
A General Computational Framework for COVID-19 Modelling with Applications to Testing Varied Interventions in Education Environments

 , , and
, , and
Abstract
:1. Introduction
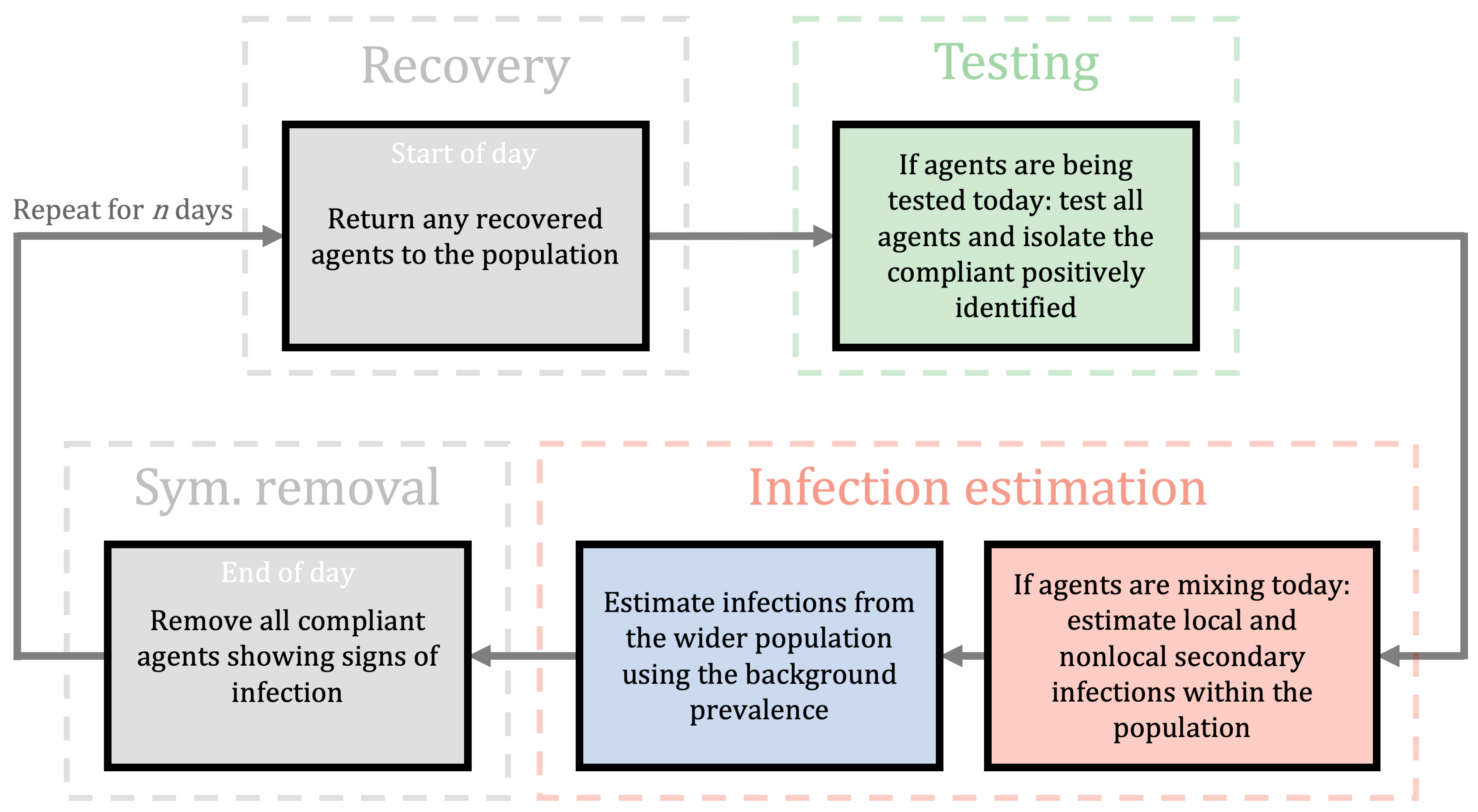
2. A Computational Framework for Estimating Transmission with NPIs
- A local number, , that measures the expected number of secondary infections within a subgroup that has an infected person; and
- A non-local number, , that measures the expected number of secondary infections that occur in the non-local compartment further away;
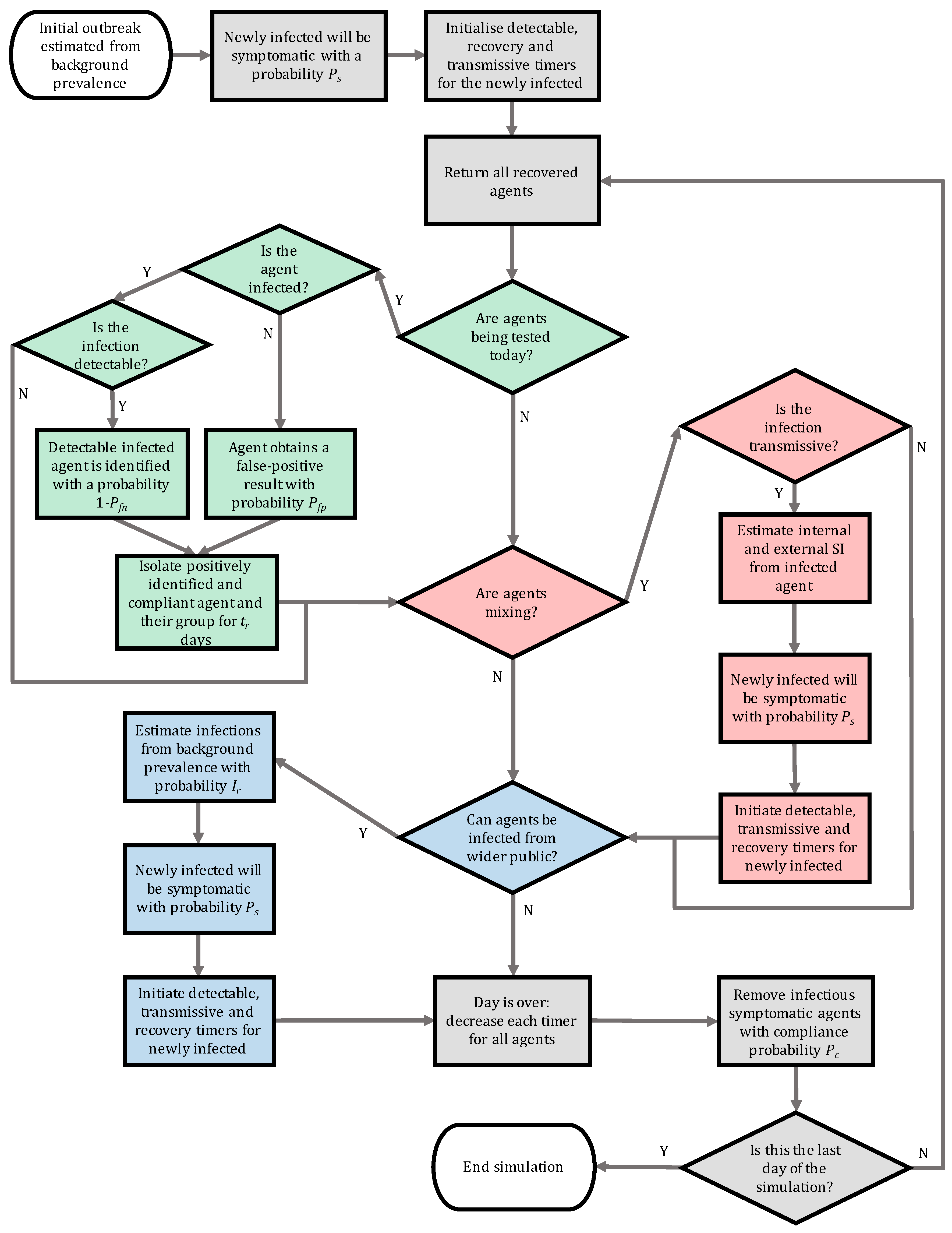
- infected;
- infectious;
- not isolated;
- The time between becoming infected to becoming infectious; we take days,
- The time between becoming infected to becoming detectable by a LFD test; we take days, and
- The time between becoming infected to recovery; we take days.
