
Gaming among Children and Adolescents during the COVID-19 Lockdown: The Role of Parents in Time Spent on Video Games and Gaming Disorder Symptoms


Abstract
:1. Introduction
2. Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Offspring’s Video Gaming Behavior
2.4. Parents’ Video Gaming Behavior
2.5. Parental Video Gaming Monitoring and Parental Knowledge of their Son/Daughter’s Life
2.6. Statistical Analyses
3. Results
3.1. Video Gaming Behavior
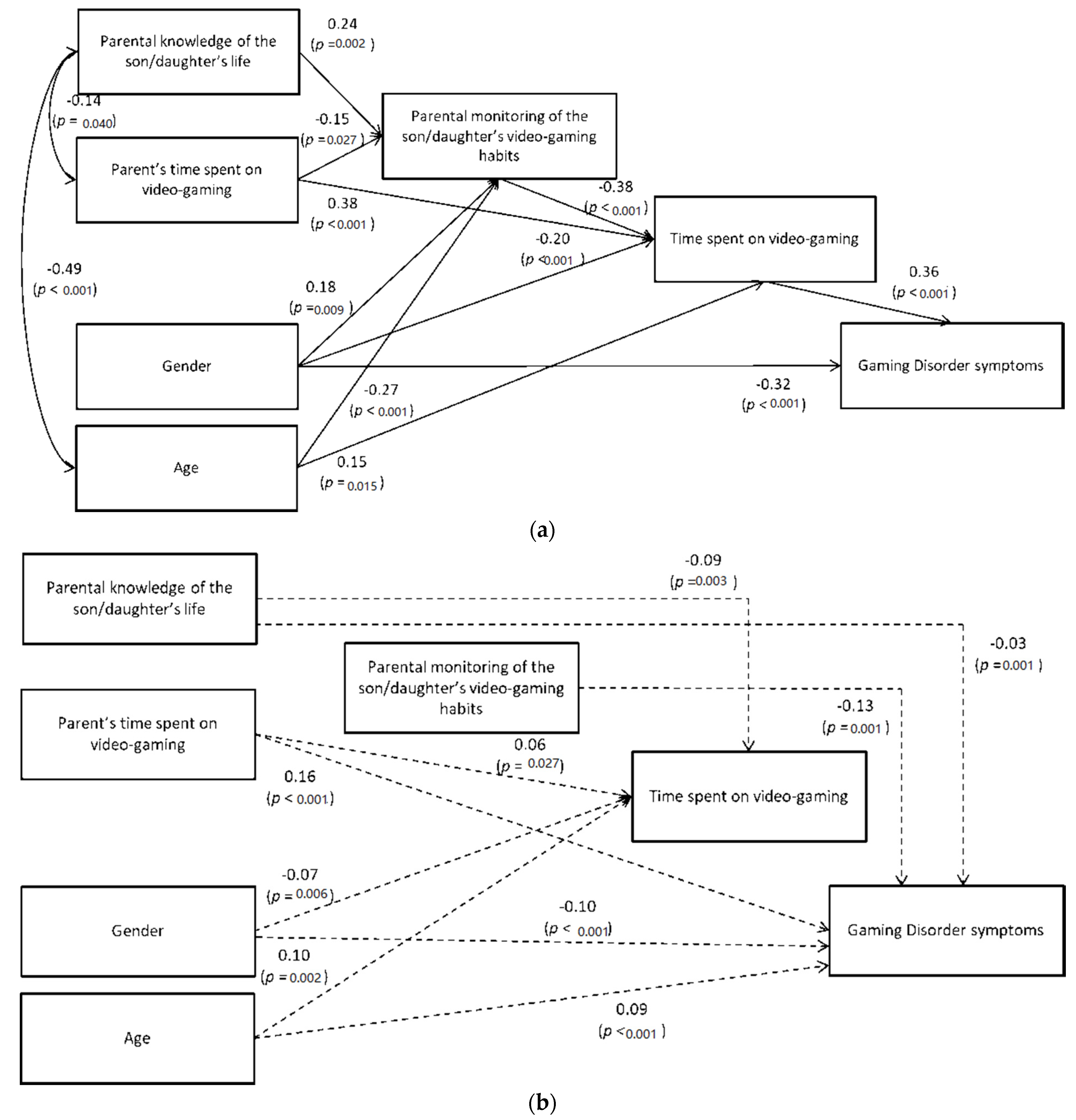
3.2. Explanatory Model of Video Gaming Behavior by Parental Influences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Statement
Appendix A
References
- Kefalis, C.; Kontostavlou, E.Z.; Drigas, A. The effects of video games in memory and attention. iJEP 2020, 10, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Entertainment Software Association; 2016 Annual Report. Available online: https://www.theesa.com/wp-content/uploads/2016/12/ESAAnnualReport2016.pdf (accessed on 31 March 2021).
