
Addressing Different Needs: The Challenges Faced by India as the Largest Vaccine Manufacturer While Conducting the World’s Biggest COVID-19 Vaccination Campaign

Abstract
:1. Introduction
Current Situation in India
2. Materials and Methods
3. Results
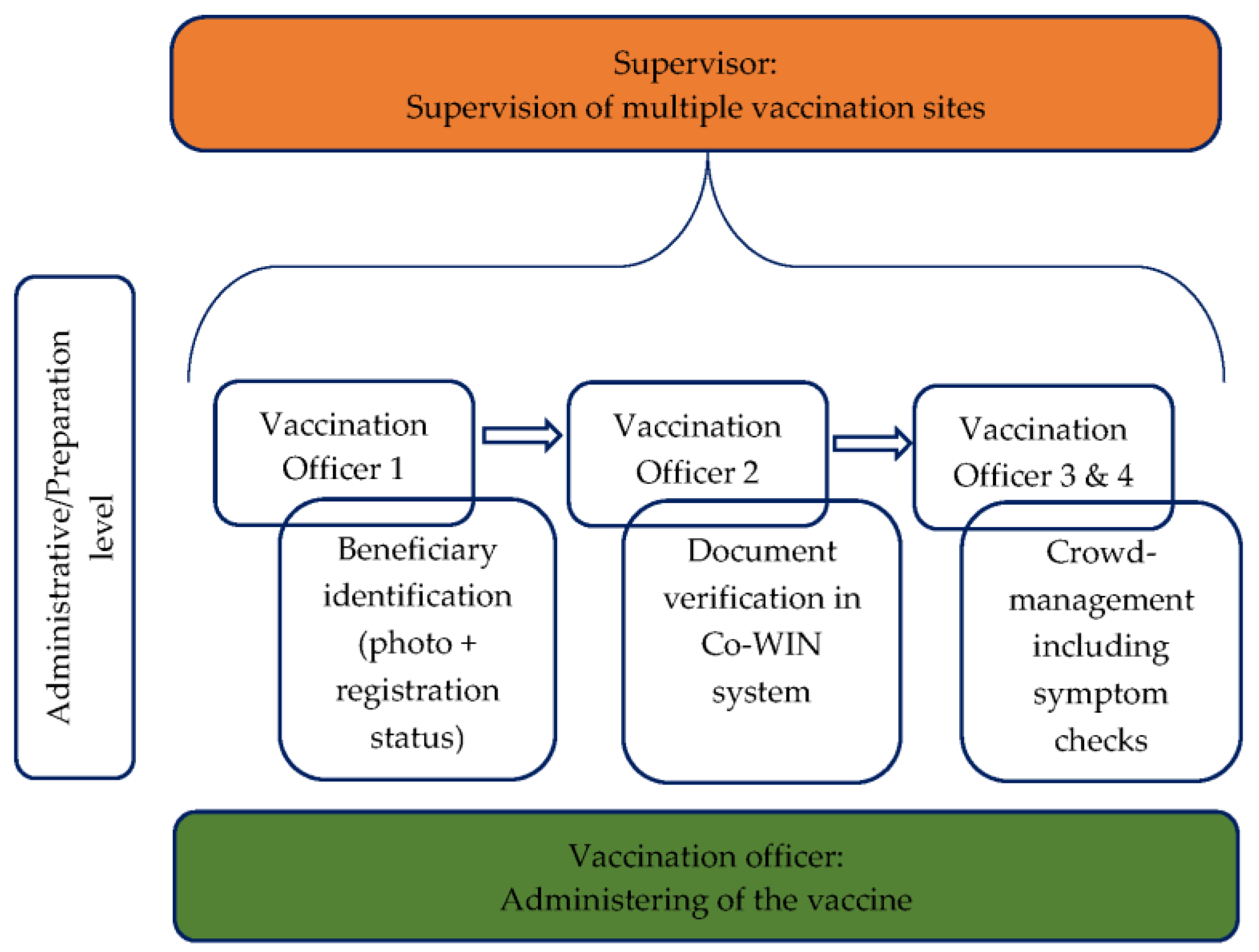
3.1. Vaccination Strategy
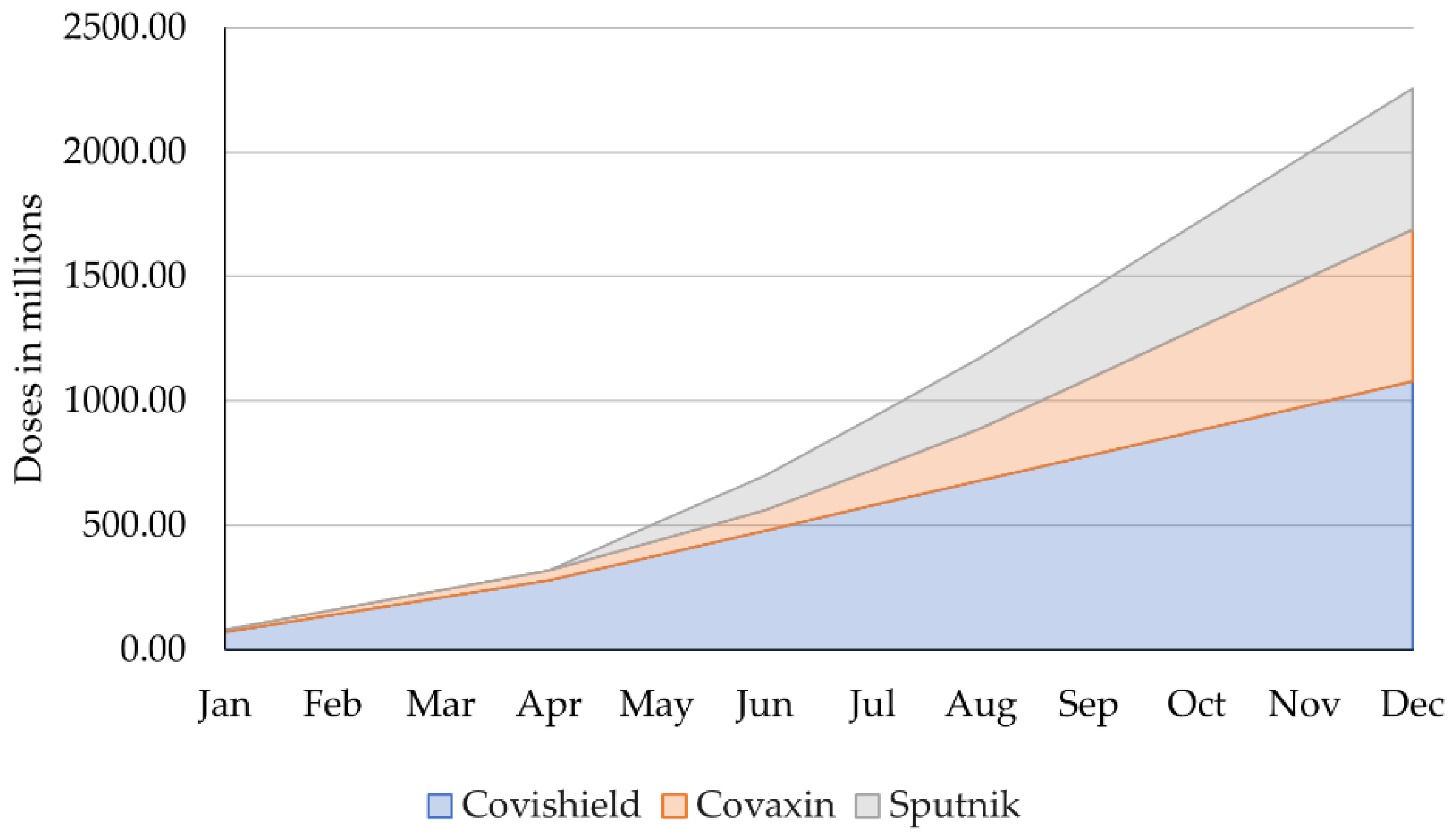
3.2. Vaccine Manufacturing
- Financial support for vaccine producers;
- Institutional help for vaccine producers throughout the drug development cycle;
