
Job Satisfaction of Health Practitioners Providing Outreach Health Services during COVID-19 in Rural New South Wales (NSW) and the Australian Capital Territory (ACT), Australia
 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Outreach Health Services
1.2. NSW Rural Doctors Network’s Outreach Program Model
1.3. Job Satisfaction
1.4. Impact of COVID-19 on Outreach Health Services
1.5. Study Aims
2. Methods
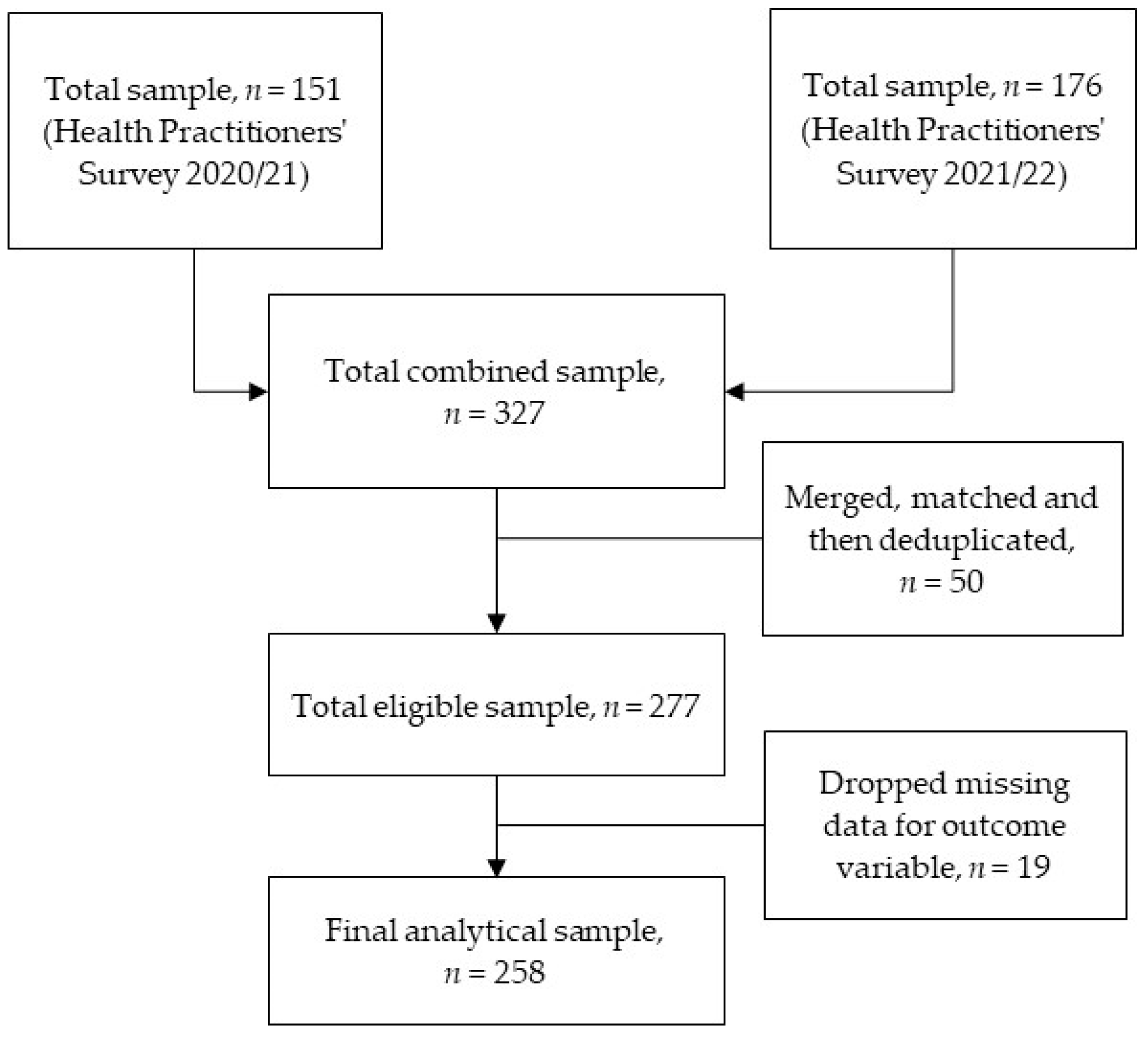
2.1. Data Source
2.2. Measures
- Country of birth: Overseas or Australia
- Type of health practitioner: Aboriginal Health Worker (AHW), Nurse/Midwife, Allied health professional (e.g., Therapist, Nutritionist, Optometrist, and others) or Medical Practitioner (i.e., Specialist/GP).
- Self-confidence in being culturally responsive when treating patients: The responses were self-reported and categorised into two, somewhat confident or confident.
