
Effect of Mindfulness-Based Stress Reduction on the Well-Being, Burnout and Stress of Italian Healthcare Professionals during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
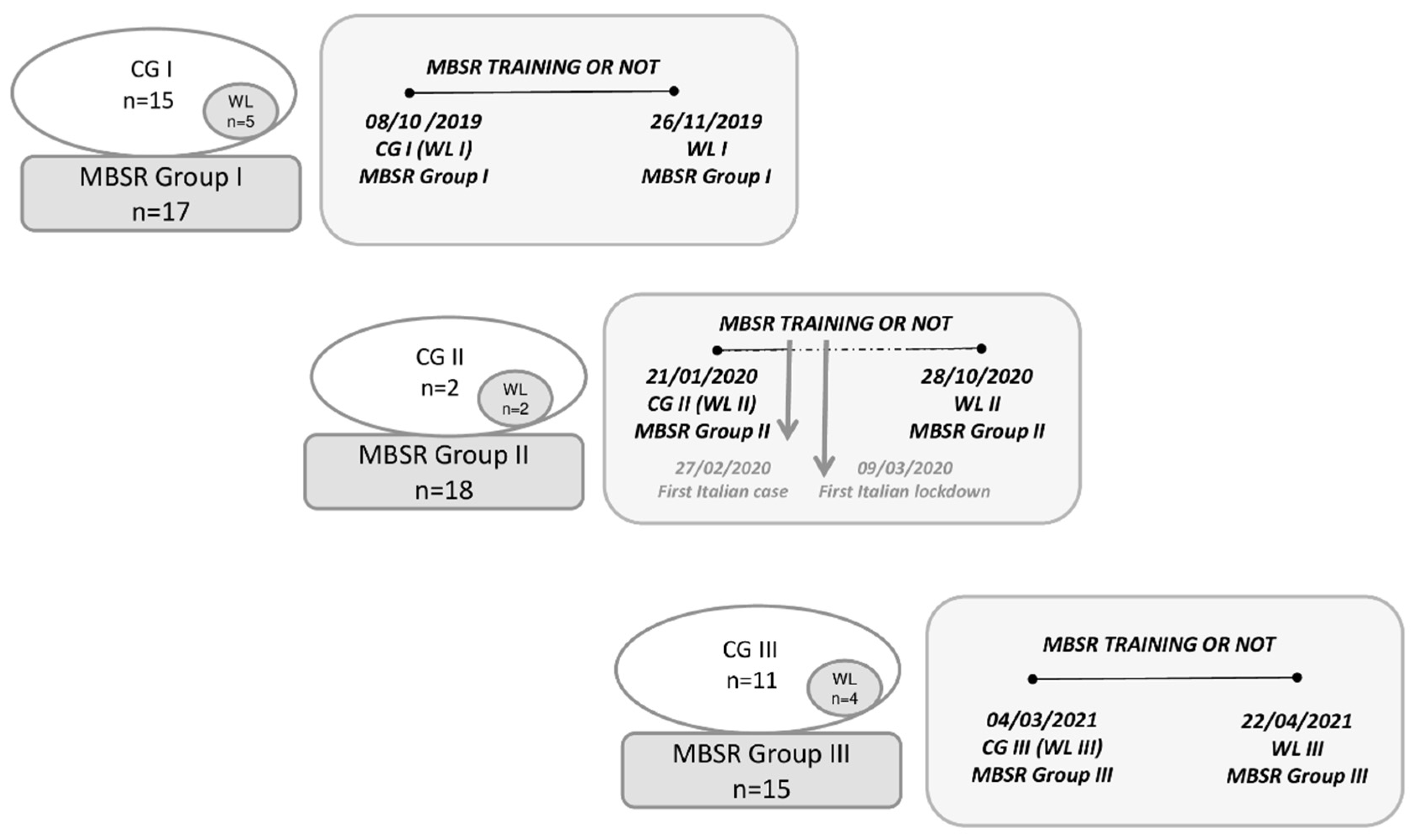
2.1. Study Sample and Procedures
2.2. Mindfulness-Based Stress Reduction Course
- -
- focus on the breath;
- -
- meditation on an object of interest for the person, focusing on its shape, size, color and smell;
- -
- mindful eating, focusing on a food, involving all the senses: smell, taste, touch, sight, and even sound;
- -
- attention paid to the sensations while walking on and when the feet touch the floor;
- -
- training in formal mindfulness meditation techniques involving simple stretches and postures (Mindfulness Yoga) and “Bodyscan” (a meditative practice increasing body awareness and sensations in a gradual mental scan from the feet to the head).