- Optimized pathway to vaccine approval;
- Boost of production through ‘out-of-the-box’ solutions [41].
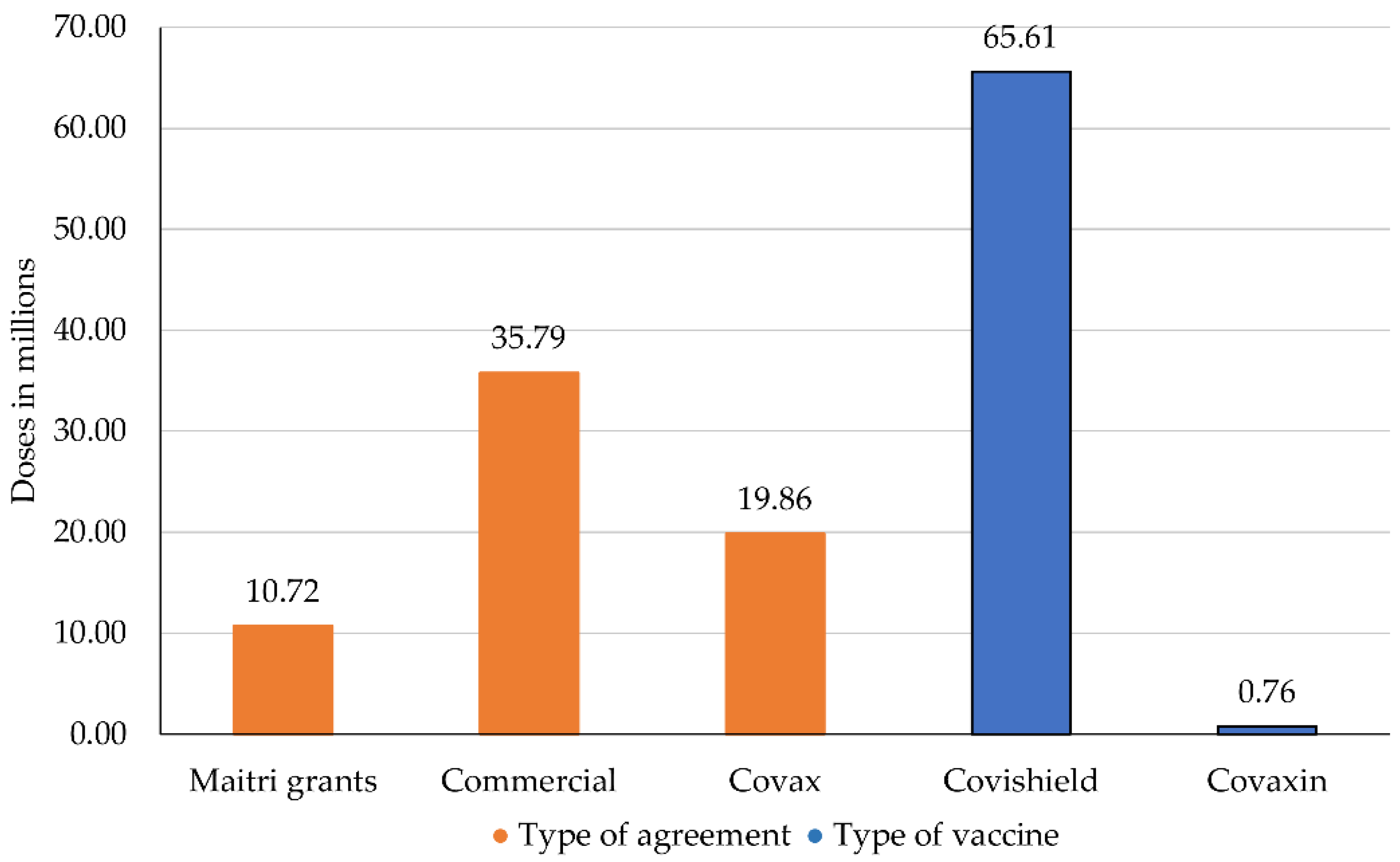
3.3. Vaccine Exports: International Contracts and Relations
4. Discussion
4.1. Scenario 1: Production Capacity Increased as Promised
4.2. Scenario 2: The Production Remains as It Was until April 2021
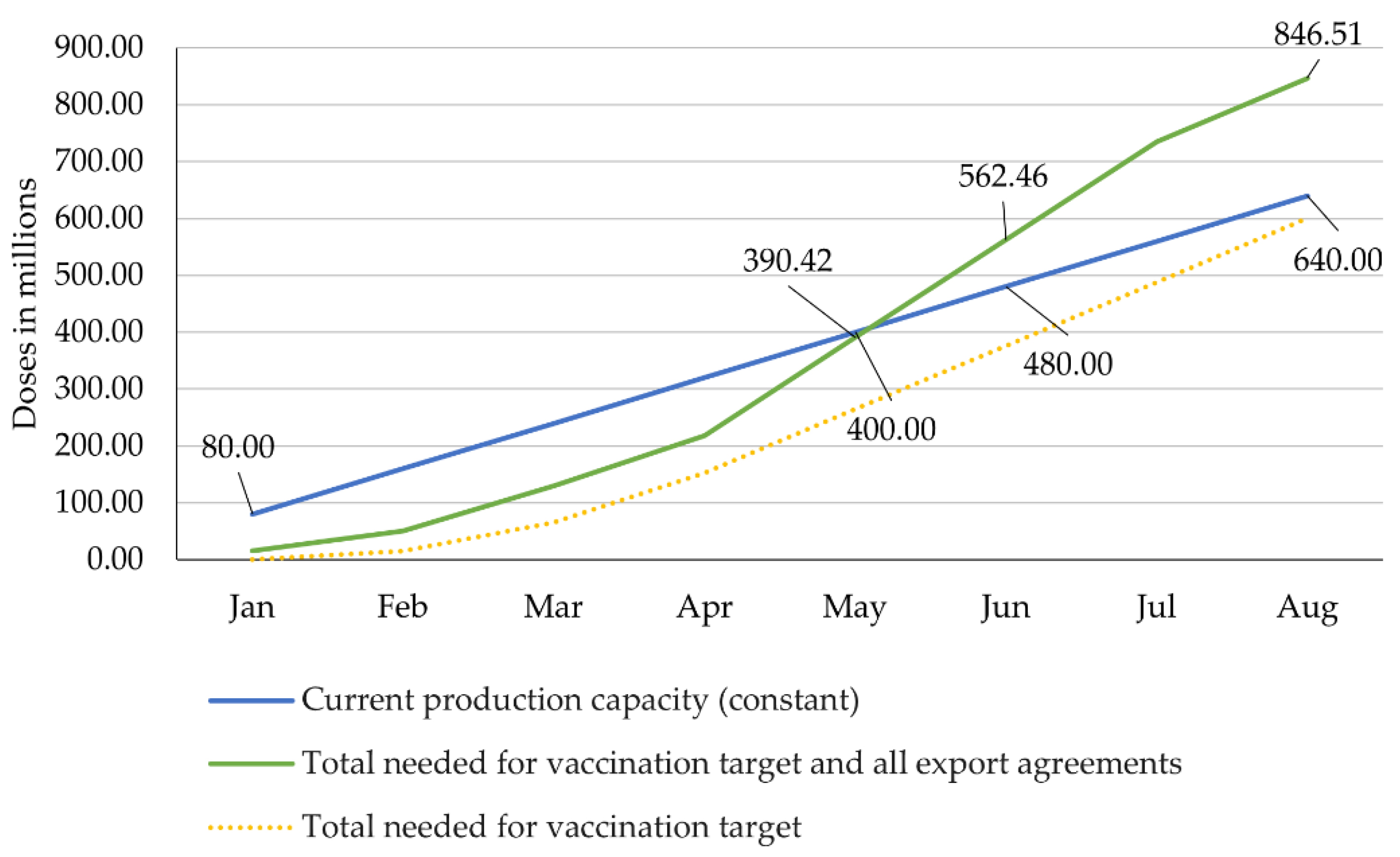