- Presence of motivating factors: On the basis of previous research [42,43] and context of outreach services in Australia, the survey team included the following six motivating factors—(a) To grow my practice, (b) To provide healthcare to disadvantaged people or regions, (c) To maintain a personal connection to a region, (d) To provide complex healthcare in challenging situations, (e) To provide support for rural health staff, and (f) Outreach is a requirement for employment. A five-point Likert scale was used to rank each selected motivating factor, rated from strongly disagree to strongly agree. Since high motivation has positive impact on job satisfaction and subsequently on job performance of health practitioners [42,43], we created a new variable as ‘presence of motivating factors’ from each response in this study. Categories were as follows: health practitioners with no motivating factors (coded as 0), with 1–2 motivating factors (coded as 1), with 3–4 motivating factors (coded as 2), and with 4 or more factors (coded as 3).
- Communication with other local health practitioners: A four-point Likert scale (very dissatisfied, dissatisfied, satisfied, very satisfied) was used. In this study, we created a dichotomous variable from the responses; ‘satisfied’ and ‘very satisfied’ were categorised as ‘satisfied’ (coded as 1), and while ‘very dissatisfied’ and ‘dissatisfied’ were classified as ‘dissatisfied’ (coded as 0).
- Using only paper-based referrals: Yes or No
- Using only electronic referrals: Yes or No
- Health practitioners providing telehealth: Yes or No
- Self-reported capability: The following question was used to measure capability, ‘Acknowledging that on different days we all feel (more or less) on top of our working and personal lives, in your most recent outreach visits how would you describe your overall level of capability in fulfilling your healthcare role?’, rated on a 10-point Likert scale ranged from 0-Not capable to 10-Fully capable. For the analyses, we created a new variable as ‘Self-reported capability’ from the responses, scores 0–3 was categorised as ‘Less capable’ (coded 0), scores 4–6 labelled as ‘Capable’ (coded 1) and scores 7–10 classified as ‘More capable’ (coded 2). Note that RDN used the term ‘capability’ in the context of an ‘intersection between individual capacity and ability to respond to work considering the whole of life challenges, including work, travel, family, schools, partner, education, and social options’.
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
4. Discussion
4.1. Communication with Other Local Health Practitioners
4.2. Access to Telehealth (Virtual Care)
4.3. Self-Reported Capability
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aith, F.; Castilla Martínez, M.; Cho, M.; Dussault, G.; Harris, M.; Padilla, M.; Murphy, G.T.; Tomlin, P.; Valderas, J.M. Is COVID-19 a turning point for the health workforce? Rev. Panam. Salud Publica 2020, 44, e102. [Google Scholar] [CrossRef] [PubMed]
- Buchan, J.; Campbell, J. Challenges posed by the global crisis in the health workforce. BMJ Br. Med. J. 2013, 347, f6201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khasne, R.; Dhakulkar, B.; Mahajan, H. Burnout among Healthcare Workers during COVID-19 Pandemic in India: Results of a Questionnaire-based Survey. Indian J. Crit. Care Med. 2020, 24, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Leo, C.; Sabina, S.; Tumolo, M.; Bodini, A.; Ponzini, G.; Sabato, E.; Mincarone, P. Burnout among Healthcare Workers in the COVID-19 Era: A Review of the Existing Literature. Front. Public Health 2021, 9, 750529. [Google Scholar] [CrossRef] [PubMed]
- Dugani, S.; Afari, H.; Hirschhorn, L.R.; Ratcliffe, H.; Veillard, J.; Martin, G.; Lagomarsino, G.; Basu, L.; Bitton, A. Prevalence and factors associated with burnout among frontline primary health care providers in low-and middle-income countries: A systematic review. Gates Open Res. 2018, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Retention of the Health Workforce in Rural and Remote Areas: A Systematic Review. Available online: https://apps.who.int/iris/handle/10665/337300 (accessed on 23 June 2022).
- World Health Organization. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies; World Health Organization: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/258734 (accessed on 23 June 2022).
- O’Sullivan, B.; Leader, J.; Couch, D.; Purnell, J. Rural Pandemic Preparedness: The Risk, Resilience and Response Required of Primary Healthcare. Risk Manag. Healthc. Policy 2020, 13, 1187–1194. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Profile of Indigenous Australians. 2020. Available online: https://www.aihw.gov.au/reports/australias-health/profile-of-indigenous-australians (accessed on 25 June 2022).
- Cosgrave, C.; Malatzky, C.; Gillespie, J. Social Determinants of Rural Health Workforce Retention: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 314. [Google Scholar] [CrossRef] [Green Version]
- Gruen, R.L.; Weeramanthri, T.S.; Bailie, R.S. Outreach and improved access to specialist services for Indigenous people in remote Australia: The requirements for sustainability. J. Epidemiol. Community Health 2002, 56, 517–521. [Google Scholar] [CrossRef]
- Wakerman, J.; Humphreys, J.; Russell, D.; Guthridge, S.; Bourke, L.; Dunbar, T.; Zhao, Y.; Ramjan, M.; Murakami-Gold, L.; Jones, M.P. Remote health workforce turnover and retention: What are the policy and practice priorities? Hum. Resour. Health 2019, 17, 99. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Rural and Remote Health. 2020. Available online: https://www.aihw.gov.au/reports/australias-health/rural-and-remote-health (accessed on 25 November 2022).