- Mentzoni, R.A.; Brunborg, G.S.; Molde, H.; Myrseth, H.; Skouverøe, K.J.M.; Hetland, J.; Pallesen, S. Problematic video game use: Estimated prevalence and associations with mental and physical health. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Panagiotidi, M. Problematic video game play and ADHD traits in an adult population. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 292–295. [Google Scholar] [CrossRef] [Green Version]
- Donati, M.A.; Chiesi, F.; Ammannato, G.; Primi, C. Versatility and addiction in gaming: The number of video-game genres played is associated with pathological gaming in male adolescents. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, B.S.; Sherry, J.; Lachlan, K.; Lucas, K.; Holmstrom, A. Orientations to Video Games among Gender and Age Groups. Simul. Gaming 2010, 41, 238–259. [Google Scholar] [CrossRef] [Green Version]
- Gentile, D. Pathological video game use among youth ages 8 to 18: A national study. Psychol Sci. 2009, 20, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Kowert, R.; Domahidi, E.; Festl, R.; Quandt, T. Social gaming, lonely life? The impact of digital game play on adolescents’ social circles. Comput. Hum. Behav. 2014, 36, 385–390. [Google Scholar] [CrossRef]
- Müller, K.W.; Janikian, M.; Dreier, M.; Wölfling, K.; Beutel, M.E.; Tzavara, C.; Richardson, C.; Tsitsika, A. Regular gaming behavior and internet gaming disorder in European adolescents: Results from a cross-national representative survey of prevalence, predictors, and psychopathological correlates. Eur. Child. Adolesc. Psychiatry 2015, 24, 565–574. [Google Scholar] [CrossRef]
- Pontes, H.M.; Macur, M.; Griffiths, M.D. Internet Gaming Disorder among Slovenian primary schoolchildren: Findings from a nationally representative sample of adolescents. J. Behav. Addict. 2016, 5, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Rehbein, F.; Kliem, S.; Baier, D.; Mößle, T.; Petry, N.M. Prevalence of Internet Gaming Disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction 2015, 110, 842–851. [Google Scholar] [CrossRef]
- Donati, M.A.; Sanson, F.; Mazzarese, M.; Primi, C. Assessing video game habits and pathological behaviour in children through a new scale: Psychometric properties of the Video-Gaming Scale—For Children (VGS-C). Psychology 2019, 10, 2190–2208. [Google Scholar] [CrossRef] [Green Version]
- Gentile, D.A.; Choo, H.; Liau, A.; Sim, T.; Li, D.; Fung, D.; Khoo, A. pathological video game use among youths: A two-year longitudinal study. Pediatrics 2011, 127, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Hamlen, K.R. Children’s choices and strategies in video games. Comput. Hum. Behav. 2010, 27, 532–539. [Google Scholar] [CrossRef]
- Lui, D.; Szeto, G.; Jones, A. The pattern of electronic game use and related bodily discomfort in Hong Kong primary school children. Comput. Educ. 2011, 57, 1665–1674. [Google Scholar] [CrossRef]
- Nogueira, M.; Faria, H.; Vitorino, A.; Silva, F.G.; Neto, A.S. Addictive video game use: An emerging pediatric problem? Acta Med. Port. 2019, 32, 183–188. [Google Scholar] [CrossRef]
- Rideout, V.J.; Foehr, U.G.; Roberts, D.F. Generation M2: Media in the Lives of 8- to 18-Year-Olds, a Kaiser Family Foundation Study 2010. Kaiser Family Foundation. Available online: https://files.eric.ed.gov/fulltext/ED527859.pdf (accessed on 26 March 2021).
