
E-Learning perception and satisfaction among health sciences students amid the COVID-19 pandemic
Abstract
BACKGROUND:
E-learning is increasingly used during the COVID-19 pandemic, however the impact of this change on students is not known. This study aimed to evaluate perception and satisfaction of health sciences students towards E-learning during the COVID-19 lockdown.
METHODS:
A structured questionnaire was distributed to 2000 health care students either through email or social media platforms. The questionnaire was divided into two sections: the first section addressed demographic information such as age, education level, course of study, number of lectures attended and country. The second section gathered information on perception and satisfaction of students using 13 close-ended questions. Frequencies and percentages were assessed for demographic data, perception and satisfaction level of students. The paired sample t-test, independent t test and Spearman correlation were applied to evaluate statistical significance between different variables of the study. A p-value of <0.05 was considered significant.
RESULTS:
Data from 1255 participants were included at a response rate of 66.4%. More than one third (37%) of the students took 25 or more online E-learning sessions and 47% preferred Zoom as an online platform. Participants belonged to 11 countries from developed and developing nations. 41% reported interference of E-learning due to network problems. 60% considered that clinical and practical skills are best learned in clinics and laboratories. More than one third of the students preferred classroom teaching and 34% of the students did not feel confident enough to take exit exams after E-learning sessions.
CONCLUSION:
E-learning satisfaction levels were better among developed countries (7.34) compared to developing countries (5.82). The majority of participants agreed that E-learning was satisfactory in acquiring knowledge, however not effective in acquiring clinical and technical skills. As the COVID-19 lockdown eases, there is a need for improvement in the methods employed in E-learning and more blended learning among healthcare students is recommended.
1Introduction
The spread of the coronavirus disease 2019 (COVID-19) caused by SARS-CoV 2 across the globe has led to profound changes in all aspects of human life including healthcare facilities, business opportunities, transportation and traveling, and social structure [1]. The education sector has not been immune to the effects of COVID-19, resulting in closure of schools and educational facilities in most affected countries for observing social distancing [2]. UNESCO estimates suggest that over 90% of the world’s students are not currently attending schools in the response to the pandemic, with over 1.5 billion learners affected [3]. However within these extraordinary times, one common trend is the increase in academic activities around the world using E-Learning, making a swift transition from place-based classes to virtual online learning systems [4]. The American Society for Training and Development defines E-learning as a broad set of applications and processes, which include web-based learning, computer-based learning, virtual classrooms, and digital contents. The definition of E-learning varies depending on the organization and how it is used, but at its core it involves electronic means of communication, education, and training [5].
Although online education is developing rapidly around the world, more applications of online education are used as a supplement to regular place-based school education. In the conventional education and teaching practice, more students go to schools to participate in traditional classroom teaching. However, during the COVID-19 pandemic, the luxury of using E-learning as an adjunct to traditional learning is not possible. The majority of schools and institutions worldwide are relying solely on virtual learning to fulfill their basic needs of education. Drawing the experience through previous crisis situations, adaptation of web-based learning and supporting continuation of educational activities through online classes has been effective and successful [6, 7]. Studies on E-learning have suggested multiple benefits including interaction between the teacher and learner with increased flexibility and versatility. E-learning sessions can be arranged at any day, place and time, and can reach a large audience irrespective of their location [7, 8]. However, there are certain prerequisites and possible limitations to the effective use of E-learning [9]. Brown et al. explained that any student seeking to enroll for E-learning program needs to invest in a range of minimum equipment including a personal computer, webcam, and a stable Internet connection [10]. As instruction medium is completely through the Internet, software and hardware dysfunction can totally compromise the sessions and interrupt the learning process [11]. In addition, teachers and students need a standard of training and knowledge of the technology being implemented in E-learning for effective teaching and learning. Else the benefits of E-learning will be limited to only those who are technology oriented [12].
The teaching and learning process among health care faculties including medicine, dentistry and other allied departments is diverse, a major part of which involves learning of clinical and technical skills in the wards, clinics and laboratories. It is critical in these times of the COVID-19 pandemic to assess how E-learning among health faculties is used as a sole way of teaching and instruction compares to place-, clinic- or laboratory-based learning. In addition, how the trend of E-learning influences perception, confidence and satisfaction among students is pivotal for the development of future health professionals. Although limited evidence shows E-learning courses to compare favorably with classroom instructions with good satisfaction levels among students [13, 14], investigations on the perception and satisfaction of E-learning among health sciences students during the COVID-19 pandemic is not available. It is hypothesized the health students will exhibit satisfaction towards E-learning and training during the pandemic. Therefore the aim of the present study was to assess the experience, perception and satisfaction among students in health science faculties towards E-learning.