2.3. Assessments/Questionnaires
- -
- EE categorized into 0–18 (low), 19–26 (moderate), ≥27 (high);
- -
- DP divided into 0–5 (low), 6–9 (moderate), ≥10 (high);
- -
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
- -
- control group I (CG I) = 15 subjects, mean age 42.1 ± 9.9, 12 women, 8 nurses, 5 physicians, 2 allied care professionals;
- -
- control group II (CG II) = 2 subjects, mean age 42.2 ± 4.1, 1 woman, 1 nurse, 1 physician;
- -
- control group III (CG III) = 11 subjects, mean age 39.2 ± 15.1, 10 women, 7 nurses, 2 physicians, 2 allied care professionals.
3.2. Psychological General Well-Being Index
3.2.1. Baseline Characteristics and Differences between Groups at Baseline
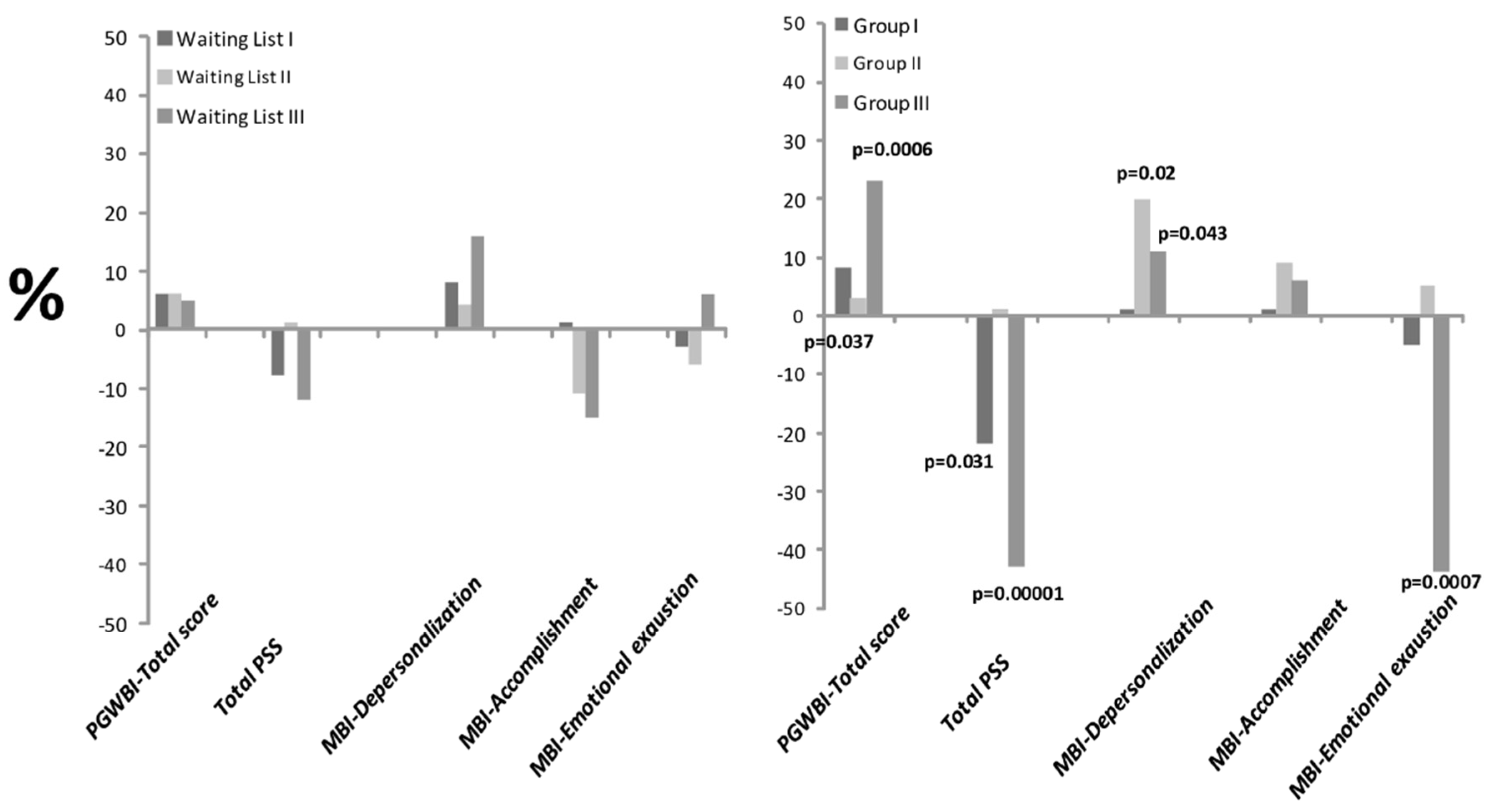
3.2.2. MBSR Effects on Psychological General Well-Being Index
3.3. Perceived Stress Scale
3.3.1. Baseline Characteristics and Differences between Groups at Baseline
3.3.2. MBSR Effects on Perceived Stress Scale
3.4. Maslach Burnout Inventory
3.4.1. Baseline Characteristics and Differences between Groups at Baseline
3.4.2. MBSR Effects on Maslach Burnout Inventory
3.5. Fear of COVID-19 in Group III
3.5.1. Baseline Characteristics and Differences between Groups at Baseline
3.5.2. MBSR Effects on “Fear of COVID-19”
4. Discussion
- In the baseline measures (T0), there was no statistical difference between the experimental and control groups, with all HCP groups exhibiting moderate stress;
- Wellbeing (total PGWBI) decreased with aging. Moreover, FCV-19S positively correlated with age in HCPs;
- MBSR was able to lower distress levels, except for increasing DP, while EE decreased in the MBSR groups trained after the pandemic onset (Group III);
- HCPs had fear of COVID-19 (FCV-19S), but levels significantly decreased after MSRB training.
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DP | Depersonalization |
| EE | Emotional exhaustion |
| FCV-19S | Fear of COVID-19 Scale |
| HCP | Healthcare professional |
| MBI | Maslach Burnout Inventory |
| MBSR | Mindfulness-Based Stress Reduction |
| PA | Personal or professional accomplishment |
| PGWBI | Psychological General Well-Being Index |
| PS | Perceived Stress |
| PSS | Perceived Stress Scale |
| WL | Waiting list |
References
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef] [PubMed]
- Di Tella, M.; Romeo, A.; Benfante, A.; Castelli, L. Mental health of healthcare workers during the COVID-19 pandemic in Italy. J. Eval. Clin. Pract. 2020, 26, 1583–1587. [Google Scholar] [CrossRef] [PubMed]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiol Psychiatr. Sci. 2020, 30, e1. [Google Scholar] [CrossRef]
- Fournier, A.; Laurent, A.; Lheureux, F.; Ribeiro-Marthoud, M.A.; Ecarnot, F.; Binquet, C.; Quenot, J.P. Impact of the COVID-19 pandemic on the mental health of professionals in 77 hospitals in France. PLoS ONE 2022, 17, e0263666. [Google Scholar] [CrossRef]
