The Impact of ABO Blood Grouping on COVID-19 Vulnerability and Seriousness: A Retrospective Cross-Sectional Controlled Study among the Arab Community

 , , ,
, , ,
Abstract
:1. Introduction
2. Subjects and Method
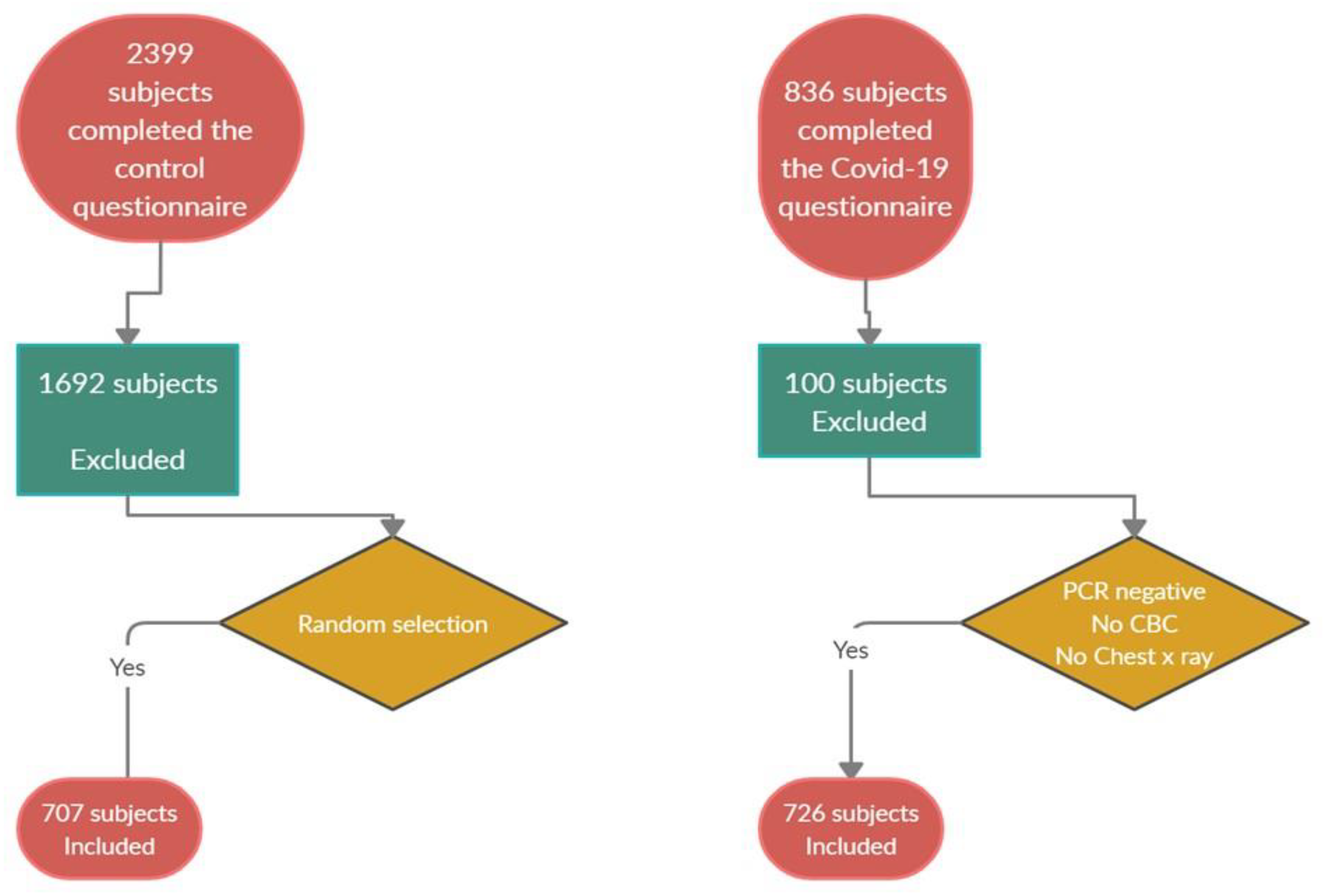
2.1. Study Protocol
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Sample Size
Study Variables
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Blood Grouping of the Study Population
3.2. Association between COVID-19 Virus Infection and the ABO Blood Group
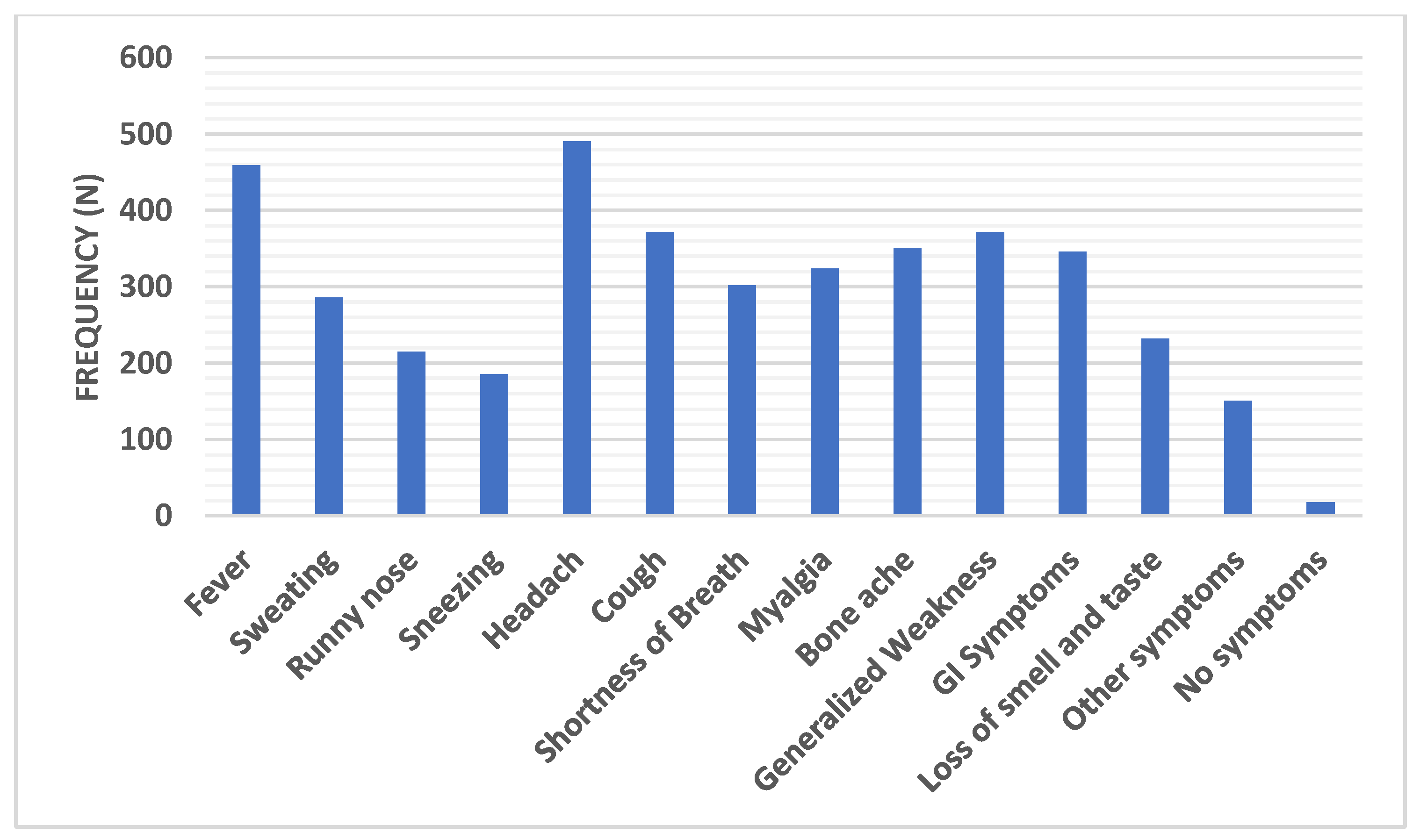
3.3. Distribution of the Common Symptoms Recorded among the COVID-19 Group
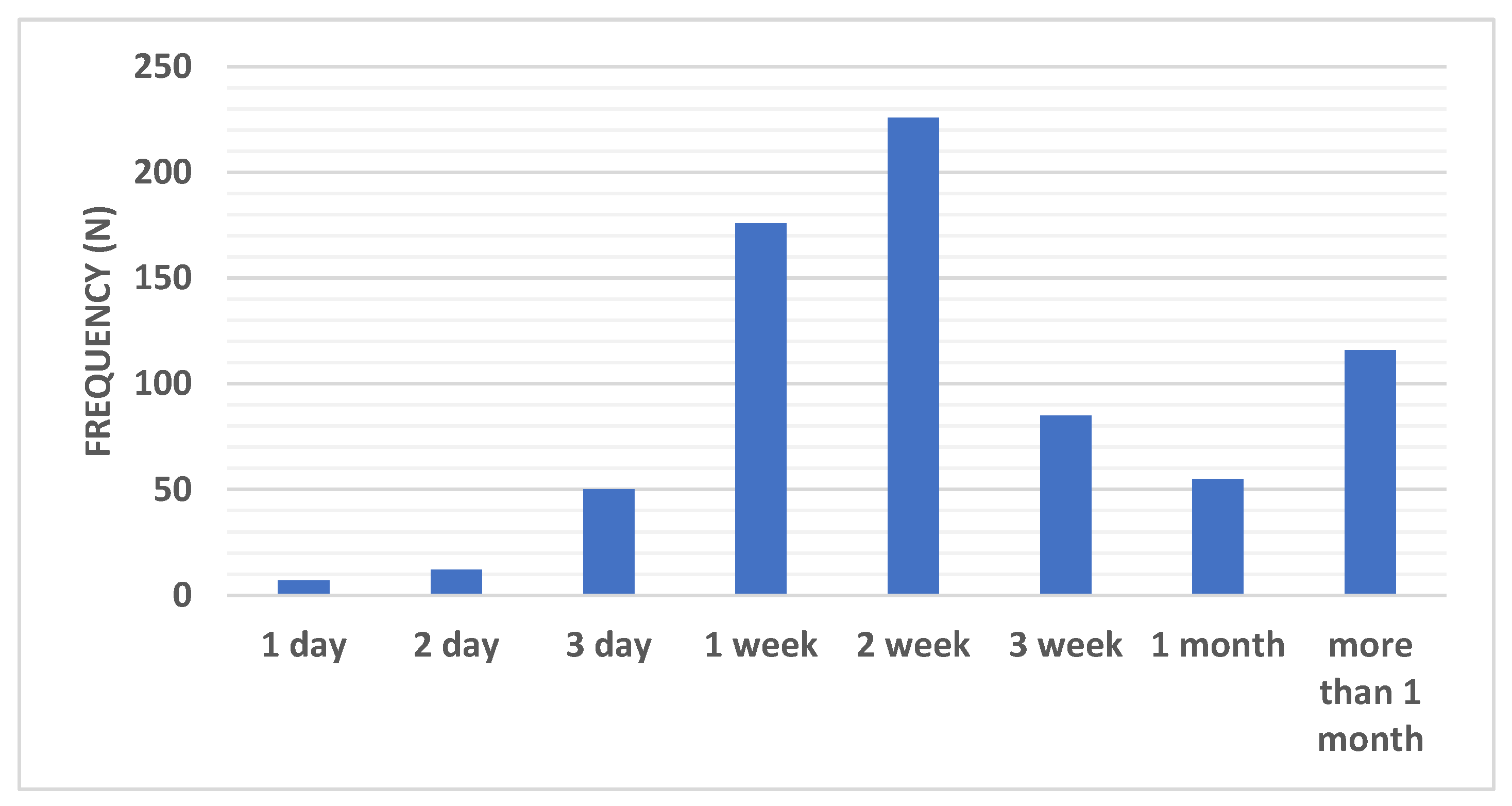
3.4. Distribution of Recovery Periods Recorded among the COVID-19 Group
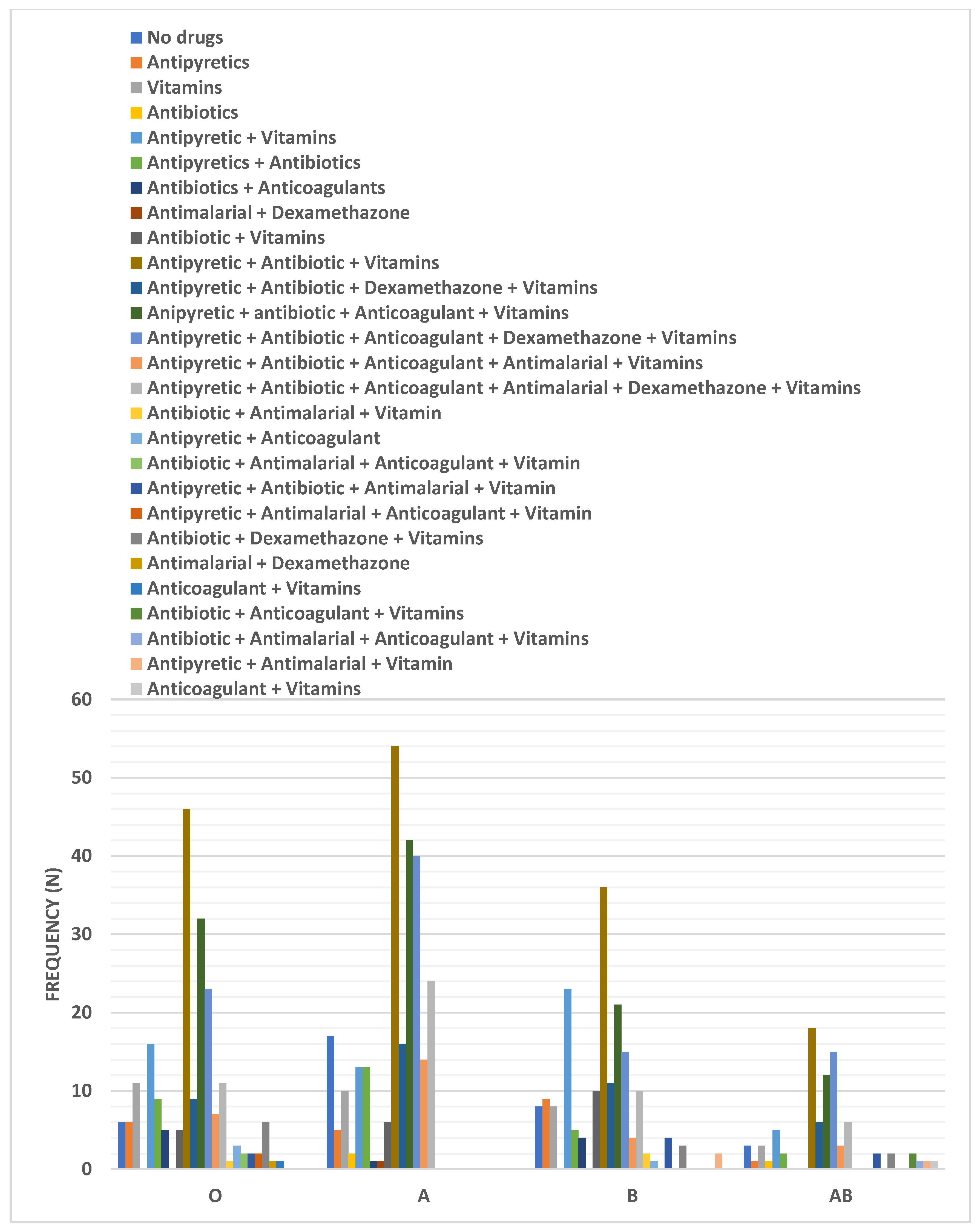
3.5. Distribution of Different Treatment Regimens among the COVID-19 Group According to Blood Grouping
3.6. Correlation of Different COVID-19 Symptoms, the Need for Hospitalization, Recovery Time, PCR Results, and ABO Blood Grouping
3.7. Outcomes of Some Research Studies Which Document the Effect of ABO Blood Grouping on the Risk of COVID-19 Infection and Severity in Comparison with the Present Study Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy Eur. J. Allergy Clin. Immunol. 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Malik, Y. Properties of Coronavirus and SARS-CoV-2—PubMed. Malays. J. Pathol. 2020, 42, 3–11. [Google Scholar] [PubMed]
- Du, Z.; Xu, X.; Wang, L.; Fox, S.; Cowling, B.; Galvani, A.; Meyers, L. Effects of Proactive Social Distancing on COVID-19 Outbreaks in 58 Cities, China. Emerg. Infect. Dis. 2020, 26, 2267–2269. [Google Scholar] [CrossRef]
- Guo, Z.; Wang, Z.; Zhang, S.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.; Dong, Y.; Chi, X.; et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg. Infect. Dis. 2020, 26, 1586–1591. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Feng, X.; Li, P.; Ma, L.; Liang, H.; Lei, J.; Li, W.; Wang, K.; Song, Y.; Li, S.; Yang, W.; et al. Clinical Characteristics and Short-Term Outcomes of Severe Patients with COVID-19 in Wuhan, China. Front. Med. 2020, 7, 491. [Google Scholar] [CrossRef]
- Udugama, B.; Kadhiresan, P.; Kozlowski, H.; Malekjahani, A.; Osborne, M.; Li, V.; Chen, H.; Mubareka, S.; Gubbay, J.; Chan, W. Diagnosing COVID-19: The Disease and Tools for Detection. ACS Nano 2020, 14, 3822–3835. [Google Scholar] [CrossRef] [Green Version]
- Anstee, D. The relationship between blood groups and disease. Blood 2010, 115, 4635–4643. [Google Scholar] [CrossRef] [Green Version]