- Cosgrave, C. The Whole-of-Person Retention Improvement Framework: A Guide for Addressing Health Workforce Challenges in the Rural Context. Int. J. Environ. Res. Public Health 2020, 17, 2698. [Google Scholar] [CrossRef]
- Humphreys, J.; Wakerman, J. Learning from history: How research evidence can inform policies to improve rural and remote medical workforce distribution. Aust. J. Rural Health 2018, 26, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Cultural Safety in Health Care for Indigenous Australians: Monitoring Framework. 2022. Available online: https://www.aihw.gov.au/reports/indigenous-australians/cultural-safety-health-care-framework (accessed on 27 November 2022).
- McGirr, J.; Seal, A.; Barnard, A.; Cheek, C.; Garne, D.; Greenhill, J.; Kondalsamy-Chennakesavan, S.; Luscombe, G.M.; May, J.; McLeod, J.; et al. The Australian Rural Clinical School (RCS) program supports rural medical workforce: Evidence from a cross-sectional study of 12 RCSs. Rural Remote Health 2019, 19, 4971. [Google Scholar] [CrossRef] [PubMed]
- Lyle, D.; Greenhill, J. Two decades of building capacity in rural health education, training and research in Australia: University Departments of Rural Health and Rural Clinical Schools. Aust. J. Rural Health 2018, 26, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Mason, J. Review of Australian Government Health Workforce Programs. 2013. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/review-australian-government-health-workforce-programs (accessed on 27 June 2022).
- Stanković, A.; Nikolić, M.; Nikic, D.S.; Arandjelović, M. Job Satisfaction in Health Care Workers. Acta Med. Median. 2008, 47, 9–12. Available online: https://www.researchgate.net/profile/Mirjana-Arandjelovic/publication/26605370_Job_satisfaction_in_health_care_workers/links/09e4150aa6945c34ac000000/Job-satisfaction-in-health-care-workers.pdf (accessed on 27 June 2022).
- Bimpong, K.; Khan, A.; Slight, R.; Tolley, C.L.; Slight, S.P. Relationship between labour force satisfaction, wages and retention within the UK National Health Service: A systematic review of the literature. BMJ Open 2020, 10, e034919. [Google Scholar] [CrossRef]
- Søvold, L.; Naslund, J.; Kousoulis, A.; Saxena, S.; Qoronfleh, M.; Grobler, C.; Münter, L. Prioritizing the Mental Health and Well-Being of Healthcare Workers: An Urgent Global Public Health Priority. Front. Public Health 2021, 9, 679397. [Google Scholar] [CrossRef]
- New South Wales Parliament; Legislative Council. Portfolio Committee No. 2—Health (Report No. 57). Health Outcomes and Access to Health and Hospital Services in Rural, Regional and Remote New South Wales. 2022. Available online: https://www.parliament.nsw.gov.au/lcdocs/inquiries/2615/Report%20no%2057%20-%20PC%202%20-%20Health%20outcomes%20and%20access%20to%20services.pdf (accessed on 1 July 2022).
- O’Sullivan, B.G.; Stoelwinder, J.U.; McGrail, M.R. Specialist outreach services in regional and remote Australia: Key drivers and policy implications. Med. J. Aust. 2017, 207, 98–99. [Google Scholar] [CrossRef]
- Roodenbeke, E.D.; World Health Organization. Outreach Services as a Strategy to Increase Access to Health Workers in Remote and Rural Areas: Increasing Access to Health Workers in Rural and Remote Areas; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/bitstream/handle/10665/44589/9789241501514_eng.pdf (accessed on 2 July 2022).
