragalli, B.; Sperandeo, M. The Role of Transthoracic Ultrasound in the novel Coronavirus Disease (COVID-19): A Reappraisal. Information and Disinformation: Is There Still Place for a Scientific Debate? Front. Med. 2020, 7, 271. [Google Scholar] [CrossRef] [PubMed]
- Sperandeo, M.; Rea, G. Interstitial Lung Diseases. In Thoracic Ultrasound and Integrated Imaging; Feletti, F., Malta, B., Aliverti, A., Eds.; Springer International Publishing: Berlin, Germany, 2020; pp. 61–82. [Google Scholar] [CrossRef]
- Zhang, Y.-K.; Li, J.; Yang, J.-P.; Zhan, Y.; Chen, J. Lung ultrasonography for the diagnosis of 11 patients with acute respiratory distress syndrome due to bird flu H7N9 infection. Virol. J. 2015, 12, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Quarato, C.M.I.; Venuti, M.; Sperandeo, M. The artificial count of artifacts for thoracic ultrasound: What is the clinical usefulness? J. Clin. Monit. 2020, 34, 1379–1381. [Google Scholar] [CrossRef] [PubMed]
- Abramowicz, J.; Basseal, J. World Federation for Ultrasound in Medicine and Biology Position Statement: How to Perform a Safe Ultrasound Examination and Clean Equipment in the Context of COVID-19. Ultrasound Med. Biol. 2020, 46, 1821–1826. [Google Scholar] [CrossRef]
- Lichtenstein, D.A. BLUE-Protocol and FALLS-Protocol. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Q.; Zhang, Y.; Wang, H.; Chen, L.; Yang, Z.; Peng, Z.; Liu, Y.; Feng, C.; Huang, X.; Jiang, N.; et al. Semiquantitative lung ultrasound scores in the evaluation and follow-up of critically ill patients with COVID-19: A single-center study. Acad. Radiol. 2020, 27, 1363–1372. [Google Scholar] [CrossRef] [PubMed]
- Manivel, V.; Lesnewski, A.; Shamim, S.; Carbonatto, G.; Govindan, T. CLUE: COVID-19 lung ultrasound in emergency department. Emerg. Med. Australas. 2020, 32, 694–696. [Google Scholar] [CrossRef]
- Ottaviani, S.; Franc, M.; Ebstein, E.; DeMaria, L.; Lheure, C.; Debray, M.; Khalil, A.; Crestani, B.; Borie, R.; Dieudé, P. Lung ultrasonography in patients with COVID-19: Comparison with CT. Clin. Radiol. 2020, 75, 877.e1–877.e6. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.; Cao, C.; Gao, Y.; Zhang, W.; Xie, Y.; Duan, Y.; Kong, S.; You, M.; Ma, R.; Jiang, L.; et al. Prognostic value of bedside lung ultrasound score in patients with COVID-19. Crit. Care 2020, 24, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cox, E.G.M.; SICS Study Group; Wiersema, R.; Wong, A.; Van Der Horst, I.C.C. Six versus eight and twenty-eight scan sites for B-line assessment: Differences in examination time and findings. Intensiv. Care Med. 2020, 46, 1063–1064. [Google Scholar] [CrossRef]
- Zieleskiewicz, L.; Markarian, T.; Lopez, A.; Taguet, C.; Mohammedi, N.; Boucekine, M.; Baumstarck, K.; Besch, G.; Mathon, G.; Duclos, G.; et al. Comparative study of lung ultrasound and chest computed tomography scan in the assessment of severity of confirmed COVID-19 pneumonia. Intensiv. Care Med. 2020, 46, 1707–1713. [Google Scholar] [CrossRef]
- Chiumello, D.; Mongodi, S.; Algieri, I.; Vergani, G.L.; Orlando, A.; Via, G.; Crimella, F.; Cressoni, M.; Mojoli, F. Assessment of lung aeration and recruitment by CT scan and ultrasound in acute respiratory distress syndrome patients. Crit. Care Med. 2018, 46, 1761–1768. [Google Scholar] [CrossRef] [Green Version]
- Buessler, A.; Chouihed, T.; Duarte, K.; Bassand, A.; Huot-Marchand, M.; Gottwalles, Y.; Pénine, A.; André, E.; Nace, L.; Jaeger, D.; et al. Accuracy of Several Lung Ultrasound Methods for the Diagnosis of Acute Heart Failure in the ED. Chest 2020, 157, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichter, Y.; Topilsky, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, A.G.; Vine, J.; Goren, O.; Cohen, B.; et al. Lung ultrasound predicts clinical course and outcomes in COVID-19 patients. Intensiv. Care Med. 2020, 46, 1873–1883. [Google Scholar] [CrossRef]
- Zotzmann, V.; Lang, C.N.; Wengenmayer, T.; Bemtgen, X.; Schmid, B.; Mueller-Peltzer, K.; Supady, A.; Bode, C.; Duerschmied, D.; Staudacher, D.L. Combining lung ultrasound and Wells score for diagnosing pulmonary embolism in critically ill COVID-19 patients. J. Thromb. Thrombolysis 2020, 3, 1–9. [Google Scholar] [CrossRef]