4.2.1. Scenario 2.1: Constant Production Capacity vs. Fulfilment of Vaccination Target and All Export Agreements
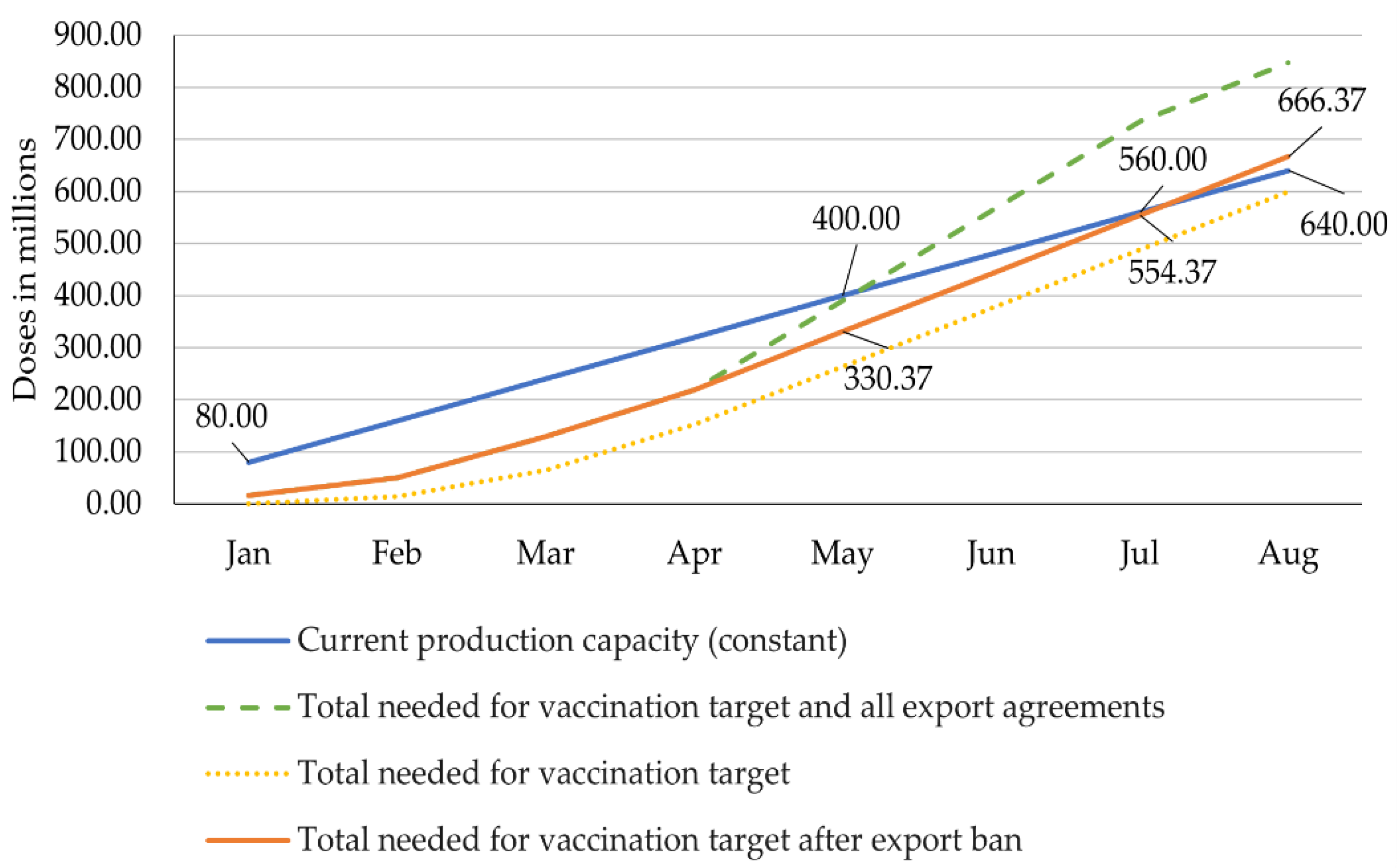
4.2.2. Scenario 2.2: Constant Production Capacity vs. Vaccine Needs after Export Ban in April
4.3. Limitations
5. Conclusions
- if it does, the vaccination target and all the export agreements will be accomplished (Figure 4);
- if it does not, the country will face severe shortage in June at the latest and will not meet either the internal or the export needs (Figure 5), or;
- if it does not accelerate, but the ban of exports introduced at the end of April continues, the country will still face a shortage in August, which can be avoided with a small increase in production capacity so that the country achieves its vaccination target (Figure 6).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- The World Bank Data. Population, Total—India. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=IN (accessed on 29 April 2021).
