


Mortality and Survival Factors in Patients with Moderate and Severe Pneumonia Due to COVID-19
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
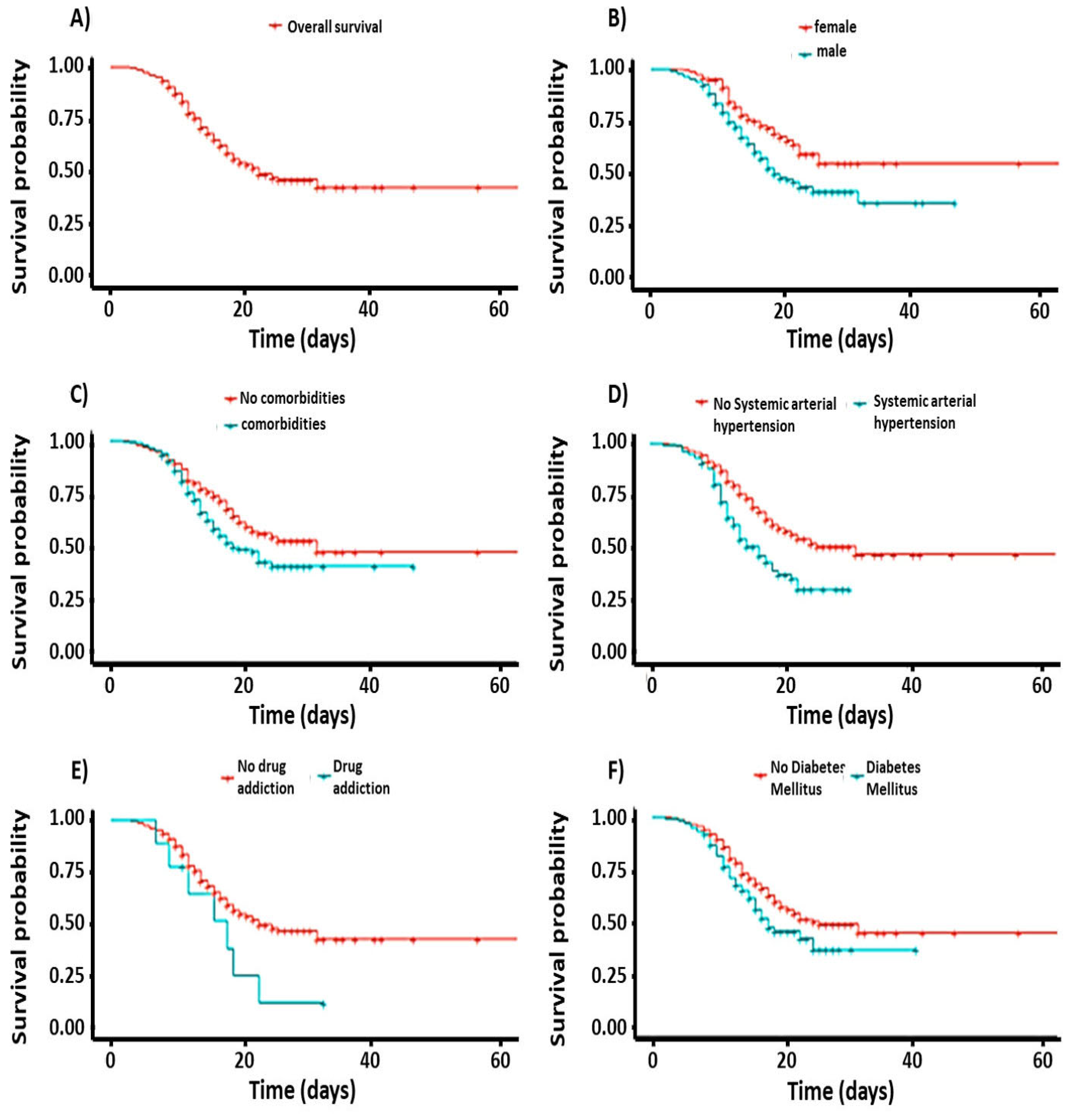
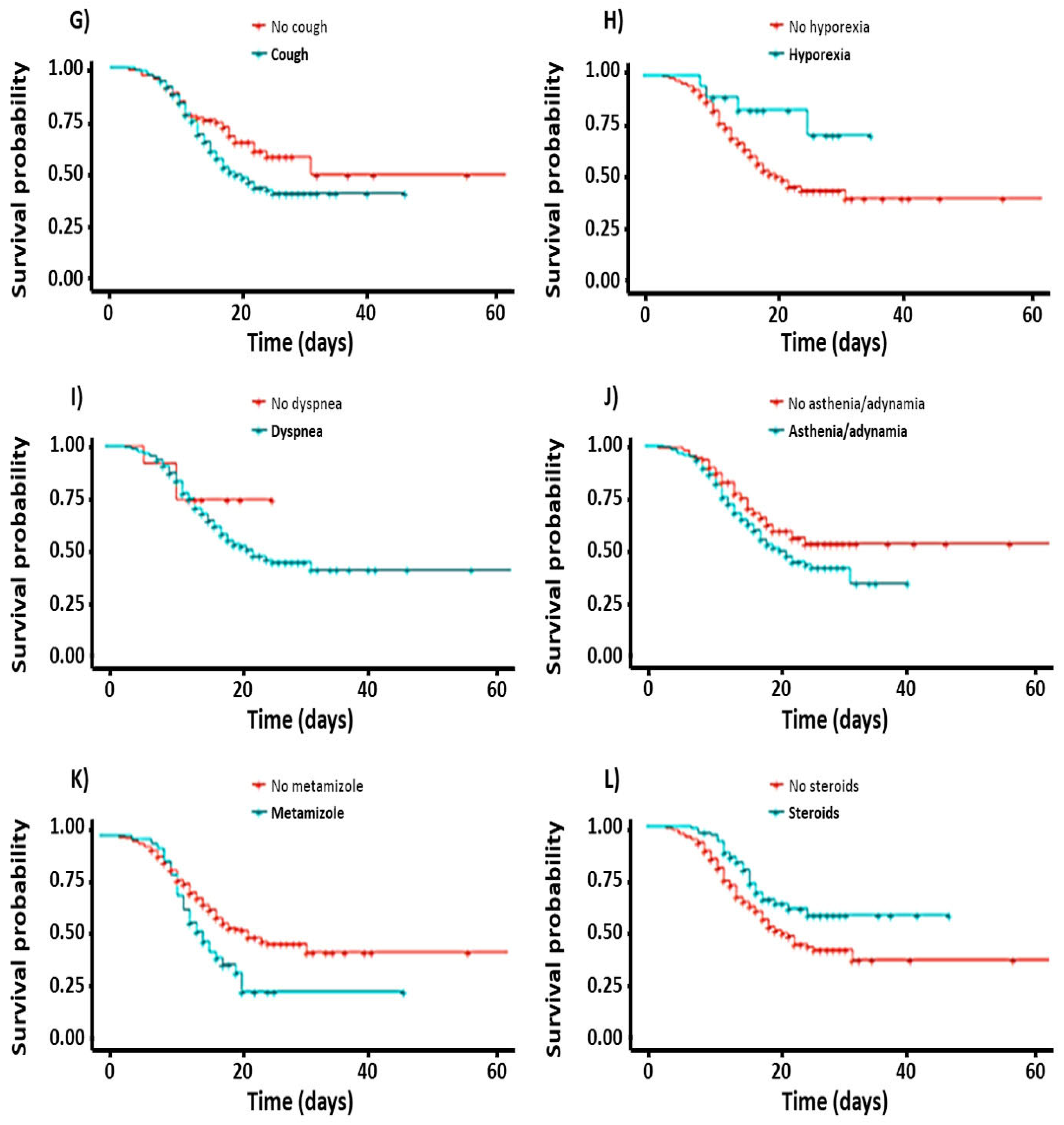
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mascolo, P.; Feola, A.; Sementa, C.; Leone, S.; Zangani, P.; Della-Pietra, B.; Campobasso, C. A Descriptive Study on Causes of Death in Hospitalized Patients in an Acute General Hospital of Southern Italy during the Lockdown due to COVID-19 Outbreak. Healthcare 2021, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/?mapFilter=cases (accessed on 23 December 2022).