- Silva-Filho, J.; de Melo, C.; Oliveira, J. The influence of ABO blood groups on COVID-19 susceptibility and severity: A molecular hypothesis based on carbohydrate-carbohydrate interactions. Med. Hypotheses 2020, 144, 110155. [Google Scholar] [CrossRef]
- Groot, H.; Sierra, L.; Said, M.; Lipsic, E.; Karper, J.; Van Der Harst, P. Genetically determined ABO blood group and its associations with health and disease. Arter. Thromb. Vasc. Biol. 2020, 40, 830–838. [Google Scholar] [CrossRef]
- Stowell, S.; Stowell, C. Biologic roles of the ABH and Lewis histo-blood group antigens part II: Thrombosis, cardiovascular disease and metabolism. Vox Sang. 2019, 114, 535–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Yang, Y.; Huang, H.; Li, D.; Gu, D.; Lu, X.; Zhang, Z.; Liu, L.; Liu, T.; Liu, Y.; et al. Relationship between the ABO Blood Group and the COVID-19 Susceptibility. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Gu, D.; Yu, J.; Yang, J.; Wang-Qin, S. Association between ABO blood groups and COVID-19 infection, severity and demise: A systematic review and meta-analysis. Infect. Genet. Evol. 2020, 84, 104485. [Google Scholar] [CrossRef] [PubMed]
- Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi PJuzėnas, S. Genomewide Association Study of Severe Covid-19 with Respiratory Failure. N. Engl. J. Med. 2020, 383, 1522–1534. [Google Scholar] [CrossRef] [PubMed]
- Muñiz-Diaz, E.; Llopis, J.; Parra, R.; Roig, I.; Ferrer, G.; Grifols, J.; Millán, A.; Ene, G.; Ramiro, L.; Maglio, L.; et al. Relationship between the ABO blood group and COVID-19 susceptibility, severity and mortality in two cohorts of patients. Blood Transfus. 2020. [Google Scholar] [CrossRef]
- Flegel, W. COVID-19: Risk of infection is high, independently of ABO blood group. Haematologica 2020, 105, 2706–2708. [Google Scholar] [CrossRef]
- Boudin, L.; Janvier, F.; Bylicki, O.; Dutasta, F. ABO blood groups are not associated with risk of acquiring the SARS-CoV-2 infection in young adults. Haematologica 2020, 105, 2841–2843. [Google Scholar] [CrossRef]
- Kibler, M.; Dietrich, L.; Kanso, M.; Carmona, A.; Marchandot, B.; Matsushita, K.; Trimaille, A.; How-Choong, C.; Odier, A.; Gennesseaux, G.; et al. Risk and Severity of COVID-19 and ABO Blood Group in Transcatheter Aortic Valve Patients. J. Clin. Med. 2020, 9, 3769. [Google Scholar] [CrossRef]