- Peschel, G.; Jung, E.; Fisser, C.; Putz, F.; Wertheimer, T.; Sinner, B.; Lunz, D.; Jung, F.; Müller, M. Interstitial lung opacities in patients with severe COVID-19 pneumonia by bedside high-resolution ultrasound in association to CO2 retention. Clin. Hemorheol. Microcirc. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Herpe, G.; Lederlin, M.; Naudin, M.; Ohana, M.; Chaumoitre, K.; Gregory, J.; Vilgrain, V.; Freitag, C.A.; De Margerie-Mellon, C.; Flory, V.; et al. Efficacy of Chest CT for COVID-19 Pneumonia Diagnosis in France. Radiology 2021, 298, E81–E87. [Google Scholar] [CrossRef] [PubMed]
- Hermans, J.J.; Groen, J.; Zwets, E.; Boxma-De Klerk, B.M.; Van Werkhoven, J.M.; Ong, D.S.; Hanselaar, W.E.; Waals-Prinzen, L.; Brown, V. Chest CT for triage during COVID-19 on the emergency department: Myth or truth? Emerg. Radiology 2020, 27, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, A.; Scotti, G.M.; Ippolito, D.; Morelli, M.J.; Vignale, D.; Gandola, D.; Sironi, S.; De Cobelli, F.; Ferrante, L.; Spessot, M.; et al. Chest CT in the emergency department for suspected COVID-19 pneumonia. Radiol. Med. 2020, 9, 1–5. [Google Scholar] [CrossRef]
- Skalidis, I.; Nguyen, V.K.; Bothorel, H.; Poli, L.; Da Costa, R.R.; Younossian, A.B.; Petriccioli, N.; Kherad, O. Unenhanced computed tomography (CT) utility for triage at the emergency department during COVID-19 pandemic. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brun, A.L.; Gence-Breney, A.; Trichereau, J.; Ballester, M.C.; Vasse, M.; Chabi, M.L.; Mellot, F.; Grenier, P.A. COVID-19 pneumonia: High diagnostic accuracy of chest CT in patients with intermediate clinical probability. Eur. Radiol. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Falaschi, Z.; Danna, P.S.; Arioli, R.; Pasché, A.; Zagaria, D.; Percivale, I.; Tricca, S.; Barini, M.; Aquilini, F.; Andreoni, S.; et al. Chest CT accuracy in diagnosing COVID-19 during the peak of the Italian epidemic: A retrospective correlation with RT-PCR testing and analysis of discordant cases. Eur. J. Radiol. 2020, 130, 109192. [Google Scholar] [CrossRef]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; De Dominicis, C.; Laghi, A. Chest CT Features of COVID-19 in Rome, Italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef]
- Kim, H.; Hong, H.; Yoon, S.H. Diagnostic Performance of CT and Reverse Transcriptase Polymerase Chain Reaction for Coronavirus Disease 2019: A Meta-Analysis. Radiology 2020, 296, E145–E155. [Google Scholar] [CrossRef] [PubMed]
- Borakati, A.; Perera, A.; Johnson, J.; Sood, T. Diagnostic accuracy of X-ray versus CT in COVID-19: A propensity-matched database study. BMJ Open 2020, 10, e042946. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Long, C.; Xu, H.; Shen, Q.; Zhang, X.; Fan, B.; Wang, C.; Zeng, B.; Li, Z.; Li, X.; Li, H. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur. J. Radiol. 2020, 126, 108961. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for Typical Coronavirus Disease 2019 (COVID-19) Pneumonia: Relationship to Negative RT-PCR Testing. Radiology 2020, 296, E41–E45. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Jiang, X.; Hong, Y.; Wen, Z.; Wei, S.; Peng, G.; Wei, X. Can Chest CT Features Distinguish Patients With Negative From Those With Positive Initial RT-PCR Results for Coronavirus Disease (COVID-19)? Am. J. Roentgenol. 2021, 216, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Luo, F.; Xie, L.; Gao, Y.; Zhang, N.; Wu, B. Chest CT study of fifteen COVID-19 patients with positive RT-PCR retest results after discharge. Quant. Imaging Med. Surg. 2020, 10, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Guillo, E.; Gomez, I.B.; Dangeard, S.; Bennani, S.; Saab, I.; Tordjman, M.; Jilet, L.; Chassagnon, G.; Revel, M.-P. COVID-19 pneumonia: Diagnostic and prognostic role of CT based on a retrospective analysis of 214 consecutive patients from Paris, France. Eur. J. Radiol. 2020, 131, 109209. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Kovács, A.; Palásti, P.; Veréb, D.; Bozsik, B.; Palkó, A.; Kincses, Z.T. The sensitivity and specificity of chest CT in the diagnosis of COVID-19. Eur. Radiol. 2020, 13, 1–6. [Google Scholar] [CrossRef]
- Chen, L.-D.; Li, H.; Ye, Y.-M.; Wu, Z.; Huang, Y.-P.; Zhang, W.-L.; Lin, L. A COVID-19 patient with multiple negative results for PCR assays outside Wuhan, China: A case report. BMC Infect. Dis. 2020, 20, 1–4. [Google Scholar] [CrossRef]