- Informe Técnico Diario e Informe Semanal COVID-19 2022 | Secretaría de Salud | Gobierno | gob.mx. Available online: https://www.gob.mx/salud/documentos/informe-tecnico-diario-covid19-2022 (accessed on 23 December 2022).
- Allenbach, Y.; Saadoun, D.; Maalouf, G.; Vieira, M.; Hellio, A.; Boddaert, J.; Gros, H.; Salem, J.E.; Rigon, M.R.; Menyssa, C.; et al. Development of a multivariate prediction model of intensive care unit transfer or death: A French prospective cohort study of hospitalized COVID-19 patients. PLoS ONE 2020, 15, e0240711. [Google Scholar] [CrossRef] [PubMed]
- Both, L.; Botgros, R.; Cavaleri, M. Analysis of licensed over-the-counter (OTC) antibiotics in the European Union and Norway, 2012. Eurosurveillance 2015, 20, 30002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chon, Y.; Kim, J.Y.; Suh, Y.J.; Lee, J.Y.; Park, J.S.; Moon, S.M.; Lee, M.S.; Yi, J. Adverse initial CT findings associated with poor prognosis of coronavirus disease. J Korean Med. Sci. 2020, 35, e316. [Google Scholar] [CrossRef] [PubMed]
- Donamou, J.; Touré, A.; Camara, A.Y.; Camara, D.; Camara, M.L.; Traoré, A.D.; Bangoura, A.; Dramé, B.A.; Sossa, L.K.; Abékan, J.-M.R.; et al. Predictive factors of mortality in patients with COVID-19 in Guinea: Analysis of the first 140 cases admitted to the intensive care unit. Pan Afr. Med. J. 2021, 38, 205. [Google Scholar] [CrossRef]
- Torres, I.; Sacoto, F. Localising an asset-based COVID-19 response in Ecuador. Lancet 2020, 1339, 1339–1340. [Google Scholar] [CrossRef]
- Van Halem, K.; Bruyndonckx, R.; Van Der Hilst, J.; Cox, J.; Driesen, P.; Opsomer, M.; Van Steenkiste, E.; Stessel, B.; Dubois, J.; Messiaen, P. Risk factors for mortality in hospitalized patients with COVID-19 at the start of the pandemic in Belgium: A retrospective cohort study. BMC Infect. Dis. 2020, 20, 897. [Google Scholar] [CrossRef]
- Vena, A.; Giacobbe, D.R.; Di Biagio, A.; Mikulska, M.; Taramasso, L.; De Maria, A.; Ball, L.; Brunetti, I.; Loconte, M.; Patroniti, N.A.; et al. Clinical characteristics, management and in-hospital mortality of patients with coronavirus disease 2019 in Genoa, Italy. Clin. Microbiol. Infect. 2020, 26, 1537–1544. [Google Scholar] [CrossRef]
- Prediabetes: More Than Just a Risk Factor for Developing Diabetes—Federación Mexicana de Diabetes. Available online: https://fmdiabetes.org/prediabetes-mas-solo-factor-riesgo-desarrollar-diabetes (accessed on 14 February 2022).
- Statistics About the World Diabetes Day. National Data. Available online: https://www.paho.org/es/campanas/dia-mundial-diabetes-2020 (accessed on 14 February 2022).
- The Diabetes Pandemic in Mexico. Available online: https://www.ciad.mx/la-pandemia-de-la-diabetes-en-mexico/ (accessed on 20 November 2022).