2Methods
2.1Study setting and sample
This qualitative survey was conducted during the months of March and April 2020, to assess the perception and satisfaction of medical students regarding E-learning during the COVID-19 pandemic. The institutional ethics and review committee approved the study. A well-structured questionnaire was designed with a discussion with senior teaching faculty. A pilot study using the questionnaire was carried out on 50 participants to validate and assess internal consistency of items showing intra-class correlation of 0.75. The sample size was identified using means and standard deviations from previous studies and a maximum of 2000 health sciences student participants were approached to test their perception and satisfaction of E-learning during the COVID-19 pandemic [15–18]. A conscious effort was made by the investigators to identify and forward (through networking websites) the survey questionnaire among participants belonging to developed and developing countries in equality.
2.2Questionnaire
The objective of the study was included in the questionnaire and all participants agreed to consent statement for voluntary participations and declarations of anonymity and confidentiality prior to participation. The questionnaire was divided into two sections. The first section addressed the demographic features of the cohort including age, education level, education course, education year, number of E-lectures attended and country. The second section was designed to gather information regarding the experience and perception of E-learning among the students. For that purpose, a total of 13 close ended questions were created and response options comprised of a Likert scale; Strongly agree, agree, neutral, disagree, strongly disagree, and not applicable. The questions assessed, commonly used online platform used for E-learning in the COVID-19 pandemic, previous experience, common problems encountered, comparison of theoretical knowledge and clinical and technical skill learning through E-learning and comparison of E-learning and class-room learning. Some questions addressed outcomes of E-learning including timely teachers response, feedback regarding assignments, scheduling and management of sessions, student’s confidence in taking examinations and to practice on patients and preference of blended learning (E-learning, clinics, classroom). Using a visual analog scale (VAS), the satisfaction among students regarding the switch to E-learning from traditional teaching and learning was assessed.
2.3Data collection