- Hummel, S.; Oetjen, N.; Du, J.; Posenato, E.; Resende de Almeida, R.M.; Losada, R.; Ribeiro, O.; Frisardi, V.; Hopper, L.; Rashid, A.; et al. Mental Health Among Medical Professionals During the COVID-19 Pandemic in Eight European Countries: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e24983. [Google Scholar] [CrossRef]
- Botha, E.; Gwin, T.; Purpora, C. The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: A systematic review of quantitative evidence protocol. JBI Database Syst. Rev. Implement Rep. 2015, 13, 21–29. [Google Scholar] [CrossRef]
- Dharmawardene, M.; Givens, J.; Wachholtz, A.; Makowski, S.; Tjia, J. A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support Palliat. Care. 2016, 6, 160–169. [Google Scholar] [CrossRef] [Green Version]
- McConville, J.; McAleer, R.; Hahne, A. Mindfulness Training for Health Profession Students-The Effect of Mindfulness Training on Psychological Well-Being, Learning and Clinical Performance of Health Professional Students: A Systematic Review of Randomized and Non-randomized Controlled Trials. Explore 2017, 13, 26–45. [Google Scholar] [CrossRef]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A systematic review of the impact of mindfulness on the well-being of healthcare professionals. J. Clin. Psychol. 2018, 74, 319–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinelli, C.; Wisener, M.; Khoury, B. Mindfulness training for healthcare professionals and trainees: A meta-analysis of randomized controlled trials. J. Psychosom. Res. 2019, 20, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Vega, B.; Palao, Á.; Muñoz-Sanjose, A.; Torrijos, M.; Aguirre, P.; Fernández, A.; Amador, B.; Rocamora, C.; Blanco, L.; Marti-Esquitino, J.; et al. Implementation of a Mindfulness-Based Crisis Intervention for Frontline Healthcare Workers During the COVID-19 Outbreak in a Public General Hospital in Madrid, Spain. Front. Psychiatry 2020, 11, 562578. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, P.; Narayanan, S.; Khera, T.; Kelly, L.; Mathur, P.A.; Shanker, A.; Novack, L.; Sadhasivam, S.; Hoffman, K.A.; Pérez-Robles, R.; et al. Perceived stress, resilience, well-being, and COVID 19 response in Isha yoga practitioners compared to matched controls: A research protocol. Contemp. Clin. Trials Commun. 2021, 22, 100788. [Google Scholar] [CrossRef] [PubMed]
