 Juan Antonio García-Carmona1,2†‡
Juan Antonio García-Carmona1,2†‡ Enzo von Quednow3†
Enzo von Quednow3† Francisco Hernández-Fernández4,5*‡
Francisco Hernández-Fernández4,5*‡ Juan David Molina-Nuevo4,6Jorge García-García5María Palao5Tomás Segura5,7
Juan David Molina-Nuevo4,6Jorge García-García5María Palao5Tomás Segura5,7- 1Department of Neurology, Santa Lucia University Hospital, Cartagena, Spain
- 2Group of Clinical and Experimental Pharmacology, Institute for Biomedical Research of Murcia (IMIB), Murcia, Spain
- 3Department of Neurophysiology, General University Hospital, Albacete, Spain
- 4Unit of Interventional Neuroradiology, General University Hospital, Albacete, Spain
- 5Department of Neurology, General University Hospital, Albacete, Spain
- 6Department of Radiology, General University Hospital, Albacete, Spain
- 7Medical School, Institute for Research in Neurologic Disabilities (IDINE), University of Castilla-La-Mancha, Albacete, Spain
Background: Severe COVID-19 has been shown to produce convulsions, encephalitis, Guillain-Barré syndrome, or cerebrovascular disease. However, only 4 case reports described subarachnoid or brain hemorrhage caused by ruptured cerebral aneurysms or pseudoaneurysms in patients with COVID-19. Cerebral pseudoaneurysms represent <1% of all intracranial aneurysms and have been related to radiation therapy, vasculitis, rupture of true saccular aneurysms, arteriovenous malformations, and infections by bacteria and viruses, such as Epstein-Bar and Herpes virus.
Case presentation: A 28-year-old Caucasian woman, with no medical history of interest and completely vaccinated against SARS-CoV-2, was admitted to Neurology due to progressive tetraparesis with areflexia, a cough, and a fever of 38°C. SARS-CoV2 PCR was positive while lumbar puncture, blood tests, and electromyogram showed criteria for Guillain-Barré syndrome. Despite the treatment, the patient developed dyspnea and tetraplegia requiring invasive mechanical ventilation. There was motor neurological improvement but a decreased level of consciousness was observed on day 13. A brain CT scan demonstrated an acute haematoma and cerebral arteriography showed a 4-mm pseudoaneurysm located in a branch of the left middle cerebral artery. Given the high risk of rebleeding, endovascular treatment was decided upon. Therefore, complete embolization of the pseudoaneurysm was carried out by using the synthetic glue N-butyl-cyanocrylate. Two days later, the patient was clinically and neurologically recovered and was discharged. Lastly, a new angiography showed no evidence of the pseudoaneurysm 3-weeks later.
Conclusions: We report, for the first time, a patient suffering a severe immune reaction caused by SARS-CoV2 infection and developing a cerebral pseudoaneurysm treated with endovascular embolization without complications.
Introduction
The SARS-CoV-2 infection is well-known for causing common symptoms such as fever, cough, fatigue, pneumonia, and severe acute respiratory distress syndrome (SARS), leading to multi-organ failure and death. Furthermore, severe COVID-19 has been related to the impairment of the nervous system in hospitalized patients producing convulsions, encephalitis, and Guillain-Barré syndrome (1). Finally, haemostatic function represents a complex interaction between the coagulation and fibrinolytic systems, platelets, and the vascular wall (2). This haemostatic function is impaired by the SARS-CoV2 infection (3), causing cerebrovascular disease (1).
Cerebrovascular disease occurs in 1–2% of hospitalized patients suffering from COVID-19 and it has been extensively reported as ischemic stroke, while a few cases of brain hemorrhage have been reported (4). Three case reports published subarachnoid hemorrhage caused by ruptured cerebral aneurysms with COVID-19 (5) and another case was reported in an adolescent suffering an intracerebral haematoma due to cerebral distal pseudoaneurysm rupture (6).
Cerebral pseudoaneurysms represent <1% of all intracranial aneurysms (7) and their treatment and management is a challenge. Pseudoaneurysms are characterized by complete disruption of the artery wall, resulting in an extravascular hematoma contained by just a thin layer of connective tissue (8). Thus, these lesions have been shown to cause intracranial hemorrhage in up to 60% of patients and 31–54% mortality (7, 8). Several causes have been related to the formation of intracranial pseudoaneurysms including radiation therapy, vasculitis, rupture of true saccular aneurysms, arteriovenous malformations, and infections (8). Infectious pseudoaneurysms have a slight preference for younger people, most of them are located in the anterior circulation and often multiple (8). They are known to be caused by bacteria, mainly streptococcus and staphylococcus, fungi, tuberculosis, and by viruses, such as the Epstein-Bar and Herpes viruses (7, 8).