- Hastings, E.C.; Karas, T.L.; Winsler, A.; Way, E.; Madigan, A.; Tyler, S. Young children’s video/computer game use: Relations with school performance and behavior. Issues Ment. Health Nurs. 2009, 30, 638–649. [Google Scholar] [CrossRef] [Green Version]
- Kovess-Masfety, V.; Keyes, K.; Hamilton, A.; Hanson, G.; Bitfoi, A.; Golitz, D.; Koc, C.; Kuijpers, R.; Lesinskiene, S.; Mihova, Z.; et al. Is time spent playing video games associated with mental health, cognitive and social skills in young children? Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 349–357. [Google Scholar] [CrossRef] [Green Version]
- European School Survey Project on Alcohol and Other Drugs Group; ESPAD Report 2019. Results from the European School Survey Project on Alcohol and Other Drugs; Publication Office of the European Union: Luxembourg, 2019.
- Gómez-Gonzalvo, F.; Molina, P.; Devís-Devís, J. Which are the patterns of video game use in Spanish school adolescents? Gender as a key factor. Entertain. Comput. 2020, 34, 100366. [Google Scholar] [CrossRef]
- Homer, B.D.; Hayward, E.O.; Frye, J.; Plass, J.L. Gender and player characteristics in video game play of preadolescents. Comput. Hum. Behav. 2012, 28, 1782–1789. [Google Scholar] [CrossRef]
- Lobel, A.; Engels, R.C.; Stone, L.L.; Burk, W.J.; Granic, I. Video gaming and children’s psychosocial wellbeing: A longitudinal study. J. Youth Adolesc. 2017, 46, 884–897. [Google Scholar] [CrossRef] [Green Version]
- Fazeli, S.; Zeidi, I.M.; Lin, C.Y.; Namdar, P.; Griffiths, M.D.; Ahorsu, D.K.; Pakpour, A.H. Depression, anxiety, and stress mediate the associations between internet gaming disorder, insomnia, and quality of life during the COVID-19 outbreak. Addict. Behav. Rep. 2020, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nielsen. 3, 2, 1 Go! Video Gaming Is at an All-Time High during COVID-19. Available online: https://www.nielsen.com/us/en/insights/article/2020/3-2-1-go-video-gaming-is-at-an-all-time-high-during-covid-19/ (accessed on 31 March 2021).
- Flynn, B. Geography of the digital hearth. Inf. Commun. Soc. 2003, 6, 551–576. [Google Scholar] [CrossRef]
- King, D.L.; Delfabbro, P.H.; Billieux, J.; Potenza, M.N. Problematic online gaming and the COVID-19 pandemic. J. Behav. Addict. 2020, 2, 184–186. [Google Scholar] [CrossRef]
- Broughton, M. Europe Mobile Game Revenue Hits Record High; Riot Acquires Hypixel. The Gaming Economy. Available online: https://www.thegamingeconomy.com/2020/04/17/europe-mobile-game-revenue-hits-record-high-riot-acquires-hypixel/ (accessed on 29 March 2021).
- Shin, W.; Huh, J. Parental mediation of teenagers’ video game playing: Antecedents and consequences. New Media Soc. 2011, 13, 945–962. [Google Scholar] [CrossRef]
- Paulus, F.W.; Ohmann, S.; von Gontard, A.; Popow, C. Internet gaming disorder in children and adolescents: A systematic review. DMCN 2018, 60, 645–659. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Lee, S.Y.; Lee, H.K.; Potenza, M.N.; Lee, H. Factors associated with severity, incidence or persistence of internet gaming disorder in children and adolescents: A 2-year Longitudinal Study. Addiction 2021. [Google Scholar] [CrossRef]
- Lemmens, J.; Valkenburg, P.; Peter, J. Psychosocial causes and consequences of pathological gaming. Comput. Hum. Behav. 2011, 27, 144–152. [Google Scholar] [CrossRef]
- Fauth-Bühler, M.; Mann, K. Neurobiological Correlates of Internet Gaming Disorder: Similarities to Pathological Gambling. Addict. Behav. 2017, 64, 349–356. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; WHO: Geneva, Switzerland, 2020; Available online: https://icd.who.int/en (accessed on 19 June 2021).
