1. Introduction
Fibromyalgia is a rheumatic disease characterized by musculoskeletal disorders [
1], such as changes in the capacity of muscle strength production and sustenance, with consequent disorders in the patient’s functional competence [
2]. The estimated prevalence is from 3.0 to 6.6% of the world population [
1,
3], while in Brazil, this prevalence is 2.5% [
4]. It primarily affects women, with an estimated prevalence of 80 to 90% [
5], between 30 and 50 years old [
6]. The divergence between the worldwide and Brazilian fibromyalgia prevalence, which was the target population of our study, can be justified by the socioeconomic differences that often make diagnostic access difficult [
4]. Epidemiological studies with individuals with fibromyalgia seek to clarify the prevalence in certain regions around the world; however, they present several biases such as sample selection, socioeconomic situation, gender, and cultural aspects, characteristics that undermine the data extrapolation to the entire population of individuals with fibromyalgia [
7]. Studies have reported the need for multi-professional treatment and demonstrated that the muscle physiology and mechanisms involving exercise are critical factors for the non-pharmacological treatment of fibromyalgia [
8].
The League Against Rheumatism (EULAR) has considered physical exercise the only treatment with proven scientific evidence for fibromyalgia control [
3,
9]. Muscle stretching may be highlighted among the different physical capacities to be developed with exercise programs for this population because it improves the functional range of motion [
10] by relieving myofascial tension, with muscle fiber length gain and local blood supply increase [
11]. Such effects in women with fibromyalgia are clinically related to the reduction in pain and improvement in fatigue, quality of life, and sleep [
12].
Studies have compared different exercise programs for individuals with fibromyalgia and observed a significant reduction in anxiety, depression, and mood alterations after interventions with muscle stretching exercises [
8,
13]. The analysis of such responses is essential because people with fibromyalgia present changes in autonomic regulation, with reduced activity in the sympathetic and parasympathetic branches, generating high reactivity to physical and emotional stress, with a greater tendency towards depression and anxiety [
14,
15]. However, the recommendations regarding the stretching program structure for fibromyalgia treatment still need to be more consistent because the applied methods are heterogeneous. Moreover, the description is not detailed enough to enable the replicability of the exercise protocols [
16].
Between February and March 2020, the World Health Organization declared the COVID-19 pandemic [
17,
18]. Therefore, a set of strategies for safe interventions was needed to treat individuals with fibromyalgia since this disease requires continuous treatment [
8]. Respiratory complications were associated with the viral agent since coronavirus disease progresses to severe acute respiratory syndrome (SARS-CoV-2) [
19]. Therefore, correctly managing rheumatic patients was essential; social isolation was the most assertive option. However, this measure of pandemic control resulted in a reduction in the levels of physical activity of the entire population [
20].
A cross-sectional study performed in 2021 with 1156 individuals with fibromyalgia in Brazil inferred that 40% to 50% of individuals who regularly exercised stopped exercising during the pandemic, with an even greater impact on those who did not regularly practice physical activity [
17]. Online management practices were adopted as an alternative for maintaining health care during social distancing. Within that scenario, the practices described in the literature for individuals with fibromyalgia used cognitive behavioral therapies, making it necessary to offer physical exercise practice in this similar format [
21], aiming at maintaining social distance and ensuring functionality [
22].
Therefore, the present study is justified by adopting a safe healthcare strategy using online physical exercise for women with fibromyalgia in times of COVID-19. Promoting access to healthcare in this critical period was extremely important. Therefore, we developed this study using telehealth to reach a population of women with fibromyalgia from diverse social classes with no cost of displacement and no need for a specific physical space, which are considered barriers to physical exercise practice, ensuring the sustainable management in fitness and health services during COVID-19 Pandemic [
23]. We aimed to verify the effects of 12 weeks of a supervised telehealth stretching exercise program compared to a self-care program on pain, sleep, depression, and functionality of women with fibromyalgia during the COVID-19 pandemic. We hypothesized that both programs would significantly benefit the analyzed outcomes, with a higher effect for the supervised telehealth stretching exercise program than the self-care program.