- Bansal, M. Cardiovascular disease and COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 247–250. [Google Scholar] [CrossRef]
- Pérez-Martínez, P.; Sánchez, F.J.C.; Gómez, J.C.; Gómez-Huelgas, R. Solving one of the pieces of the puzzle: COVID-19 and type 2 diabetes. Rev. Clin. Esp. 2020, 220, 507–510. [Google Scholar] [CrossRef]
- Encuesta Nacional de Salud y Nutrición 2020 Sobre COVID-19 Resultados Nacionales. Available online: https://insp.mx/avisos/reporte-completo-resultados-nacionales (accessed on 29 June 2022).
- Encuesta Nacional de Salud y Nutrición 2018 Presentación de Resultados. Available online: https://www.inegi.org.mx/programas/ensanut/2018/default.html (accessed on 30 May 2022).
- Sulmont, A.; Martínez, C.; De Alva, M.G.; Correa, A.; Leal, V.; Mendoza, O. Development Challenges in the Face of COVID-19 in Mexico. Socio-Economic Overview UNDP Country Office Mexico 2020. Available online: https://www.undp.org/latin-america/publications/development-challenges-face-covid-19-mexico-socio-economic-overview (accessed on 20 October 2022).
- Fantin, R.; Brenes-Camacho, G.; Barboza-Solís, C. COVID-19 deaths: Distribution by age and universal medical coverage in 22 countries. Pan Am. J. Public Health 2021, 45, e42. [Google Scholar] [CrossRef]
- Población. Censos y Conteos Población y Vivienda. Available online: https://www.inegi.org.mx/temas/estructura (accessed on 22 November 2022).
- O’Driscoll, M.; Dos Santos, G.R.; Wang, L.; Cummings, D.A.T.; Azman, A.S.; Paireau, J.; Fontanet, A.; Cauchemez, S.; Salje, H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature 2021, 590, 140–145. [Google Scholar] [CrossRef]
- Lutz, M.; Arancibia, M.; Papuzinski, C.; Stojanova, J. Immunosenescence, viral infections and nutrition: A narrative review of scientific available evidence. Rev. Esp. Geriatr. Gerontol. 2022, 57, 33–38. [Google Scholar] [CrossRef]
- Saldivia, R.K.O.; Ojeda, S.; Ivanissevich, M.L. Aging and Respiratory Diseases in the Elderly. The case of a Rio Gallegos retirement center. Inf. Científicos Técnicos UNPA 2020, 12, 166–193. [Google Scholar] [CrossRef]
- Gadi, N.; Wu, S.C.; Spihlman, A.P.; Moulton, V.R. What’s Sex Got to Do with COVID-19? Gender-Based Differences in the Host Immune Response to Coronaviruses. Front. Immunol. 2020, 11, 2147. [Google Scholar] [CrossRef]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol Sex Differ. 2020, 11, 29. [Google Scholar] [CrossRef]
- Ueyama, H.; Kuno, T.; Takagi, H.; Krishnamoorthy, P.; Vengrenyuk, Y.; Sharma, S.K.; Kini, A.S.; Lerakis, S. Gender Difference Is Associated with Severity of Coronavirus Disease 2019 Infection: An Insight from a Meta-Analysis. Crit. Care Explor. 2020, 2, e0148. [Google Scholar] [CrossRef]
- Diferencias Por Razones de Sexo en Relación Con la Pandemia de COVID-19 en la Región de las Américas. Available online: https://www.paho.org/es/documentos/diferencias-por-razones-sexo-relacion-con-pandemia-covid-19-region-americas (accessed on 26 December 2022).
- Resultados de salud Desglosados Por Sexo en Relación Con la Pandemia de COVID-19 en la Región de las Américas. Available online: https://iris.paho.org/handle/10665.2/53603 (accessed on 21 November 2022).