- OECD. DAC List of ODA Recipients. Available online: https://www.oecd.org/dac/financing-sustainable-development/development-finance-standards/DAC-List-ODA-Recipients-for-reporting-2021-flows.pdf (accessed on 29 April 2021).
- Indian Brand Equity Foundation. Pharmaceuticals. Available online: https://www.ibef.org/download/Pharmaceuticals-January-2021.pdf (accessed on 30 April 2021).
- OECD. Economic Policy Reforms 2021: Going for Growth Country Note India. Available online: https://www.oecd.org/economy/growth/India-country-note-going-for-growth-2021.pdf (accessed on 30 April 2021).
- World Health Organization. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline#! (accessed on 29 April 2021).
- Andrews, M.A.; Areekal, B.; Rajesh, K.R.; Krishnan, J.; Suryakala, R.; Krishnan, B.; Muraly, C.P.; Santhosh, P.V. First confirmed case of COVID-19 infection in India: A case report. Indian J. Med Res. 2020, 151, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Immigration. Advisory: Travel and Visa Restrictions Related to COVID-19. Available online: https://boi.gov.in/content/advisory-travel-and-visa-restrictions-related-covid-19 (accessed on 30 April 2021).
- Ministry of Health and Family Welfare. Advisory on Social Distancing Measure in View of Spread of COVID-19 Disease. Available online: https://www.mohfw.gov.in/pdf/SocialDistancingAdvisorybyMOHFW.pdf (accessed on 30 April 2021).
- Press Information Bureau—Government of India. Government of India Issues Orders Prescribing Lockdown for Containment of COVID-19 Epidemic in the Country. Available online: https://www.mha.gov.in/sites/default/files/PR_NationalLockdown_26032020_0.pdf (accessed on 30 April 2021).
- Ministry of Health and Family Welfare. Dashboard. Available online: https://www.mohfw.gov.in/ (accessed on 30 April 2021).
- The BBC. Zydus Cadila: What We Know about India’s New Covid Vaccine. Available online: https://www.bbc.com/news/world-asia-india-55748124 (accessed on 18 April 2021).
- The Times of India. Covid-19: India Records Highest-Ever 401,993 New Cases, 3523 Deaths. Available online: https://timesofindia.indiatimes.com/india/covid-19-india-records-highest-ever-401993-new-cases-3523-deaths/articleshow/82339160.cms (accessed on 30 April 2021).
- Gentleman, J.; Venugopal, S.; Mandavilli, A. India Blames Covid-19 Variant for its Pandemic Crisis. The New York Times. 28 April 2021. Available online: https://www.nytimes.com/2021/04/28/world/asia/india-covid19-variant.html (accessed on 29 April 2021).
- Pandey, V.; Nazmi, S. India Coivd-19: Deadly Second Wave Spreads from Cities to Small Towns. The BBC. 29 April 2021. Available online: https://www.bbc.com/news/world-asia-india-56913047 (accessed on 29 April 2021).
- Joi, P.; Gavi the Vaccine Alliance. Why is India’s COVID-19 Pandemic Skyrocketing. Available online: https://www.gavi.org/vaccineswork/why-indias-covid-19-pandemic-skyrocketing (accessed on 23 April 2021).
- The Indian Express. 1.33 Crore Sign in as COVID-19 Vaccine Doors Open, States Flag Stock Shortage. Available online: https://indianexpress.com/article/india/registration-on-cowin-1-33-crore-sign-in-states-flag-vaccine-stock-shortage-7293029/ (accessed on 29 April 2021).