- Meng, H.; Xiong, R.; He, R.; Lin, W.; Hao, B.; Zhang, L.; Lu, Z.; Shen, X.; Fan, T.; Jiang, W.; et al. CT imaging and clinical course of asymptomatic cases with COVID-19 pneumonia at admission in Wuhan, China. J. Infect. 2020, 81, e33–e39. [Google Scholar] [CrossRef]
- Uchida, S.; Uno, S.; Uwamino, Y.; Hashimoto, M.; Matsumoto, S.; Obara, H.; Jinzaki, M.; Kitagawa, Y.; Hasegawa, N. CT screening for COVID-19 in asymptomatic patients before hospital admission. J. Infect. Chemother. 2021, 27, 232–236. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, W.; Pan, F.; Li, L.; Yang, L.; Zheng, D.; Wang, J.; Liang, B. The pulmonary sequalae in discharged patients with COVID-19: A short-term observational study. Respir. Res. 2020, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.-M.; Shang, Y.-M.; Song, W.-B.; Li, Q.-Q.; Xie, H.; Xu, Q.-F.; Jia, J.-L.; Li, L.-M.; Mao, H.-L.; Zhou, X.-M.; et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClin. Med. 2020, 25, 100463. [Google Scholar] [CrossRef]
- Urciuoli, L.; Guerriero, E. Chest CT Findings after 4 Months from the Onset of COVID-19 Pneumonia: A Case Series. Diagnostics 2020, 10, 899. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Tang, N.; Chen, Y.; Ma, L.; Wei, Y.; Lu, Y.; Ye, K.; Liu, H.; Tang, F.; Huang, G.; et al. CT features of COVID-19 patients with two consecutive negative RT-PCR tests after treatment. Sci. Rep. 2020, 10, 11548. [Google Scholar] [CrossRef]
- Dai, W.-C.; Zhang, H.-W.; Yu, J.; Xu, H.-J.; Chen, H.; Luo, S.-P.; Zhang, H.; Liang, L.-H.; Wu, X.-L.; Lei, Y.; et al. CT Imaging and Differential Diagnosis of COVID-19. Can. Assoc. Radiol. J. 2020, 71, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.-B.; Wang, D.-C.; Mei, J.; et al. Performance of Radiologists in Differentiating COVID-19 from Non-COVID-19 Viral Pneumonia at Chest CT. Radiology 2020, 296, 200823. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zeng, W.; Wen, Y.; Zheng, Y.; Lv, F.; Xiao, K. COVID-19 pneumonia: CT findings of 122 patients and differentiation from influenza pneumonia. Eur. Radiol. 2020, 30, 1–7. [Google Scholar] [CrossRef]
- Homayounieh, F.; Babaei, R.; Mobin, H.K.; Arru, C.D.; Sharifian, M.; Mohseni, I.; Zhang, E.; Digumarthy, S.R.; Kalra, M.K. Computed Tomography Radiomics Can Predict Disease Severity and Outcome in Coronavirus Disease 2019 Pneumonia. J. Comput. Assist. Tomogr. 2020, 44, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Kalra, M.K.; Homayounieh, F.; Arru, C.; Holmberg, O.; Vassileva, J. Chest CT practice and protocols for COVID-19 from radiation dose management perspective. Eur. Radiol. 2020, 30, 6554–6560. [Google Scholar] [CrossRef] [PubMed]
- Radpour, A.; Bahrami-Motlagh, H.; Taaghi, M.T.; Sedaghat, A.; Karimi, M.A.; Hekmatnia, A.; Haghighatkhah, H.-R.; Sanei-Taheri, M.; Arab-Ahmadi, M.; Azhideh, A. COVID-19 Evaluation by Low-Dose High Resolution CT Scans Protocol. Acad. Radiol. 2020, 27, 901. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei, S.M.H.; Talari, H.; Gholamrezanezhad, A.; Farhood, B.; Rahimi, H.; Razzaghi, R.; Mehri, N.; Rajebi, H. A low-dose chest CT protocol for the diagnosis of COVID-19 pneumonia: A prospective study. Emerg. Radiol. 2020, 27, 607–615. [Google Scholar] [CrossRef]
- Kang, Z.; Li, X.; Zhou, S. Recommendation of low-dose CT in the detection and management of COVID-2019. Eur. Radiol. 2020, 30, 4356–4357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiri, I.; Akhavanallaf, A.; Sanaat, A.; Salimi, Y.; Askari, D.; Mansouri, Z.; Shayesteh, S.P.; Hasanian, M.; Rezaei-Kalantari, K.; Salahshour, A.; et al. Ultra-low-dose chest CT imaging of COVID-19 patients using a deep residual neural network. Eur. Radiol. 2021, 31, 1420–1431. [Google Scholar] [CrossRef] [PubMed]
- Léonard-Lorant, I.; Delabranche, X.; Séverac, F.; Helms, J.; Pauzet, C.; Collange, O.; Schneider, F.; Labani, A.; Bilbault, P.; Molière, S.; et al. Acute Pulmonary Embolism in Patients with COVID-19 at CT Angiography and Relationship to d-Dimer Levels. Radiology 2020, 296, E189–E191. [Google Scholar] [CrossRef] [Green Version]
- Lang, M.; Som, A.; Carey, D.; Reid, N.; Mendoza, D.P.; Flores, E.J.; Li, M.D.; Shepard, J.-A.O.; Little, B.P. Pulmonary Vascular Manifestations of COVID-19 Pneumonia. Radiol. Cardiothorac. Imaging 2020, 2, e200277. [Google Scholar] [CrossRef]
- Minnesota Department of Health. Infection Control Precautions. Available online: http://www.health.state.mn.us/index.html (accessed on 18 November 2020).