- Ray, J.; Schull, M.; Vermeulen, M.; Park, A. Association Between ABO and Rh Blood Groups and SARS-CoV-2 Infection or Severe COVID-19 Illness. Ann. Intern. Med. 2020, 24, m20-4511. [Google Scholar] [CrossRef]
- Hoiland, R.; Fergusson, N.; Mitra, A.; Griesdale, D.; Devine, D.; Stukas, S.; Cooper, J.; Thiara, S.; Foster, D.; Chen, L.; et al. The association of ABO blood group with indices of disease severity and multiorgan dysfunction in COVID-19. Blood Adv. 2020, 4, 4981–4989. [Google Scholar] [CrossRef] [PubMed]
- Solmaz, I.; Araç, S. ABO Blood groups in COVID-19 patients; cross-sectional study. Int J. Clin. Pract. 2020, e13927. [Google Scholar] [CrossRef]
- Göker, H.; Aladağ-Karakulak, E.; Demiroğlu, H.; Ayaz, C.; Büyükaşik, Y.; İnkaya, A.; Aksu, S.; Sayinalp, N.; Haznedaroğlu, İ.; Uzun, Ö.; et al. The effects of blood group types on the risk of COVID-19 infection and its clinical outcome. Turk. J. Med. Sci. 2020, 50, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, X.; Chen, J.; Cai, Y.; Deng, A.; Yang, M. Association between ABO blood groups and risk of SARS-CoV-2 pneumonia. Br. J. Haematol. 2020, 190, 24–27. [Google Scholar] [CrossRef]
- Fan, Q.; Zhang, W.; Li, B.; Li, D.J.; Zhang, J.; Zhao, F. Association Between ABO Blood Group System and COVID-19 Susceptibility in Wuhan. Front. Cell. Infect. Microbiol. 2020, 10, 404. [Google Scholar] [CrossRef]
- May, J.; McGwin, G.; Gangaraju, R.; Paschal, R.; Weaver, K.; Lima, J.; Marques, M. Questioning the association between ABO type and outcomes in patients with COVID-19. Ann. Hematol. 2020, 1–2. [Google Scholar] [CrossRef]
- Barnkob, M.; Pottegård, A.; Støvring, H.; Haunstrup, T.; Homburg, K.; Larsen, R.; Hansen, M.; Titlestad, K.; Aagaard, B.; Møller, B.; et al. Reduced prevalence of SARS-CoV-2 infection in ABO blood group O. Blood Adv. 2020, 4, 4990–4993. [Google Scholar] [CrossRef]
- Ad’hiah, A.; Allami, R.; Mohsin, R.; Abdullah, M.; AL-Sa’ady, A.; Alsudani, M. Evaluating of the association between ABO blood groups and coronavirus disease 2019 (COVID-19) in Iraqi patients. Egypt. J. Med. Hum. Genet. 2020, 21, 50. [Google Scholar] [CrossRef]
- Padhi, S.; Suvankar, S.; Dash, D.; Panda, V.; Pati, A.; Panigrahi, J.; Panda, A. ABO blood group system is associated with COVID-19 mortality: An epidemiological investigation in the Indian population. Transfus. Clin. Biol. 2020, 27, 253–258. [Google Scholar] [CrossRef]
- Taha, S.A.H.; Osman, M.E.M.; Abdoelkarim, E.A.A.; Holie, M.A.I.; Elbasheir, M.M.; Abuzeid, N.M.K.; Al-Thobaiti, S.A.; Fadul, S.B.; Konozy, E.H.E. Individuals with a Rh-positive but not Rh-negative blood group are more vulnerable to SARS-CoV-2 infection: Demographics and trend study on COVID-19 cases in Sudan. New Microbes New Infect. 2020, 38, 100763. [Google Scholar] [CrossRef]