- Cantero, M.T.R. Health statistics and invisibility by sex and gender during the COVID-19 epidemic. Gac. Sanit. 2021, 35, 95–98. [Google Scholar] [CrossRef]
- Mena, G.E.; Martinez, P.P.; Mahmud, A.S.; Marquet, P.A.; Buckee, C.O.; Santillana, M. Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile. Science 2021, 372, eabg5298. [Google Scholar] [CrossRef]
- Mortalidad por COVID-19 y Las Desigualdades por Nivel Socioeconómico y Por Territorio|Comisión Económica Para América Latina y el Caribe. Available online: https://www.cepal.org/es/enfoques/mortalidad-covid-19-desigualdades-nivel-socioeconomico-territorio (accessed on 2 November 2022).
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: A systematic review and meta-analysis of observational studies. Aging Male 2021, 23, 1416–1424. [Google Scholar] [CrossRef]
- Salazar, M.; Barochiner, J.; Espeche, W.; Ennis, I. COVID-19 and its relationship with hypertension and cardiovascular disease. Hipertens. Y Riesgo Vasc. 2020, 37, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Perrone, M.A.; Feola, A.; Pieri, M.; Donatucci, B.; Salimei, C.; Lombardo, M.; Perrone, A.; Parisi, A. The effects of reduced physical activity on the lipid profile in patients with high cardiovascular risk during COVID-19 lockdown. Int. J. Environ. Res. Public Health 2021, 18, 8858. [Google Scholar] [CrossRef] [PubMed]
- El Alcohol y la COVID-19: Lo Que Debe Saber. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov-technical-guidance/food- (accessed on 10 October 2022).
- Garcia-Cerde, R.; Valente, J.Y.; Sohi, I.; Falade, R.; Sanchez, Z.M.; Monteiro, M.G. Alcohol use during the COVID-19 pandemic in Latin America and the Caribbean. Rev. Panam. De Salud Pública 2021, 45, e52. [Google Scholar] [CrossRef] [PubMed]
- Consumo de Alcohol Durante COVID-19. Available online: https://www.paho.org/es/consumo-alcohol-durante-covid-19 (accessed on 26 November 2022).
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Reyes, A.S.; Valverde, C.A.V. Características y especialización de la respuesta inmunitaria en la COVID-19. Rev. Fac. Med. 2020, 63, 7–18. [Google Scholar] [CrossRef]
- Naretto, O.; Emilio, Á.; Patricia, P.M.; Angélica, S.M. Fisiopatología Pulmonar de la COVID-19. RAMR 2020, 20, 402–409. [Google Scholar]
- de León-Delgado, J.; Cruz, A.P.; Ramirez, P.A.; Valencia, Y.E.; Carrillo, C.Q.; Ayala, E.V. SARS-CoV-2 y sistema inmune: Una batalla de titanes. Horiz. Médico 2020, 20, e1209. [Google Scholar] [CrossRef]
- López-Pérez, T.G.; Lourdes, M.; Ramírez-Sandoval, P.; Torres-Altamirano, M.S.; Especial, A.; Tiburcio, G. Fisiopatología del Daño Multiorgánico en la Infección Por SARS-CoV-2. Available online: https://www.actapediatrica.org.mx (accessed on 25 October 2022).
- La FDA Aprueba el Primer Tratamiento Para el COVID-19|FDA. Available online: https://www.fda.gov/news-events/press-announcements/la-fda-aprueba-el-primer-tratamiento-para-el-covid-19 (accessed on 14 January 2022).
- Lineamiento Para la Atención de Pacientes Por COVID-19. Available online: http://cvoed.imss.gob.mx/lineamiento-para-la-atencion-de-pacientes-por-covid-19/ (accessed on 19 October 2022).
- Llover, M.N.; Jiménez, M.C. Estado Actual de Los Tratamientos Para la COVID-19. FMC 2021, 28, 40–56. [Google Scholar] [CrossRef]
- Uso no Indicado de Medicamentos Contra la COVID-19. Available online: https://www.who.int/es/news-room/commentaries/detail/off-label-use-of-medicines-for-covid-19 (accessed on 23 December 2022).