2.1. Interventions
2.1.1. Scenario: Classrooms
2.1.2. Scenario: Halls of Residence
2.1.3. Vaccinations
2.2. Testing Regimes
2.3. Isolation Regimes
- Isolating individuals due to the individual being symptomatic, or receiving a positive test result;
- Isolating subgroups due to at least one individual in the subgroup being symptomatic, or receiving a positive test result;
- Isolating an entire population due to at least one individual being symptomatic, or receiving a positive test result.
2.4. Robustness of LFD Testing Strategies: Parameter Estimation
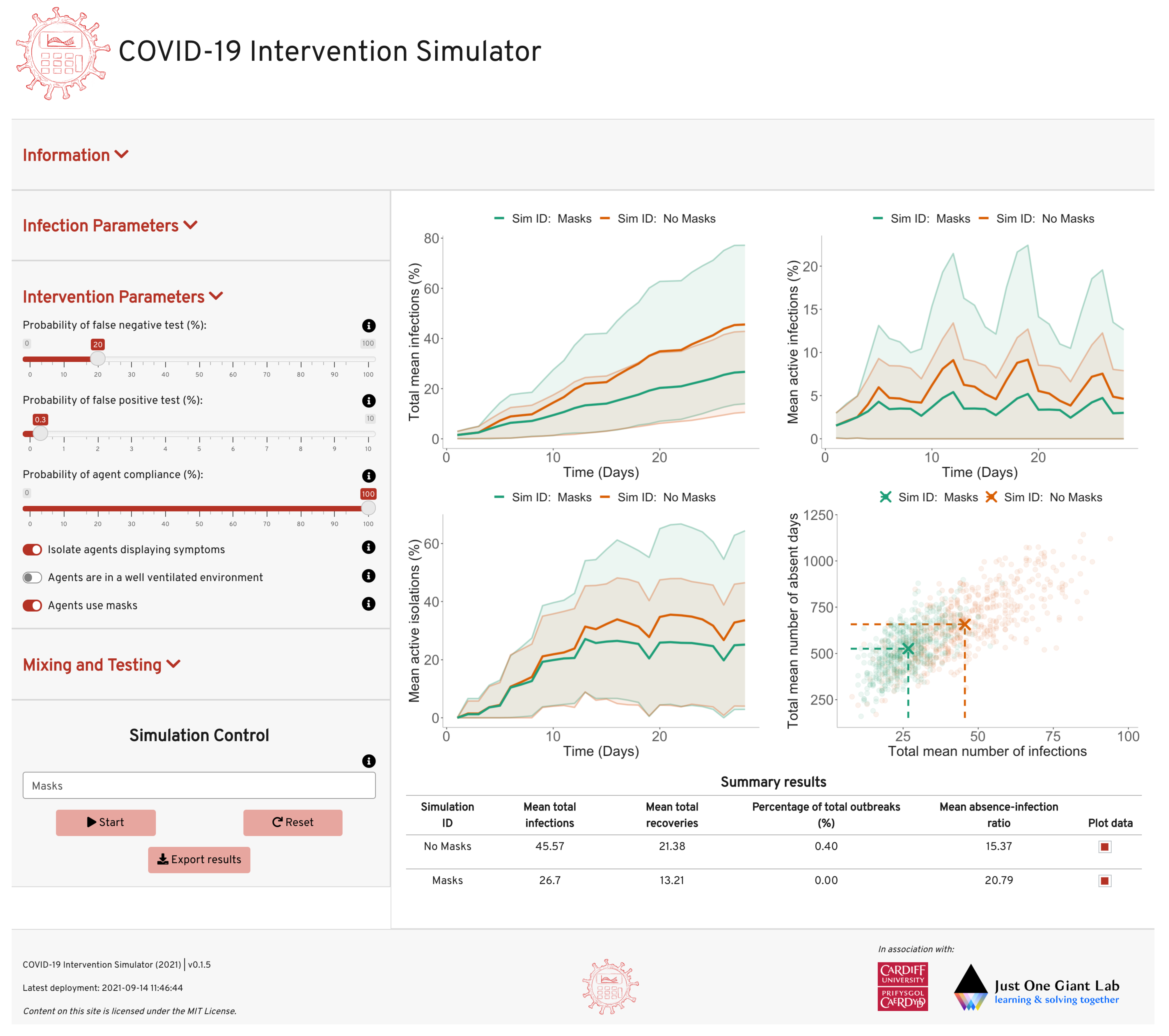
2.5. Open-Source Code and User-Friendly Applet
3. Results
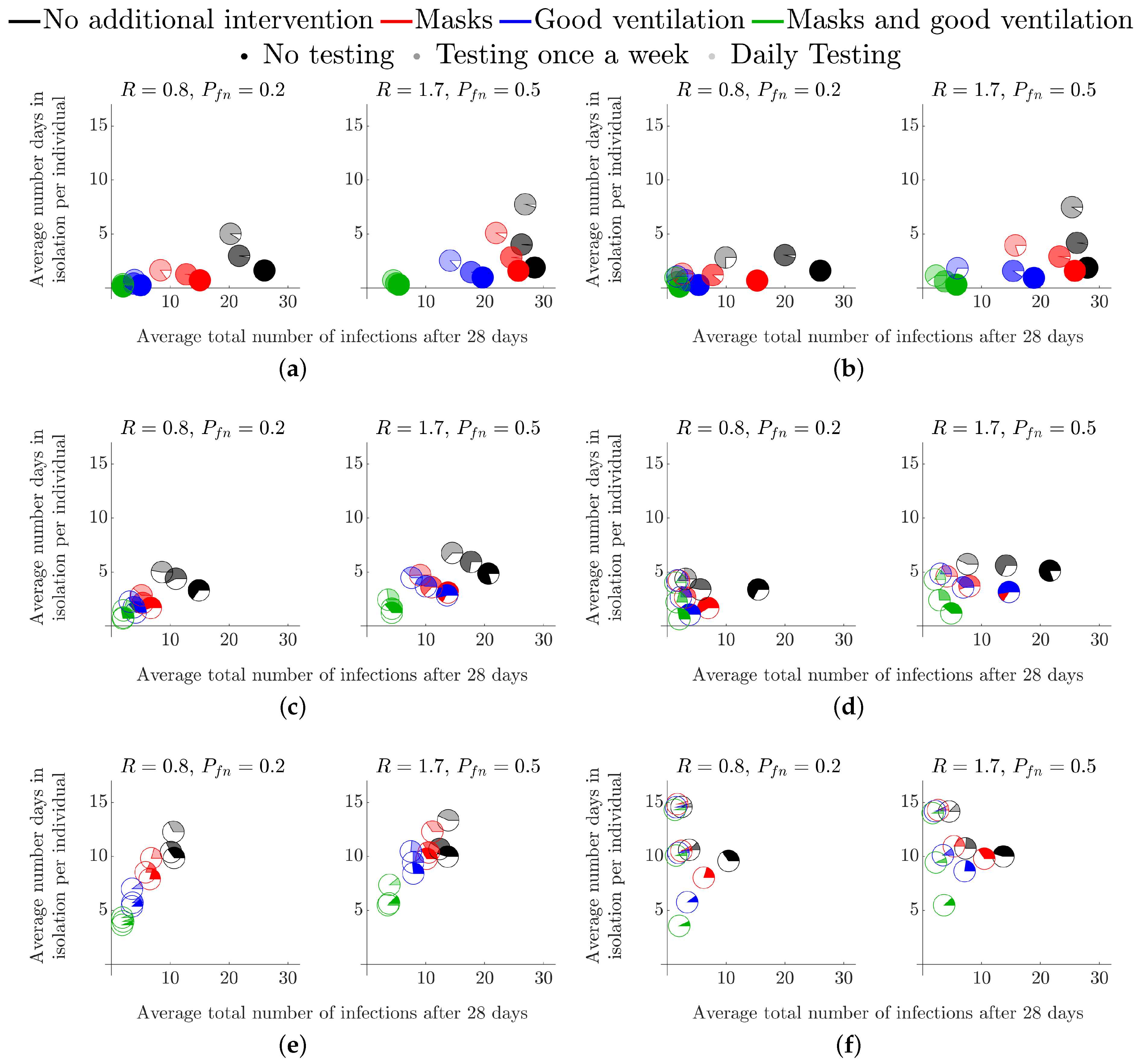
3.1. Secondary School Environments
3.1.1. Without Testing
3.1.2. With Testing
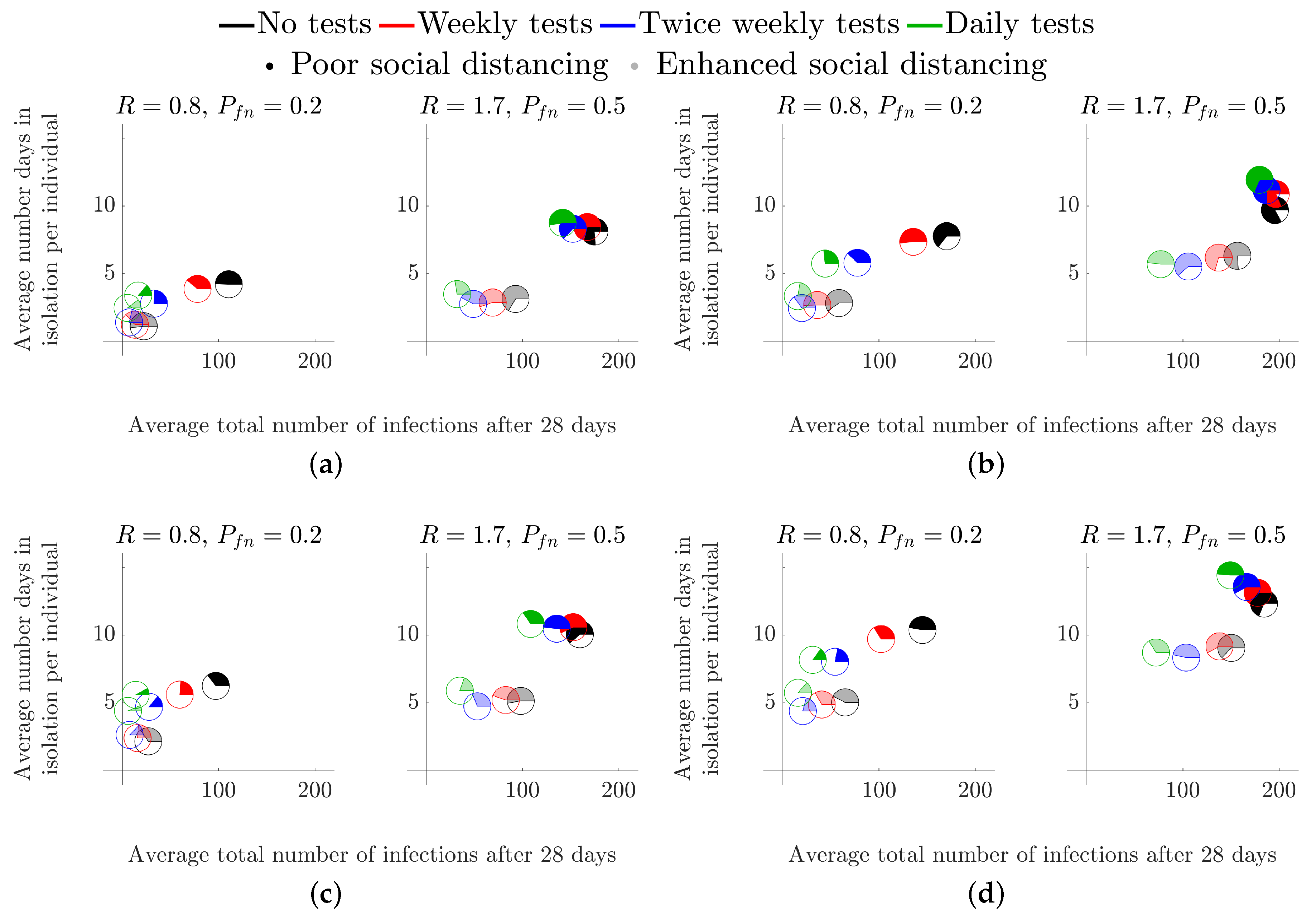
3.2. Higher Education Environments
3.2.1. Start of Term
3.2.2. Middle of Term
4. Discussion
4.1. Impact
4.2. Future Work
4.3. Summary
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Individual Based Model Interpretation and Implementation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Real-World Event | Infection Classification | Infectious to the Population at Post Event | Maximum Number of Days Infectious Prior to Event (Days) | Maximum Number of Days Infectious Post Event (Days) | Isolation Status Post Event | Susceptible Status Post Event |
|---|---|---|---|---|---|---|
| Presymptomatic student attending school | Asymptomatic | ✓ | 0 | ✗ | ✗ | |
| Non-compliant symptomatic student attending school | Asymptomatic | ✓ | ✗ | ✗ | ||