- Arora, N.; Jain, R.; India hopes U.S. Will Soon Ease Ban on Vaccine Material Exports. Reuters. 19 April 2021. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/india-hopeful-us-will-soon-end-curbs-vaccine-raw-materials-export-govt-sources-2021-04-19/ (accessed on 20 April 2021).
- The BBC. Coronavirus: India Temporarily Halts Oxford-AstraZeneca Vaccine Exports. Available online: https://www.bbc.com/news/world-asia-india-56513371 (accessed on 29 April 2021).
- World Health Organization. COVAX Updates Participants on Delivery Delays for Vaccines from Serum Institute of India (SII) and AstraZeneca. Available online: https://www.who.int/news/item/25-03-2021-covax-updates-participants-on-delivery-delays-for-vaccines-from-serum-institute-of-india-(sii)-and-astrazeneca (accessed on 24 March 2021).
- Ellis-Petersen, H. WHO Blames ‘Perfect Storm’ of Factors for India Covid Crisis. The Guardian. 27 April 2021. Available online: https://www.theguardian.com/world/2021/apr/27/international-aid-arrives-in-india-to-combat-deadly-covid-crisis (accessed on 24 April 2021).
- The Wall Street Journal. Exchange Rates. Available online: https://www.wsj.com/market-data/currencies/exchangerates (accessed on 27 May 2021).
- Ministry of Health and Family Welfare of India. Update on COVID-19 Vaccination—Day 24. Available online: https://pib.gov.in/PressReleasePage.aspx?PRID=1696292 (accessed on 29 April 2021).
- Bagcchi, S. The world’s largest COVID-19 vaccination campaign. Lancet 2021, 21, 323. [Google Scholar] [CrossRef]
- Ministry of Health and Family Welfare Government of India. COVID-19 Vaccines Operational Guidelines. Available online: https://www.mohfw.gov.in/pdf/COVID19VaccineOG111Chapter16.pdf (accessed on 29 April 2021).
- World Health Organization. WHO Concept for Fair Access and Equitable Allocation of COVID-19 Health Products. Available online: https://www.who.int/docs/default-source/coronaviruse/who-covid19-vaccine-allocation-final-working-version-9sept.pdf (accessed on 30 April 2021).
- Foy, B.H.; Wahl, B.; Mehta, K.; Shet, A.; Menon, G.I.; Britto, C. Comparing COVID-19 vaccine allocation strategies in India: A mathematical modelling study. Int. J. Infect. Dis. 2020, 103, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Raghavan, P. Vaccine Makers Had Sought Funding Help, Market Access Opens Up Revenue Source. The Indian Express. 20 April 2021. Available online: https://indianexpress.com/article/india/covid-vaccine-funding-centre-7280781/ (accessed on 29 April 2021).
- Agarwal, N. COVID-19 Vaccination Will be Provided for Free at Government Facilities: Health Ministry. Zee News. 27 February 2021. Available online: https://zeenews.india.com/india/covid-19-vaccination-will-be-provided-for-free-at-government-facilities-union-health-ministry-2344726.html (accessed on 28 April 2021).
- McGregor, G. The World’s Largest Vaccine Maker Can’t Keep Up with the World’s Worst COVID Wave. Fortune. 20 April 2021. Available online: https://fortune.com/2021/04/20/india-covid-cases-vaccine-vaccinations-serum-institute/ (accessed on 26 April 2021).
- Arora, N.; Das, K. Analysis: India Shifts from Mass Vaccine Exporter to Importer, Worrying the World. Reuters. 16 April 2021. Available online: https://www.reuters.com/world/india/india-shifts-mass-vaccine-exporter-importer-worrying-world-2021-04-16/ (accessed on 5 May 2021).
- Ministry of External Affairs. Vaccine Supply. Available online: https://www.mea.gov.in/vaccine-supply.htm (accessed on 29 April 2021).
- Janssen Pharmaceutical Companies of Johnson & Johnson. ‘Products in Belgium’, Our Medicines. Available online: https://www.janssen.com/belgium/products (accessed on 29 April 2021).
- Bhuyan, A. Patent Waiver for Covid Vaccine Without Tech Transfer Won’t Speed Up Supply. Business Standard. 18 May 2021. Available online: https://www.business-standard.com/article/current-affairs/patent-waver-for-covid-vaccine-without-tech-transfer-won-t-speed-up-supply-121051800392_1.html (accessed on 5 July 2021).
- Ranjan, P. Voluntary Licensing of Covaxin Will Boost Vaccine Production. Hindustan Times. 4 May 2021. Available online: https://www.hindustantimes.com/opinion/voluntary-licensing-of-covaxin-will-boost-vaccine-production-101620130941033.html (accessed on 5 July 2021).
- Central Drugs Standard Control Organization. Draft Regulatory Guidelines for Development of Vaccines with Special Consideration for Covid-19 Vaccine. Available online: https://cdsco.gov.in/opencms/export/sites/CDSCO_WEB/Pdf-documents/biologicals/Regulatory_guidelines_for__development_of_Vaccine.pdf (accessed on 29 April 2021).