- Echeverría-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; Cuscó, M.D.-A.; Ferrández, O.; Horcajada, J.P.; Grau, S. Azithromycin in the treatment of COVID-19: A review. Expert Rev. Anti-Infect. Ther. 2021, 19, 147–163. [Google Scholar] [CrossRef]
- Guía Clínica Para el Tratamiento de la COVID-19 en México. Available online: https://www.gob.mx/cms/uploads/attachment/file/659911/GuiaTx_COVID19_Consenso_2021.08.02_compressed.pdf (accessed on 12 March 2022).
- Manejo Clínico de la COVID-19 Orientaciones Evolutivas. Available online: https://apps.who.int/iris/bitstream/handle/10665/338871/WHO-2019-nCoV-clinical-web_annex-2021.1-eng.pdf (accessed on 25 January 2022).
- Evidencias Sobre el Tratamiento Farmacológico. Available online: https://bancos.salud.gob.ar/sites/default/files/2021-06/COVID19_Evidencias_sobre_Tratamiento_Farmacologico.pdf (accessed on 14 September 2021).
- Ishaqui, A.A.; Khan, A.H.; Sulaiman, S.A.S.; Alsultan, M.T.; Khan, I.; Naqvi, A.A. Assessment of efficacy of Oseltamivir-Azithromycin combination therapy in prevention of Influenza-A (H1N1) pdm09 infection complications and rapidity of symptoms relief. Expert Rev. Respir. Med. 2020, 14, 533–541. [Google Scholar] [CrossRef] [Green Version]
- Kakeya, H.; Seki, M.; Izumikawa, K.; Kosai, K.; Morinaga, Y.; Kurihara, S.; Nakamura, S.; Imamura, Y.; Miyazaki, T.; Tsukamoto, M.; et al. Efficacy of combination therapy with oseltamivir phosphate and azithromycin for influenza: A multicenter, open-label, randomized study. PLoS ONE 2014, 9, e91293. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Alothman, A.; Balkhy, H.H.; Al-Dawood, A.; Aljohani, S.; Al Harbi, S.; Kojan, S.; Aljeraisy, M.; Deeb, A.M.; Assiri, A.M.; et al. Treatment of Middle East Respiratory Syndrome with a combination of lopinavir-ritonavir and interferon-β1b (MIRACLE trial): Study protocol for a randomized controlled trial. Trials 2018, 19, 81. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Krempaska, K.; Barnowski, S.; Gavini, J.; Hobi, N.; Ebener, S.; Simillion, C.; Stokes, A.; Schliep, R.; Knudsen, L.; Geiser, T.K.; et al. Azithromycin has enhanced effects on lung fibroblasts from idiopathic pulmonary fibrosis (IPF) patients compared to controls. Respir. Res. 2020, 21, 25. [Google Scholar] [CrossRef] [Green Version]
- Lee, N.; Wong, C.-K.; Chan, M.C.; Yeung, E.S.; Tam, W.W.; Tsang, O.T.; Choi, K.-W.; Chan, P.K.; Kwok, A.; Lui, G.C.; et al. Anti-inflammatory effects of adjunctive macrolide treatment in adults hospitalized with influenza: A randomized controlled trial. Antivir. Res. 2017, 144, 48–56. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; Bermejo-Martin, J.F.; Vallés, J.; Granada, R.; Vidaur, L.; Vergara-Serrano, J.C.; Martín, M.; Figueira, J.C.; Sirvent, J.M.; Blanquer, J.; et al. Macrolide-based regimens in absence of bacterial co-infection in critically ill H1N1 patients with primary viral pneumonia. Intensive Care Med. 2013, 39, 693–702. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Min, J.Y.; Jang, Y.J. Macrolide therapy in respiratory viral infections. Mediat. Inflamm. 2012, 2012, 649570. [Google Scholar] [CrossRef] [Green Version]