Here, we report a case of an adult Caucasian woman suffering from COVID-19 with progressive respiratory symptoms, who developed a Guillain-Barré syndrome and a brain hemorrhage caused by a pseudoaneurysm.
Case description
A 28-year-old Caucasian woman, with no medical history of interest and completely vaccinated against SARS-CoV-2 4 months ago, was admitted to Neurology due to a fever of 38°C and simultaneous progressive distal onset tetraparesis with areflexia. She also suffered mild respiratory symptoms, asthenia, and a cough from 1 week before (see Figure 1 for timeline scheme). No previous family history of autoimmune diseases, aneurysms, or stroke.
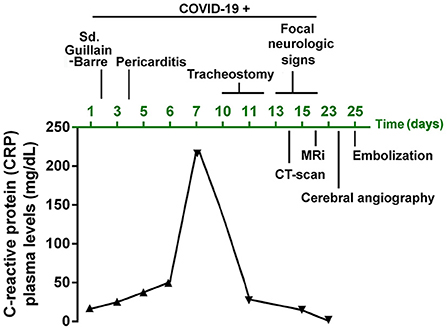
Figure 1. Timeline of the case report scheme summarizing the disease, complications and progression of the patient. Study follow-up of the C-reactive protein (CRP) plasma levels.
A chest X-ray showed bilateral pulmonary infiltrates and SARS-CoV2 PCR was positive. A lumbar puncture, blood tests, and an electromyogram (see Table 1 for details) were performed showing criteria for idiopathic acute demyelinating polyneuropathy or Guillain-Barré syndrome with positive IgG antiganglioside (GM1, aGM1, and GD1b) antibodies in relation to COVID-19 (day 2). Nonetheless, SARS-CoV2 subtype genotyping and PCR in cerebrospinal fluid (CSF) were not available. No other risk factors were identified underlying or related to Guillain-Barré syndrome (other viral or bacterial infections, recent surgery, hematological malignant diseases, or immune diseases such as lupus). Despite the patient being treated with immunoglobulins and corticosteroids she developed pericarditis on day 4 and progressed the polyneuropathy until she developed dyspnea and tetraplegia. No cranial nerve palsy was observed and neither was bowel or bladder dysfunction. Thus, she was transferred to the Intensive Care Unit (ICU), requiring invasive mechanical ventilation. As shown in Figure 1, neurological and respiratory worsening was in parallel with an increase in C-reactive protein (CRP) which peaked (>200 mg/dL) on day 7. As observed in a new chest X-ray, acute respiratory failure was probably secondary to a mucus plug causing airway obstruction and left lung atelectasis.