- Abdollahi, A.; Mahmoudi-Aliabadi, M.; Mehrtash, V.; Jafarzadeh, B.; Salehi, M. The novel coronavirus sars-cov-2 vulnerability association with abo/rh blood types. Iran. J. Pathol. 2020, 15, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Golinelli, D.; Boetto, E.; Maietti, E.; Fantini, M. The association between ABO blood group and SARS-CoV-2 infection: A meta-analysis. PLoS ONE 2020, 15, e0239508. [Google Scholar] [CrossRef]
- Zietz, M.; Zucker, J.; Tatonetti, N. Associations between blood type and COVID-19 infection, intubation, and death. Nat. Commun. 2020, 11, 5761. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Fan, H.; Lu, D.; Huang, F.; Meng, X.; Li, Z.; Tang, M.; Zhang, J.; Liu, N.; Liu, Z.; et al. Association between ABO blood groups and clinical outcome of coronavirus disease 2019: Evidence from two cohorts. medRxiv 2020. [Google Scholar] [CrossRef]
- Latz, C.A.; DeCarlo, C.; Boitano, L.; Png, C.Y.M.; Patell, R.; Conrad, M.F.; Eagleton, M.; Dua, A. Blood type and outcomes in patients with COVID-19. Ann. Hematol. 2020, 99, 2113–2118. [Google Scholar] [CrossRef]
- Cooling, L. Blood groups in infection and host susceptibility. Clin. Microbiol. Rev. 2015, 28, 801–870. [Google Scholar] [CrossRef] [Green Version]
- Guillon, P.; Clément, M.; Sébille, V.; Rivain, J.G.; Chou, C.F.; Ruvoën-Clouet, N.; Le Pendu, J. Inhibition of the interaction between the SARS-CoV Spike protein and its cellular receptor by anti-histo-blood group antibodies. Glycobiology 2008, 18, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Moore, M.J.; Vasllieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greeneugh, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Krüger, N.; Müller, M.; Drosten, C.; Pöhlmann, S. The novel coronavirus 2019 (2019-nCoV) uses the SARS-coronavirus receptor ACE2 and the cellular protease TMPRSS2 for entry into target cells. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94, 127–147. [Google Scholar] [CrossRef] [Green Version]
- Naitza, S.; Porcu, E.; Steri, M.; Taub, D.; Mulas, A.; Xiao, X.; Strait, J.; Dei, M.; Lai, S.; Busonero, F.; et al. A genome-wide association scan on the levels of markers of inflammation in sardinians reveals associations that underpin its complex regulation. PLoS Genet. 2012, 8, e1002480. [Google Scholar] [CrossRef] [PubMed]