- Faragher, E.B.; Cass, M.; Cooper, C.L. The relationship between job satisfaction and health: A meta-analysis. Occup. Env. Med. 2005, 62, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Klockner, K.; Crawford, C.; Craigie, M.; Tsai, L.; Hegney, D. A qualitative exploration of a mindful resiliency program for community healthcare providers. Nurs. Health Sci. 2021, 23, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Islam, M.; George, P.; Sankaran, S.; Su Hui, J.L.; Kit, T. Impact of COVID-19 on the mental health of healthcare workers in different regions of the world. BJPsych Open. 2021, 7, S258–S259. [Google Scholar] [CrossRef]
- Zhang, Q.; Dong, G.; Meng, W.; Chen, Z.; Cao, Y.; Zhang, M. Perceived Stress and Psychological Impact Among Healthcare Workers at a Tertiaty Hospital in China During the COVID-19 Outbreak: The Moderating Role of Resilience and Social Support. Front. Psychiatry 2022, 12, 570971. [Google Scholar] [CrossRef]
- Shbeer, A.; Ageel, M. Assessment of Occupational Burnout among Intensive Care Unit Staff in Jazan, Saudi Arabia, Using the Maslach Burnout Inventory. Crit. Care Res. Pract. 2022, 2022, 1298887. [Google Scholar] [CrossRef]
- Alyami, H.; Krägeloh, C.U.; Medvedev, O.N.; Alghamdi, S.; Alyami, M.; Althagafi, J.; Lyndon, M.; Hill, A.G. Investigating Predictors of Psychological Distress for Healthcare Workers in a Major Saudi COVID-19 Center. Int. J. Environ. Res. Public Health 2022, 19, 4459. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, H.J. Psychological General Well-Being Index (PGWB). In Assessment of Quality of Life in Clinical Trials of Cardiovascular Therapies; Chapter 9; Wenger, N.K., Mattson, M.E., Furberg, C.D., Elinson, J., Eds.; Le Jacq Publishing: Darien, CT, USA, 1984; pp. 170–183. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Ozen, G.; Zanfardino, A.; Ozen, G.; Acan, B.; Piscopo, A.; Casaburo, F.; Gicchino, F.; Confetto, S.; Troncone, A.; Iafusco, D. Comparison of emotional approaches of medical doctors against COVID-19 pandemic: Eastern and Western Mediterranean countries. Int. J. Clin. Pract. 2021, 75, e14973. [Google Scholar] [CrossRef] [PubMed]
- Maslach‚, C.; Jackson‚, S. MBI: Maslach Burnout Inventory Manual; Consulting Psychologists Press: Palo Alto‚ CA, USA, 1981. [Google Scholar]
- Demartini, B.; Nisticò, V.; D’Agostino, A.; Priori, A.; Gambini, O. Early Psychiatric Impact of COVID-19 Pandemic on the General Population and Healthcare Workers in Italy: A Preliminary Study. Front. Psychiatr. 2020, 11, 561345. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.; Leiter, M. The Maslach Burnout Inventory Manual; Mind Garden: Menlo Park, CA, USA, 1997. [Google Scholar]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Majani, G.; Di Tano, G.; Giardini, A.; De Maria, R.; Russo, G.; Maestri, R.; Marini, M.; Milli, M.; Aspromonte, N. Prevalence of job-related distress and satisfaction in a nationwide cardiology setting: The IANUS—Italian cardiologists’ Undetected distress Study. J. Cardiovasc. Med. (Hagerstown) 2016, 17, 587–594. [Google Scholar] [CrossRef]