- Rumpf, H.J.; Achab, S.; Billieux, J.; Bowden-Jones, H.; Carragher, N.; Demetrovics, Z.; Higuchi, S.; King, D.L.; Mann, K.; Potenza, M.; et al. Including Gaming Disorder in the ICD-11: The need to do so from a clinical and public health perspective. J Behav. Addict. 2018, 7, 556–561. [Google Scholar] [CrossRef]
- Rehbein, F.; Psych, G.; Kleimann, M.; Mediasci, G.; Mößle, T. Prevalence and risk factors of video game dependency in adolescence: Results of a German nationwide survey. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 269–277. [Google Scholar] [CrossRef]
- Brunborg, G.S.; Mentzoni, R.A.; Melkevik, O.R.; Torsheim, T.; Samdal, O.; Hetland, J.; Andreassen, C.S.; Palleson, S. Gaming addiction, gaming engagement, and psychological health complaints among Norwegian adolescents. Media Psychol. 2013, 16, 115–128. [Google Scholar] [CrossRef]
- Pápay, O.; Urbán, R.; Griffiths, M.D.; Nagygyörgy, K.; Farkas, J.; Kökönyei, G.; Felvinczi, K.; Oláh, A.; Elekes, Z.; Demetrovics, Z. Psychometric properties of the Problematic Online Gaming Questionnaire Short-Form and prevalence of problematic online gaming in a national sample of adolescents. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Haagsma, M.C.; Marcel, E.P.; Oscar, P. The Prevalence of Problematic Video Gamers in The Netherlands. Cyberpsychol. Behav. Soc. Netw. 2012, 15, 62–68. [Google Scholar] [CrossRef]
- Bonnaire, C.; Phan, O. Relationships between parental attitudes, family functioning and Internet gaming disorder in adolescents attending school. Psychiatry Res. 2017, 255, 104–110. [Google Scholar] [CrossRef]
- Chiu, S.I.; Lee, J.Z.; Huang, D.H. Video game addiction in children and teenagers in Taiwan. Cyberpsychol. Behav. 2004, 7, 571–581. [Google Scholar] [CrossRef]
- Guido, C.A.; Amedeo, I.; Avenoso, F.; Bruni, J.; Zicari, A.M.; Loffredo, L.; Spalice, A. Risk factors and mental health promotion strategies in children during COVID-19. Front. Public Health 2020. [Google Scholar] [CrossRef]
- Ko, C.H.; Yen, J.Y. Impact of COVID-19 on gaming disorder: Monitoring and prevention. J. Behav. Addict. 2020, 9, 187–189. [Google Scholar] [CrossRef]
- Hoenig, K.; Wenz, S. Education, health behavior, and working conditions during the pandemic: Evidence from a German sample. Eur. Soc. 2020, 23, S275–S288. [Google Scholar] [CrossRef]
- Teng, Z.; Pontes, H.M.; Nie, Q.; Griffiths, M.D.; Guo, C. Depression and anxiety symptoms associated with internet gaming disorder before and during the COVID-19 pandemic: A longitudinal study. J. Behav. Addict. 2021, 10, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Paschke, K.; Austermann, M.I.; Simon-Kutscher, K.; Thomasius, R. Adolescent gaming and social media usage before and during the COVID-19 pandemic. Sucht 2021, 67. [Google Scholar] [CrossRef]
- Zhu, S.; Zhuang, Y.; Lee, P.; Li, J.C.M.; Wong, P.W. Leisure and Problem Gaming Behaviors Among Children and Adolescents During School Closures Caused by COVID-19 in Hong Kong: Quantitative Cross-sectional Survey Study. JMIR Serious Games 2021, 9, e26808. Available online: https://preprints.jmir.org/preprint/26808 (accessed on 13 June 2021). [CrossRef]
- De Pasquale, C.; Chiappedi, M.; Sciacca, F.; Martinelli, V.; Hichy, Z. Online videogames use and anxiety in children during the COVID-19 pandemic. Children 2021, 8, 205. [Google Scholar] [CrossRef]