The questionnaire was uploaded on Google Surveys (www.surveys.google.com) and the link to the survey was sent to different health sciences student networks through emails and social media platforms (WhatsApp, Facebook, LinkedIn and Twitter). All the undergraduate and postgraduate students currently studying in health sciences (medical and dental) or other allied sciences were included in the study. The data obtained was tabulated using statistical program for social sciences (SPSS, IBM version 25) for statistical analysis. Frequency and percentages were calculated for demographics features and responses to questions. The paired sample t test, independent t test and Spearman correlation were applied to find statistical difference between different variables of the study. The level of significance was set to P < 0.05.
3Results
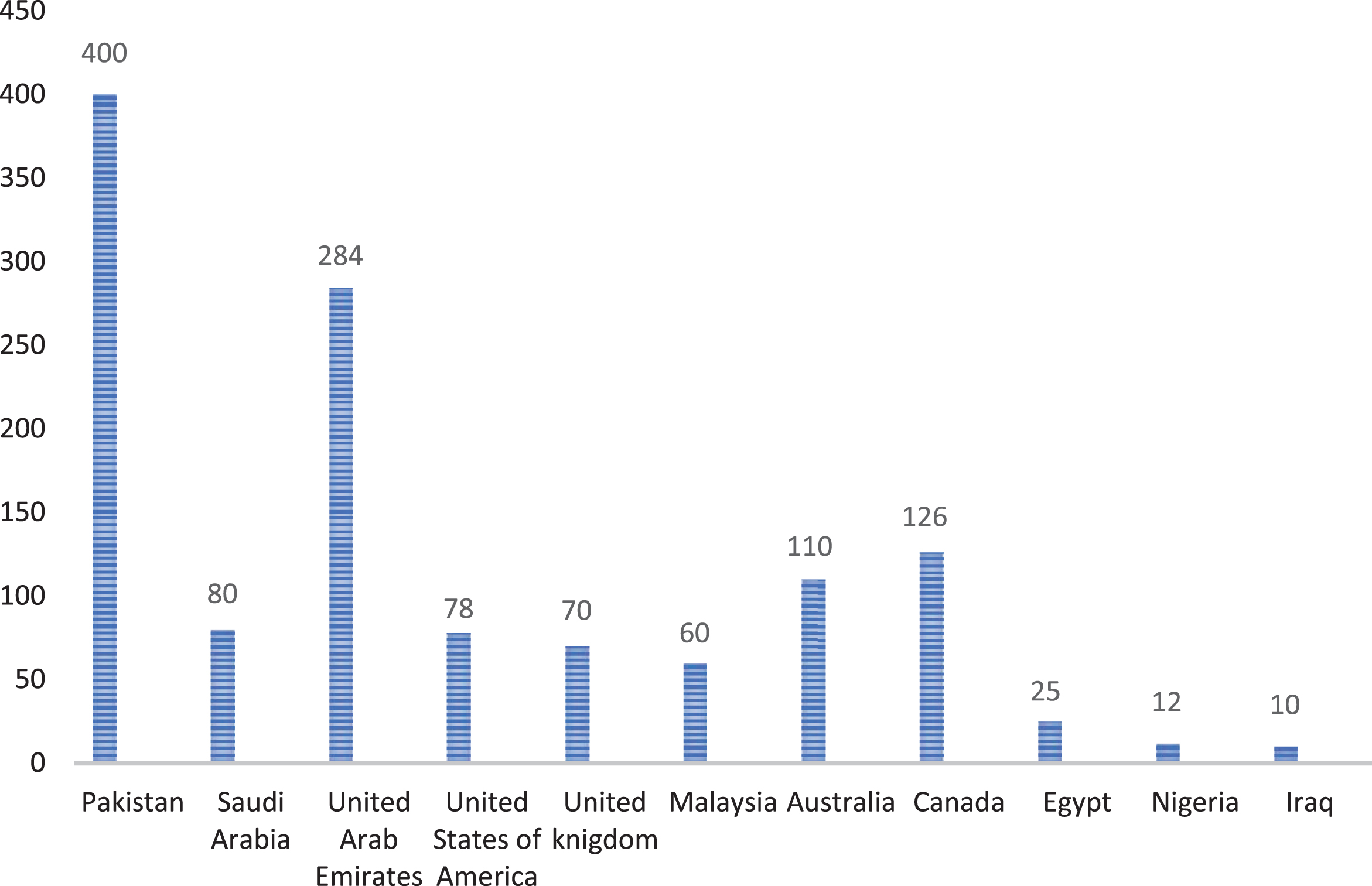
A total of 1328 students from health science colleges/institutes of 11 developed and developing countries around the globe participated in the study at a response rate of 66.4%. 73 questionnaires were excluded due to duplication or deficiency and 1255 responses were included in the assessment. The general characteristics of the cohort are presented in Table 1. Out of the total 1255 participants, 368 (29.3%) were males and 887 (70.6%) females, with 71% belonging to a common age group (18 and 22 years). Regarding the level of education, 89% were undergraduate and 11% were postgraduate students, 57.3% were bachelor students of dental surgery (BDS), 34.9% were bachelor students in medicine and the remaining students belonged to nursing, dental care professionals, pharmacy, occupational therapists and medical technicians. Moreover, Zoom (47%) was the most commonly used platform for E-learning followed by Google Hangouts (29%), however online registered university portals were used in only 11% of the cases. More than 53% of the participants were from developed countries (UAE, USA, UK, Australia and Canada) while nearly 47% belonged to developing countries (Egypt, Iraq, Malaysia, Nigeria, Pakistan and Saudi Arabia) (Fig. 1).
Table 1
Characteristics of the study participants (n = 1255)
| Number (%) | ||
| Gender | Male | 368(29) |
| Female | 887(71) | |
| Age group | 18 –22 | 897(71) |
| 23 –27 | 260(21) | |
| 28 –32 | 61(5) | |
| 33 –37 | 26(2) | |
| 38 –42 | 11(1) | |
| Education level | Undergraduate | 1119(89) |
| Postgraduate | 136(11) | |
| Education year | 1st year | 334(27) |
| 2nd year | 146(11) | |
| 3rd year | 271(22) | |
| 4th year | 288(23) | |
| 5th year | 164(13) | |
| Post grad | 48(4) | |
| Field of education | BDS (Dentistry) | 720(57) |
| MBBS (Medicine) | 438(34) | |
| FCPS (Fellowship) | 12(1) | |
| DPT (Diploma) | 40(3) | |
| MSc (Masters) | 7(1) | |
| MBA (Masters) | 10(1) | |
| Others | 23(2) | |
| Education sector | Private | 839(89) |
| Government | 416(11) | |
| Number of online sessions attended | <10 | 367(29) |
| 10–15 | 163(13) | |
| 16–20 | 142(11) | |
| 21–25 | 118(10) | |
| >25 | 465(37) | |
| Type of platform for E-learning | Google Hangouts | 365(29) |
| Zoom | 589(47) | |
| Online University Portal/ | 95(8) | |
| Recorded lectures | ||
| Moodle | 137(11) | |
| Microsoft Team | 42(3) | |
| Others | 27(2) |
Fig. 1
Geographic distribution of the students included in the study (n = 1255).