- Gubernatorova, E.; Gorshkova, E.; Polinova, A.; Drutskaya, M. IL-6: Relevance for immunopathology of SARS-CoV-2. Cytokine Growth Factor Rev. 2020, 53, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, F.; Yamamoto, M.; Muñiz-Diaz, E. Blood group ABO polymorphism inhibits SARS-CoV-2 infection and affects COVID-19 progression. Vox Sang. 2020. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lian, J.; Jin, X.; Hao, S.; Jia, H.; Cai, H.; Zhang, X.; Hu, J.; Zheng, L.; Wang, X.; Zhang, S.; et al. Epidemiological, clinical, and virological characteristics of 465 hospitalized cases of coronavirus disease 2019 (COVID-19) from Zhejiang province in China. Influenza Other Respi. Viruses 2020, 14, 564–574. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.; et al. Clinical characteristics of 2019 novel coronavirus infection in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Zhan, T.; Liu, M.; Tang, Y.; Han, Z.; Cheng, X.; Deng, J.; Chen, X.; Tian, X.; Huang, X. Retrospective analysis of clinical characteristics of 405 patients with COVID-19. J. Int. Med. Res. 2020, 48, 1–10. [Google Scholar] [CrossRef]
- Xia, J.; Tong, J.; Liu, M.; Shen, Y.; Guo, D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J. Med. Virol. 2020, 92, 589–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Kang, Z.; Gong, H.; Xu, D.; Wang, J.; Li, Z.; Cui, X.; Xiao, J.; Meng, T.; Zhou, W.; et al. The digestive system is a potential route of 2019-nCov infection: A bioinformatics analysis based on single-cell transcriptomes. bioRxiv 2020. [Google Scholar] [CrossRef]
- Jin, X.; Lian, J.S.; Hu, J.H.; Gao, J.; Zheng, L.; Zhang, Y.M.; Hao, S.R.; Jia, H.Y.; Cai, H.; Zhang, X.L.; et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Agrawal, S.; Ish, P.; Mishra, S.; Gaind, R.; Usha, G.; Singh, B.; Sen, M.K.; Chakrabarti, S.; Gupta, N.K.; et al. Clinical and epidemiologic profile of the initial COVID-19 patients at a tertiary care centre in India. Monaldi Arch. Chest Dis. 2020, 90, 193–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency, n (%) | |||
|---|---|---|---|
| Control (n = 707) | COVID-19 (n = 726) | Chi-Square p Value | |
| Nationality | |||
| Egyptians | 699 (98.9%) | 700 (96.4%) | 0.0007 *** |
| Saudi | 2 (0.3%) | 20 (2.8%) | |
| Other | 6 (0.8%) | 6 (0.8%) | |
| Gender | |||
| Male | 117 (16.5%) | 110 (15.2%) | 0.4689 |
| Female | 590 (83.5%) | 616 (84.8%) | |
| Age (year) | |||
| <20 | 38 (5.4%) | 9 (1.3%) | 0.0002 *** |
| 20–40 | 565 (79.9%) | 596 (82.1%) | |
| 40–60 | 90 (12.7%) | 104 (14.3%) | |