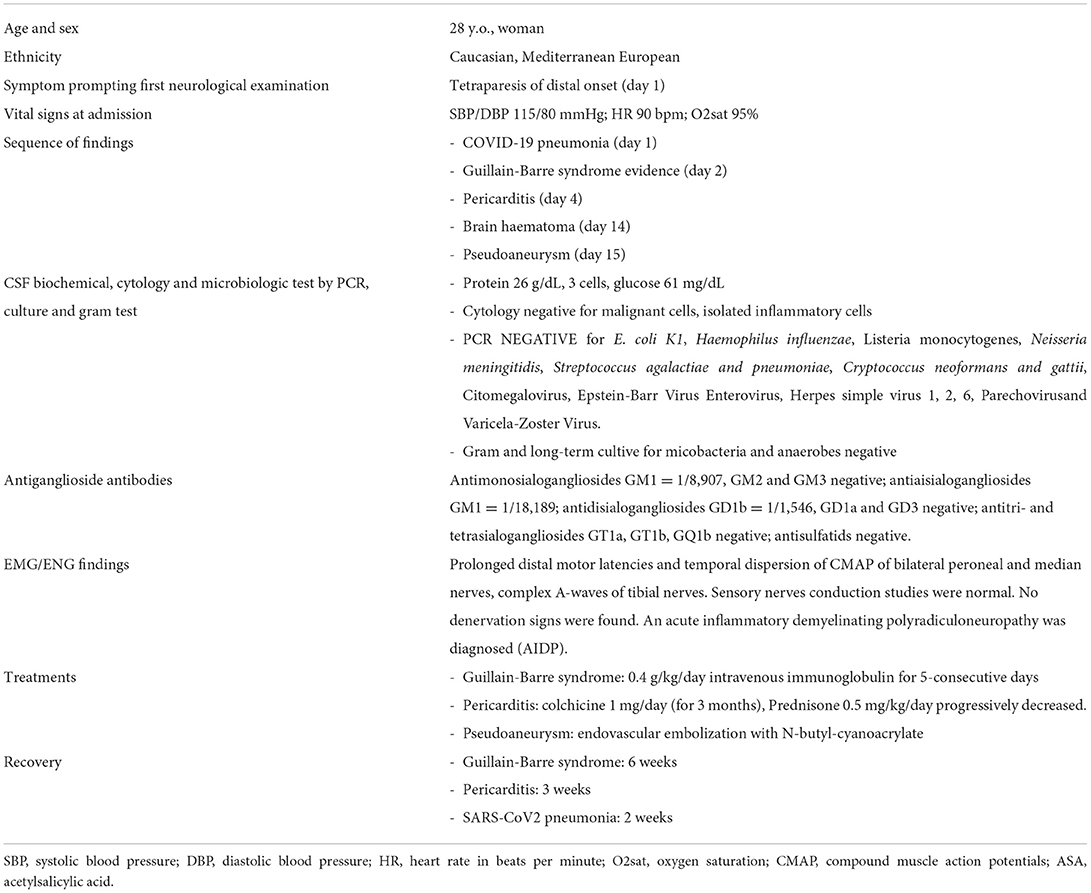
Table 1. Patient's demographic and clinical data.
On day 10, an elective tracheostomy was performed and sedation was suspended. Then, motor neurological improvement was observed on examination. Strikingly, a decreased level of consciousness and an absence of spontaneous language was observed on day 13. A brain CT scan (day 14) demonstrated an acute left parietal lobar haematoma (Figure 2A). It is worth noting that the patient was previously treated with a non-anticoagulant dose of enoxaparin 40 mg once/day (normal INR range in blood tests). A body CT and echography of the carotid, renal arteries, and heart were performed, finding no other aneurysms or pseudoaneurysms. Given these findings (and the arteriography results below), the absence of clinical features, and the lack of family history, other causes of aneurysms were reasonably discarded such as polycystic kidney disease, hereditary haemorrhagic telangiectasia, Ehlers-Danlos syndrome IV, Marfan syndrome, and neurofibromatosis I (7).
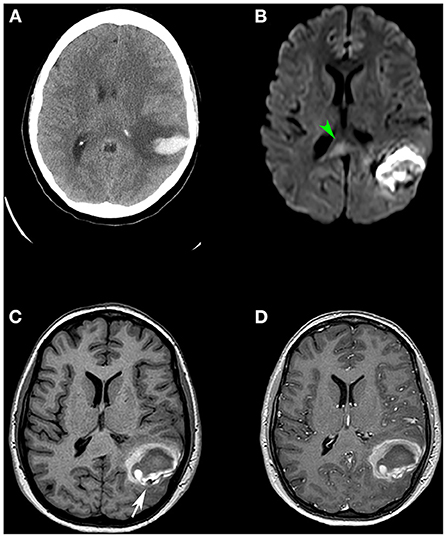
Figure 2. (A) Cranial CT scan showing left temporo-occipital intraparenchymal haematoma. (B) Diffusion-weighted MR image showing increased signal (diffusion restriction) and thickening of the splenium of the corpus callosum (green arrowhead), suggestive of a cytotoxic lesion of the corpus callosum (CLOCC). (C,D) 3D T1-weighted volumetric sequence without contrast (C) and with contrast (D) demonstrating the existence of a nodular image adjacent to the haematoma (white arrow). It presents as a signal void and after contrast administration, it enhances in an analogous way to vascular structures, compatible with a pseudoaneurysmal lesion.
On day 18, an MRI confirmed the haematoma and showed a striking image of an irregular artery (Figures 2C,D). Interestingly, the MRI also revealed a non-specific focus of increased signal in the splenium of the corpus callosum (Figure 2B) on DWI sequences suggesting a cytotoxic lesion of the corpus callosum (CLOCC).