- O’Sullivan, B.G.; Joyce, C.M.; McGrail, M.R. Adoption, implementation and prioritization of specialist outreach policy in Australia: A national perspective. Bull. World Health Organ. 2014, 92, 512–519. [Google Scholar] [CrossRef]
- O’Sullivan, B.; McGrail, M.; Stoelwinder, J. Reasons why specialist doctors undertake rural outreach services: An Australian cross-sectional study. Hum. Resour. Health 2017, 15, 3. [Google Scholar] [CrossRef] [Green Version]
- Alrawashdeh, H.; Al-Tammemi, A.; Alzawahreh, M.; Al-Tamimi, A.; Elkholy, M.; Al Sarireh, F.; Abusamak, M.; Elehamer, N.M.; Malkawi, A.; Al-Dolat, W.; et al. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: A convergent parallel mixed-method study. BMC Public Health 2021, 21, 811. [Google Scholar] [CrossRef]
- Hussain, R.; Maple, M.; Hunter, S.; Mapedzahama, V.; Reddy, P. The Fly-in Fly-out and Drive-in Drive-out model of health care service provision for rural and remote Australia: Benefits and disadvantages. Rural Remote Health 2015, 15, 3068. [Google Scholar] [CrossRef] [PubMed]
- Busbridge, M.; Smith, A. Fly in/fly out health workers: A barrier to quality in health care. Rural Remote Health 2015, 15, 3339. [Google Scholar] [CrossRef] [PubMed]
- Carey, T.A.; Sirett, D.; Wakerman, J.; Russell, D.; Humphreys, J.S. What principles should guide visiting primary health care services in rural and remote communities? Lessons from a systematic review. Aust. J. Rural Health 2018, 26, 146–156. [Google Scholar] [CrossRef]
- Janicijevic, I.; Seke, K.; Djokovic, A.; Filipovic, T. Healthcare workers satisfaction and patient satisfaction—where is the linkage? Hippokratia 2013, 17, 157–162. [Google Scholar] [PubMed]
- Huhtala, M.; Geurts, S.; Mauno, S.; Feldt, T. Intensified job demands in healthcare and their consequences for employee well-being and patient satisfaction: A multilevel approach. J. Adv. Nurs. 2021, 77, 3718–3732. [Google Scholar] [CrossRef] [PubMed]
- Aloisio, L.D.; Gifford, W.A.; McGilton, K.S.; Lalonde, M.; Estabrooks, C.A.; Squires, J.E. Individual and organizational predictors of allied healthcare providers’ job satisfaction in residential long-term care. BMC Health Serv. Res. 2018, 18, 491. [Google Scholar] [CrossRef]
- Grujičić, M.; Jovičić-Bata, J.; Rađen, S.; Novakovic, B.; Šipetić-Grujičić, S. Work motivation and job satisfaction of health workers in urban and rural areas. Vojnosanit. Pregl. 2016, 73, 735–743. [Google Scholar] [CrossRef] [Green Version]
- Gilles, I.; Burnand, B.; Peytremann-Bridevaux, I. Factors associated with healthcare professionals’ intent to stay in hospital: A comparison across five occupational categories. Int. J. Qual. Health Care 2014, 26, 158–166. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Rural and Remote Health. 2022. Available online: https://www.aihw.gov.au/reports/rural-remote-australians/rural-and-remote-health (accessed on 27 November 2022).
- Australian Institute of Health and Welfare. Health Workforce. 2022. Available online: https://www.aihw.gov.au/reports/workforce/health-workforce (accessed on 27 November 2022).
- CCmedical. What’s the Difference between Rural and Remote Doctor Work? 2018. Available online: https://www.ccjobs.com.au/blog/whats-the-difference-between-rural-and-remote-doctor-work (accessed on 27 November 2022).
- Satuf, C.; Monteiro, S.; Pereira, H.; Esgalhado, G.; Marina Afonso, R.; Loureiro, M. The protective effect of job satisfaction in health, happiness, well-being and self-esteem. Int. J. Occup. Saf. Ergon. 2018, 24, 181–189. [Google Scholar] [CrossRef]
- Marinucci, F.; Majigo, M.; Wattleworth, M.; Paterniti, A.D.; Hossain, M.B.; Redfield, R. Factors affecting job satisfaction and retention of medical laboratory professionals in seven countries of Sub-Saharan Africa. Hum. Resour. Health 2013, 11, 38. [Google Scholar] [CrossRef] [Green Version]
- Mathauer, I.; Imhoff, I. Health worker motivation in Africa: The role of non-financial incentives and human resource management tools. Hum. Resour. Health 2006, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, M.; Cuong, P.V.; Anh, L.V.; Martineau, T. Identifying factors for job motivation of rural health workers in North Viet Nam. Hum. Resour. Health 2003, 1, 10. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, M.W.; Chen, P.G.; Van Busum, K.R.; Aunon, F.; Pham, C.; Caloyeras, J.; Mattke, S.; Pitchforth, E.; Quigley, D.D.; Brook, R.H.; et al. Factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Rand Health Q. 2014, 3, 1. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5051918/ (accessed on 16 July 2022). [PubMed]