More than 36% of the respondents had prior experience of E-learning and an excess of 60% agreed that networking issues were common hindrance for E-learning (Table 2). 40% of the students accepted E-learning as a good medium for acquiring theoretical knowledge; however almost 42% of the students did not consider E-learning useful for developing clinical and technical skills. Nearly 52% of the students were satisfied with timely response from teachers, however, more than 45% were satisfied with the feedback on assessment and assignments. 69% of the participants approved that it took more effort staying home and keeping up with course schedules and deadlines during the pandemic lockdown. Nearly 75% of the students considered clinics and laboratory environment as more effective than E-learning for acquiring clinical and technical skills. More than half of the participants did not favor E-learning to classroom teaching based on level of interest, focus and lack of distractions.
Table 2
Experience and perception of E-learning by health sciences students (n = 1255)
| Strongly agree % | Agree % | Neutral % | Disagree % | Strongly disagree % | Not applicable % | |
| EL experience prior to pandemic was useful | 14.1 | 22.0 | 30.1 | 8.0 | 6.2 | 19.6 |
| Poor Internet connection is a hindrance for EL | 40.7 | 28.4 | 17.1 | 6.1 | 4.1 | 2.7 |
| EL is good for theoretical knowledge | 14.4 | 26.9 | 29.0 | 15.2 | 12.4 | 2.2 |
| EL is good for clinical and practical skills | 4.2 | 9.2 | 12.8 | 23.3 | 41.4 | 9.0 |
| Teachers’ response to questions is timely | 18.1 | 34.0 | 223.6 | 11.7 | 7.9 | 4.7 |
| Teachers provide feedback on exams and assignments | 13.9 | 31.7 | 27.7 | 12.2 | 9.4 | 5.0 |
| Difficult to manage E-learning schedule during pandemic | 44.6 | 24.5 | 14.9 | 7.4 | 6.5 | 2.2 |
| Learning of clinical/practical skills in a clinic/lab setup is effective | 60.0 | 14.7 | 8.0 | 4.4 | 10.3 | 2.6 |
| EL allows learning environment as the traditional classroom learning | 5.9 | 10.2 | 17.0 | 27.1 | 35.9 | 3.9 |
| I am confident to practice on patients after E-learning | 4.0 | 7.4 | 13.1 | 22.0 | 45.3 | 8.2 |
| I am confident to sit exams after taking online sessions | 5.9 | 10.8 | 21.8 | 21.3 | 34.6 | 5.7 |
| Would prefer blended learning (classroom, clinics, E-learning) | 22.0 | 24.1 | 21.5 | 14.1 | 15.5 | 2.8 |
EL. E-learning.
More than 75% of the students were not confident to manage patients on returning to health facilities post pandemic without practical and hands-on clinical sessions. Nearly two third of the students were not confident to take examinations based on E-learning sessions. Nearly half of the participant preferred incorporation of blended learning (classroom, clinics, E-learning) in their courses post-pandemic for better outcomes.
