
Impact of the Covid-19 Pandemic on Care of Patients with Diabetes Mellitus at Kitwe Teaching Hospital in 2021
Abstract:
Coronavirus disease 2019 (Covid-19) pandemic tested the
resilience of the health care system in many countries including Zambia. At the
peak, disruption of the global supply chain affected availability of essential commodities
needed to manage many health ailments like diabetes mellitus (DM). The study was
aimed to understand the challenges faced by DM patients in accessing specialist
services at KTH DM specialist clinic during the Covid-19 pandemic in 2021. A cross
sectional descriptive study was conducted with a total of 293 participants (109
males and 184 females) recruited using a designed structured questionnaire and results
analyzed using Microsoft Office Excel 2016 and the Statistical Package for Social
Sciences (SPSS) version 16.0 software. The mean age was 54.0 ± 13.0 years old with
78(26.6%) being below the age of 45 years. 197(67.2%) were married and 157(53.6%)
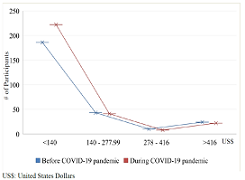
had primary education or less. 216(73.7%) and 222(75.8%) were earning <US$5.00
per day before and during Covid-19 pandemic respectively while the majority were
spending one fifth of their earned income on medication from private pharmacies
alone. 231(78.8%) had T2DM while 149(50.8%) had high plasma glucose levels; high
BMI, high waist circumference and hypertension 184(62.8%). The study suggested that
disruption of outpatient services led to patients presenting with high plasma glucose
levels, poorly controlled weight (high BMI and high waist circumference). Commonest
complications included hypertension and peripheral neuropathy. There is a need to
devise a more pragmatic and resilient healthcare system in future to minimize the
effects of any pandemic should they arise.
References:
[1] R.
(chair) et al. Williams, IDF Diabetes Atlas 9th. 2019.
[2] American
Diabetes Association, “Standards of Medical Care in Diabetes—2022 Abridged for
Primary Care Providers,” Clin. Diabetes, vol. 40, no. 1, pp. 10–38, Jan. 2022,
doi: 10.2337/cd22-as01.
[3] A. Ramachandran,
C. Snehalatha, E. Latha, M. Manoharan, and V. Vijay, “Impacts of urbanisation
on the lifestyle and on the prevalence of diabetes in native Asian Indian
population,” Diabetes Res. Clin. Pract., vol. 44, no. 3, pp. 207–213, Jun.
1999, doi: 10.1016/S0168-8227(99)00024-8.
[4] T. I.
A. SØrensen, “The changing lifestyle in the world: Body weight and what else?”
in Diabetes Care, 2000, vol. 23, no. SUPPL. 2.
[5] N. G.
Forouhi and N. J. Wareham, “Epidemiology of diabetes,” Medicine (Baltimore).,
vol. 38, no. 11, pp. 602–606, Nov. 2010, doi: 10.1016/j.mpmed.2010.08.007.
[6] S.
Mallapaty, “Evidence suggests the coronavirus might trigger diabetes,” Nature,
pp. 16–17, 2020.
[7] S.
Peric and T. M. Stulnig, “Diabetes and Covid-19,” Wien. Klin. Wochenschr., vol.
132, no. 13–14, pp. 356–361, Jul. 2020, doi: 10.1007/s00508-020-01672-3.
[8] L.
Marchand, M. Pecquet, and C. Luyton, “Type 1 diabetes onset triggered by Covid-19,”
Acta Diabetol., vol. 57, no. 10, pp. 1265–1266, Oct. 2020, doi:
10.1007/s00592-020-01570-0.
[9] S. Lou
Bailey et al., “Diabetes mellitus in Zambia and the Western Cape province of
South Africa: Prevalence, risk factors, diagnosis and management,” Diabetes
Res. Clin. Pract., vol. 118, pp. 1–11, 2016, doi:
10.1016/j.diabres.2016.05.001.
[10] Zambia
Statistical Agency, “The Zambia Statistical Agency (ZamStats).” https://www.zamstats.gov.zm
(accessed May 20, 2021).
[11] IMF,
World Economic Outlook: Recovery During a Pandemic, no. May. 2021.
[12] African
Development Bank (AfDB) Group, “Zambia Economic Outlook,” 2021. https://www.afdb.org/en/countries-southern-africa-zambia/zambia-economic-outlook
(accessed May 20, 2021).
[13] Zambia Ministry of Finance, “Annual Economic Report - 2019,” Lusaka, 2020. [Online]. Available: https://www.mof.gov.zm/?wpfb_dl=264.