- Barac, A.; Krnjaic, P.; Vujnovic, N.; Matas, N.; Runjic, E.; Rogoznica, M.; Markic, J.; Jelicic Kadic, A. The impact of the COVID-19 pandemic on resident physicians: A cross-sectional study. Work 2021, 69, 751–758. [Google Scholar] [CrossRef]
- Coto, J.; Restrepo, A.; Cejas, I.; Prentiss, S. The impact of COVID-19 on allied health professions. PLoS ONE 2020, 15, e0241328. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Bio-Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Jazieh, A.R.; Coutinho, A.K.; Bensalem, A.A.; Alsharm, A.A.; Errihani, H.; Mula-Hussain, L.; Al-Sukhun, S.; Sampaio-Filho, C.A.; Khorshid, O.; De Guzman, R.B.; et al. Impact of the COVID-19 Pandemic on Oncologists: Results of an International Study. JCO Glob. Oncol. 2021, 7, 242–252. [Google Scholar] [CrossRef]
- Bernacki, K.; Keister, A.; Sapiro, N.; Joo, J.; Mattle, L. Impact of COVID-19 on patient and healthcare professional attitudes, beliefs, and behaviors toward the healthcare system and on the dynamics of the healthcare pathway. BMC Health Serv. Res. 2021, 21, 1309. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Xiong, Y.; Peng, L. Focusing on health-care providers’ experiences in the COVID-19 crisis. Lancet Glob. Health 2020, 8, e740–e741. [Google Scholar] [CrossRef]
- Shi, L.; Song, K.; Rane, S.; Sun, X.; Li, H.; Meng, Q. Factors associated with job satisfaction by Chinese primary care providers. Prim. Health Care Res. Dev. 2014, 15, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Savageau, J.A.; Ferguson, W.J.; Bohlke, J.L.; Cragin, L.J.; O’Connell, E. Recruitment and retention of primary care physicians at community health centers: A survey of Massachusetts physicians. J. Health Care Poor Underserv. 2011, 22, 817–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoen, C.; Osborn, R.; Doty, M.M.; Squires, D.; Peugh, J.; Applebaum, S. A Survey of Primary Care Physicians in Eleven Countries, 2009: Perspectives on Care, Costs, and Experiences: Doctors say problems exist across all eleven countries, although some nations are doing a better job than others. Health Aff. 2009, 28 (Suppl. S1), w1171–w1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veall, M.R.; Zimmermann, K.F. Pseudo-R2 measures for some common limited dependent variable models. J. Econ. Surv. 1996, 10, 241–259. [Google Scholar] [CrossRef] [Green Version]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013; Volume 398. [Google Scholar] [CrossRef]
- Jones, A.M. Models for Health Care; Centre for Health Economics, University of York: New York, NY, USA, 2012. [Google Scholar] [CrossRef]
- Murray, L.; Nguyen, H.; Lee, Y.; Remmenga, M.; Smith, D.W. Variance inflation factors in regression models with dummy variables. In Proceedings of the Conference on Applied Statistics in Agriculture, Perth, Australia, 24–27 June 2012. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; You, Y.; Wang, Y.; Wang, Y.; Dai, T. Global Insights into Rural Health Workers’ Job Satisfaction: A Scientometric Perspective. Front. Public Health 2022, 10, 895659. [Google Scholar] [CrossRef]
- Rostami, F.; Babaei-Pouya, A.; Teimori-Boghsani, G.; Jahangirimehr, A.; Mehri, Z.; Feiz-Arefi, M. Mental Workload and Job Satisfaction in Healthcare Workers: The Moderating Role of Job Control. Front. Public Health 2021, 9, 683388. [Google Scholar] [CrossRef]
- Yi, M.; Jiang, D.; Wang, J.; Zhang, Z.; Jia, Y.; Zhao, B.; Guo, L.; Chen, O. Relationships among thriving at work, organisational commitment and job satisfaction among Chinese front-line primary public health workers during COVID-19 pandemic: A structural equation model analysis. BMJ Open 2022, 12, e059032. [Google Scholar] [CrossRef]
- Stobbe, E.J.; Groenewegen, P.P.; Schäfer, W. Job satisfaction of general practitioners: A cross-sectional survey in 34 countries. Hum. Resour. Health 2021, 19, 57. [Google Scholar] [CrossRef]
- Kagan, I.; Hendel, T.; Savitsky, B. Personal initiative and work environment as predictors of job satisfaction among nurses: Cross-sectional study. BMC Nurs. 2021, 20, 87. [Google Scholar] [CrossRef]
- Barili, E.; Bertoli, P.; Grembi, V.; Rattini, V. Job Satisfaction among Healthcare Workers in the Aftermath of the COVID-19 Pandemic (No. 22/04). HEDG, c/o Department of Economics, University of York. 2022. Available online: https://www.york.ac.uk/media/economics/documents/hedg/workingpapers/2022/2204.pdf (accessed on 26 July 2022).