After treatment and stabilization in the ICU, the patient presented clinical-neurological improvement (day 19). Then, diagnostic cerebral arteriography (day 24) showed a 4-mm distal pseudoaneurysm located in a branch of the temporo-occipital artery of the left middle cerebral artery (MCA), at the M4 level (Figure 3A). The parental artery of the pseudoaneurysm was a very thin caliber with irregular morphology, such as mycotic or vasculitic angiographic appearance (Figure 3B). Moreover, a hypoperfused left parietal lobe was observed, due to the mass effect of the haematoma, and a parieto-occipital artery from the left posterior cerebral artery (PCA) was compensating for the blood flow (Figure 3E). Given the high risk of rebleeding, endovascular treatment was decided upon. Therefore, complete embolization of the pseudoaneurysm (day 25) was carried out by sacrificing the parental artery by using the synthetic glue N-butyl-cyanocrylate (Glubran®, GME, Italy) through a 1.2F microcatheter (Magic®, Balt group, France) (Figures 3C,D). As expected, following the procedure, blood circulation was compensated by a parieto-occipital artery from the left PCA (Figure 3E). Two days later, the patient was clinically and neurologically recovered (excepting mild distal weakness in both hands) and was discharged from the hospital. A new MRI (Figure 3F) showed no ischemia, the CLOCC lesion had disappeared and the haematoma was reduced. Finally, a new angiography performed 3-weeks later showed no evidence of the pseudoaneurysm. At this point, motor function was completely recovered.
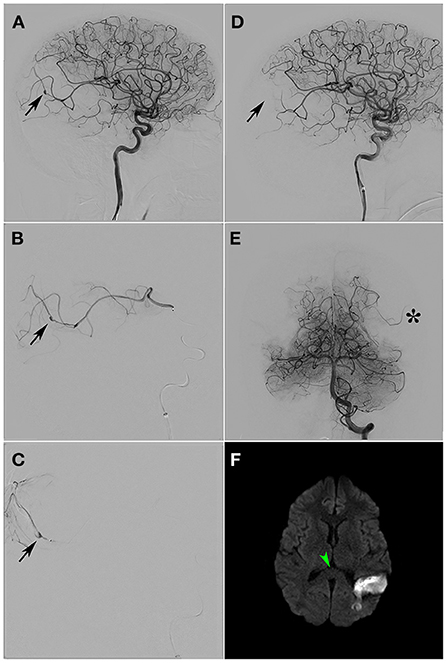
Figure 3. (A) Selective arteriography of RICA. The presence of a pseudoaneurysm is detected at the level of the distal temporo-occipital vasculature (black arrow). (B) Angular artery supraselective arteriography. The branch presenting the pseudoaneurysm shows an irregularity of the arterial wall suggesting arteritis (black arrow). (C) Glue cast after embolization (black arrow). (D) Selective arteriography of RICA after branch embolisation. Absence of pseudoaneurysm (black arrow). (E) Selective arteriography of LVA. Compensation of the left temporo-occipital territory through temporal branches of the left vertebral artery (black asterisk) is demonstrated. (F) Diffusion weighted MR image 1 month after treatment. Morphological and signal normalization of the splenium of the corpus callosum (green arrowhead). Absence of additional ischemic lesion after embolisation. RICA, Right internal carotid artery; LVA, Left vertebral artery.
Discussion
As previously reported, infectious pseudoaneurysms are often caused by bacteria or fungi and less frequently by viruses (8). COVID-19 has been reported as causing aneurysms and pseudoaneurysms in the heart and peripheral arteries (9–11). Nonetheless, only one case of cerebral pseudoaneurysm has been reported in an adolescent suffering from COVID-19 (6). This patient was diagnosed with a brain haematoma and a pseudoaneurysm in the left M2 segment. At this point, the patient had no respiratory symptoms caused by COVID-19 and the severe inflammatory or immune dysregulation took place 10 days after the treatment of the pseudoaneurysm by surgery.