- Choo, H.; Sim, T.T.; Liau, A.K.F.; Gentile, D.A.; Khoo, A. Parental influences on pathological symptoms of video-gaming among children and adolescents: A prospective study. J. Child. Fam. Stud. 2015, 24, 1429–1441. [Google Scholar] [CrossRef]
- Kwon, J.H.; Chung, C.S.; Lee, J. The effects of escape from self and interpersonal relationship on the pathological use of internet games. Community Ment. Health J. 2011, 47, 113–121. [Google Scholar] [CrossRef]
- Punamäki, R.L.; Wallenius, M.; Hölttö, H.; Nygård, C.H.; Rimpelä, A. The associations between information and communication technology (ICT) and peer and parent relations in early adolescence. Int. J. Behav. Dev. 2009, 33, 556–564. [Google Scholar] [CrossRef]
- Abelman, R. Fighting the war on indecency: Mediating TV, internet, and videogame usage among achieving and underachieving gifted children. Roeper Rev. 2006, 29, 100–112. [Google Scholar] [CrossRef]
- Vaala, S.E.; Bleakley, A. Monitoring, mediating, and modeling: Parental influence on adolescent computer and internet use in the United States. J. Child Media 2015, 9, 40–57. [Google Scholar] [CrossRef]
- Ramirez, E.R.; Norman, G.J.; Rosenberg, D.R.J.; Kerr, J.; Saelens, B.E.; Durant, N.; Sallis, J.F. Adolescent screen time and rules to limit screen time in the home. J. Adolesc. Health 2011, 48, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Darlington, G.; Ma, D.W.L.; Haines, J. Mothers’ and fathers’ media parenting practices associated with young children’s screen-time: A cross-sectional study. BMC Obes. 2018, 5, 37. [Google Scholar] [CrossRef] [Green Version]
- Nikken, P.; Jansz, J. Parental mediation of children’s videogame playing: A comparison of the reports by parents and children. Learn Media Technol. 2006, 31, 181–202. [Google Scholar] [CrossRef]
- Pelizzoni, I.; Cavallini, F.; Learn, T.; Fonticoli, V.; Cavallini, M.C. The role of parents and the use of videogames: A Systematic Review. Media Educ. Studi Ric. Buone Prat. 2019, 10, 212–231. [Google Scholar]
- Gentile, D.A.; Reimer, R.A.; Amy, I.; Nathanson, A.I.; Walsh, D.A.; Joey, C.; Eisenmann, J.C. Protective effects of parental monitoring of children’s media use. JAMA Pediatrics 2014, 168, 479–484. [Google Scholar] [CrossRef]
- Vondráčková, P.; Gabrhelík, R. Prevention of internet addiction: A Systematic Review. J. Behav. Addict. 2016, 5, 568–579. [Google Scholar] [CrossRef] [Green Version]
- Primi, C.; Donati, M.A.; Chiesi, F. Video-Gaming Scale for Adolescents, VGS-A. In Scala per la Misura dell’Uso dei Videogiochi negli Adolescenti [Video-Gaming Scale for Adolescents, VGS-A. A Scale to Assess Video-Gaming among Adolescents]; Hogrefe Editore: Florence, Italy, 2017. [Google Scholar]
- Lemmens, J.S.; Patti, M.; Valkenburg, P.M.; Peter, J. Development and validation of a game addiction scale for adolescents. Media Psychol. 2009, 12, 77–95. [Google Scholar] [CrossRef]
- Stattin, H.; Kerr, M. Parental monitoring: A reinterpretation. Child. Dev. 2000, 71, 1072–1085. [Google Scholar] [CrossRef]
- Miranda, M.C.; Bacchini, D.; Affuso, G. Validazione di uno strumento per la misura del parental monitoring in un campione di adolescenti italiani [Validation of a scale for measuring parental monitoring in a sample of Italian adolescents]. G. Psicol. Svilupp. 2012, 101, 32–47. [Google Scholar]
- Arbuckle, J.L. AMOS 16.0 (Computer Software); IBM SPSS: Chicago, IL, USA, 2007. [Google Scholar]