- Pincus, J.D. Communication Satisfaction, Job Satisfaction, And Job Performance. Hum. Commun. Res. 1986, 12, 395–419. [Google Scholar] [CrossRef]
- Vermeir, P.; Degroote, S.; Vandijck, D.; Mariman, A.; Deveugele, M.; Peleman, R.; Verhaeghe, R.; Cambré, B.; Vogelaers, D. Job Satisfaction in Relation to Communication in Health Care among Nurses: A Narrative Review and Practical Recommendations. SAGE Open 2017, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Loughman, T.P.; Snipes, R.L.; Pitts, J.P. The effects of physicians’ communication satisfaction and their perceptions of empowerment on their likelihood to recommend a hospital to their peers. Manag. Res. News 2009, 32, 354–370. [Google Scholar] [CrossRef]
- Zerden, L.d.S.; Lombardi, B.M.; Richman, E.L.; Forte, A.B.; McCollum, M. Addressing Burnout among the Frontline Healthcare Workforce during COVID-19: A Scoping Review & Expert Interviews. J. Health Hum. Serv. Adm. 2021, 44, 302–333. [Google Scholar] [CrossRef]
- Wilson, M.M.; Devasahayam, A.J.; Pollock, N.J.; Dubrowski, A.; Renouf, T. Rural family physician perspectives on communication with urban specialists: A qualitative study. BMJ Open 2021, 11, e043470. [Google Scholar] [CrossRef] [PubMed]
- Hein, S. EQ for Everybody: A Practical Guide to Emotional Intelligence; Aristotle Press: Washington, DC, USA, 1996; Available online: https://books.google.com.au/books?id=F1PoAAAACAAJ (accessed on 27 July 2022).
- Gardiner, M.; Sexton, R.; Kearns, H.; Marshall, K. Impact of support initiatives on retaining rural general practitioners. Aust. J. Rural Health 2006, 14, 196–201. [Google Scholar] [CrossRef]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.-A.; Ellis, L.; Polson, R.; O’Malley, C.M. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: Implications for supporting psychological well-being. BMC Public Health 2021, 21, 104. [Google Scholar] [CrossRef]
- Iyengar, K.P.; Jain, V.K.; Vaishya, R. Current situation with doctors and healthcare workers during COVID-19 pandemic in India. Postgrad. Med. J. 2022, 98, e121. [Google Scholar] [CrossRef]
- Isautier, J.M.; Copp, T.; Ayre, J.; Cvejic, E.; Meyerowitz-Katz, G.; Batcup, C.; Bonner, C.; Dodd, R.; Nickel, B.; Pickles, K.; et al. People’s Experiences and Satisfaction with Telehealth During the COVID-19 Pandemic in Australia: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e24531. [Google Scholar] [CrossRef]
- Snoswell, C.L.; Caffery, L.J.; Haydon, H.M.; Thomas, E.E.; Smith, A.C. Telehealth uptake in general practice as a result of the coronavirus (COVID-19) pandemic. Aust. Health Rev. 2020, 44, 737–740. [Google Scholar] [CrossRef]
- Cashman, H.; Sushil, S.; Mayson, E.; Milliken, S.; Lavee, O.; Awford, A.; Hamad, N. Telemedicine for rural and regional patient access to haematology services during the COVID-19 pandemic in Australia. Lancet Haematol. 2022, 9, e325–e326. [Google Scholar] [CrossRef]
- NSW Rural Doctors Network. COVID-19 Support. 2022. Available online: https://www.nswrdn.com.au/site/covid-19 (accessed on 2 August 2022).
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19–Related Concern—United States. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.H.M.; Kuet, M.-L.; Patel, M.K.; Puri, P. Addressing COVID-19 fear to improve clinic attendance for patients with wet age-related macular degeneration. Acta Ophthalmol. 2021, 99, e285. [Google Scholar] [CrossRef] [PubMed]
- Jessup, R.L.; Bramston, C.; Beauchamp, A.; Gust, A.; Cvetanovska, N.; Cao, Y.; Haywood, C.; Conilione, P.; Tacey, M.; Copnell, B.; et al. Impact of COVID-19 on emergency department attendance in an Australia hospital: A parallel convergent mixed methods study. BMJ Open 2021, 11, e049222. [Google Scholar] [CrossRef]
- Fisher, K.; Davey, A.R.; Magin, P. Telehealth for Australian general practice: The present and the future. Aust. J. Gen. Pract. 2022, 51, 626–629. [Google Scholar] [CrossRef]
- Haydon, H.M.; Snoswell, C.L.; Thomas, E.E.; Broadbent, A.; Caffery, L.J.; Brydon, J.A.; Smith, A.C. Enhancing a community palliative care service with telehealth leads to efficiency gains and improves job satisfaction. J. Telemed. Telec. 2021, 27, 625–630. [Google Scholar] [CrossRef]
- Salem, R.; El Zakhem, A.; Gharamti, A.; Tfayli, A.; Osman, H. Palliative care via telemedicine: A qualitative study of caregiver and provider perceptions. J. Palliat. Med. 2020, 23, 1594–1598. [Google Scholar] [CrossRef]
- Read Paul, L.; Salmon, C.; Sinnarajah, A.; Spice, R. Web-based videoconferencing for rural palliative care consultation with elderly patients at home. Support. Care Cancer 2019, 27, 3321–3330. [Google Scholar] [CrossRef]
- Fraser, S.; Greenhalgh, T. Complexity science: Coping with complexity: Educating for capability. BMJ 2001, 323, 799–803. [Google Scholar] [CrossRef]
- Martiniuk, A.; Colbran, R.; Ramsden, R.; Edwards, M.; Barrett, E.; O’Callaghan, E.; Bullock, R.; Lowe, E.F.; Karlson, D.; Curnow, J.; et al. Capability... What’s in a word? Rural Doctors Network of New South Wales Australia is shifting to focus on the capability of rural health professionals. Rural Remote Health 2020, 20, 5633. [Google Scholar] [CrossRef]
- Sen, A. Equality of What. The Tanner Lecture on Human Values. 1979. Available online: https://www.suz.uzh.ch/dam/jcr:ffffffff-df42-7cac-ffff-ffffd4ec9ff2/SEN_1.pdf (accessed on 2 August 2022).