- Mattei, A.; Fiasca, F.; Mazzei, M.; Necozione, S.; Bianchini, V. Stress and Burnout in Health-Care Workers after the 2009 L’Aquila Earthquake: A Cross-Sectional Observational Study. Front. Psychiatr. 2017, 8, 98. [Google Scholar] [CrossRef] [Green Version]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open. 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Kabasakal, E.; Özpulat, F.; Akca, A.; Özcebe, L.H. COVID-19 fear and compliance in preventive measures precautions in workers during the COVID-19 pandemic. Int. Arch. Occup. Environ. Health 2021, 94, 1239–1247. [Google Scholar] [CrossRef]
- Troisi, A.; Nanni, R.C.; Riconi, A.; Carola, V.; Di Cave, D. Fear of COVID-19 among Healthcare Workers: The Role of Neuroticism and Fearful Attachment. J. Clin. Med. 2021, 10, 4358. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Mensi, S.; Di Marco, A.; Siracusano, A.; Di Lorenzo, G. Mental Health Outcomes Among Healthcare Workers and the General Population During the COVID-19 in Italy. Front. Psychol. 2020, 11, 608986. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, T.; Walker, O.; Cann, R.; Varghese, A.K. The benefits of mindfulness in mental healthcare professionals. F1000Research 2021, 10, 1085. [Google Scholar] [CrossRef]
- Fortney, L.; Luchterhand, C.; Zakletskaia, L.; Zgierska, A.; Rakel, D. Abbreviated mindfulness intervention for job satisfaction, quality of life, and compassion in primary care clinicians: A pilot study. Ann. Fam. Med. 2013, 11, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Montero-Marin, J.; Tops, M.; Manzanera, R.; Piva Demarzo, M.M.; Álvarez de Mon, M.; García-Campayo, J. Mindfulness, Resilience, and Burnout Subtypes in Primary Care Physicians: The Possible Mediating Role of Positive and Negative Affect. Front. Psychol. 2015, 6, 1895. [Google Scholar] [CrossRef] [Green Version]
- Treadway, M.T.; Lazar, S.W. The neurobiology of mindfulness. In Clinical Handbook of Mindfulness; Didonna, F., Ed.; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2009; pp. 45–57. [Google Scholar]
- Weis, R.; Ray, S.D.; Cohen, T.A. Mindfulness as a way to cope with COVID-19-related stress and anxiety. Couns. Psychother. Res. 2020, 21, 8–18. [Google Scholar] [CrossRef]
- Matiz, A.; Fabbro, F.; Paschetto, A.; Cantone, D.; Paolone, A.R.; Crescentini, C. Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy. Int. J. Environ. Res. Public Health 2020, 17, 6450. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, A.; Liu, C.; Xiao, J.; Wang, K. A Brief Online Mindfulness-Based Group Intervention for Psychological Distress Among Chinese Residents During COVID-19: A Pilot Randomized Controlled Trial. Mindfulness 2021, 12, 1502–1512. [Google Scholar] [CrossRef]