- Cheung, G.W.; Lau, R.S. Testing mediation and suppression effects of latent variables: Bootstrapping with structural equation models. Organ Res. Methods 2008, 11, 296–325. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [Green Version]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Steiger, J.H.; Lind, J.C. Statistically Based Tests for the Number of Common Factors. In Proceedings of the Annual Meeting of the Psychometric Society, Iowa City, IA, USA, 28 May 1980; Volume 758, pp. 424–453. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Psychol. Methods 2013, 8, 23–74. [Google Scholar]
- Pujol, J.; Fenoll, R.; Forns, J.; Harrison, B.J.; Martínez-Vilavella, G.; Macià, D.; Alvarez-Pedrerol, M.; Blanco-Hinojo, L.; González-Ortiz, S.; Deus, J.; et al. Video gaming in school children: How much is enough? Annals Neuroogyl. 2016, 80, 424–433. [Google Scholar] [CrossRef]
- Fumero, A.; Marrero, R.J.; Bethencourt, J.M.; Peñate, W. Risk factors of internet gaming disorder symptoms in Spanish adolescents. Comput. Hum. Behav. 2020, 111, 106416. [Google Scholar] [CrossRef]
- Milani, L.; La Torre, G.; Fiore, M.; Grumi, S.; Gentile, D.A.; Ferrante, M.; Miccoli, S.; Di Blasio, P. Internet gaming addiction in adolescence: Risk factors and maladjustment correlates. Int. J. Ment. Health Addict. 2018, 16, 888–904. [Google Scholar] [CrossRef]
- Thomas, N.J.; Martin, F.H. Video-arcade game, computer game and Internet activities of Australian students: Participation habits and prevalence of addiction. Aust. J. Psychol. 2010, 62, 59–66. [Google Scholar] [CrossRef]
- Su, B.; Chengfu, Y.; Zhang, W.; Su, Q.; Zhu, J.; Jiang, Y. Father–child longitudinal relationship: Parental monitoring and internet gaming disorder in Chinese adolescents. Front. Psychol. 2018, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Pisarska, A.; Ostaszewski, K. Factors associated with youth gambling: Longitudinal study among high school students. Public Health 2020, 184, 33–40. [Google Scholar] [CrossRef]
- Kaynak, O.; Meyers, K.; Caldeira, K.M.; Vincent, K.B.; Winters, K.C.; Arria, A.M. Relationships among parental monitoring and sensation seeking on the development of substance use disorder among college students. Addict. Behav. 2013, 38, 1457–1463. [Google Scholar] [CrossRef] [Green Version]
- MacPherson, H.A.; Wolff, J.; Nestor, B.; Frazier, E.; Massing-Schaffer, M.; Graves, H.; Esposito-Smythers, C.; Spirito, A. Parental monitoring predicts depressive symptom and suicidal ideation outcomes in adolescents being treated for co-occurring substance use and psychiatric disorders. J. Affect. Disord. 2021, 284, 190–198. [Google Scholar] [CrossRef]
- Kutner, L.A.; Olson, C.K.; Warner, D.E.; Hertzog, S.M. Parents’ and sons’ perspectives on video game play. J. Adolesc. Res. 2008, 23, 76–96. [Google Scholar] [CrossRef]
- Deleuze, J.; Long, J.; Liu, T.Q.; Maurage, P.; Billieux, J. Passion or addiction? Correlates of healthy versus problematic use of videogames in a sample of French-speaking regular players. Addict. Behav. 2018, 82, 114–121. [Google Scholar] [CrossRef]
- González, C.S.; Gómez, N.; Navarro, V.; Cairós, M.; Quirce, C.; Toledo, P.; Marrero-Gordillo, N. Learning healthy lifestyles through active videogames, motor games and the gamification of educational activities. Comput. Hum. Behav. 2016, 55, 529–551. [Google Scholar] [CrossRef]
- Vernadakis, N.; Kouli, O.; Tsitskari, E.; Gioftsidou, A.; Antoniou, P. University students’ ability-expectancy beliefs and subjective task values for exergames. CompuT. Educ. 2014, 75, 149–161. [Google Scholar] [CrossRef]