| Symptomatic student with a true-positive test result compliant with isolation policy | Symptomatic | ✗ | 0 | ✓ | ✗ | |
| Symptomatic student with a false-negative test result compliant with isolation policy | Asymptomatic | ✓ | 0 | ✓ | ✗ | |
| Asymptomatic student with a true-positive test result compliant with isolation policy | Asymptomatic | ✗ | 0 | ✓ | ✗ | |
| Asymptomatic student with a false-negative test result | Asymptomatic | ✓ | ✗ | ✗ | ||
| Non-infected student with a false-positive test result from random testing | Non-infected | ✗ | 0 | 0 | ✓ | ✓ |
| Non-infected student with a true-negative test result from random testing | Non-infected | ✗ | 0 | 0 | ✗ | ✓ |
| Asymptomatic student in close contact with a positively identified infected student | Asymptomatic | ✗ | 0 | ✓ | ✗ | |
| Non-infected student in close contact with a positively identified infected student | Non-infected | ✗ | 0 | 0 | ✓ | ✓ |
| Number of Agents | Testing | Agent Mixing | Wider pop. Infections | Isolation Group Sizes | Probability of Symptomatic | Probability of Compliance | |
|---|---|---|---|---|---|---|---|
| Secondary school (no testing) | 30 | ✗ | Weekdays | ✗ | 1, 5 & 30 | 0.2 & 0.5 | 1.0 |
| Secondary school (with testing) | 30 | ✓ | Weekdays | ✗ | 1, 5 & 30 | 0.2 & 0.5 | 1.0 |
| Halls of residence (start of term) | 204 | ✓ | 1 week isolated followed by 3 weeks continuous mixing | ✗ | 6 & 12 | 0.4 | 0.8 |
| Halls of residence (middle of term) | 204 | ✓ | Everyday | ✗ | 6 & 12 | 0.4 | 0.8 |
| Parameter | Definition |
|---|---|
| Probability of false-positive, | The likelihood that a LFD test identifies a non-infected agent with a positive result. |
| Probability of false-negative, | The likelihood that a LFD test does not identify an infected agent with a positive result. |
| R number, R | The average number of secondary cases expected from an infected agent to generate prior to locality affects. |
| Local R number, | The proportion of R that accounts for the number of secondary infections within a subgroup of the population. |
| non-local R number, | The proportion of R that accounts for the number of secondary infections to those outside the infectives subgroup. |
| Background prevalence, | The rate at which the wider population introduces an infection to an agent. |
| Probability of compliance, C | The likelihood that an agent is compliant with testing and isolation policies. |
| Probability of symptomatic, | The likelihood that an infected agent will become symptomatic. |
| Total population size, N | The total number of agents in the simulation. |
| Subgroup size, | The number of agents that make up a subgroup within the total population. |
| Infectious time, | The time between becoming infected to becoming infectious. |
| Detectable time, | The time between becoming infected to becoming detectable by a LFD. |
| Recovery time, | The time between becoming infected to recovery from infection. |

Appendix B. Open-Access Online COVID-19 Intervention Simulator
- Immunity of individuals in the population (vaccinations/recent infections);
- Optional automatic Welsh infection data retrieval (included to aid the Welsh TAG);
- Export simulation input data and output data into a downloadable Excel document for further analysis.