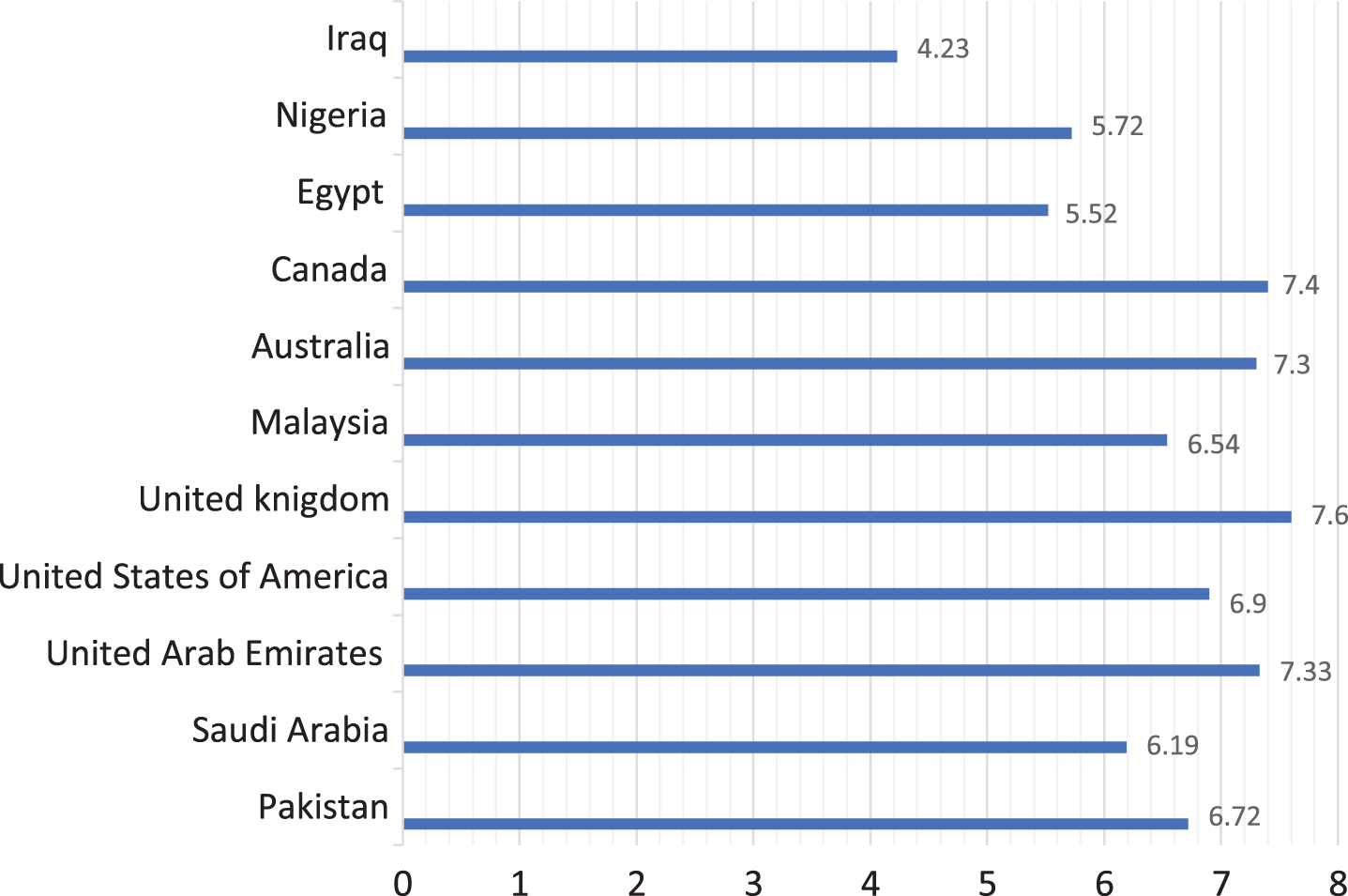
The perception and experience of E-learning in developed countries was significantly different compared to developing countries (p < 0.05). In addition, the level of satisfaction as determined using VAS was significantly higher in developed countries (7.34) as compared to developing countries (5.82) (p < 0.05) (Fig. 2). Experience of E-learning was significantly higher in students from developed as compared to developing country students (p < 0.05). The prior experience of E-learning was comparable among the students from different fields of education (p > 0.05). Among the general characteristics, level of education and field of education exhibited a significant influence on the perception and satisfaction of E-learning among students (p < 0.05). Students with increased number of attended E-learning sessions showed significantly better experience and perception (positive correlation) during the COVID-19 pandemic (r = 0.07). The education level did not show a significant influence (P = 0.12) on student confidence in examination and patient management.
Fig. 2
Geographic distribution of the satisfaction level of E-learning among students (n = 1255)
4Discussion
As E-learning is the dominant method of academic activities among health students during the COVID-19 pandemic, it is pivotal to assess its perception and satisfaction among students, to identify flaws, improve quality and revise policies from a student’s perspective. Therefore the present study aimed to assess the perception and satisfaction among students in health science faculties towards E-learning during the COVID-19 pandemic. Although E-learning is a beneficial tool for conducting academic activities for students in their opinion, an overall satisfaction score (VAS) of less than 7 was observed among students.