- López Barreda, R.; Robertson-Preidler, J.; Bedregal García, P. Health assessment and the capability approach. Glob. Bioeth. 2019, 30, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Leßmann, O.; Bonvin, J.-M. Job-satisfaction in the broader framework of the capability approach. Manag. Rev. 2011, 22, 84–99. Available online: http://www.jstor.org/stable/41783672 (accessed on 2 August 2022). [CrossRef]
- Ramsden, R.; Pit, S.; Colbran, R.; Payne, K.; Tan, A.J.H.; Edwards, M. Development of a framework to promote rural health workforce capability through digital solutions: A qualitative study of user perspectives. Digit. Health 2022, 8. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Yorke, M. Capability and Quality in Higher Education; Kogan Page: London, UK, 1998; Available online: https://books.google.com.au/books?id=jPiwJLiWtA8C (accessed on 2 August 2022).
- Nelson, T.; Johnson, S.; Bebbington, P. Satisfaction and burnout among staff of crisis resolution, assertive outreach and community mental health teams. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 44, 541–549. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Country of birth | |
| Overseas | 73 (28.3) |
| Australia | 185 (71.7) |
| Type of health practitioners | |
| Aboriginal Health Workers (AHWs) | 19 (7.4) |
| Nurses/Midwives | 32 (12.4) |
| Allied Health Professionals (AHPs) | 123 (47.7) |
| Medical Practitioners (MP) | 84 (32.5) |
| Self-confidence (Cultural perspective) | |
| Somewhat confident | 31 (12.0) |
| Confident | 94 (36.4) |
| Missing | 133 (51.6) |
| Presence of motivating factors | |
| No factors | 83 (32.2) |
| 1–2 factors | 14 (5.4) |
| 3–4 factors | 124 (48.1) |
| >4 factors | 37 (14.3) |
| Communication with local health practitioners | |
| Dissatisfactory | 24 (9.3) |
| Satisfactory | 156 (60.5) |
| Missing | 78 (30.2) |
| Using paper-based referrals | |
| No | 146 (56.6) |
| Yes | 112 (43.4) |
| Using electronic referrals | |
| No | 201 (77.9) |
| Yes | 57 (22.1) |
| Provide telehealth | |
| No | 94 (36.4) |
| Yes | 164 (63.6) |
| Self-reported capability | |
| Less capable | 7 (2.7) |
| Capable | 30 (11.6) |
| More capable | 221 (85.7) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1 Country of birth | 1.00 | ||||||||
| 2 Type of health practitioners | −0.36 * | ||||||||
| 3 Self-confidence | −0.01 | −0.11 | |||||||
| 4 Presence of motivating factors | 0.08 | −0.11 | 0.02 | ||||||
| 5 Communication with local health practitioners | −0.16 * | 0.15 * | −0.06 | −0.01 | |||||
| 6 Using paper-based referrals | −0.09 | −0.03 | 0.01 | 0.51 * | 0.23 * | ||||
| 7 Using electronic referrals | 0.04 | −0.05 | 0.06 | 0.34 * | 0.02 | 0.23 * | |||
| 8 Provide telehealth | −0.06 | 0.11 | 0.07 | 0.03 | 0.06 | 0.20 * | 0.05 | ||
| 9 Self-reported capability | 0.07 | 0.02 | 0.23 * | 0.00 | −0.04 | 0.02 | 0.02 | 0.02 | |
| 10 Overall satisfaction | −0.05 | 0.05 | 0.06 | 0.04 | 0.26 * | 0.13 * | 0.01 | 0.17 * | 0.21 * |
| Dissatisfied | Satisfied | Pearson χ2 (p-Value) | |
|---|---|---|---|
| n (%) | n (%) | ||
| Country of birth | 0.73 (0.391) | ||
| Overseas | 4 (5.5) | 69 (94.5) | |
| Australia | 16 (8.7) | 169 (91.3) | |
| Type of health practitioners | 2.60 (0.457) | ||
| AHWs | 3 (15.8) | 16 (84.2) | |
| Nurses/Midwives | 3 (9.4) | 29 (90.6) | |
| AHPs | 7 (5.7) | 116 (94.3) | |
| MPs | 7 (8.3) | 77 (91.7) | |
| Self-confidence | 0.38 (0.538) | ||
| Somewhat confident | 3 (9.7) | 28 (90.3) | |
| Confident | 6 (6.4) | 88 (93.6) | |