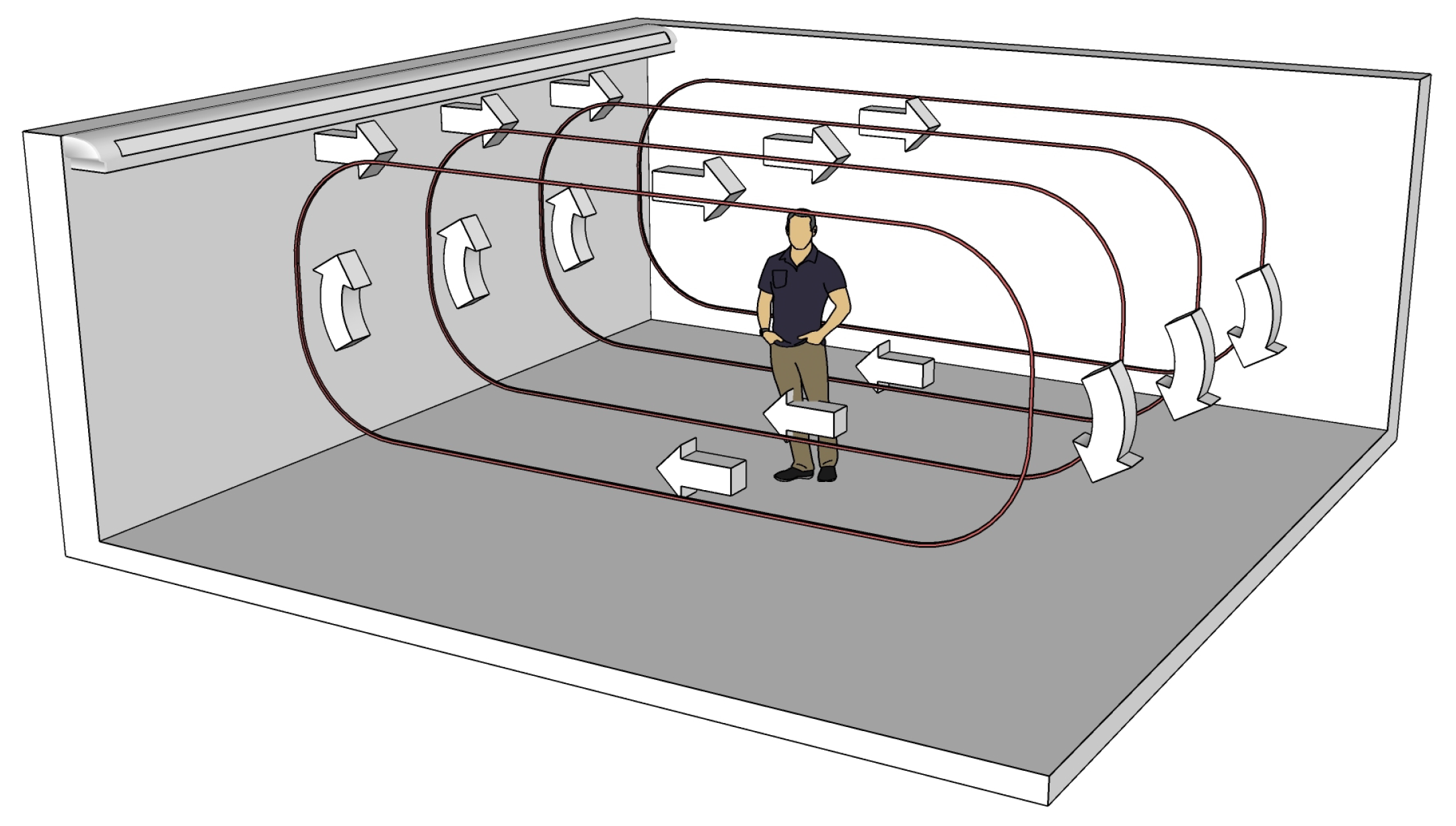
Appendix C. The Airborne Transmission Model and the Estimation of Rl and Rn

| Parameter | Value | Source |
|---|---|---|
| Classroom dimensions | 8 m × 8 m × 3 m | |
| Airflow speed | 0.15 m/s | [74] |
| Room air exchange rate | Very poor ventilation: 0.12 h−1 | [56] |
| (ACH) | Poor ventilation: 0.72 h−1 | [56] |
| ASHRAE recommended ventilation: 3.00 h−1 | [55] | |
| Eddy diffusion coefficient | Very poor ventilation: 8.8 m2/s | [59] |
| Poor ventilation: 5.3 × 10−3 m2/s | ||
| ASHRAE recommended ventilation (good ventilation): 2.2 × 10−2 m2/s | ||
| Breathing rate | 1.3 × 10−4 m3/s | [75] |
| Generation rate of | Breathing: 0.5 particles/s | [76] |
| infectious particles | Low activity (20% talking, 80% breathing): 1.4 particles/s | |
| Talking: 5 particles/s | ||
| Efficiency of mask | 0.5 | [57] |
| Virus deactivation rate | 1.7 × 10−4 s−1 | [77] |
| Aerosol settling rate | 1.1 × 10−4 s−1 | [78] |
| Median infectious dose | 100 particles | [79] |
| ACH = 0.12 h−1 | ACH = 0.72 h−1 | ACH = 3.00 h−1 | ||||
|---|---|---|---|---|---|---|
| Al | An | Al | An | Al | An | |
| Breathing | ||||||
| With mask | 21.1 | 3.7 | 8.2 | 4.3 | 3.1 | 2.0 |
| No mask | 42.2 | 7.3 | 16.4 | 8.6 | 6.2 | 4.1 |
| Low activity (20% Talking and 80% Breathing) | ||||||
| With mask | 59.4 | 10.2 | 23.0 | 12.0 | 8.7 | 5.8 |
| No mask | 118.3 | 20.5 | 46.0 | 24.1 | 17.5 | 11.5 |
| Talking/Superspreader | ||||||
| With mask | 202.8 | 35.1 | 78.8 | 41.3 | 30 | 19.8 |
| No mask | 422.4 | 73.1 | 164.2 | 86.1 | 62.5 | 41.2 |
| ACH = 0.12 h−1 | ACH = 0.72 h−1 | ACH = 3.00 h−1 | ||||
|---|---|---|---|---|---|---|
| PAl | PAn | PAl | PAn | PAl | PAn | |
| Breathing | ||||||
| With mask | 0.267 | 0.041 | 0.115 | 0.058 | 0.047 | 0.031 |
| No mask | 0.462 | 0.080 | 0.217 | 0.113 | 0.092 | 0.061 |
| Low activity (20% Talking and 80% Breathing) | ||||||
| With mask | 0.581 | 0.110 | 0.289 | 0.154 | 0.127 | 0.084 |
| No mask | 0.824 | 0.207 | 0.495 | 0.284 | 0.238 | 0.161 |
| Talking/Superspreader | ||||||
| With mask | 0.949 | 0.329 | 0.690 | 0.436 | 0.372 | 0.260 |
| No mask | 0.998 | 0.534 | 0.913 | 0.697 | 0.621 | 0.466 |
| ACH = 0.12 h−1 | ACH = 0.72 h−1 | ACH = 3.00 h−1 | ||||
|---|---|---|---|---|---|---|
| + No Mask | + No Mask | + No Mask | + No Mask | + No Mask | + No Mask | |
| Effective R number | R | |||||
| Local to non-local infection ratio (:) | 3.98:1 | 5.20:1 | 1.74:1 | 1.88:1 | 1.47:1 | 1.51:1 |
| ACH = 0.12 h−1 | ACH = 0.72 h−1 | ACH = 3.00 h−1 | ||||
|---|---|---|---|---|---|---|
| Without mask | 0.64–1.36 | 0.16–0.34 | 0.31–0.65 | 0.17–0.37 | 0.14–0.29 | 0.09–0.20 |
| With mask | 0.34–0.71 | 0.06–0.14 | 0.16–0.33 | 0.08–0.18 | 0.07–0.15 | 0.05–0.10 |
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Chahrour, M.; Assi, S.; Bejjani, M.; Nasrallah, A.A.; Salhab, H.; Fares, M.; Khachfe, H.H. A bibliometric analysis of COVID-19 research activity: A call for increased output. Cureus 2020, 12, e7357. [Google Scholar] [CrossRef] [Green Version]
- Sahu, P. Closure of universities due to Coronavirus Disease 2019 (COVID-19): Impact on education and mental health of students and academic staff. Cureus 2020, 12, e7541. [Google Scholar] [CrossRef] [Green Version]
- Rapanta, C.; Botturi, L.; Goodyear, P.; Guàrdia, L.; Koole, M. Online university teaching during and after the Covid-19 crisis: Refocusing teacher presence and learning activity. Postdigi. Sci. Edu. 2020, 2, 1–23. [Google Scholar] [CrossRef]
- English Government. Education, Universities and Childcare. Available online: https://www.gov.uk/coronavirus/education-and-childcare (accessed on 12 June 2021).