In the present study the overall response rate was low at 66.4%. Surveys conducted through online platforms and emails are reported to show lower response rates compared to hand distributed surveys; in some cases as low as 50% [15, 16]. An interesting finding in the present study was the preferred use of Zoom platform by nearly half of the participants. Zoom was initially launched as a business meeting platform, however it has gained popularity in its application in academics. Comparatively, another popular platform being increasingly used is Moodle, however it was the third most commonly used platform (11%) by students in the present survey. Moodle is reported to offer the novelty of assessing targeted audience, benefit of teaching clinical skills, high number of interactions and enhanced tools [19, 20]. In the authors’ view Zoom was preferred due to its user-friendly interface, versatility, and ease of integration with different hardware.
In contrast to place-based learning in person, E-learning is dependent on accessibility and functionality of technological gadgets (Personal computers, Laptops, Tablets and Smart phones) and an incessant Internet connection [21]. 40% of the students attributed interruptions of Internet connections as a compromise in E-learning. This is in line with previous studies associating connectivity issues to limited use of E-learning [22]. More than 40% of the students accepted E-learning as a medium for acquiring theoretical knowledge; however a similar percentage did not consider E-learning useful for developing clinical and technical skills. By contrast, a study among medical students by Gormley et al. reported E-learning just as highly as other traditional methods for clinical skill teaching [23]. Other studies have reported similar outcomes [24]. Explanations for the findings in the present study could be related to the unavailability of proper stimulant (patient) or appropriate gear and instruments. However, Gormley et al. suggested the use of E-learning in a blended approach, similar to present study findings [23]. Interestingly, among medical students it is also suggested that use of mixed learning approach with virtual clinical case studies with different styles and modes, not only facilitate learning but also brings a positive change in practice [25, 26]. A majority of participants appreciated E-learning for timely response and feedback from teachers on assignments and assessments. This showing efficacy of teaching methods that define goals, allow interaction of teachers and peers and provide prompt feedback [27].
E-learning has shown to improve student motivation and concentration levels, better rate of assignment submissions then traditional teaching, and higher convenience and student attendance [28–30]. However, in the present study, a majority of the students showed displeasure in keeping up with course schedules and deadlines during the pandemic lockdown. This could be due to the immediate social isolation imposed in the pandemic, resulting in low motivation levels and other psychological problems. Studies have suggested that college students have suffered from anxiety symptoms in the COVID-19 pandemic and there is a need for monitoring of mental health among college student during this period [31]. In addition, E-learning can promote isolation, as Kheng et al. suggested that the lack of face-to-face interaction contributes to professional isolation and decreased learning experiences [32]. Self-isolation also aggravates lack of self-discipline, compromises learning environment and create lack of suitable learning material [33]. In the present study, the majority of students who did not find the self-isolated environment during the pandemic conducive for academics and learning reflected this.
A possible influence of E-learning in comparison to traditional learning for improvement in clinical skills and outcomes for health professionals has been investigated in multiple studies [34]. However, cumulative evidence concludes that it is uncertain if E-learning improves or reduces health professional skills [34]. A majority of the students in the present study did not feel confident to clinically manage patients as an outcome of E-learning. However, E-learning has shown to motivate students to join clinical attachments and practice their clinical skills on patients [23]. Furthermore, nearly half of the participants in the present study preferred blended learning (E-learning with traditional learning) for improving knowledge and patient management. Blended learning combines the structured high quality content of E-learning, which allows students to fill gaps in their knowledge, and through tutorials with teachers they can identify these gaps [30]. Therefore students do not want to see complete replacement of academic activities with online learning [23, 30]. The overall satisfaction level of E-learning among developed countries was significantly higher, with a positive correlation with prior experience of E-learning. These findings suggest that students in developed countries (including USA, UK, Canada) are well trained and equipped in methods of E-learning and virtual medium of education. In the developed world, E-learning methods gained popularity in undergraduate medical education in the 2000 s [35]. With continuous improvements these electronic teaching and learning methods have become an integral part of the academic system. Within developing countries E-learning still needs rapid progress and development, and the lack of resources, infrastructure and training could be associated with its low efficacy [33, 36].
It is pertinent to mention that student psychological behavior along with the customized correlation of clinical skills to E-learning was not assessed in the present study. However, these findings suggest that E-learning is an effective means of education among health care students during the COVID-19 pandemic. However, E-learning process needs drastic improvements with emphasis on clinical skill development through innovative electronic methods of learning. Regular training with update of software’s and technological methods with emphasis on familiarizing with platforms used in E-learning should be at student’s disposal [37, 38]. In addition as the study findings reflect psychological distress among students, counseling sessions for monitoring and managing mental health issues among students are required. Therefore, further studies relating specific procedural skills of health trainees and their psychological conduct to E-learning are recommended. As authorities start to ease the lockdown, blended learning combining structured E-learning with tutorials and case-based learning on the premises should be implemented.