2. Materials and Methods
2.1. Trial Design
The study was a randomized clinical trial, prospectively registered in ClinicalTrials.gov (NCT04690400). The study was a parallel, two-armed, assessor-blinded, superiority randomized controlled trial with an allocation ratio of 1:1. It comprised experimental and active control groups and three assessment points (baseline, middle point, and post-intervention). The experimental and active control groups received the same remote treatment protocol, differing only in terms of online supervision, during the execution of the treatment, for the experimental group. The report is described according to the CONSORT Statement for randomized trials (consort-statemente.org). This project was approved by the Research Ethics Committee of the Physical Education School of the Federal University of Pelotas (CAAE: 3935720.9.0000.5313).
2.2. Participants
The sample comprised women with fibromyalgia from the South of Brazil (Pelotas city region). The eligibility criteria comprised women between 30 and 60 years old due to the high prevalence in females and the fact that the disease is often underdiagnosed in younger age groups by the difficulty in confirming the diagnosis. In addition, the medical diagnosis of fibromyalgia at least three months before eligibility, no regular physical exercise practice in the last three months, access to the internet, and agreement to participate in the study regardless of the allocation group. Exclusion criteria included the presence of another rheumatic disease (secondary fibromyalgia), uncontrolled systemic diseases, and/or being under physiotherapeutic treatment. Participants were recruited through notes shared on social media, lists with names of potential participants drawn up from the medical records of public and private health sectors, and the local association of fibromyalgia individuals (Pelotas, RS). In addition, due to the data collection being performed by a self-applicable questionnaire, they should be semi-literate.
The recruitment occurred in two periods during the year 2021, in which social distancing measures due to the COVID-19 pandemic were still being adopted in Pelotas city and the region. The first wave of recruitment and intervention was from January to March 2021, and the second was from August to September 2021. Phone calls on first contact verified the eligibility criteria. Volunteers who met the criteria were invited to participate in the research. Those who agreed to participate received the digital informed consent with all the research details for the signature. All study procedures, including recruitment, data collection, and intervention, were conducted online due to the COVID-19 pandemic. After inclusion in the study, each participant received an internal identifying number (ID) to ensure concealment. They were also instructed regarding the blinding assessments.
2.3. Sample Size
The sample size calculation for the trial’s primary outcomes was performed in the G*Power version 3.9.1.4 program. We estimated a total of 22 participants considering an alpha level of 5%, a power of 95%, and the
f effect size corresponding to 0.37 for pain and 0.46 for sleep quality, based on a previous study by Gómez-Hernández et al. [
24]. An excess of 6 subjects (~25%) due to the expected dropout rate was considered, totalizing 28 participants divided into the two groups.
2.4. Randomization, Allocation, and Blinding
The randomization sequence for 28 participants was stratified by age (i.e., 30–45 y or 46–60 y) in blocks of different sizes (i.e., 4, 6, 8) with a 1:1 ratio in the Excel random function with reordering of the generated numbers (from the lowest to the highest number). The researcher responsible for the randomization sequence had no contact with the participants. After completing the baseline data collection, an email was sent with the ID of the participants and the corresponding age group, requesting the allocation of the participant to one of the two groups. The randomization sequence was performed before the entire sample was reached. Thus, we had to adjust the randomization procedure because the sequence was stratified by two age group categories in the same proportion. Our recruitment reached more women aged 46–60, missing three women aged 30–45 years to complete the first randomization performed. Therefore, we generated another randomization block of size 4, with a proportion of 1:1, considering only the age group of 46–60. In total, 15 participants were randomized to the control group and 13 to the experimental group.
Blinding was implemented for the outcome assessors at the three different time points. For this purpose, all questionnaires and functional tests were supervised remotely by an investigator blinded to the participant’s group. Due to the nature of the intervention, the investigators who conducted exercise sessions and participants were not blinded.