In contrast, our patient suffered a severe immune reaction causing pericarditis and a severe Guillain-Barre syndrome with positive antiganglioside antibodies. Research on COVID-19 shows a prevalence of pericarditis of ~1.5% and it has been associated with increased odds of cardiac arrest, heart failure, and new-onset cardiovascular sequelae (12). Nonetheless, to the best of our knowledge, this is the first report of a patient suffering pericarditis and an intracranial pseudoaneurysm as COVID-19 complications. Moreover, in recent systematic reviews and meta-analyses, Guillain-Barre syndrome has been described in 1 per 10,000 cases of COVID-19 and antiganglioside antibodies have been reported in 0.8% of patients with Guillain-Barre and COVID-19 (13, 14). While few cases of Guillain-Barre and peripheral aneurysms have been reported, this is the first case reporting Guillain-Barre syndrome and an intracranial pseudoaneurysm related to COVID-19. No research has been conducted on antigangliosde antibodies and pseudoaneurysm formation. Furthermore, following the peak of the immune reaction, as suggested by the respiratory distress and the CRP plasma levels, our patient suffered a cerebral haematoma, and simultaneously, imaging tests demonstrated the presence of a CLOCC lesion and a pseudoaneurysm. CLOCCs have been described in a wide variety of conditions, including immune diseases, seizures, toxins, nutritional deficiencies, and infections such as the SARS-CoV2 as previously reported (15).
The SARS-CoV2 entry to the endothelial cell is facilitated by the binding of a spike protein to the angiotensin-converting enzyme-2 (ACE2) receptor leading to the inflammation and lesion of the artery wall through various mechanisms (16). Briefly, cell ACE2 internalization following SARS-CoV-2 entry impairs angiotensin 2 degradation and angiotensin 1–7 formation. Further, infected endothelial cells secrete cytokines and interferons which are recognized by their myeloid cell receptors mediating their migration and inflammatory activity. Moreover, spike protein exposure increases interleukins, MHC II, and costimulatory molecule (CD80 and CD86) expression by macrophages and dendritic cells, increasing the inflammatory and T cell-stimulatory activity (16). Finally, brain injury creates hypoxaemia, increasing proaneurysmal hypoxia-inducible factor (HIF)-1 levels. In this regard, previous studies have demonstrated that smooth muscle within the tunica media responds to localized hypoxia first by increasing HIF-1, resulting in the stabilization of the HIF-1α subunit, nuclear transcription, and binding to the hypoxia response element of VEGF and ets-1 transcription factor. The up-regulation of these genes induces the up-regulation of the matrix metalloproteinase (MMP)-2 and 9 and their increased protein levels. MMP-2 and 9 induce extensive artery matrix remodeling from tissue hypoxia (17). Therefore, we hypothesized that, through these mechanisms, SARS-CoV2 could cause aneurysms and pseudoaneurysms. Interestingly, evidence suggests that vascular dysfunction caused by COVID-19 manifests as deep venous thrombosis, embolism, and large arterial thrombosis. These manifestations are caused by hypoxaemia, viral sepsis, immobility, and vasculitis or vasculitis mimics (18, 19). Other cases of peripheral aneurysms and pseudoaneurysms have been reported (20, 21). These pseudoaneurysms secondary to COVID-19 are supposed to be secondary to inflammatory and vasculitis processes linked to viral multisystem inflammatory syndrome (18). Despite our radiological findings, the body CT scan and arteriography not being compatible with large/medium artery vasculitis means we cannot rule out that the formation of the pseudoaneurysm was caused by a multisystem inflammatory syndrome.
Several cases of endovascular treatment in pseudoaneurysms have been reported by using different approaches such as stents (22, 23), stent-assisted coils (24), embolic liquids/glues (25), and a case was even treated with a flow diverter device (26). In our case, we discarded the use of coils, stents, and flow diverter device because of the poor quality of the wall, thin artery caliber, and because the risk of haemorrhagic event was higher with the need for dual antiplatelet therapy. The reported case of pseudoaneurysm with simultaneous COVID-19 was treated with surgery (6). Nonetheless, we discarded that option to avoid significant periprocedural complications or poor outcomes as described (6).
In the present report, given the distal localization and the small caliber of the parental artery of the pseudoaneurysm, the evident collateral circulation from a parietal branch from the PCA, and the diminished parenchymal irrigation from the parental artery, we decided to sacrifice it by using embolic agents such as adhesive liquids and were successful.
Conclusion
To the best of our knowledge, here we report for the first time, a patient suffering a severe immune reaction caused by SARS-CoV2 infection and developing a cerebral pseudoaneurysm treated with endovascular embolization without complications.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comité de Ética de la Investigación con Medicamentos de la Gerencia de Atención integrada de Albacete. The patients/participants provided their written informed consent to participate in this study.