5Conclusion
E-learning satisfaction levels were better among developed country students (7.34) compared to students from developing countries (5.82). A majority of participants agreed that E-learning was satisfactory in acquiring knowledge, however not effective in acquiring clinical and technical skills. There is a need for improvement in the methods employed in E-learning and a move towards blended learning among healthcare students as the COVID-19 lockdown eases is required. Monitoring and management of psychological distress among students through counseling is recommended for improving academic outcomes.
Authorship contribution
MA and NA: Conceptualization, methodology, supervision, investigation, software, data curation, writing - original draft.
FV and TAJ: Investigation, questionnaire design and distribution, data curation, writing and revision of manuscript.
AA and RSA: Investigation, writing and revision of manuscript, data inference, data assessment.
BS and SS: Data collection, data analyses, data inference.
ShS: Questionnaire design, questionnaire validity, data curation, manuscript writing.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
The authors are grateful to the Researchers Supporting Project at King Saud University for the funding through project no. RSP-2019-44.
References
[1] | Montemurro N . The emotional impact of COVID-19: From medical staff to common people. Brain Behav Immun 2020. doi: 10.1016/j.bbi.2020.03.032 |
[2] | Bayham J , Fenichel EP . Impact of school closures for COVID-19 on the US health-care workforce and net mortality: a modelling study. Lancet Public Health. (2020) ;5: :e271–e278. |
[3] | UNESCO, United Nations Educational, Scientific and Cultural Organization COVID-19 educational disruption and response. https://en.unesco.org/themes/education-emergencies/coronavirus-school-closures(2020), Accessed 19th Mar 2020. |
[4] | Murphy MP . COVID-19 and emergency eLearning: Consequences of the securitization of higher education for post-pandemic pedagogy. Contemp Sec Policy. (2020) ;1: :1–4. |
[5] | Nedeva V , Dimova E . Some advantages of e-learning in English language training. Trakia J Sci. (2010) ;8: :21–28. |
[6] | Franchi T . The Impact of the Covid-19 Pandemic on Current Anatomy Education and Future Careers: A Student’s Perspective. Anat Sci Educ. (2020) doi: 10.1002/ase.1966 |
[7] | Nortvig AM , Petersen AK , Balle SH . A Literature Review of the Factors Influencing E-Learning and Blended Learning in Relation to Learning Outcome, Student Satisfaction and Engagement. Electr J E-learning. (2018) ;16: :46–55. |
[8] | Ryan S , Kaufman J , Greenhouse J , She R , Shi J . The effectiveness of blended online learning courses at the community college level. Comm Coll J Res Pract. (2016) ;40: :285–98. |
[9] | Roe D , Carley S , Sherratt C . Potential and limitations of e-learning in emergency medicine. Emerg Medic J. (2010) ;27: :100–4. |
[10] | Brown DG , Burg JJ , Dominick JL . A strategic plan for ubiquitous laptop computing, Communications of the ACM. (1998) ;41: :26–35. |
[11] | Wong D . A critical literature review on e-learning limitations. J Advance Sci Arts. (2007) ;2: :55–62. |
[12] | Basilaia G , Dgebuadze M , Kantaria M , Chokhonelidze G . Replacing the Classic Learning Form at Universities as an Immediate Response to the COVID-19 Virus Infection in Georgia. Int J Res App Sci Eng Tech. (2020) ;8: :101–8. |
[13] | Wutoh R , Boren SA , Balas EA . E-Learning: a review of Internet-based continuing medical education. J Contin Edu Health Profes. (2004) ;24: :20–30. |
[14] | Cook DA , Levinson AJ , Garside S , Dupras DM , Erwin PJ , Montori VM . Internet-based learning in the health professions: a meta-analysis. JAMA. (2008) ;300: :1181–96. |
[15] | Nulty D . The adequacy of response rates to online and paper surveys: What can be done. Assess Eval High Educ. (2008) ;33: :301–14. |
[16] | Vohra F , Habib R . Knowledge and attitude of dentists toward implant retained restorations in Saudi Arabia. Niger J Clin Prac. (2015) ;18: :312–7. |