- Lerman, T.T.; Sagi, M.; Shafir, Y.; Sheena, L.; Cohen, E.; Goldberg, E.; Krause, I. A possible increased risk of metamizole-associated neutropenia among COVID-19 patients. Br. J. Clin. Pharmacol. 2021, 87, 2902–2906. [Google Scholar] [CrossRef]
- Ospina-Tascón, G.A.; Calderón-Tapia, L.E.; García, A.F.; Zarama, V.; Gómez-Álvarez, F.; Álvarez-Saa, T.; Pardo-Otálvaro, S.; Bautista-Rincón, D.F.; Vargas, M.P.; Aldana-Díaz, J.L.; et al. Effect of High-Flow Oxygen Therapy vs Conventional Oxygen Therapy on Invasive Mechanical Ventilation and Clinical Recovery in Patients with Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 326, 2161–2171. [Google Scholar] [CrossRef]
- Jiang, B.; Wei, H. Oxygen therapy strategies and techniques to treat hypoxia in COVID-19 patients. In European Review for Medical and Pharmacological. Sciences 2020, 24, 10239–10246. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Alive | Dead | OR | 95% CI | p-Value |
|---|---|---|---|---|---|
| Sex | |||||
| Female | 96 | 43 | 0.47 | 0.30–0.72 | p < 0.05 * |
| Male | 142 | 135 | |||
| Occupation | |||||
| Home | 47 | 24 | 0.51 | 0.30–0.82 | p < 0.05 * |
| Construction worker | 3 | 8 | 5.22 | 1.37–2.55 | p < 0.05 * |
| Unemployed | 4 | 6 | 2.93 | 0.76–1.24 | p = 0.06 |
| Carrier | 12 | 14 | 2.28 | 0.91–5.79 | p = 0.07 |
| Healthcare personnel | 15 | 2 | 0.26 | 0.03–1.02 | p = 0.09 |
| Comorbidities | |||||
| present | 93 | 92 | 1.66 | 1.12–2.47 | p < 0.05 * |
| absent | 145 | 86 | |||
| High blood pressure | |||||
| present | 42 | 57 | 2.19 | 1.39–3.49 | p < 0.05 * |
| absent | 196 | 121 | |||
| Alcoholism | |||||
| present | 49 | 49 | 1.58 | 1.00–2.51 | p < 0.05 * |
| absent | 192 | 192 | |||
| Drug addiction | |||||
| present | 2 | 7 | 4.83 | 1.15–32.68 | p = 0.05 |
| absent | 236 | 172 | |||
| Diabetes mellitus | |||||
| present | 50 | 49 | 1.42 | 0.90–2.24 | p = 0.12 |
| absent | 188 | 129 | |||
| Headache | |||||
| present | 143 | 108 | 0.9 | 0.83–0.96 | p < 0.05 * |
| absent | 95 | 70 | |||
| Arthralgias | |||||
| present | 168 | 115 | 0.91 | 0.85–0.97 | p < 0.05 * |
| absent | 70 | 63 | |||
| Myalgias | |||||
| present | 172 | 118 | 0.92 | 0.86–0.98 | p < 0.05 * |
| absent | 66 | 60 | |||
| Ageusia | |||||
| present | 25 | 10 | 0.87 | 0.81–0.93 | p < 0.05 * |
| absent | 213 | 168 | |||
| Dyspnea | |||||
| present | 229 | 175 | 0.93 | 0.87–1.00 | p = 0.06 |
| absent | 9 | 3 | |||
| Paracetamol | |||||
| present | 100 | 57 | 0.65 | 0.43–0.97 | p < 0.05 * |
| absent | 138 | 121 | |||
| Sodium metamizole | |||||