A. Sharma, P. Gupta, and R. Jha, “Covid-19: Impact on Health Supply Chain and Lessons to Be Learnt,” J. Health Manag., vol. 22, no. 2, pp. 248–261, Jun. 2020, doi: 10.1177/0972063420935653.
[14] V.
Haldane et al., “Health systems resilience in managing the Covid-19 pandemic:
lessons from 28 countries,” Nat. Med., vol. 27, no. 6, pp. 964–980, Jun. 2021,
doi: 10.1038/s41591-021-01381-y.
[15] A. Sagan
et al., “Covid-19 and Health Systems Resilience: Lessons Going Forward,”
Eurohealth (Lond)., vol. 26, no. 2, pp. 20–24, 2020, [Online]. Available: https://apps.who.int/iris/bitstream/handle/10665/336290/Eurohealth.
[16] A.
Desta et al., “Impacts of Covid-19 on essential health services in Tigray,
Northern Ethiopia: A pre-post study,” PLoS One, vol. 16, no. 8, p. e0256330,
Aug. 2021, doi: 10.1371/journal.pone.0256330.
[17] M.
Zakoji and T. Sundararaman, “Emerging good practices and lessons learnt to
maintain essential health services during the Covid-19 pandemic,” WHO
South-East Asia J. Public Heal., vol. 10, no. 3, p. 26, 2021, doi:
10.4103/2224-3151.309868.
[18] Z.
Aranda et al., “Disruptions in maternal health service use during the Covid-19
pandemic in 2020: Experiences from 37 health facilities in low-income and
middle-income countries,” BMJ Glob. Heal., vol. 7, no. 1, pp. 1–10, 2022, doi:
10.1136/bmjgh-2021-007247.
[19] K.
Blanchet et al., “Protecting essential health services in low-income and middle-income
countries and humanitarian settings while responding to the Covid-19 pandemic,”
BMJ Glob. Heal., vol. 5, no. 10, pp. 1–9, 2020, doi: 10.1136/bmjgh-2020-003675.
[20] World
Health Organization, “Covid-19 continues to disrupt essential health services in
90% of countries,” 2021. https://www.who.int/news/item/23-04-2021-covid-19-continues-to-disrupt-essential-health-services-in-90-of-countries
(accessed May 20, 2021).
[21] World
Health Organization, “Nearly 1 in 5 Covid-19 deaths in the African region
linked to diabetes,” 2020. https://www.afro.who.int/news/nearly-1-5-covid-19-deaths-african-region-linked-diabetes
(accessed May 20, 2021).
[22] A. Huang
et al., “Clinical features of patients infected with 2019 novel coronavirus in
Wuhan, China,” Lancet, vol. 395, no. 10223, pp. 497–506, Feb. 2020, doi:
10.1016/S0140-6736(20)30183-5.
[23] A. Flyvbjerg,
“Pathogenesis of Microvascular Complications,” in Textbook of Diabetes,
Chichester, UK: John Wiley & Sons, Ltd, 2016, pp. 541–553.
[24] M.
Khamaisi, G. L. King, K. Park, and Q. Li, “Pathogenesis of Microvascular
Complications,” in Diabetes Complications, Comorbidities and Related Disorders,
2nd ed., Springer, Cham, 2020, pp. 161–201.
[25] M. J.
Fowler, “Microvascular and Macrovascular Complications of Diabetes,” Clin.
Diabetes, vol. 26, no. 2, pp. 77–82, Apr. 2008, doi: 10.2337/diaclin.26.2.77.
[26] Diabetes
Control and Complications Trial Research Group, “Effect of intensive diabetes
treatment on the development and progression of long-term complications in adolescents
with insulin-dependent diabetes mellitus: Diabetes Control and Complications
Trial,” J. Pediatr., vol. 125, no. 2, pp. 177–188, Aug. 1994, doi:
10.1016/S0022-3476(94)70190-3.
[27] UK
Prospective Diabetes Study (UKPDS) Group, “Effect of intensive blood-glucose
control with metformin on complications in overweight patients with type 2
diabetes (UKPDS 34),” Lancet, vol. 352, no. 9131, pp. 854–865, Sep. 1998, doi:
10.1016/S0140-6736(98)07037-8.
[28] Z. He
and G. L. King, “Microvascular complications of diabetes,” Endocrinol. Metab.
Clin. North Am., vol. 33, no. 1, pp. 215–238, Mar. 2004, doi:
10.1016/j.ecl.2003.12.003.
[29] G.
Rayman et al., “Guidelines for the management of diabetes services and patients
during the COVID‐19 pandemic,” Diabet. Med., vol. 37, no. 7, pp. 1087–1089,
Jul. 2020, doi: 10.1111/dme.14316.
[30] A.
Kazi and L. Blonde, Classification of diabetes mellitus, vol. 21, no. 1. 2001.