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [Green Version]
- Garg, M.; Gupta, P.; Maralakunte, M.; Kumar-M, P.; Sinha, A.; Kang, M.; Agarwal, R.; Sandhu, M.S. Diagnostic accuracy of CT and radiographic findings for novel coronavirus 2019 pneumonia: Systematic review and meta-analysis. Clin. Imaging 2021, 72, 75–82. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, F.; Lou, J.; Xi, D.; Bai, Y.; Ma, G.; Zhao, B.; Liu, D.; Bao, G.; Lei, Z.; Wang, M. Chest computed tomography findings of coronavirus disease 2019 (COVID-19) pneumonia. Eur. Radiol. 2020, 30, 5489–5498. [Google Scholar] [CrossRef]
- Ojha, V.; Mani, A.; Pandey, N.N.; Sharma, S.; Kumar, S. CT in coronavirus disease 2019 (COVID-19): A systematic review of chest CT findings in 4410 adult patients. Eur. Radiol. 2020, 30, 6129–6138. [Google Scholar] [CrossRef]
- Zhou, S.; Zhu, T.; Wang, Y.; Xia, L. Imaging features and evolution on CT in 100 COVID-19 pneumonia patients in Wuhan, China. Eur. Radiol. 2020, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA - Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.I.S.; Müller, N.L. Chest CT target sign in a couple with COVID-19 pneumonia. Radiol. Bras. 2020, 53, 252–254. [Google Scholar] [CrossRef]
- Wang, Y.; Jin, C.; Wu, C.C.; Zhao, H.; Liang, T.; Liu, Z.; Jian, Z.; Li, R.; Wang, Z.; Li, F.; et al. Organizing pneumonia of COVID-19: Time-dependent evolution and outcome in CT findings. PLOS ONE 2020, 15, e0240347. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Prokop, M.; Van Everdingen, W.; van Rees Vellinga, T.; Quarles van Ufford, H.; Stöger, L.; Beenen, L.; Geurts, B.; Gietema, H.; Krdzalic, J.; Schaefer-Prokop, C.; et al. CO-RADS: A Categorical CT Assessment Scheme for Patients Suspected of Having COVID-19—Definition and Evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [Green Version]
- Lv, H.; Chen, T.; Pan, Y.; Wang, H.; Chen, L.; Lu, Y. Pulmonary vascular enlargement on thoracic CT for diagnosis and differential diagnosis of COVID-19: A systematic review and meta-analysis. Ann. Transl. Med. 2020, 8, 878. [Google Scholar] [CrossRef]
- Borczuk, A.C.; Salvatore, S.P.; Seshan, S.V.; Patel, S.S.; Bussel, J.B.; Mostyka, M.; Elsoukkary, S.; He, B.; Del Vecchio, C.; Fortarezza, F.; et al. COVID-19 pulmonary pathology: A multi-institutional autopsy cohort from Italy and New York City. Mod. Pathol. 2020, 33, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Liu, Y.; Xu, D.; Zhang, R.; Lan, L.; Xu, H. Prediction of the Development of Pulmonary Fibrosis Using Serial Thin-Section CT and Clinical Features in Patients Discharged after Treatment for COVID-19 Pneumonia. Korean J. Radiol. 2020, 21, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Han, X.; Gu, J.; Li, Y.; Liu, J.; Alwalid, O.; Cui, Y.; Zhang, X.; Zheng, C.; Fan, Y.; et al. Prognostic value of baseline clinical and HRCT findings in 101 patients with severe COVID-19 in Wuhan, China. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef]
- Feng, Z.; Yu, Q.; Yao, S.; Luo, L.; Zhou, W.; Mao, X.; Li, J.; Duan, J.; Yan, Z.; Yang, M.; et al. Early prediction of disease progression in COVID-19 pneumonia patients with chest CT and clinical characteristics. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei, S.M.H.; Rahimi, H.; Moghaddas, F.; Rajebi, H. Predictive value of CT in the short-term mortality of Coronavirus Disease 2019 (COVID-19) pneumonia in nonelderly patients: A case-control study. Eur. J. Radiol. 2020, 132, 109298. [Google Scholar] [CrossRef]
- Wang, X.; Hu, X.; Tan, W.; Mazzone, P.; Mireles-Cabodevila, E.; Han, X.-Z.; Huang, P.; Hu, W.; Dweik, R.; Cheng, Z. Multi-Center Study of Temporal Changes and Prognostic Value of a CT Visual Severity Score in Hospitalized Patients with COVID-19. Am. J. Roentgenol. 2020. [Google Scholar] [CrossRef]
- Khosravi, B.; Aghaghazvini, L.; Sorouri, M.; Atashi, S.N.; Abdollahi, M.; Mojtabavi, H.; Khodabakhshi, M.; Motamedi, F.; Azizi, F.; Rajabi, Z.; et al. Predictive value of initial CT scan for various adverse outcomes in patients with COVID-19 pneumonia. Hear. Lung 2021, 50, 13–20. [Google Scholar] [CrossRef]