| present | 18 | 31 | 2.57 | 1.40–4.86 | p < 0.05 * |
| absent | 220 | 147 | |||
| Azithromycin | |||||
| present | 190 | 146 | 0.47 | 0.30–0.74 | p < 0.05 * |
| absent | 48 | 32 | |||
| Steroids | |||||
| present | 67 | 32 | 0.55 | 0.34–0.89 | p < 0.05 * |
| absent | 171 | 146 | |||
| Ceftriaxone | 65 | 41 | 0.63 | 0.42–0.92 | p < 0.05 * |
| Dexamethasone | 57 | 28 | 0.49 | 0.30–0.76 | p < 0.05 * |
| Enoxaparin | 17 | 8 | 0.47 | 0.19–1.05 | p = 0.07 |
| In-hospital oxygen therapy | |||||
| Nasal tips | 58 | 9 | 0.15 | 0.07–0.29 | p < 0.05 * |
| Reservoir mask | 161 | 165 | 6.6 | 3.32–1.46 | p < 0.05 * |
| Risk Factor | Mean | OR | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Alive | Deceased | ||||
| Age | 45.4 | 49.1 | 1.04 | 1.02–1.07 | p < 0.05 * |
| Total stay (days) | 9.56 | 4.6 | 0.75 | 0.69–0.79 | p < 0.05 * |
| Urgent care stay (days) | 0.7 | 0.8 | 2.32 | 1.27–4.43 | p < 0.05 * |
| In-hospital stay 1 (days) | 8.6 | 3.6 | 0.71 | 0.66–0.77 | p < 0.05 * |
| Days of evolution | 10.5 | 8.5 | 0.89 | 0.84–0.94 | p < 0.05 * |
| Duration of symptoms | |||||
| Headache | 9.1 | 7.5 | 0.9 | 0.83–0.96 | p < 0.05 * |
| Arthralgias | 9.5 | 8.1 | 0.91 | 0.85–0.97 | p < 0.05 * |
| Myalgias | 9.4 | 8.2 | 0.92 | 0.86–0.98 | p < 0.05 * |
| Dynamia and/or asthenia | 9.4 | 7.6 | 0.87 | 0.81–0.93 | p < 0.05 * |
| Dyspnea | 3.5 | 2.9 | 0.93 | 0.87–1.00 | p = 0.06 |
| Oseltamivir dosage | 129 | 220 | 1.02 | 1.01–1.06 | p < 0.05 * |
| Length of use | |||||
| Paracetamol | 6 | 4.8 | 0.85 | 0.72–0.99 | p = 0.05 * |
| Azithromycin | 2.9 | 4 | 0.74 | 0.55–0.96 | p < 0.05 * |
| In-hospital oxygen therapy duration | |||||
| Device 1 | 4.9 | 2.6 | 0.72 | 0.65–0.79 | p < 0.05 * |
| Device 2 | 3.42 | 2.17 | 0.91 | 0.84–0.98 | p < 0.05 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galindo-Oseguera, E.; Pinto-Almazán, R.; Arellano-Ramírez, A.; Gasca-López, G.A.; Ocharan-Hernández, M.E.; Calzada-Mendoza, C.C.; Castillo-Cruz, J.; Martínez-Herrera, E. Mortality and Survival Factors in Patients with Moderate and Severe Pneumonia Due to COVID-19. Healthcare 2023, 11, 932. https://doi.org/10.3390/healthcare11070932
Galindo-Oseguera E, Pinto-Almazán R, Arellano-Ramírez A, Gasca-López GA, Ocharan-Hernández ME, Calzada-Mendoza CC, Castillo-Cruz J, Martínez-Herrera E. Mortality and Survival Factors in Patients with Moderate and Severe Pneumonia Due to COVID-19. Healthcare. 2023; 11(7):932. https://doi.org/10.3390/healthcare11070932
Chicago/Turabian StyleGalindo-Oseguera, Evelyn, Rodolfo Pinto-Almazán, Alfredo Arellano-Ramírez, Gilberto Adrián Gasca-López, María Esther Ocharan-Hernández, Claudia C. Calzada-Mendoza, Juan Castillo-Cruz, and Erick Martínez-Herrera. 2023. "Mortality and Survival Factors in Patients with Moderate and Severe Pneumonia Due to COVID-19" Healthcare 11, no. 7: 932. https://doi.org/10.3390/healthcare11070932