- Thiagarajan, K. Covid-19: India is at center of global vaccine manufacturing, but opacity threatens public trust. BMJ 2021, 372, n196. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A. India to Fund Capacity Boost at Serum Institute, Bharat Biotech as Vaccines Run Short. Reuters. 19 April 2021. Available online: https://www.reuters.com/world/india/india-fund-capacity-boost-serum-institute-vaccines-run-short-source-2021-04-19/ (accessed on 29 April 2021).
- Press Information Bureau—Government of India. Government Launches Mission COVID Suraksha to Accelerate Indian COIVD-19 Vaccine Development. Available online: https://pib.gov.in/PressReleaseIframePage.aspx?PRID=1676998 (accessed on 30 April 2021).
- Sharma, E.K. Where Did the Govt’s Rs 900 Crore R&D Grant for COVID Vaccine Development Go? The Financial Express. 14 April 2021. Available online: https://www.financialexpress.com/lifestyle/health/where-did-the-govts-rs-900-crore-rd-grant-for-covid-vaccine-development-go/2232734/ (accessed on 29 April 2021).
- Naik, S.; Paleja, A.; Mahajan, M.; Ramachandran, N.; Dixit, S.; Matthan, R.; Pai, N.; Kotasthane, P. A COVID-19 vaccine deployment strategy for India. Indian Public Policy Rev. 2020, 1, 42–58. [Google Scholar]
- Chaturvedi, R.M. Covid-19: Govt’s 4-Pronged Strategy for Vaccine Development. The Economic Times. 17 April 2021. Available online: https://economictimes.indiatimes.com/news/india/govts-4-pronged-strategy-for-vaccine-development/articleshow/82107211.cms (accessed on 26 April 2021).
- Press Information Bureau—Government of India. Augmentation of Manufacturing Capacity for COVAXIN Production under Mission COVID Suraksha. Available online: https://www.pib.gov.in/PressReleseDetail.aspx?PRID=1712271 (accessed on 5 May 2021).
- Press Trust of India. India Approves Sputnik V Vaccine, to Produce 850 mn Doses Annually: RDIF. Available online: https://www.business-standard.com/article/current-affairs/india-approves-sputnik-v-vaccine-to-produce-850-mn-doses-annually-rdif-121041300177_1.html (accessed on 29 April 2021).
- Ministry of Health and Family Welfare. Government of India Announces a Liberalised and Accelerated Phase 3 Strategy of Covid-19 Vaccination from 1st May. Available online: https://pib.gov.in/PressReleasePage.aspx?PRID=1712710 (accessed on 30 April 2021).
- World Health Organization. The ACT-Accelerator Frequently Asked Questions. Available online: https://www.who.int/initiatives/act-accelerator/faq (accessed on 14 April 2021).
- Berkley, S. COVAX Explained. The Economic Times. 3 September 2020. Available online: https://www.gavi.org/vaccineswork/covax-explained (accessed on 14 April 2021).
- Serum Institute of India. Serum Institute of India to Produce Up to an Additional 100 Million COVID-19 Vaccine Doses for India and Low-and Middle-Income Countries in 2021. Available online: https://www.seruminstitute.com/news_sii_gavi_bmgf.php (accessed on 14 April 2021).
- Unicef. UNICEF Executive Director Henrietta Fore’s Remarks at Briefing on COVAX Publishing Interim Distribution Forecast. Available online: https://www.unicef.org/press-releases/unicef-executive-director-henrietta-fores-remarks-briefing-covax-publishing-interim (accessed on 29 April 2021).
- World Health Organization. COVAX Announces Additional Deals to Access Promising COVID-19 Vaccine Candidates; Plans Global Rollout Starting Q1 2021. Available online: https://www.who.int/news/item/18-12-2020-covax-announces-additional-deals-to-access-promising-covid-19-vaccine-candidates-plans-global-rollout-starting-q1-2021 (accessed on 29 April 2021).
- Das, K.N. Biggest Share of Indian-Made Vaccines for Poor Country Programme Stays in India. Reuters. 30 March 2021. Available online: https://www.reuters.com/article/health-coronavirus-india-covax-idUSKBN2BM0XW (accessed on 28 April 2021).
- Unicef. COVID-19 Vaccine Market Dashboard. Available online: https://www.unicef.org/supply/covid-19-vaccine-market-dashboard (accessed on 29 April 2021).
- AnandRathi. Covid-19 Vaccine Update. Available online: https://images.assettype.com/bloombergquint/2020-12/c8d891f5-e8b7-4ae3-acbd-e6697bcf70a4/Anand_Rathi_Covid_19_Vaccine_Update.pdf (accessed on 29 April 2021).