- Li, S.; Liu, S.; Wang, B.; Li, Q.; Zhang, H.; Zeng, L.; Ge, H.; Ma, Q.; Shen, N. Predictive value of chest CT scoring in COVID-19 patients in Wuhan, China: A retrospective cohort study. Respir. Med. 2021, 176, 106271. [Google Scholar] [CrossRef]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, E86–E96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, J.; Li, H.; Yu, H.; Liu, X.; Zeng, X.; Peng, D.; Zhang, W. 2019 novel coronavirus (COVID-19) pneumonia: CT manifestations and pattern of evolution in 110 patients in Jiangxi, China. Eur. Radiol. 2021, 31, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, R.; Li, X.; Liu, H.; Zhen, Y.; Zhang, X.; Xiong, Q.; Luo, Y.; Gao, C.; Zeng, W. Chest CT Severity Score: An Imaging Tool for Assessing Severe COVID-19. Radiol. Cardiothorac. Imaging 2020, 2, e200047. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; He, G.; Yang, X.; Chen, J.; Wu, J.; Ma, M.; Lu, W.; Li, Q.; Cheng, T.; Huang, X. Dynamic changes of Chest CT follow-up in Coronavirus Disease-19 (COVID-19) pneumonia: Relationship to clinical typing. BMC Med. Imaging 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhan, C.; Chen, C.; Ai, T.; Xia, L. Chest CT findings related to mortality of patients with COVID-19: A retrospective case-series study. PLOS ONE 2020, 15, e0237302. [Google Scholar] [CrossRef]
- Abbasi, B.; Akhavan, R.; Khameneh, A.G.; Zandi, B.; Farrokh, D.; Rad, M.P.; Laein, A.F.; Darvish, A.; Bijan, B. Evaluation of the relationship between inpatient COVID-19 mortality and chest CT severity score. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Caruso, D.; Polici, M.; Zerunian, M.; Pucciarelli, F.; Polidori, T.; Guido, G.; Rucci, C.; Bracci, B.; Muscogiuri, E.; De Dominicis, C.; et al. Quantitative Chest CT analysis in discriminating COVID-19 from non-COVID-19 patients. La Radiologia Medica 2021, 126, 243–249. [Google Scholar] [CrossRef]
- Gieraerts, C.; Dangis, A.; Janssen, L.; Demeyere, A.; De Bruecker, Y.; De Brucker, N.; Bergh, A.V.D.; Lauwerier, T.; Heremans, A.; Frans, E.; et al. Prognostic Value and Reproducibility of AI-assisted Analysis of Lung Involvement in COVID-19 on Low-Dose Submillisievert Chest CT: Sample Size Implications for Clinical Trials. Radiol. Cardiothorac. Imaging 2020, 2, e200441. [Google Scholar] [CrossRef]
- Henkel, M.; Weikert, T.; Marston, K.; Schwab, N.; Sommer, G.; Haslbauer, J.; Franzeck, F.; Anastasopoulos, C.; Stieltjes, B.; Michel, A.; et al. Lethal COVID-19: Radiologic-Pathologic Correlation of the Lungs. Radiol. Cardiothorac. Imaging 2020, 2, e200406. [Google Scholar] [CrossRef]
- Recalde-Zamacona, B.; García-Tobar, L.; Argueta, A.; Álvarez, L.; De Andrea, C.E.; Alonso, M.F.; Ezponda, A.; Torre, F.C.; Iborra, C.J.; Quiroga, J.A.; et al. Histopathological findings in fatal COVID-19 severe acute respiratory syndrome: Preliminary experience from a series of 10 Spanish patients. Thorax 2020, 75, 1116–1118. [Google Scholar] [CrossRef]
- Suess, C.; Hausmann, R. Gross and histopathological pulmonary findings in a COVID-19 associated death during self-isolation. Int. J. Leg. Med. 2020, 134, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Ducloyer, M.; Gaborit, B.; Toquet, C.; Castain, L.; Bal, A.; Arrigoni, P.P.; LeComte, R.; Clement, R.; Sagan, C. Complete post-mortem data in a fatal case of COVID-19: clinIcal, radiological and pathological correlations. Int. J. Leg. Med. 2020, 134, 2209–2214. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in suspected COVID-19 cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, R.A.A.; BIAS—Brazilian Image Autopsy Study Group; De Oliveira, E.P.; Saldiva, P.H.N.; Dolhnikoff, M.; Duarte-Neto, A.N. Histological–ultrasonographical correlation of pulmonary involvement in severe COVID-19. Intensiv. Care Med. 2020, 46, 1766–1768. [Google Scholar] [CrossRef]
- Sauter, J.L.; Baine, M.K.; Butnor, K.J.; Buonocore, D.J.; Chang, J.C.; Jungbluth, A.A.; Szabolcs, M.J.; Morjaria, S.; Mount, S.L.; Rekhtman, N.; et al. Insights into pathogenesis of fatal COVID-19 pneumonia from histopathology with immunohistochemical and viral RNA studies. Histopathology 2020, 77, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID -19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre- COVID -19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brogna, B.; Brogna, C.; Martino, A.; Minichiello, S.; Romeo, D.M.; Romano, P.; Bignardi, E.; Mazza, E.M.; Musto, L. SARS-CoV-2 Infection with Different Radiological Insights. Diagnostics 2020, 10, 283. [Google Scholar] [CrossRef]
- Wilson, J.G.; Simpson, L.J.; Ferreira, A.-M.; Rustagi, A.; Roque, J.; Asuni, A.; Ranganath, T.; Grant, P.M.; Subramanian, A.; Rosenberg-Hasson, Y.; et al. Cytokine profile in plasma of severe COVID-19 does not differ from ARDS and sepsis. JCI Insight 2020, 5, 140289. [Google Scholar] [CrossRef]
- Ragab, D.; Eldin, H.S.; Taeimah, M.; Khattab, R.; Salem, R. The COVID-19 Cytokine Storm; What We Know So Far. Front. Immunol. 2020, 11, 1446. [Google Scholar] [CrossRef]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef]