| >60 | 14 (2%) | 17 (2.3%) | |
| PCR Result | |||
| Positive | 278 (38.3%) | ||
| Negative | 157 (21.6%) | ||
| Not done | 291 (40.1) | ||
| Type of Blood Group | |||
| O | 253 (36%) | 204 (28%) | 0.0096 ** |
| A | 207 (29%) | 258 (35%) | |
| B | 163 (23%) | 180 (25%) | |
| AB | 84 (12%) | 84 (12%) | |
| Type of Rh | |||
| Negative | 113 (16%) | 135 (18.6%) | 0.1913 |
| Positive | 594 (84%) | 591 (81.4%) | |
| Frequency, n (%) | |||||
|---|---|---|---|---|---|
| O (n = 204) | A (n = 258) | B (n = 180) | AB (n = 84) | Chi-Square p Value | |
| Body Temperature (°C) | |||||
| 37–38 | 86 (42.2%) | 110 (42.6%) | 84 (46.7%) | 32 (38.1%) | 0.3765 |
| 38–39 | 90 (44.1%) | 96 (37.2%) | 65 (36.1%) | 33 (39.3%) | |
| 39–40 | 21 (10.3%) | 45 (17.5%) | 24 (13.3%) | 17 (20.2%) | |
| 40–41 | 7 (3.4%) | 7 (2.7%) | 7 (3.9%) | 2 (2.4%) | |
| Headache | |||||
| Yes | 128 (62.7%) | 150 (58.1%) | 101 (56.1%) | 57 (67.9%) | 0.2300 |
| No | 76 (37.3%) | 108 (41.9%) | 79 (43.9%) | 27 (32.1%) | |
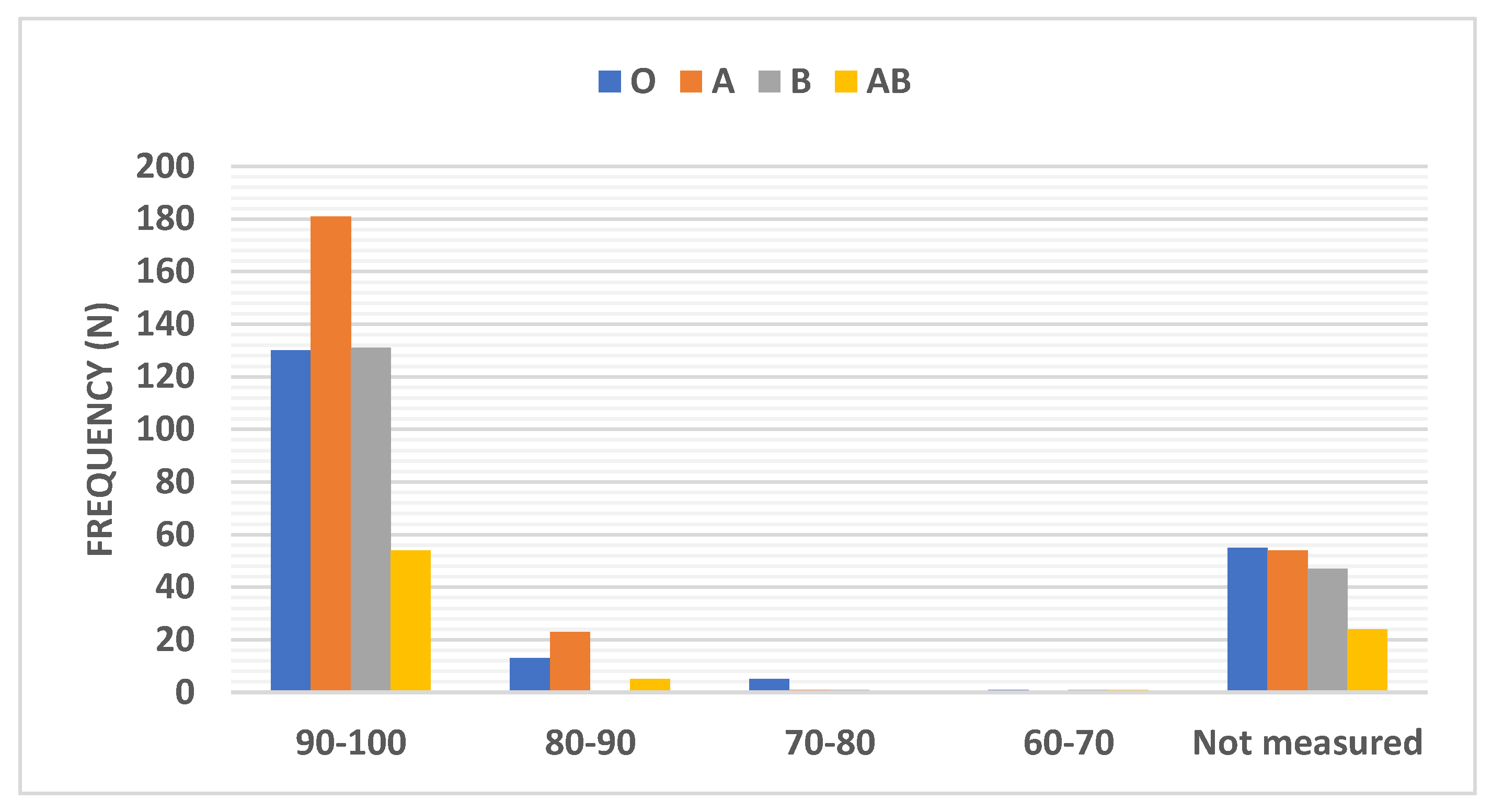
| Oxygen Saturation (%) | |||||
| 90–100 | 130 (63.7%) | 181 (69.9%) | 131 (72.8%) | 54 (64.3%) | |
| 80–90 | 13 (6.4%) | 23 (8.9%) | 0.0 (0.0%) | 5 (5.9%) | 0.0029 ** |
| 70–80 | 5 (2.5%) | 1 (0.4%) | 1 (0.6%) | 0.0 (0.0%) | |
| 60–70 | 1 (0.5%) | 0.0 (0.0%) | 1 (0.6%) | 1 (1.2%) | |
| Not measured | 55 (26.9%) | 54 (20.5%) | 47 (26.1%) | 24 (28.6) | |
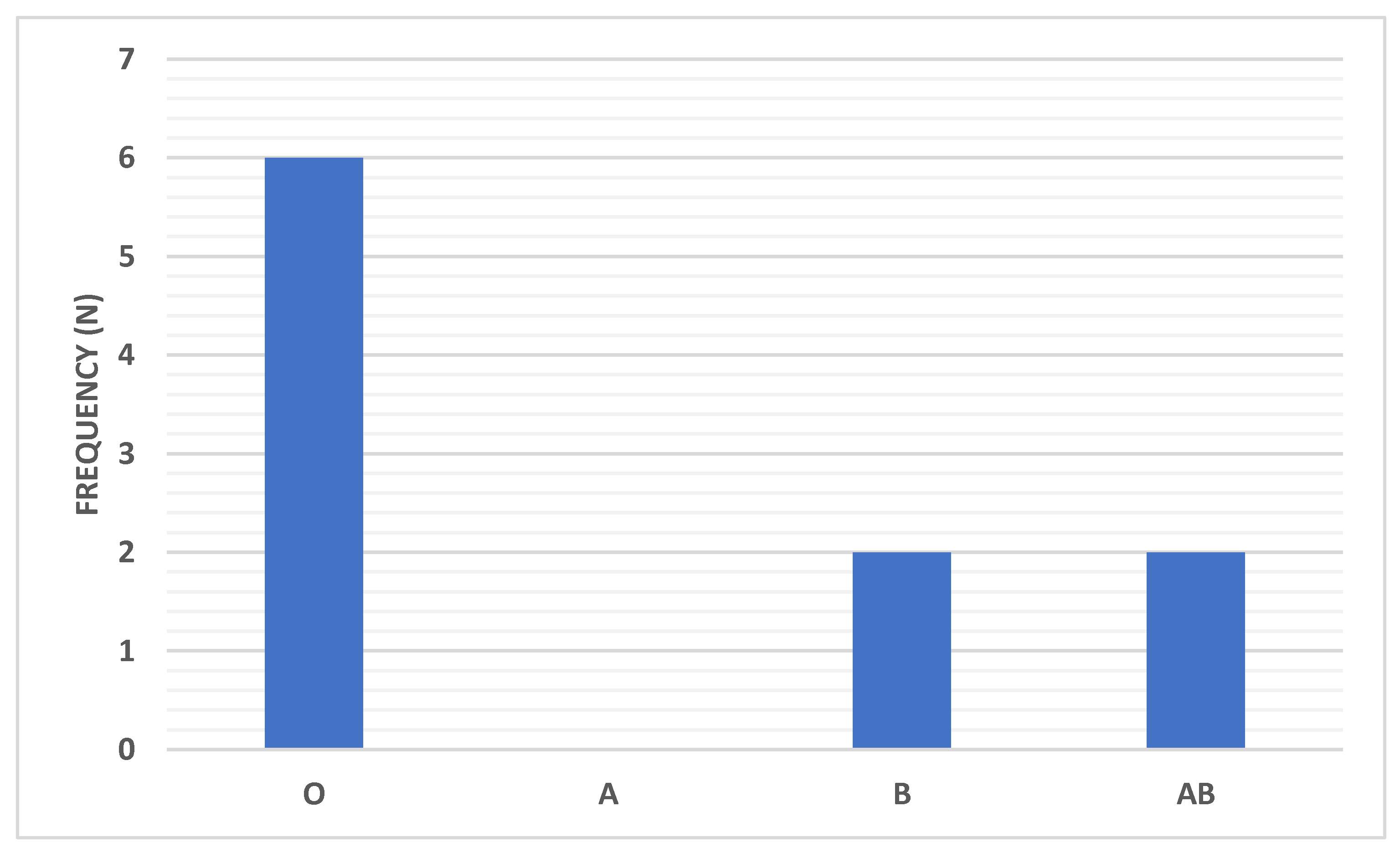
| Artificial respiration | |||||
| Yes | 6 (2.9%) | 0 (0%) | 2 (1.1%) | 2 (2.4%) | 0.0462 |
| No | 198 (97.1%) | 258 (100%) | 178 (98.9%) | 82 (97.6%) | |
| Shortness of Breath | |||||
| Yes | 85 (41.7%) | 117 (45.3%) | 63 (35%) | 35 (41.7%) | 0.1946 |
| No | 119 (58.3%) | 141 (54.7%) | 117 (65.5%) | 49 (58.3%) | |
| Cough | |||||
| Yes | 103 (50.5%) | 136 (52.7%) | 88 (48.9%) | 38 (45.2%) | 0.6576 |
| No | 101 (49.5%) | 122 (47.3%) | 92 (51.1%) | 46 (54.8%) | |
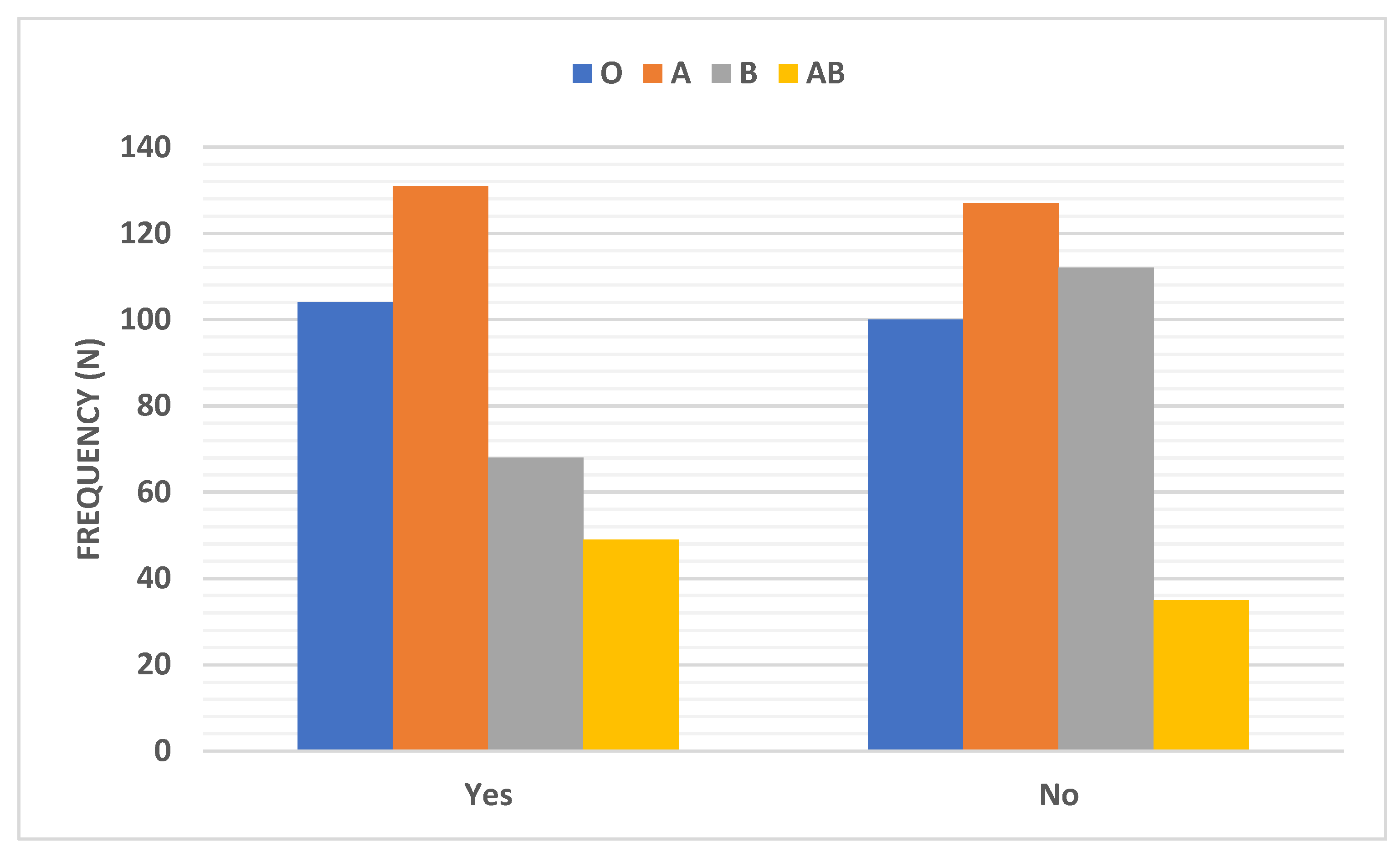
| Myalgia | |||||
| Yes | 104 (51%) | 131 (51%) | 68 (37.8%) | 49 (58.3%) | 0.0057 ** |
| No | 100 (49%) | 127 (49%) | 112 (62.2%) | 35 (41.7%) | |
| Bone ache | |||||
| Yes | 96 (47.1%) | 120 (46.5%) | 66 (36.7%) | 43 (51.2%) | 0.0742 |
| No | 108 (52.9%) | 138 (53.5%) | 114 (63.3%) | 41 (48.8%) | |
| GIT Symptoms | |||||
| Yes | 104 (51%) | 124 (48%) | 83 (46%) | 41 (49%) | 0.8166 |
| No | 100 (49%) | 134 (52%) | 97 (54%) | 43 (51%) | |
| Hospitalization | |||||
| Yes | 16 (7.8%) | 18 (7.0%) | 15 (8.3%) | 6 (7.1%) | 0.9556 |
| No | 188 (92.2%) | 240 (93.0) | 165 (91.7%) | 78 (92.9%) | |