2.5. Interventions
2.5.1. Experimental Group: Active Care Intervention
The intervention comprised a telehealth stretching exercise program, with remote professional supervision twice a week for 12 weeks. The stretching exercises were chosen because studies suggest this technique may cause a modification in the muscle fiber due to the reduction in local blood supply by vasomotor dysregulation, promoting gain in muscle fiber length and improving local circulation, with consequent relaxation [
1,
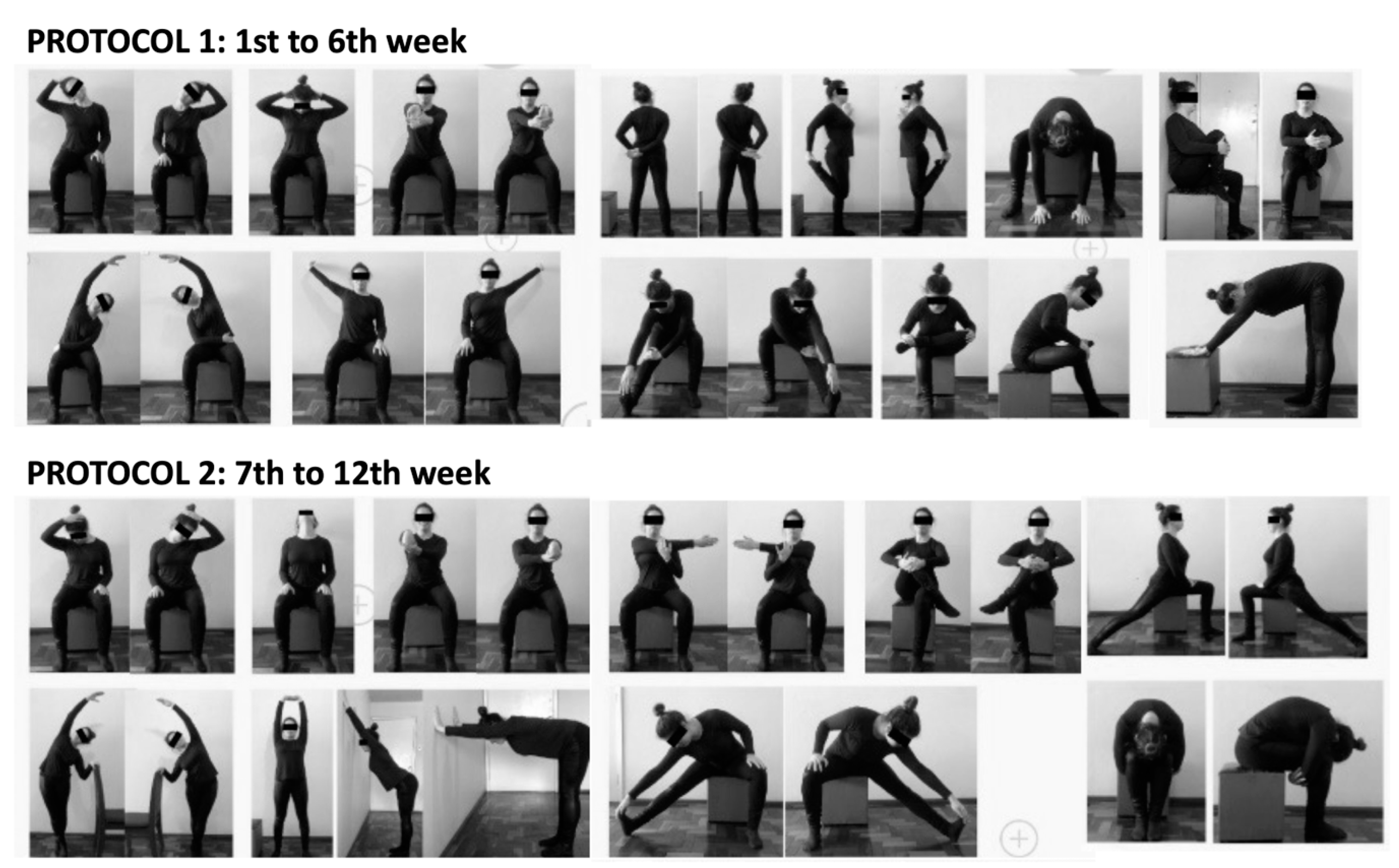
11]. Each session was individually scheduled and supervised by a physiotherapist via WhatsApp, lasting ≈ 45–50 min. This session duration was based on the necessary time to perform the sets and intervals for each movement according to the American College of Sports Medicine recommendations. In case of participants’ unavailability, the session could be rescheduled and recovered within the week to improve the intervention attendance. Each session consisted of 12 stretching exercises for different muscle groups (
Figure 1), performed by fixing the origin and lengthening the insertion. According to the American College of Sports Medicine recommendations [
16,
24,
25,
26], three sets of 10 s of stretching, with 10 s intervals, were used for each muscle, totaling 30 s for each exercise. The intensity was graduated to maintain a position with moderate discomfort without reaching a pain threshold. Therefore, volume was maintained constant during the intervention, while the intensity was self-adjusted by subjective perception. The target muscle used in the intervention were selected according to the disease symptomatology (i.e., the main ones affected by tender points). The same protocol was maintained through the first six weeks. In the seventh week, it was changed, with exercise variations for the same muscles, while the structure, intensity, and volume were maintained. The intervention duration corresponding to 12 weeks was based on previous studies with the same population, which aimed for positive chronic adaptations to exercise [
16,
24]. An exercise guide and videos with all stretching exercises used during the 12 weeks of intervention, elaborated to the control group, were also sent to the experimental group participants to make the interventions more similar.
2.5.2. Control Group: Self-Care Intervention
The intervention comprised counseling to stretching via exercises guide and videos to be performed individually without supervision for 12 weeks. The exercise guide included photos of the corporal position in each exercise and all instructions regarding intensity, volume, and weekly frequency, which were identical to those used for the experimental group. In addition, explanatory videos were sent to provide a complementary understanding of the performance of the exercises. The guide (