- Kaur, S.; Tripathi, D.M.; Yadav, A. The Enigma of Endothelium in COVID-19. Front. Physiol. 2020, 11, 989. [Google Scholar] [CrossRef]
- Archer, S.L.; Sharp, W.W.; Weir, E.K. Differentiating COVID-19 Pneumonia from Acute Respiratory Distress Syndrome and High Altitude Pulmonary Edema. Circulation 2020, 142, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Busana, M.; Coppola, S.; Romitti, F.; Formenti, P.; Bonifazi, M.; Pozzi, T.; Palumbo, M.M.; Cressoni, M.; Herrmann, P.; et al. Physiological and quantitative CT-scan characterization of COVID-19 and typical ARDS: A matched cohort study. Intensiv. Care Med. 2020, 46, 2187–2196. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respira-tory treatments for different phenotypes? Intens. Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Rambaldi, A.; Gritti, G.; Micò, M.C.; Frigeni, M.; Borleri, G.; Salvi, A.; Landi, F.; Pavoni, C.; Sonzogni, A.; Gianatti, A.; et al. Endothelial injury and thrombotic microangiopathy in COVID-19: Treatment with the lectin-pathway inhibitor narsoplimab. Immunobiology 2020, 225, 152001. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Ooi, M.; Rajai, A.; Patel, R.; Gerova, N.; Godhamgaonkar, V.; Liong, S. Pulmonary thromboembolic disease in COVID-19 patients on CT pulmonary angiography—Prevalence, pattern of disease and relationship to D-dimer. Eur. J. Radiol. 2020, 132, 109336. [Google Scholar] [CrossRef]
- Spagnolo, P.; Cozzi, A.; Foà, R.A.; Spinazzola, A.; Monfardini, L.; Bnà, C.; Alì, M.; Schiaffino, S.; Sardanelli, F. CT-derived pulmonary vascular metrics and clinical outcome in COVID-19 patients. Quant. Imaging Med. Surg. 2020, 10, 1325–1333. [Google Scholar] [CrossRef]
- McGuinness, G.; Zhan, C.; Rosenberg, N.; Azour, L.; Wickstrom, M.; Mason, D.M.; Thomas, K.M.; Moore, W.H. Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation. Radiology 2020, 297, E252–E262. [Google Scholar] [CrossRef]
- Udi, J.; Lang, C.N.; Zotzmann, V.; Krueger, K.; Fluegler, A.; Bamberg, F.; Bode, C.; Duerschmied, D.; Wengenmayer, T.; Staudacher, D.L. Incidence of Barotrauma in Patients With COVID-19 Pneumonia During Prolonged Invasive Mechanical Ventilation—A Case-Control Study. J. Intensiv. Care Med. 2020, 22. [Google Scholar] [CrossRef]
- Zantah, M.; Castillo, E.D.; Townsend, R.; Dikengil, F.; Criner, G.J. Pneumothorax in COVID-19 disease- incidence and clinical characteristics. Respir. Res. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Volpi, S.; Ali, J.M.; Suleman, A.; Ahmed, R.N. Pneumomediastinum in COVID-19 patients: A case series of a rare complication. Eur. J. Cardio-Thoracic Surg. 2020, 58, 646–647. [Google Scholar] [CrossRef]
- Brogna, B.; Bignardi, E.; Salvatore, P.; Alberigo, M.; Brogna, C.; Megliola, A.; Fontanella, G.; Mazza, E.M.; Musto, L. Unusual presentations of COVID-19 pneumonia on CT scans with spontaneous pneumomediastinum and loculated pneumothorax: A report of two cases and a review of the literature. Heart Lung 2020, 49, 864–868. [Google Scholar] [CrossRef]
- Diaz, A.; Patel, D.; Sayedy, N.; Anjum, F. COVID-19 and Spontaneous Pneumomediastinum: A case series. Heart Lung 2021, 50, 202–205. [Google Scholar] [CrossRef]
- Zhou, C.; Gao, C.; Xie, Y.; Xu, M. COVID-19 with spontaneous pneumomediastinum. Lancet Infect. Dis. 2020, 20, 510. [Google Scholar] [CrossRef]
- Mallick, T.; Dinesh, A.; Engdahl, R.; Sabado, M. COVID-19 Complicated by Spontaneous Pneumothorax. Cureus 2020, 12, e9104. [Google Scholar] [CrossRef]
- Oye, M.; Ali, A.; Kandah, F.; Chowdhury, N. Two cases of spontaneous pneumomediastinum with pneumothorax in patients with COVID-19 associated pneumonia. Respir. Med. Case Rep. 2020, 31, 101308. [Google Scholar] [CrossRef]
- Manna, S.; Maron, S.Z.; Cedillo, M.A.; Voutsinas, N.; Toussie, D.; Finkelstein, M.; Steinberger, S.; Chung, M.; Bernheim, A.; Eber, C.; et al. Spontaneous subcutaneous emphysema and pneumomediastinum in non-intubated patients with COVID-19. Clin. Imaging 2020, 67, 207–213. [Google Scholar] [CrossRef]
- Letellier, A.; Gibelin, A.; Voiriot, G.; Fartoukh, M.; Djibré, M. Destructive pulmonary fibrosis after severe COVID-19 pneumonia. Int. J. Infect. Dis. 2020, 100, 377–378. [Google Scholar] [CrossRef]
- Amaral, L.T.W.; Beraldo, G.L.; Brito, V.M.; Rosa, M.E.E.; De Matos, M.J.R.; Fonseca, E.K.U.N.; Yokoo, P.; Silva, M.M.A.; Teles, G.B.D.S.; Shoji, H.; et al. Lung cavitation in COVID-19: Co-infection complication or rare evolution? Einstein 2020, 18, 5822. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiology Societies with Consensus Statements on Imaging Guidelines for COVID-19 | CXR | LUS | CT |
|---|---|---|---|