[17] | Ahmed N , Shakoor M , Vohra F , Abduljabbar T , Mariam Q , Rehman MA . Knowledge, Awareness and Practice of Health care Professionals amid SARS-CoV-2, Corona Virus Disease Outbreak Pak J Med Sci. (2020) ;36: :S4. |
[18] | Vohra F , Bukhari IA , Sheikh SA , Albaijan R , Qureshi AH , Arif Z , Akram Z . Knowledge, behavior and attitudes of dental practitioners towards photodynamic therapy use in dental practice. Photo Photodyn Ther. (2017) ;20: :221–6. |
[19] | Umek L , Keržič D , Aristovnik A , Tomaževič N . Analysis of selected aspects of students’ performance and satisfaction in a Moodle-based e-learning system environment. Eurasia J Math Sci Tech Edu. (2015) ;11: :1495–505. |
[20] | Luo L , Cheng X , Wang S , Zhang J , Zhu W , Yang J , Liu P . Blended learning with Moodle in medical statistics: an assessment of knowledge, attitudes and practices relating to e-learning. BMC Med Edu. (2017) ;17: :170. |
[21] | Linjawi AI , Alfadda LS . Students’ perception, attitudes, and readiness toward online learning in dental education in Saudi Arabia: a cohort study. Adv Med Edu Prac. (2018) ;9: :855. |
[22] | Frehywot S , Vovides Y , Talib Z , Mikhail N , Ross H , Wohltjen H , Bedada S , Korhumel K , Koumare AK , Scott J . E-learning in medical education in resource constrained low-and middle-income countries. Human Res Health. (2013) ;11: :4. |
[23] | Gormley GJ , Collins K , Boohan M , Bickle IC , Stevenson M . Is there a place for e-learning in clinical skills? A survey of undergraduate medical students’ experiences and attitudes. Med Teach. (2009) ;31: :e6–12. |
[24] | Maertens H , Madani A , Landry T , Vermassen F , Van Herzeele I , Aggarwal R . Systematic review of e-learning for surgical training. B J Surg. (2016) ;11: :1428–37. |
[25] | Ikram UZ , Essink-Bot M , Suumond J . How we developed an effective e-leaning module for medical students on using professional interpreters. Med Teach. (2015) ;37: :422–7. |
[26] | Khasawneh R , Simonsen K , Snowden J , Higgins J , Beck G . The effectiveness of e-learning in pediatric medical student education. Med Educ Online. (2016) ;21: :29516. |
[27] | Fredricks JA . Engagement in school and out-of-school contexts: A multidimensional view of engagement. Theory Prac. (2011) ;50: :327–35. |
[28] | Rodrigues H , Almeida F , Figueiredo V , Lopes SL . Tracking e-learning through published papers: A systematic review. Comp Educ. (2019) ;136: :87–98. |
[29] | Bhuasiri W , Xaymoungkhoun O , Zo H , Rho JJ , Ciganek AP . Critical success factors for e-learning in developing countries: A comparative analysis between ICT experts and faculty. Computers & Education. (2012) ;58: (2):843–55. |
[30] | Morton CE , Saleh SN , Smith SF , et al. Blended learning: how can we optimise undergraduate student engagement? BMC Med Edu. (2016) ;16: :195. |
[31] | Cao W , Fang Z , Hou G , Han M , Xu X , Dong J , Zheng J . The psychological impact of the COVID-19 epidemic on college students in China, Psychiatry Res. 34. (2020) ;6: :112934. doi: 10.1016/j.psychres.2020.112934.Epub 2020 Mar 20. |
[32] | Kheng S . The challenges of upgrading from ISPO Category II level to Bachelor Degree level by distance education. Prosthet Orthot Int. (2008) ;32: :299–312. |
[33] | Bao W . COVID-19 and online teaching in higher education: A case study of Peking University. Human Behav Emerg Techn. (2020). |
[34] | Vaona A , Banzi R , Kwag KH , Rigon G , Cereda D , Pecoraro V , Tramacere I , Moja L . E-learning for health professionals. Cochrane Database Syst Rev. 2018;1. |
[35] | Cook J . Reviewof virtual learning environments in UK medical, dental and veterinary education. Higher Edu Acad Med Den Vet Med. (2005). |
[36] | Oye ND , M Salleh M , Iahad NA . Challenges of e-learning in Nigerian university education based on the experience of developed countries. Int J Manag Inform Tech. (2011) ;3: :39–48. |
[37] | Cook DA . Web-based learning: pros, cons and controversies. Clin Med. (2007) ;7: :37. |
[38] | Childs S , Blenkinsopp E , Hall A , Walton G . Effective e-learning for health professionals and students—barriers and their solutions, A systematic review of the literature—findings from the HeXL project. Health Info Lib J. (2005) ;22: :20–32. |