[31] M. A.
B. Khan, M. J. Hashim, J. K. King, R. D. Govender, H. Mustafa, and J. Al Kaabi,
“Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted
Trends,” J. Epidemiol. Glob. Health, vol. 10, no. 1, p. 107, 2019, doi:
10.2991/jegh.k.191028.001.
[32] H. A.
van Dam, F. G. van der Horst, L. Knoops, R. M. Ryckman, H. F. J. M. Crebolder,
and B. H. W. van den Borne, “Social support in diabetes: a systematic review of
controlled intervention studies,” Patient Educ. Couns., vol. 59, no. 1, pp.
1–12, Oct. 2005, doi: 10.1016/j.pec.2004.11.001.
[33] J. L.
Strom and L. E. Egede, “The Impact of Social Support on Outcomes in Adult
Patients with Type 2 Diabetes: A Systematic Review,” Curr. Diab. Rep., vol. 12,
no. 6, pp. 769–781, Dec. 2012, doi: 10.1007/s11892-012-0317-0.
[34] K. Y.
Chan, W. Cockshaw, K. Smith, E. Holmes-Truscott, F. Pouwer, and J. Speight,
“Social support and self-care outcomes in adults with diabetes: The mediating
effects of self-efficacy and diabetes distress. Results of the second diabetes
MILES – Australia (MILES-2) study,” Diabetes Res. Clin. Pract., vol. 166, p.
108314, Aug. 2020, doi: 10.1016/j.diabres.2020.108314.
[35] K. D.
Adam et al., “Factors affecting diabetes knowledge in Type 2 diabetic
veterans,” Diabetologia, vol. 46, no. 8, pp. 1170–1178, Aug. 2003, doi:
10.1007/s00125-003-1161-1.
[36] F.
Fernanda et al., “Relationship between knowledge, attitude , education and
duration of disease in individuals with diabetes mellitus,” Acta Paul Enferm,
vol. 25, no. 2, pp. 284–290, 2012.
[37] M.
Delamater, “Improving Patient Adherence,” Clin. Diabetes, vol. 24, no. 2, pp.
71–77, Apr. 2006, doi: 10.2337/diaclin.24.2.71.
[38] A.
Kalungia, M. Mwale, I. S. Sondashi, B. Mweetwa, P. Yassa, and G. Kadimba,
“Availability of Essential Antihypertensive and Antidiabetic Medicines in
Public Health Facilities in Lusaka District, Zambia,” Med. J. Zambia, vol. 44,
no. 3, pp. 140–148, 2017.
[39] H.
Kaiser, L. Hehman, B. C. Forsberg, W. M. Simangolwa, and J. Sundewall,
“Availability, prices and affordability of essential medicines for treatment of
diabetes and hypertension in private pharmacies in Zambia,” PLoS One, vol. 14,
no. 12, p. e0226169, Dec. 2019, doi: 10.1371/journal.pone.0226169.
[40] amnath
S. Ramanathan, “Correlation of duration, hypertension and glycemic control with
microvascular complications of diabetes mellitus at a tertiary care hospital,”
Integr. Mol. Med., vol. 4, no. 1, 2017, doi: 10.15761/IMM.1000272.
[41] S.
Zoungas et al., “Association of HbA1c levels with vascular complications and
death in patients with type 2 diabetes: evidence of glycaemic thresholds,”
Diabetologia, vol. 55, no. 3, pp. 636–643, Mar. 2012, doi:
10.1007/s00125-011-2404-1.
[42] T.-C.
Li et al., “Glycemic control paradox: Poor glycemic control associated with
higher one-year and eight-year risks of all-cause hospitalization but lower
one-year risk of hypoglycemia in patients with type 2 diabetes,” Metabolism,
vol. 64, no. 9, pp. 1013–1021, Sep. 2015, doi: 10.1016/j.metabol.2015.05.004.
[43] L.
Perreault et al., “Sex Differences in Diabetes Risk and the Effect of Intensive
Lifestyle Modification in the Diabetes Prevention Program,” Diabetes Care, vol.
31, no. 7, pp. 1416–1421, Jul. 2008, doi: 10.2337/dc07-2390.
[44] M. A.
M. Jacobs-van der Bruggen et al., “Cost-Effectiveness of Lifestyle Modification
in Diabetic Patients,” Diabetes Care, vol. 32, no. 8, pp. 1453–1458, Aug. 2009,
doi: 10.2337/dc09-0363.
[45] S.
Carlsson, N. Hammar, and V. Grill, “Alcohol consumption and type 2 diabetes,”
Diabetologia, vol. 48, no. 6, pp. 1051–1054, Jun. 2005, doi:
10.1007/s00125-005-1768-5.