| American College of Radiology | Portable radiography units when CXR is considered medically necessary | No data | Only in symptomatic and hospitalized patients with specific clinical indications |
| British Society of Thoracic Imaging | Clinically stable patients with fever and respiratory symptoms if clinically required; for critically ill patients | Monitor critically ill patients | Seriously ill patients with uncertain or normal chest X-ray findings and if any complication is suspected during follow-up; if RT-PCR is not available |
| Canadian Association of Thoracic Radiology/Canadian Association of Radiologists | CXR may be useful in patients presenting with moderate to severe symptoms; in emergency department when RT-PCR assay is not available | No data | Low-dose CT only if results are expected to influence patient management or in high-risk individuals; CT pulmonary angiography in setting of suspected acute pulmonary embolism |
| Chinese Society of Radiologists | Follow-up for critically ill patients; lower sensitivity than CT for evaluation of early stage of pneumonia | Emergency and critical care setting | Chest CT is the most valuable imaging tool for clinical diagnosis of early-stage COVID-19 pneumonia when symptoms are nonspecific; chest CT can also evaluate time course and assess evolution of disease severity |
| European Society of Radiology and European Society of Thoracic Imaging | For ICU and in patients that are too fragile to be sent to CT | At bedside for pregnant women, children, ICU patients | In patients with respiratory symptoms such as dyspnea and desaturation; allows evaluation of disease extent at baseline, which may help predict poor outcome and need for ventilation |
| Fleischner Society | The choice of imaging modality is left to the judgement of clinical teams. CXR is usually preferred as the first imaging tool; however, it has lower sensitivity than CT. CXR is indicated in a resource-constrained environment where access to CT is limited. Daily chest radiographs are NOT indicated in stable intubated patients with COVID-19 | Not suggested for limited experience | Choice of imaging modality left to judgment of clinical team; CT usually indicated for patients with functional impairment and/or hypoxemia after recovery or for evaluation of complications |
| Italian Society of Medical and Interventional Radiology | First overview of the patients, especially in the emergency room; in hospitalized patients and in ICU | Critically ill patients | CT may be useful for monitoring lung involvement and managing suspected cases |
| Royal Australian and New Zealand College of Radiologists | In hospitalized patients | No data | In patients with chronic or acute disease |
| Royal College of Radiology | Critically ill patient | No data | In seriously ill patients |
| Structured Report Example |
|---|
| Technique: The examination was performed with unenhanced volumetric low-dose high-resolution (HRCT) technique with DLP: (mGy.cm) Indication: COVID-19 suspicion/initial assessment/follow-up Findings: Report parenchymal findings:
|
| Paper | Number of Patients | CT Severity Scores (CT-SS) in COVID-19 Pneumonia | Correlations of Higher CT-SS and CT Findings/Outcomes |
|---|---|---|---|
| Abbasi et al. [158] | 262 patients | Degree of involvement in each zone scored as follows:
| CT-SS can discriminate admitted patients with higher risk of in-hospital mortality with acceptable accuracy (area under the curve, 0.839). Mortality was significantly higher in patients with higher CT severity score even after adjustment for clinical, demographic, and laboratory parameters. |
| Khosravi et al. [150] | 121 patients | Patients with baseline CT-SS > 8 had 3-fold higher risk of poor outcome (ICU admission, intubation, mortality). | |
| Li et al. [151] | 53 patients | Higher CT-SS in severe/critical patients with higher GGO in second week, higher consolidation and crazy paving score in third week. Overall lung involvement score in second week appeared to have predictive value for whole-course clinical severity with optimal cut-off of 5.25 points. | |
| Chung et al. [154] | 21 patients | Each lung lobe scored using 0–4 Likert scale:
| Higher CT-SS for patients in ICU. |
| Hu et al. [157] | 73 patients | Moderate positive correlation between CT severity scores and inflammation-related factors of leucocytes, neutrophils, and IL-2R. CT-SS of lung involvement for patients who died from COVID-19 was significantly greater compared patients with mild to moderate disease. | |
| Li et al. [132] | 78 patients | Higher CT-SS (range of 8–18) in the severe critical type compared with the common type (range 1–11). | |