- The Lancet. Access to COVID-19 vaccines: Looking beyond COVAX. Lancet 2021, 397, 941. [Google Scholar] [CrossRef]
- Rai, V. India Extends ‘Vaccine Maitri’ to its Neighbours. Available online: https://www.isas.nus.edu.sg/wp-content/uploads/2021/02/822.pdf (accessed on 29 April 2021).
- Paravincini, G. India’s Halt to Vaccine Exports ‘Very Problematic’ for Africa. Reuters. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/indias-halt-vaccine-exports-very-problematic-africa-2021-05-18/ (accessed on 3 July 2021).
- Arora, N.; Das, K.; Jain, R. EXCLUSIVE: India Unlikely to Resume Sizeable COVID-19 Vaccine Exports Until October. Reuters. 18 May 2021. Available online: https://www.reuters.com/world/india/exclusive-india-unlikely-resume-sizable-covid-19-vaccine-exports-until-october-2021-05-18/ (accessed on 3 July 2021).
- Padma, T.V. India’s COVID-vaccine woes—by the numbers. Nature 2021, 592, 500–501. [Google Scholar] [CrossRef] [PubMed]
- Aljazeera. India Vaccine-Maker Hopes to Share Shots by End of the Year. Available online: https://www.aljazeera.com/news/2021/5/18/india-unlikely-to-resume-covid-jab-exports-until-october-report (accessed on 18 July 2021).
- Ekström, A.M.; Berggren, C.; Tomson, G.; Gostin, L.O.; Friberg, P.; Ottersen, O.P. The battle for COVID-19 vaccines highlights the need for a new global governance mechanism. Nat. Med. 2021, 27, 739–740. [Google Scholar] [CrossRef] [PubMed]
- The Lancet. Global governance for COVID-19 vaccines. Lancet 2020, 395, 1883. [Google Scholar] [CrossRef]
- World Trade Organization. TRIPS Council to Continue to Discuss Temporary IP Waiver, Revised Proposal Expected in May. Available online: https://www.wto.org/english/news_e/news21_e/trip_30apr21_e.htm (accessed on 30 June 2021).
- Times of India. EXPLAINED: How Intellectual Property Waiver Can Boost Production of Covid Vaccines in India. Available online: https://timesofindia.indiatimes.com/business/india-business/explained-how-intellectual-property-waiver-can-boost-production-of-covid-vaccines/articleshow/83718825.cms (accessed on 30 June 2021).
- Mantri, G. Why Removing Patents on COVID-19 Vaccines is the Need of the Hour. The News Minute. 6 May 2021. Available online: https://www.thenewsminute.com/article/why-removing-patents-covid-19-vaccines-need-hour-148408 (accessed on 5 July 2021).
- Our Word in Data. ‘COVID-19 Vaccine Doses Administered’, COVID-19 Data Explorer. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-01..latest&pickerSort=desc&pickerMetric=total_vaccinations_per_hundred&Metric=Vaccine+doses&Interval=Cumulative&Relative+to+Population=false&Align+outbreaks=false&country=~IND (accessed on 7 May 2021).
- Unicef. No-One Is Safe until Everyone Is Safe—Why We Need a Global Response to COVID-19. Available online: https://www.unicef.org/press-releases/no-one-safe-until-everyone-safe-why-we-need-global-response-covid-19 (accessed on 28 May 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Indian Distributer | International Collaborator |
|---|---|---|
| Covishield | Serum Insititute of India | Astra Zeneca |
| Covaxin | Bharat Biotech International Ltd. | |
| Sputnik V | Dr. Reddy’s Laboratories | Gamaleya National Center |
| NVX-CoV2373 | Serum Institute of India | Novavax |
| COVID-19 Vaccine Janssen | Biological E | Johnson & Johnson |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koller, C.N.; Schwerzmann, C.J.; Lang, A.S.A.; Alexiou, E.; Krishnakumar, J. Addressing Different Needs: The Challenges Faced by India as the Largest Vaccine Manufacturer While Conducting the World’s Biggest COVID-19 Vaccination Campaign. Epidemiologia 2021, 2, 454-470. https://doi.org/10.3390/epidemiologia2030032
Koller CN, Schwerzmann CJ, Lang ASA, Alexiou E, Krishnakumar J. Addressing Different Needs: The Challenges Faced by India as the Largest Vaccine Manufacturer While Conducting the World’s Biggest COVID-19 Vaccination Campaign. Epidemiologia. 2021; 2(3):454-470. https://doi.org/10.3390/epidemiologia2030032
Chicago/Turabian StyleKoller, Cinja Nadana, Cléo Josephine Schwerzmann, Alexia Suzanne Aimée Lang, Eleni Alexiou, and Jaya Krishnakumar. 2021. "Addressing Different Needs: The Challenges Faced by India as the Largest Vaccine Manufacturer While Conducting the World’s Biggest COVID-19 Vaccination Campaign" Epidemiologia 2, no. 3: 454-470. https://doi.org/10.3390/epidemiologia2030032