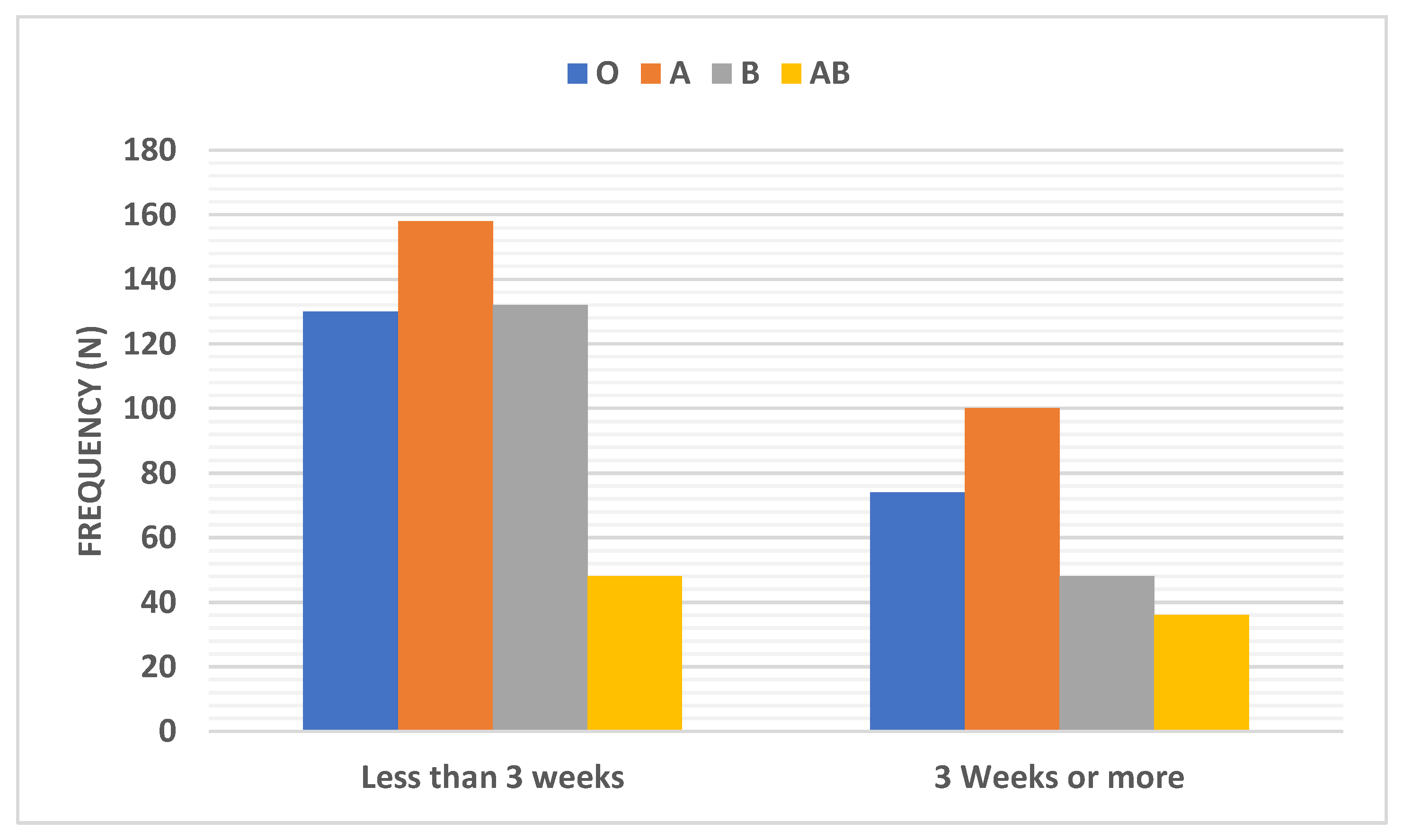
| Recovery Time | |||||
| Less than 3 weeks | 130 (63.7%) | 158 (61.2%) | 132 (73.3%) | 48 (57.1%) | 0.0248 * |
| 3 Weeks or more | 74 (36.3%) | 100 (38.8%) | 48 (26.7%) | 36 (42.9%) | |
| PCR Result | |||||
| Positive | 70 (34.3%) | 110 (42.6%) | 69 (38.3%) | 30 (35.7%) | 0.1571 |
| Negative | 43 (21.1%) | 42 (16.3%) | 43 (23.8) | 20 (23.8%) | |
| Not done | 91 (44.6%) | 106 (41.1) | 68 (37.8) | 34 (40.5%) | |
| Study | Location | Number of COVID-19 Patients | ABO and Risk of COVID-19 Infection | ABO and COVID-19 Severity | Drawbacks | Agreement with the Present Study Results | |
|---|---|---|---|---|---|---|---|
| Infection | Severity | ||||||
| Ellinghaus et al. [15] | Italy Spain | 1980 ICU | GroupA+ at higher risk of respiratory failure, group O at lower risk | No | |||
| Muñiz-Diaz et al. [16] | Spain | 854 MCPD 956 SCPT | MCPD Group A at higher risk Group O at lower risk SCPT No association | MCPD Group A high mortality risk, group O low mortality SCPT No association | Yes O less | No | |
| Boudin et al. and Flegel, [17,18] | France | 1279 | No association between ABO and Rh blood groups and risk of COVID-19 infection | Concerning O2 therapy requirement, 5 patients were group A; 5 group B, and 10 group O The patients admitted to the ICU were 1 group B and 2 group O | Missed blood groups of 16 patient | No | Yes More group O patients required O2 and ICU |
| Kibler et al. [19] | France | 19 TAVR | Group A at higher risk | Group A showed unfavorable outcomes | No | No | |
| Ray et al. [20] | Canada | 225 556 | Group O− at lower risk | Group O− may be associated with severe illness | Yes O less | Yes O more | |
| Hoiland et al. [21] | Canada | 22 ICU | Groups A or AB showed more required mechanical ventilation, CRRT, and prolonged ICU admission than groups O or B | No | |||
| Solmaz and Araç, [22] | Turkey | 1667 | Group A at higher risk Group O at lower risk | Group A does not affect the course of the disease and is not associated with mortality | Yes Group O less | Yes Group A did not have increased mortality | |
| Göker et al. [23] | Turkey | 207 | Group A at higher risk Group O at lower risk | ABO groups do not influence clinical outcome | No | No | |
| Li et al. [24] | China | 3959 | Group A at higher risk Group O at lower risk | Group A was at higher risk of hospitalization, and group O had a lower risk | Yes Group O less | No | |
| Fan et al. [25] | China | 105 | Group A (females) at higher risk | Small sample size | No | ||