| Liu et al. [156] | 53 patients | In severe and critical group, GGO, fibrosis, and pleural thickening or adhesion could be found in every follow-up CT and were main signs in the two CTs. Right lung more involved in severe and critical group. | |
| Tabetabei et al. [148] | 30 patients | CT-SS ≥7.5 has highest sensitivity and specificity in ROC curve to predict mortality. | |
| Zhan et al. [153] | 110 patients | Higher CT-SS for patients with more prolonged disease course. | |
| Francone et al. [145] | 130 patients | Each lung lobe scored on a scale of 0 to 5:
| Death of patients with CT-SS ≥ 18. |
| Li et al. [159] | 83 patients | Severe/critical patients were older and had more underlying diseases than others. Decreased lymphocyte count in severe/critical patients. | |
| Pan et al. [109] | 21 patients | CT-SS correlated with disease stage. | |
| Guillo et al. [108] | 214 patients | Severity of COVID-19 pneumonia graded as minimal (<10% lung parenchyma), moderate (10–25%), intermediate (25–50%), severe (50–75%), critical (50–75%). | 68 % of patients with disease extent exceeding 25 % of the lung parenchyma were intubated or deceased in the 3 weeks following CT. |
| Yang et al. [155] | 102 patients | Considered 20 lung regions, assigning scores for parenchymal opacification of 0 (0% involvement of each region), 1 (<50% involvement), or 2 (>50% involvement) (CT-SS 0–40). | Higher CT-SS in patients with severe COVID-19 disease with CT-SS of 19.5 for identifying severe cases with a PPV of 75% and an NVP of 96.3%. |
| Wang et al. [149] | 161 patients | CT visual severity levels:
| Higher CT-SS were associated to the severity clinical course. Non-survivors showed much higher CT-SS compared with survivors, without a visually apparent decrease between week 1 and week 2. |
| COVID-19 Imaging Tools | General Indications | Advantages | Limitations |
|---|---|---|---|
| CXR | For symptomatic stable patients in ED; for patients in ED at moderate–high risk of progression, choice between CXR and CT based on judgment of clinical team, availability of local resources, and expertise of radiologists; in the ICU to evaluate complications (PMS, PX, ARDS) and chest tube positioning | Low cost, portable, lower dose burden than CT | Lower sensitivity than CT for evaluating COVID-19 pneumonia, especially in early phase; inadequate information on specificity |
| Chest CT | In ED in presence of high pretest probability for symptomatic patients with comorbidities or functional impairment and during FU for patients at moderate–high risk of progression; evaluation of fibrotic changes complications (barotrauma, SPM, SPX, ARDS, TE); CT can be indicated for symptomatic patients with multiple negative RT-PCR results; long-term FU | Easily available, rapid, high sensitivity in early phase of COVID-19 pneumonia, prognostic and predictive value in mortality through evaluation of pneumonia extension with CT-SS index; possible to visualize Macklin effect on CT; post-mortem evaluation | Low specificity, high dose burden, not used for screening asymptomatic patients or those with mild symptoms |
| LUS | For monitoring critically ill patients, especially in ICU | Low cost, portable, rapid, no radiation dose | Presence of air, low specificity, operator-dependent with intra- and inter-operator variability in B lines counted based on type and frequency of probe used and ultrasound machine setting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brogna, B.; Bignardi, E.; Brogna, C.; Volpe, M.; Lombardi, G.; Rosa, A.; Gagliardi, G.; Capasso, P.F.M.; Gravino, E.; Maio, F.; et al. A Pictorial Review of the Role of Imaging in the Detection, Management, Histopathological Correlations, and Complications of COVID-19 Pneumonia. Diagnostics 2021, 11, 437. https://doi.org/10.3390/diagnostics11030437
Brogna B, Bignardi E, Brogna C, Volpe M, Lombardi G, Rosa A, Gagliardi G, Capasso PFM, Gravino E, Maio F, et al. A Pictorial Review of the Role of Imaging in the Detection, Management, Histopathological Correlations, and Complications of COVID-19 Pneumonia. Diagnostics. 2021; 11(3):437. https://doi.org/10.3390/diagnostics11030437
Chicago/Turabian StyleBrogna, Barbara, Elio Bignardi, Claudia Brogna, Mena Volpe, Giulio Lombardi, Alessandro Rosa, Giuliano Gagliardi, Pietro Fabio Maurizio Capasso, Enzo Gravino, Francesca Maio, and et al. 2021. "A Pictorial Review of the Role of Imaging in the Detection, Management, Histopathological Correlations, and Complications of COVID-19 Pneumonia" Diagnostics 11, no. 3: 437. https://doi.org/10.3390/diagnostics11030437