- Welsh Government. Schools: Coronavirus Guidance. Available online: https://gov.wales/schools-coronavirus-guidance (accessed on 12 June 2021).
- Welsh Government Higher Education: Coronavirus. Available online: https://gov.wales/higher-education-coronavirus-guide (accessed on 12 June 2021).
- Scientific Pandemic Influenza Group on Modelling, Operational Sub-Group, SPI-M-O: Summary of Modelling on Scenarios for Easing Restrictions. 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/963400/S1116_SPI-M-O_Summary_of_modelling_on_scenario_for_easing_restrictions.pdf (accessed on 13 June 2021).
- Melnick, H.; Darling-Hammond, L. Reopening schools in the context of COVID-19: Health and safety guidelines from other countries. Policy Brief. Learn. Policy Inst. 2020. Available online: https://learningpolicyinstitute.org/product/reopening-schools-covid-19-brief (accessed on 12 June 2021).
- Donohue, J.M.; Miller, E. COVID-19 and school closures. JAMA 2020, 324, 845–847. [Google Scholar] [CrossRef]
- Daniel, J. Education and the COVID-19 pandemic. Prospects 2020, 49, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Asanov, I.; Flores, F.; McKenzie, D.; Mensmann, M.; Schulte, M. Remote-learning, time-use, and mental health of Ecuadorian high-school students during the COVID-19 quarantine. World Dev. 2021, 138, 105225. [Google Scholar] [CrossRef]
- Amodio, E.; Battisti, M.; Kourtellos, A.; Maggio, G.; Maida, C.M. Schools opening and Covid-19 diffusion: Evidence from geolocalized microdata. COVID Econom. 2020, 65, 7–77. [Google Scholar]
- European Centre for Disease Prevention and Control (ECDC). COVID-19 in Children and the Role of School Settings in Transmission. Available online: https://www.ecdc.europa.eu/en/publications-data/children-and-school-settings-covid-19-transmission (accessed on 28 August 2021).
- Lordan, R.; FitzGerald, G.A.; Grosser, T. Reopening schools during COVID-19. Science 2020, 369, 1146. [Google Scholar] [CrossRef]
- Association of School and College Leaders. Lateral Flow Testing in Schools and Colleges FAQs. Available online: https://www.ascl.org.uk/Help-and-Advice/Leadership-and-governance/Health,-safety-and-safeguarding/Coronavirus-essential-information/Coronavirus-FAQs/Lateral-flow-testing-in-schools-and-colleges (accessed on 14 March 2021).
- National Education Union. Coronavirus: Testing in Schools and Colleges. Available online: https://neu.org.uk/coronavirus-school-testing (accessed on 13 March 2021).
- Welsh Government. Routine Testing for Education and Childcare Staff. Available online: https://gov.wales/routine-testing-education-and-childcare-staff-html (accessed on 23 March 2021).
- Torjesen, I. Covid-19: How the UK is using lateral flow tests in the pandemic. BMJ 2021, 372, n287. [Google Scholar] [CrossRef]
- UK Government. Coronavirus (COVID-19): Test to Release for International Travel. Available online: https://www.gov.uk/guidance/coronavirus-covid-19-test-to-release-for-international-travel#how-the-scheme-works (accessed on 12 March 2021).
- Deeks, J.; Gill, M.; Bird, S.; Richardson, S.; Ashby, D. Covid-19 INNOVA Testing in Schools: Don’t Just Test, Evaluate. 2021. Available online: https://blogs.bmj.com/bmj/2021/01/12/covid-19-innova-testing-in-schools-dont-just-test-evaluate (accessed on 12 June 2021).
- Joint PHE Porton Down & University of Oxford SARS-CoV-2 Test Development and Validation Cell. Rapid Evaluation of Lateral Flow Viral Antigen Detection Devices (LFDs) for Mass Community Testing. Available online: https://www.ox.ac.uk/sites/files/oxford/media_wysiwyg/UK_evaluation_PHE_Porton_Down_University_of_Oxford_final.pdf (accessed on 12 March 2021).
- Scientific Advisory Group for Emergencies SPI-B: Possible Impact of the COVID-19 Vaccination Programme on Adherence to Rules and Guidance about Personal Protective Behaviours Aimed at Preventing Spread of the Virus, 17 Decemeber 2020; UK Government: London, UK, 2021.
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Gal Levin, E.; Rubin, C.; Indenbaum, V.; et al. Covid-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Havers, F.P.; Pham, H.; Taylor, C.A.; Whitaker, M.; Patel, K.; Anglin, O.; Kambhampati, A.K.; Milucky, J.; Zell, E.; Chai, S.J.; et al. COVID-19-associated hospitalizations among vaccinated and unvaccinated adults ≥18 years–COVID-NET, 13 states, January 1–July 24, 2021. medRxiv 2021. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Your Guide to Masks. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/about-face-coverings.html (accessed on 24 September 2021).
- Young, B.C.; Eyre, D.W.; Kendrick, S.; White, C.; Smith, S.; Beveridge, G.; Nonnenmacher, T.; Ichofu, F.; Hillier, J.; Oakley, S.; et al. Daily testing for contacts of individuals with SARS-CoV-2 infection and attendance and SARS-CoV-2 transmission in English secondary schools and colleges: An open-label, cluster-randomised trial. Lancet 2021, 398, 1217–1229. [Google Scholar] [CrossRef]
- Office for National Statistics. Coronavirus (COVID-19) Latest Insights: Infections. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19latestinsights/infections (accessed on 15 September 2021).
- UK Health Security Agency. The Latest Reproduction Number (R) and Growth Rate of Coronavirus (COVID-19). Available online: https://www.gov.uk/guidance/the-r-value-and-growth-rate (accessed on 17 September 2021).