Author contributions
FH-F, JG-C, and EQ conceived the study and drafted the manuscript. FH-F, JG-C, EQ, JM-N, JG-G, MP, and TS acquired the data and critically reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Asociación Médica para Investigación y la Docencia de Albacete (AMIDA).
Acknowledgments
The authors thank the patient and her family for participating in the study as well as the staff from the Departments of Neurology, Radiology and ICU for their medical efforts in this case.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. (2020) 77:683–90. doi: 10.1001/jamaneurol.2020.1127
2. Catto AJ, Grant PJ. Risk factors for cerebrovascular disease and the role of coagulation and fibrinolysis. Blood Coagul Fibrinol. (1995) 6:497–510. doi: 10.1097/00001721-199509000-00001
3. Lazzaroni MG, Piantoni S, Masneri S, Garrafa E, Martini G, Tincani A, et al. Coagulation dysfunction in COVID-19: the interplay between inflammation, viral infection and the coagulation system. Blood Rev. (2021) 46:100745. doi: 10.1016/j.blre.2020.100745
4. Hernández-Fernández F, Sandoval Valencia H, Barbella-Aponte RA, Collado-Jiménez R, Ayo-Martín Ó, Barrena C, et al. Cerebrovascular disease in patients with COVID-19: neuroimaging, histological and clinical description. Brain. (2020) 143:3089–103. doi: 10.1093/brain/awaa239
5. Sweid A, Hammoud B, Bekelis K, Missios S, Tjoumakaris SI, Gooch MR, et al. Cerebral ischemic and hemorrhagic complications of coronavirus disease 2019. Int J Stroke. (2020) 15:733–42. doi: 10.1177/1747493020937189
6. Savić D, Alsheikh TM, Alhaj AK, Lazovic L, Alsarraf L, Bosnjakovic P, et al. Ruptured cerebral pseudoaneurysm in an adolescent as an early onset of COVID-19 infection: case report. Acta Neurochir. (2020) 162:2725–9. doi: 10.1007/s00701-020-04510-7
7. Brown R, Broderick J. Unruptured intracranial aneursyms: epidemiology, natural history, management options, and familial screening. Lancet Neurol. (2014) 13:393–404. doi: 10.1016/S1474-4422(14)70015-8
8. Zheng Y, Lu Z, Shen J, Xu F. Intracranial pseudoaneurysms: evaluation and management. Front Neurol. (2020) 11:582. doi: 10.3389/fneur.2020.00582
9. Khurram R, Karia P, Naidu V, Quddus A, Woo WL, Davies N. Pulmonary artery pseudoaneurysm secondary to COVID-19 treated with endovascular embolisation. Eur J Radiol Open. (2021) 8:100346. doi: 10.1016/j.ejro.2021.100346
10. Brennan S, Sulong S, Barret M. Left ventricular pseudoaneurysm: an inadvertent consequence of COVID-19-a case report. Eur Hert J Case Report. (2021) 5:ytab203. doi: 10.1093/ehjcr/ytab203
11. Basso C, Leone O, Rizzo S, De Gaspari M, Van Der Wal AC, Aubry MC, et al. Pathological features of COVID-19-associated myocardial injury: a multicentre cardiovascular pathology study. Eur Heart J. (2020) 41:3827–35. doi: 10.1093/eurheartj/ehaa664
12. Buckley B, Harrison S, Fazio-Eynullayeva E, Underhill P, Lane DA, Lip G. Prevalence and clinical outcomes of myocarditis and pericarditis in 718,365 COVID-19 patients. Eur J Clin Invest. (2021) 51:e13679. doi: 10.1111/eci.13679
13. Palaiodimou L, Stefanou MI, Katsanos AH, Fragkou PC, Papadopoulou M, Moschovos C, et al. Prevalence, clinical characteristics and outcomes of Guillain-Barré syndrome spectrum associated with COVID-19: a systematic review and meta-analysis. Eur J Neurol. (2021) 10:3517–29. doi: 10.1111/ene.14860
14. Guilmot A, Maldonado-Slootjes S, Sellimi A, Bronchain M, Hanseeuw B, Belkhir L, et al. Immune-mediated neurological syndromes in SARS-CoV-2-infected patients. J Neurol. (2021) 268:751–7. doi: 10.1007/s00415-020-10108-x