| May et al. [26] | USA | 165 | No association between ABO and Rh blood groups and risk of COVID-19 infection | No association between blood group and severity | Small sample size | No | No |
| Barnkob et al. [27] | Denmark | 7422 | Group O at low risk | No association between ABO blood group and the risk for hospitalization or death | Yes Group O less | No | |
| Ad’hiah et al. [28] | Iraq | 300 | Group AB at higher risk | Group A may be associated with an increased risk of death | No | No | |
| Padhi et al. [29] | India | 8452 | Group O associated with a decreased mortality rate, group B associated with an increased mortality rate | No | |||
| Taha et al. [30] | Sudan | 557 | Group A+ at higher risk Group O+ at lower risk | Yes Group O less | |||
| Abdollahi et al. [31] | Iran | 397 | Group AB at higher risk Group O at lower risk | Yes Group O less | |||
| Golinelli et al. [32] | Meta-analysis heterogenous population | 7503 | Group A at higher risk Group O at lower risk | Considerable heterogeneity found in the study population and the online date, which are still preliminary | Yes O less | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Shitany, N.A.; El-Hamamsy, M.; Alahmadi, A.A.; Eid, B.G.; Neamatallah, T.; Almukadi, H.S.; Arab, R.A.; Faddladdeen, K.A.; Al-Sulami, K.A.; Bahshwan, S.M.; et al. The Impact of ABO Blood Grouping on COVID-19 Vulnerability and Seriousness: A Retrospective Cross-Sectional Controlled Study among the Arab Community. Int. J. Environ. Res. Public Health 2021, 18, 276. https://doi.org/10.3390/ijerph18010276
El-Shitany NA, El-Hamamsy M, Alahmadi AA, Eid BG, Neamatallah T, Almukadi HS, Arab RA, Faddladdeen KA, Al-Sulami KA, Bahshwan SM, et al. The Impact of ABO Blood Grouping on COVID-19 Vulnerability and Seriousness: A Retrospective Cross-Sectional Controlled Study among the Arab Community. International Journal of Environmental Research and Public Health. 2021; 18(1):276. https://doi.org/10.3390/ijerph18010276
Chicago/Turabian StyleEl-Shitany, Nagla A., Manal El-Hamamsy, Ahlam A. Alahmadi, Basma G. Eid, Thikryat Neamatallah, Haifa S. Almukadi, Rana A. Arab, Khadija A. Faddladdeen, Khayria A. Al-Sulami, Safia M. Bahshwan, and et al. 2021. "The Impact of ABO Blood Grouping on COVID-19 Vulnerability and Seriousness: A Retrospective Cross-Sectional Controlled Study among the Arab Community" International Journal of Environmental Research and Public Health 18, no. 1: 276. https://doi.org/10.3390/ijerph18010276