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Currie, C.S.M.; Fowler, J.W.; Kotiadis, K.; Monks, T.; Onggo, B.S.; Robertson, D.A.; Tako, A.A. How simulation modelling can help reduce the impact of COVID-19. J. Simul. 2020, 14, 83–97. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, N.M.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunubá, Z.; Cuomo-Dannenburg, G.; et al. Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand; Imperial College London: London, UK, 2020. [Google Scholar]
- Latif, S.; Usman, M.; Manzoor, S.; Iqbal, W.; Qadir, J.; Tyson, G.; Castro, I.; Razi, A.; Boulos, M.N.K.; Weller, A. Leveraging data science to combat COVID-19: A comprehensive review. IEEE Trans. Art. Int. 2020, 1, 85–103. [Google Scholar] [CrossRef]
- Harper, P.R.; Moore, J.W.; Woolley, T.E. Covid-19 transmission modelling of students returning home from university. Health Syst. 2021, 10, 31–40. [Google Scholar] [CrossRef]
- Zhigljavsky, A.; Whitaker, R.; Fesenko, I.; Kremnizer, K.; Noonan, J.; Harper, P.; Gillard, J.; Woolley, T.; Gartner, D.; Grimsley, J. Generic probabilistic modelling and non-homogeneity issues for the UK epidemic of COVID-19. arXiv 2020, arXiv:2004.01991. [Google Scholar]
- Auger, P.; Moussaoui, A. On the threshold of release of confinement in an epidemic SEIR model taking into account the protective effect of mask. Bull. Math. Biol. 2021, 83, 25. [Google Scholar] [CrossRef]
- Scientific Pandemic Influenza Group on Modelling. SPI-M Modelling Summary for Pandemic Influenza; UK Government: London, UK, 2021.
- Keeling, M.J.; Tildesley, M.J.; Atkins, B.D.; Penman, B.; Southall, E.; Guyver-Fletcher, G.; Holmes, A.; McKimm, H.; Gorsich, E.E.; Hill, E.M.; et al. The impact of school reopening on the spread of COVID-19 in England. Philos. Trans. R. Soc. B 2021, 376, 20200261. [Google Scholar] [CrossRef]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sust. Citi. Soc. 2020, 62, 102390. [Google Scholar] [CrossRef]
- UK Government. COVID-19 in the UK. Available online: https://coronavirus.data.gov.uk/details/download (accessed on 13 September 2021).
- Anderson, D.H. Compartmental Modeling and Tracer Kinetics; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013; Volume 50. [Google Scholar]
- Jacquez, J.A. Compartmental Analysis in Biology and Medicine; Elsevier Pub. Co.: New York, NY, USA, 1972. [Google Scholar]
- Evans, W.C. Linear Systems, Compartmental Modeling, and Estimability Issues in IAQ Studies; ASTM International: West Conshohocken, PA, USA, 1996. [Google Scholar]
- Lau, Z.; Griffiths, I.; English, A.; Kaouri, K. Predicting the Spatially Varying Infection Risk in Indoor Spaces Using an Efficient Airborne Transmission Model. arXiv 2021, 12267. Available online: https://europepmc.org/article/ppr/ppr340373 (accessed on 12 June 2021).
- Riley, E.; Murphy, G.; Riley, R. Airborne spread of measles in a suburban elementary school. Am. J. Epidemiol. 1978, 107, 421–432. [Google Scholar] [CrossRef]
- Gammaitoni, L.; Nucci, M. Using a mathematical model to evaluate the efficacy of TB control measures. Emerg. Infect. Dis. 1997, 3, 335. [Google Scholar] [CrossRef] [PubMed]
- ONS. Coronavirus (COVID-19) Infection Survey, UK: 19 February 2021. Off. Natl. Stat. 2021, 26, 1–18. [Google Scholar]
- Crozier, A.; Rajan, S.; Buchan, I.; McKee, M. Put to the test: Use of rapid testing technologies for covid-19. BMJ 2021, 372, n208. [Google Scholar] [CrossRef]
- Mistry, D.A.; Wang, J.Y.; Moeser, M.E.; Starkey, T.; Lee, L.Y.W. A systematic review of the sensitivity and specificity of lateral flow devices in the detection of SARS-CoV-2. BMC Infect. Dis. 2021, 21, 828. [Google Scholar] [CrossRef] [PubMed]
- Peto, T.; Affron, D.; Afrough, B.; Agasu, A.; Ainsworth, M.; Allanson, A.; Allen, K.; Allen, C.; Archer, L.; Ashbridge, N.; et al. COVID-19: Rapid antigen detection for SARS-CoV-2 by lateral flow assay: A national systematic evaluation of sensitivity and specificity for mass-testing. EClinicalMedicine 2021, 36, 100924. [Google Scholar] [CrossRef]
- Pickering, S.; Batra, R.; Merrick, B.; Snell, L.B.; Nebbia, G.; Douthwaite, S.; Reid, F.; Patel, A.; Ik, M.T.K.; Patel, B.; et al. Comparative performance of SARS-CoV-2 lateral flow antigen tests and association with detection of infectious virus in clinical specimens: A single-centre laboratory evaluation study. Lancet Microbe 2021, 2, e461–e471. [Google Scholar] [CrossRef]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.; Andreae, M.; Pöschl, U.; Su, H. Face masks effectively limit the probability of SARS-CoV-2 transmission. Science 2021, 373, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- Correia, G.; Rodrigues, L.; Da Silva, M.G.; Gonçalves, T. Airborne route and bad use of ventilation systems as non-negligible factors in SARS-CoV-2 transmission. Med. Hypotheses 2020, 141, 109781. [Google Scholar] [CrossRef]
- Zhao, B.; Liu, Y.; Chen, C. Air purifiers: A supplementary measure to remove airborne SARS-CoV-2. Build. Environ. 2020, 177, 106918. [Google Scholar] [CrossRef] [PubMed]
- American Society of Heating, Refrigerating and Air-Conditioning Engineers. Ventilation for acceptable indoor air quality. ANSI/ASHRAE Standard 2019, 62, 1. [Google Scholar]
- Guo, H.; Morawska, L.; He, C.; Gilbert, D. Impact of ventilation scenario on air exchange rates and on indoor particle number concentrations in an air-conditioned classroom. Atmos. Environ. 2008, 42, 757–768. [Google Scholar] [CrossRef] [Green Version]
- Fischer, E.; Fischer, M.; Grass, D.; Henrion, I.; Warren, W.; Westman, E. Low-cost measurement of face mask efficacy for filtering expelled droplets during speech. Sci. Adv. 2020, 6, eabd3083. [Google Scholar] [CrossRef]
- Department of Health and Social Care and Scientific Advisory Group for Emergencies. The R value and growth rate in the UK. Available online: https://www.gov.uk/guidance/the-r-number-in-the-uk (accessed on 3 August 2021).