15. Lin J, Lawson EC, Verma S, Peterson RB, Sidhu R. Cytotoxic lesion of the corpus callosum in an adolescent with multisystem inflammatory syndrome and SARS-CoV2 infection. AJNR Am J Neuroradiol. (2020) 41:2017–9. doi: 10.3174/ajnr.A6755
16. Xu B, Li G, Guo J, Ikezoe T, Kasirajan K, Zhao S, et al. Angiotensin-converting enzyme 2, coronavirus disease 2019 and abdominal aortic aneurysms. J Vasc Surg. (2021) 74:1740–51. doi: 10.1016/j.jvs.2021.01.051
17. Erdozain OJ, Pegrum S, Winrow VR, Horrocks M, Stevens CR. Hypoxia in abdominal aortic aneurysm supports a role for HIF-1 and Ets-1 as drivers of matrix metalloproteinase upregulation in human aortic smooth muscle cells. J Vasc Res. (2011) 48:163–70. doi: 10.1159/000318806
18. McGonagle D, Bridgewood C, Ramanan AV, Meaney JFM, Watad A. COVID-19 vasculitis and novel vasculitis mimics. Lancet Rheumatol. (2021) 3:e224–33. doi: 10.1016/S2665-9913(20)30420-3
19. Evans P, Ed Rainger G, Mason J, Guzik T, Osto E, Stamataki Z, et al. Endothelial dysfunction in COVID-19: a position of the ESC Working Group for Atherosclerosis and Vascular Biology and the ESC Council of Basic Cardiovascular Science. Cardiovasc Res. (2020) 116:2177–84. doi: 10.1093/cvr/cvaa230
20. Dupuis M, Ronot M, Asselah T, Bodard S. COVID-19 associated hepatic artery pseudoaneurysms. Liver Int. (2022) 42:1907–8. doi: 10.1111/liv.15344
21. Shenavandeh S, Johari HG, Aflaki E. Association of large vessel aneurysm/pseudoaneurysm/aortitis and deep vein thrombosis in patients with Behcet's disease: a case report. Curr Rheumatol Rev. (2022) 18:83–7. doi: 10.2174/1573397117666210920154400
22. Lim YC, Kang JK, Chung J. Reconstructive stent-buttressed coil embolization of a traumatic pseudoaneurysm of the supraclinoid internal carotid artery. Acta Neurochir. (2012) 154:477-80. doi: 10.1007/s00701-011-1251-7
23. Samia MT, Gattozzia DA, Solimanb HM, Reeves AR, Moran CJ, Camarata PJ, et al. Use of Pipeline™ embolization device for the treatment of traumatic intracranial pseudoaneurysms: case series and review of cases from literature. Clin Neurol Neurosurg. (2018) 169:154–60. doi: 10.1016/j.clineuro.2018.04.012
24. van Rooij WJ, Van Rooij SBT. Endovascular treatment of traumatic pericallosal artery aneurysms. A case report. Interv Neroradiol. (2013) 19:56–9. doi: 10.1177/159101991301900108
25. Medel R, Webster Crowley R, Kojo Hamilton D, Dumont AS. Endovascular obliteration of an intracranial pseudoaneurysm: the utility of Onyx. J Neurosurg Pediatr. (2009) 4:445–8. doi: 10.3171/2009.6.PEDS09104
Keywords: COVID-19, pseudoaneurysm, subarachnoid hemorrhage, embolization (therapeutic), CLOCCs, Guillain-Barre syndrome
Citation: García-Carmona JA, von Quednow E, Hernández-Fernández F, Molina-Nuevo JD, García-García J, Palao M and Segura T (2022) Case report: Endovascular embolization of a cerebral pseudoaneurysm caused by SARS-CoV2 infection. Front. Neurol. 13:991610. doi: 10.3389/fneur.2022.991610
Received: 11 July 2022; Accepted: 01 September 2022;
Published: 04 October 2022.
Edited by:
Osama O. Zaidat, Northeast Ohio Medical University, United StatesReviewed by:
Shrebash Paul, Dhaka Infectious Disease Hospital, BangladeshKatrin Barbara Magda Frauenknecht, Laboratoire National de Santé (LNS), Luxembourg
Copyright © 2022 García-Carmona, von Quednow, Hernández-Fernández, Molina-Nuevo, García-García, Palao and Segura. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco Hernández-Fernández, fco.hdez.fdez@gmail.com
†These authors have contributed equally to this work
‡ORCID: Juan Antonio García-Carmona orcid.org/0000-0003-3938-7698
Francisco Hernández-Fernández orcid.org/0000-0001-6681-2683