- Bonetti, L.; Tolotti, A.; Valcarenghi, D.; Pedrazzani, C.; Barello, S.; Ghizzardi, G.; Graffigna, G.; Sari, D.; Bianchi, M. Burnout Precursors in Oncology Nurses: A Preliminary Cross-Sectional Study with a Systemic Organizational Analysis. Sustainability 2019, 11, 1246. [Google Scholar] [CrossRef] [Green Version]
- Theorell, T.; Karasek, R.A. Current issues relating to psychosocial job strain and cardiovascular disease research. J. Occup. Health Psychol. 1996, 1, 9–26. [Google Scholar] [CrossRef]
- Kriakous, S.A.; Elliott, K.A.; Lamers, C.; Owen, R. The Effectiveness of Mindfulness-Based Stress Reduction on the Psychological Functioning of Healthcare Professionals: A Systematic Review. Mindfulness 2021, 12, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout prevention: A review of intervention programs. Patient Educ. Couns. 2010, 78, 184–190. [Google Scholar] [CrossRef]
- Crowder, R.; Sears, A. Building resilience in social workers: An exploratory study on the impacts of a mindful-ness-based intervention. Aus. Soc. Work 2017, 70, 17–29. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 58, 496–503. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Group I | Group II | Group III | p Value |
|---|---|---|---|---|
| Number | 17 | 18 | 15 | |
| Women | 15 (88) | 15 (83) | 12 (80) | ns |
| Age | 43.4 (7.3) | 44.8 (8.8) | 45.2 (15.1) | ns |
| Occupation | ||||
| Physicians | 2 (12) | 4 (22) | 3 (20) | ns |
| Nurses | 9 (53) | 9 (51) | 9 (60) | |
| Allied care professionals | 6 (35) | 4 (22) | 3 (20) |
| Test | Group I Baseline | After MBSR | p Value | Group II Baseline | After MBSR | p Value | Group III Baseline | After MBSR | p Value |
|---|---|---|---|---|---|---|---|---|---|
| PGWBI * | |||||||||
| Anxiety | 15.9 (4.8) | 17.6 (2.6) | ns | 13.4 (4.4) | 14.5 (4.9) | ns | 13.7 (4.1) | 18.0 (3.4) | 0.0005 |
| Depressed mood | 12.5 (2.9) | 12.9 (1.2) | ns | 10.8 (3.4) | 10.7 (3.6) | ns | 10.5 (2.0) | 12.4 (1.7) | 0.001 |
| Positive wellbeing | 11.2 (4.1) | 12.4 (2.6) | ns | 9.2 (3.6) | 9.5 (4.5) | ns | 9.5 (3.2) | 11.9 (3.1) | 0.005 |
| Self-control | 11.3 (2.4) | 11.4 (2.1) | ns | 8.9 (3.3) | 8.7 (3.6) | ns | 8.7 (3.1) | 11.7 (2.1) | 0.002 |
| General health | 10.1 (1.5) | 12.1 (1.7) | 0.0004 | 9.2 (3.2) | 9.2 (3.7) | ns | 9.5 (3.0) | 11.4 (2.1) | 0.008 |
| Vitality | 10.0 (2.2) | 10.8 (1.9) | ns | 8.9 (1.7) | 9.3 (2.1) | ns | 10.0 (2.1) | 10.9 (1.4) | ns |
| Total score | 71.1 (14.6) | 77.2 (8.6) | 0.04 | 60.3 (15.7) | 61.8 (18.2) | ns | 61.9 (14.9) | 76.2 (11.6) | 0.0006 |
| PSS | |||||||||
| Total PSS | 18.0 (6.8) | 14.1 (5.6) | 0.03 | 20.9 (6.9) | 20.3 (7.4) | ns | 22.8 (4.6) | 13.3 (4.5) | 0.0001 |
| MBI | |||||||||
| Depersonalization | 4.9 (4.7) | 5.5 (5.5) | ns | 3.2 (3.4) | 4.0 (4.3) | 0.02 | 5.4 (5.8) | 6.1 (6.9) | 0.04 |