- Foat, T.; Drodge, J.; Nally, J.; Parker, S. A relationship for the diffusion coefficient in eddy diffusion based indoor dispersion modelling. Build. Environ. 2020, 169, 106591. [Google Scholar] [CrossRef]
- Bazant, M.; Bush, J. A guideline to limit indoor airborne transmission of COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2018995118. [Google Scholar] [CrossRef]
- Mousavi, E.S.; Pollitt, K.J.G.; Sherman, J.; Martinello, R.A. Performance analysis of portable HEPA filters and temporary plastic anterooms on the spread of surrogate coronavirus. Build. Environ. 2020, 183, 107186. [Google Scholar] [CrossRef]
- National Health Service England. COVID-19 Vaccinations. Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/covid-19-vaccinations/ (accessed on 13 September 2021).
- Hyde, Z. COVID-19, children, and schools: Overlooked and at risk. Med. J. Aust. 2020, 213, 444–446. [Google Scholar] [CrossRef]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.M.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). J. Infect. Dis. 2020, 94, 154. [Google Scholar] [CrossRef] [PubMed]
- Day, M. Covid-19: Four fifths of cases are asymptomatic, China figures indicate. BMJ 2020, 369, m1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodeur, A.; Clark, A.E.; Fleche, S.; Powdthavee, N. COVID-19, lockdowns and well-being: Evidence from Google Trends. J. Public Econ. 2021, 193, 104346. [Google Scholar] [CrossRef]
- Labrague, L.J.; Ballad, C.A. Lockdown fatigue among college students during the COVID-19 pandemic: Predictive role of personal resilience, coping behaviors, and health. medRxiv 2020, 20213942. [Google Scholar] [CrossRef] [PubMed]
- Brouard, S.; Vasilopoulos, P.; Becher, M. Sociodemographic and psychological correlates of compliance with the COVID-19 public health measures in France. Can. J. Political Sci. Can. Sci. Polit. 2020, 53, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Huang, Y.; Tu, C.; Bi, C.; Chen, Z.; Luo, L.; Huang, M.; Chen, M.; Tan, C.; Wang, Z.; et al. Household Transmission of SARS-CoV-2, Zhuhai, China, 2020. Clin. Infect. Dis. 2020, 71, 2099–2108. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dufort, E.M.; Blog, D.S.; Hall, E.W.; Hoefer, D.; Backenson, B.P.; Muse, A.T.; Kirkwood, J.N.; St. George, K.; Holtgrave, D.R.; et al. COVID-19 Testing, Epidemic Features, Hospital Outcomes, and Household Prevalence, New York State—March 2020. Clin. Infect. Dis. 2020, 71, 1953–1959. [Google Scholar] [CrossRef]
- Lewis, N.M.; Chu, V.T.; Ye, D.; Conners, E.E.; Gharpure, R.; Laws, R.L.; Reses, H.E.; Freeman, B.D.; Fajans, M.; Rabold, E.M.; et al. Household Transmission of Severe Acute Respiratory Syndrome Coronavirus-2 in the United States. Clin. Infect. Dis. 2021, 73, e1805–e1813. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Panagiotopoulos, N.; Byers, C.; Garcia Vilaplana, T.; Boddington, N.L.; Zhang, X.; Charlett, A.; Elgohari, S.; Coughlan, L.; Whillock, R.; et al. Transmission dynamics of COVID-19 in household and community settings in the United Kingdom. medRxiv 2020, 20177188. [Google Scholar] [CrossRef]
- Chung, F.; Graham, F. Spectral Graph Theory; AMS: Washington, DC, USA, 1997; Volume 92. [Google Scholar]
- American Society of Heating, Refrigerating and Air-Conditioning Engineers. Thermal Environmental Conditions for Human Occupancy; ASHRAE Standard: New York, NY, USA, 2021; Volume 55. [Google Scholar]
- Hallett, S.; Toro, F.; Ashurst, J. Physiology, Tidal Volume; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Asadi, S.; Wexler, A.; Cappa, C.; Barreda, S.; Bouvier, N.; Ristenpart, W. Aerosol emission and superemission during human speech increase with voice loudness. Sci. Rep. 2019, 9, 2348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Doremalen, N.; Bushmaker, T.; Morris, D.; Holbrook, M.; Gamble, A.; Williamson, B.; Tamin, A.; Harcourt, J.; Thornburg, N.; Gerber, S.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, P.; Mesquita, L.; Gkantonas, S.; Giusti, A.; Mastorakos, E. Evolution of spray and aerosol from respiratory releases: Theoretical estimates for insights on viral transmission. Proc. R. Soc. A 2021, 477, 20200584. [Google Scholar] [CrossRef] [PubMed]
- Vuorinen, V.; Aarnio, M.; Alava, M.; Alopaeus, V.; Atanasova, N.; Auvinen, M.; Balasubramanian, N.; Bordbar, H.; Erästö, P.; Grande, R.; et al. Modelling aerosol transport and virus exposure with numerical simulations in relation to SARS-CoV-2 transmission by inhalation indoors. Saf. Sci. 2020, 130, 104866. [Google Scholar] [CrossRef] [PubMed]





| Environment Scenario | Effective R | Local to Non-Local Infection Ratio (:) |
|---|---|---|
| Very poor ventilation + no masks | R | 3.98:1 |
| Very poor ventilation + masks | 5.20:1 | |
| Good ventilation + no masks | 1.47:1 | |
| Good ventilation + masks | 1.51:1 |
| Parameter | Definition | Best-Case Parameter Values | Worst-Case Parameter Values |
|---|---|---|---|
| Probability of false negatives, | Likelihood that a SARS-CoV-2 test does not identify an infectious individual. | 0.2 | 0.5 |
| R number, R | The average number of secondary cases we would expect an infected student to generate prior to locality affects. | 0.8 | 1.7 |
| Background prevalence, I (%) | Additional probability that more than one person is infected. | 0.5 | 2.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, J.W.; Lau, Z.; Kaouri, K.; Dale, T.C.; Woolley, T.E. A General Computational Framework for COVID-19 Modelling with Applications to Testing Varied Interventions in Education Environments. COVID 2021, 1, 674-703. https://doi.org/10.3390/covid1040055
Moore JW, Lau Z, Kaouri K, Dale TC, Woolley TE. A General Computational Framework for COVID-19 Modelling with Applications to Testing Varied Interventions in Education Environments. COVID. 2021; 1(4):674-703. https://doi.org/10.3390/covid1040055
Chicago/Turabian StyleMoore, Joshua W., Zechariah Lau, Katerina Kaouri, Trevor C. Dale, and Thomas E. Woolley. 2021. "A General Computational Framework for COVID-19 Modelling with Applications to Testing Varied Interventions in Education Environments" COVID 1, no. 4: 674-703. https://doi.org/10.3390/covid1040055