- Gentile, D.A.; Nathanson, A.I.; Rasmussen, E.E.; Reimer, R.A.; Walsh, D.A. Do you see what I see? Parent and child reports of parental monitoring of media. Fam. Relat. 2012, 61, 470–487. [Google Scholar] [CrossRef]
- De Los Reyes, A.; Augenstein, T.M.; Wang, M.; Thomas, S.A.; Drabick, D.A.G.; Burgers, D.E.; Rabinowitz, J. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol. Bull. 2015, 14, 858–900. [Google Scholar] [CrossRef]
- Gizer, I.R.; Waldman, I.D.; Abramowitz, A.; Barr, C.L.; Feng, Y.; Wigg, K.G.; Misener, V.L.; Rowe, D.C. Relations between multi-informant assessments of ADHD symptoms, DAT1, and DRD4. J. Abnorm. Psychol. 2008, 117, 869–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, E.K.; Gullone, E. Reciprocal relationships between parent and adolescent internalizing symptoms. J. Fam. Psychol. 2010, 24, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Hunsley, J.; Mash, E.J. Evidence-Based assessment. Annu. Rev. Clin. Psychol. 2007, 3, 29–51. [Google Scholar] [CrossRef] [PubMed]
- Izzo, V.A.; Donati, M.A.; Primi, C. Assessing ADHD Through the Multi-Informant Approach: The Contribution of the Conners’ 3 Scales. J. Atten. Disord. 2019, 23, 641–650. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Male Children | Female Children | |||
|---|---|---|---|---|
| Prevalence of video gamers | 94% | 79% | ||
| Prevalence of online video gamers | 61% | 39% | ||
| Time spent on VGs (hours per week) | M | SD | M | SD |
| 13.70 | 9.90 | 7.93 | 7.85 | |
| Prevalence of video gamers by video game genre (only the video game genres with the highest prevalence rates are reported.) | First-person shooter games (39%) | Simulation games (15%) | ||
| Sports games (15%) | Sandbox games (15%) | |||
| Sandbox games (13%) | Fitness games (8%) | |||
| Prevalence of video gamers by device used to play VGs | Home video game console (63%) | Smartphone (61%) | ||
| Smartphone (63%) | Tablet (60%) | |||
| Tablet (53%) | Home video game console (32%) | |||
| Handheld game console (34%) | Handheld game console (18%) | |||
| Computer (24%) | Computer (16%) | |||
| Number of devices used to play VGs Prevalence of video gamers by time of the day | M | SD | M | SD |
| 2.36 | 1.04 | 1.86 | 1.86 | |
| In the afternoon (74%) Before dinner (47%) | In the afternoon (71%) Before dinner (60%) | |||
| Before dinner (47%) In the morning (38%) | After lunch (46%) In the morning (33%) | |||
| After lunch (36%) | After waking up (9%) | |||
| After waking up (6%) | Before falling asleep (7%) | |||
| Before falling asleep (3%) | Before falling asleep (3%) | |||
| At lunch (1%) | At dinner (3%) | |||
| At dinner (1%) | At lunch (1%) | |||
| Number of daily moments spent on video games | M | SD | M | SD |
| 2.29 | 1.14 | 2.06 | 1.02 | |
| Prevalence of video gamers by social partner | Alone (89%) | Alone (85%) | ||
| Online friends (60%) | Parents (64%) | |||
| Parents (53%) | Brothers/sisters (34%) | |||
| Brothers/sisters (51%) | Online friends (22%) | |||
| VGS-P score | M | SD | M | SD |
| 7.90 | 4.83 | 3.98 | 3.80 | |
| Prevalence of video gamers by GD category | Non-problem gaming: 34% | Non-problem gaming: 79% | ||
| At-risk gaming: 44% | At-risk gaming: 13% | |||
| Problem gaming: 22% | Problem gaming: 8% | |||
| Male Adolescents | Female Adolescents | |||
|---|---|---|---|---|
| Prevalence of video gamers | 100% | 73% | ||
| Prevalence of online video gamers | 88% | 50% | ||