| Accomplishment | 34.0 (6.4) | 34.1 (7.6) | ns | 35.0 (7.8) | 37.9 (4.5) | ns | 34.1 (6.7) | 35.6 (6.5) | ns |
| Emotional exhaustion | 18.7 (7.9) | 18.3 (7.2) | ns | 21.5 (7.8) | 21.6 (10.2) | ns | 16.4 (8.6) | 8.6 (7.2) | 0.0007 |
| Test | Group I Baseline | After MBSR | p Value | Group II Baseline | After MBSR | p Value | Group III Baseline | After MBSR | p Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| PGWBI | ||||||||||
| Total score | Moderate | 1 | 2 | ns | 6 | 4 | ns | 3 | 2 | 0.03 |
| High | 3 | 0 | 6 | 3 | 5 | 0 | ||||
| PSS | ||||||||||
| Total PSS | Moderate | 11 | 9 | 0.049 | 13 | 10 | ns | 12 | 8 | 0.026 |
| High | 3 | 0 | 3 | 2 | 2 | 0 | ||||
| MBI | ||||||||||
| Depersonalization | Moderate | 6 | 6 | ns | 1 | 3 | ns | 3 | 3 | ns |
| High | 2 | 2 | 2 | 2 | 3 | 3 | ||||
| Accomplishment | Moderate | 3 | 3 | ns | 4 | 4 | ns | 4 | 5 | ns |
| High | 3 | 5 | 4 | 4 | 4 | 4 | ||||
| Emotional exhaustion | Moderate | 8 | 8 | ns | 7 | 5 | ns | 3 | 0 | ns |
| High | 1 | 2 | 5 | 2 | 3 | 1 |
| Baseline | Post MBSR Course | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p Value | |
| 1. I am most afraid of the coronavirus | 3.8 | 1.0 | 3.0 | 1.3 | 0.015 |
| 2. It makes me uncomfortable to think about the coronavirus | 3.7 | 0.6 | 2.9 | 1.3 | 0.017 |
| 3. My hands become clammy when I think about the coronavirus | 1.6 | 0.9 | 1.2 | 0.5 | ns |
| 4. I am afraid of losing my life because of the coronavirus | 2.4 | 0.8 | 2.0 | 1.0 | ns |
| 5. When watching news and stories about the coronavirus on social media, I become nervous or anxious | 3.2 | 0.9 | 2.6 | 1.2 | ns |
| 6. I cannot sleep because I’m worrying about getting the coronavirus | 1.8 | 0.9 | 1.2 | 0.5 | 0.04 |
| 7. My heart rates or palpitates when I think about getting the coronavirus | 2.0 | 1.0 | 1.5 | 0.8 | 0.049 |
| Total score | 18.5 | 4.3 | 14.4 | 5.1 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marotta, M.; Gorini, F.; Parlanti, A.; Berti, S.; Vassalle, C. Effect of Mindfulness-Based Stress Reduction on the Well-Being, Burnout and Stress of Italian Healthcare Professionals during the COVID-19 Pandemic. J. Clin. Med. 2022, 11, 3136. https://doi.org/10.3390/jcm11113136
Marotta M, Gorini F, Parlanti A, Berti S, Vassalle C. Effect of Mindfulness-Based Stress Reduction on the Well-Being, Burnout and Stress of Italian Healthcare Professionals during the COVID-19 Pandemic. Journal of Clinical Medicine. 2022; 11(11):3136. https://doi.org/10.3390/jcm11113136
Chicago/Turabian StyleMarotta, Marco, Francesca Gorini, Alessandra Parlanti, Sergio Berti, and Cristina Vassalle. 2022. "Effect of Mindfulness-Based Stress Reduction on the Well-Being, Burnout and Stress of Italian Healthcare Professionals during the COVID-19 Pandemic" Journal of Clinical Medicine 11, no. 11: 3136. https://doi.org/10.3390/jcm11113136