| Presence of motivating factors | 0.72 (0.868) | ||
| No factors | 8 (9.6) | 75 (90.4) | |
| 1–2 factors | 1 (7.1) | 13 (92.9) | |
| 3–4 factors | 8 (6.5) | 116 (93.5) | |
| >4 factors | 3 (8.1) | 34 (91.9) | |
| Communication with local health practitioners | 13.06 (<0.001) | ||
| Dissatisfactory | 6 (25.0) | 18 (75.0) | |
| Satisfactory | 7 (4.5) | 149 (95.5) | |
| Using paper-based referrals | 4.83 (0.028) | ||
| No | 16 (11.0) | 130 (89.0) | |
| Yes | 4 (3.6) | 108 (96.4) | |
| Using electronic referrals | 0.05 (0.814) | ||
| No | 16 (8.0) | 185 (92.0) | |
| Yes | 4 (7.0) | 53 (93.0) | |
| Provide telehealth | 7.63 (0.006) | ||
| No | 13 (13.8) | 81 (86.2) | |
| Yes | 7 (4.3) | 157 (95.7) | |
| Self-reported capability | 12.20 (0.002) | ||
| Less capable | 2 (28.6) | 5 (71.4) | |
| Capable | 6 (20.0) | 24 (80.0) | |
| More capable | 12 (5.4) | 209 (94.6) |
| Unadjusted OR | 95% CI | Adjusted OR | 95% CI | VIF | |
|---|---|---|---|---|---|
| Country of birth (Ref. Overseas) | - | ||||
| Australia | 0.61 | 0.19–1.89 | - | - | |
| Type of health practitioners (Ref. AHWs) | - | ||||
| Nurses/Midwives | 1.81 | 0.32–10.04 | - | - | |
| AHPs | 3.11 | 0.72–13.24 | - | - | |
| MPs | 2.06 | 0.48–8.84 | - | - | |
| Self-confidence (Ref. Somewhat confident) | - | ||||
| Confident | 1.57 | 0.36–6.69 | - | - | |
| Presence of motivating factors (Ref. No factors) | - | ||||
| 1–2 factors | 1.38 | 0.15–12.03 | - | - | |
| 3–4 factors | 1.54 | 0.55–4.29 | - | - | |
| >4 factors | 1.21 | 0.30–4.84 | - | - | |
| Communication with local health practitioners (Ref. Dissatisfactory) | 1.08 | ||||
| Satisfactory | 7.09 ** | 2.14–23.44 | 7.76 ** | 1.86–32.37 | |
| Using paper-based referrals (Ref. No) | 1.03 | ||||
| Yes | 3.32 * | 1.07–10.23 | 2.38 | 0.59–9.58 | |
| Using electronic referrals (Ref. No) | - | ||||
| Yes | 1.14 | 0.37–3.57 | - | - | |
| Provide telehealth (Ref. No) | 1.03 | ||||
| Yes | 3.59 ** | 1.38–9.37 | 4.07 * | 1.06–15.59 | |
| Self-reported capability (Ref. Less capable) | 1.04 | ||||
| Capable | 1.60 | 0.24–10.36 | 1.72 | 0.13–21.50 | |
| More capable | 6.96 * | 1.22–39.69 | 10.92 * | 1.18–101.03 | |
| Model statistics | |||||
| McFadden’s R2 (%) | 0.263 | ||||
| Goodness-of-fit test (p-value) | 7.11 (0.789) | ||||
| Link test (OR for that of satisfaction) | 3.79 * | ||||
| Mean VIF | 1.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.I.; Bagnulo, S.; Wang, Y.; Ramsden, R.; Wrightson, T.; Masset, A.; Colbran, R.; Edwards, M.; Martiniuk, A. Job Satisfaction of Health Practitioners Providing Outreach Health Services during COVID-19 in Rural New South Wales (NSW) and the Australian Capital Territory (ACT), Australia. Healthcare 2023, 11, 3. https://doi.org/10.3390/healthcare11010003
Islam MI, Bagnulo S, Wang Y, Ramsden R, Wrightson T, Masset A, Colbran R, Edwards M, Martiniuk A. Job Satisfaction of Health Practitioners Providing Outreach Health Services during COVID-19 in Rural New South Wales (NSW) and the Australian Capital Territory (ACT), Australia. Healthcare. 2023; 11(1):3. https://doi.org/10.3390/healthcare11010003
Chicago/Turabian StyleIslam, Md Irteja, Sharif Bagnulo, Yiwen Wang, Robyn Ramsden, Trent Wrightson, Amanda Masset, Richard Colbran, Mike Edwards, and Alexandra Martiniuk. 2023. "Job Satisfaction of Health Practitioners Providing Outreach Health Services during COVID-19 in Rural New South Wales (NSW) and the Australian Capital Territory (ACT), Australia" Healthcare 11, no. 1: 3. https://doi.org/10.3390/healthcare11010003