| Time spent on VGs (hours per week) | M | SD | M | SD |
| 19.11 | 13.16 | 10.99 | 10.62 | |
| Prevalence of video gamers by video game genre (only the video game genres with the highest prevalence rates are reported.) | Management games (41%) | Simulation games (24%) | ||
| Sports games (28%) | Puzzle games (18%) | |||
| Sandbox games (6%) | Sports games (11%) | |||
| Prevalence of video gamers by time of the day | Home video game console (88%) | Smartphone (86%) | ||
| Smartphone (78%) | Home video game console (45%) | |||
| Computer (33%) | Tablet (38%) | |||
| Tablet (31%) | Computer (36%) | |||
| Handheld game console (22%) | Handheld game console (21%) | |||
| Number of devices used for playing video games Prevalence of video gamers by time of the day | M | SD | M | SD |
| 2.52 | 0.96 | 2.26 | 1.06 | |
| In the afternoon (73%) Before dinner (62%) After lunch (62%) In the morning (29%) | In the afternoon (64%) Before dinner (56%) After lunch (54%) In the morning (18%) | |||
| Before falling asleep (22%) After waking up (9%) | After waking up (13%) Before falling asleep (13%) | |||
| At dinner (5%) At lunch (2%) | At lunch (3%) At dinner (-) | |||
| Number of daily moments spent on video games | M | SD | M | SD |
| 2.64 | 1.40 | 2.20 | 1.10 | |
| Prevalence of video gamers by social partner | Online friends (87%) | Alone (95%) | ||
| Alone (78%) | Brothers/sisters (46%) | |||
| Brothers/sisters (48%) | Online friends (41%) | |||
| Parents (27%) | Parents (32%) | |||
| VGS-P score | M | SD | M | SD |
| 7.90 | 4.83 | 3.98 | 3.80 | |
| Prevalence of video gamers by GD category | Non-problem gaming: 36% | Non-problem gaming: 72% | ||
| At-risk gaming: 40% | At-risk gaming: 16% | |||
| Problem gaming: 24% | Problem gaming: 12% | |||
| Variables | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|---|
| - | |||||||
| −0.07 | - | ||||||
| 0.07 | −0.03 | - | |||||
| 0.04 | −0.37 *** | 0.02 | - | ||||
| −0.07 | 0.03 | 0.09 | −0.19 * | - | |||
| 0.14 ** | −0.41 *** | 0.04 | 0.39 *** | −0.20 ** | - | ||
| −0.26 *** | 0.25 *** | 0.07 | −0.33 *** | 0.49 *** | −0.53 *** | - | |
| −0.33 *** | 0.05 | 0.03 | −0.23 ** | 0.27 *** | −0.22 *** | 0.43 *** | - |
| M | - | 11.11 | - | 17.67 | 7.56 | 19.24 | 14.81 | 7.00 |
| SD | - | 3.37 | - | 3.44 | 8.48 | 3.47 | 11.76 | 4.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donati, M.A.; Guido, C.A.; De Meo, G.; Spalice, A.; Sanson, F.; Beccari, C.; Primi, C. Gaming among Children and Adolescents during the COVID-19 Lockdown: The Role of Parents in Time Spent on Video Games and Gaming Disorder Symptoms. Int. J. Environ. Res. Public Health 2021, 18, 6642. https://doi.org/10.3390/ijerph18126642
Donati MA, Guido CA, De Meo G, Spalice A, Sanson F, Beccari C, Primi C. Gaming among Children and Adolescents during the COVID-19 Lockdown: The Role of Parents in Time Spent on Video Games and Gaming Disorder Symptoms. International Journal of Environmental Research and Public Health. 2021; 18(12):6642. https://doi.org/10.3390/ijerph18126642
Chicago/Turabian StyleDonati, Maria Anna, Cristiana Alessia Guido, Giuliano De Meo, Alberto Spalice, Francesco Sanson, Carola Beccari, and Caterina Primi. 2021. "Gaming among Children and Adolescents during the COVID-19 Lockdown: The Role of Parents in Time Spent on Video Games and Gaming Disorder Symptoms" International Journal of Environmental Research and Public Health 18, no. 12: 6642. https://doi.org/10.3390/ijerph18126642