Figure 1) and videos were sent via WhatsApp, similar to the experimental group, with a protocol change in the seventh week (exercise variations for the same muscles, while structure, intensity, and volume were maintained). In addition, control group participants received biweekly messages to control attendance and provide protocol clarification if necessary.
2.6. Outcomes
All outcomes were assessed online in three moments: baseline (before randomization), middle point (end of week 6), and post-intervention (13th week). The same blinded assessor collected data at different time points, adopting the same procedures. All questionnaires related to the outcomes were self-applicable via Google Docs. The assessor sent an individual WhatsApp message with the hyperlink and performed a phone call for each participant before and immediately after completing the questionnaires to clarify any doubts. In addition, for the functional assessments, the assessor performed a video call via WhatsApp to instruct about the test and register the scores.
2.6.1. Primary Outcomes
The primary outcomes of the present study were the Widespread Pain Index and Sleep Quality, based on their impact on the quality of life in patients with fibromyalgia and considering that one variable directly interferes with the responses of the other, where poor sleep quality leads to painful exacerbation [
24].
Pain index. The Widespread Pain Index was used to measure the amplitude of patients’ clinical symptoms with fibromyalgia [
27]. It is considered a diagnostic scale, presenting 90.8% accuracy for the American College of Rheumatology’s first criteria in 1990 and validated by the same institution in 2010 [
27]. The Brazilian Society of Rheumatology recognized it in 2017. It comprises the body areas usually affected by the disease, in which the participant indicates where she felt pain in the last seven days [
28]. Total scores range from 0 to 18; those above seven are considered high [
24].
Sleep quality. The Pittsburgh Sleep Quality Index Self-Report Questionnaire (PSQI) was used to register the sleep quality in the previous four weeks [
24]. It was developed in 1989 and validated in the Brazilian version in 2011 [
29]. The questionnaire includes 19 self-reported questions, divided into seven domains [
24] and five questions to be answered by the roommate (when applicable). The score for each question ranges from 0 to 3, where higher scores indicate worse sleep quality [
29]. This questionnaire was self-applicable at the three assessed time points.
2.6.2. Secondary Outcomes
Symptom severity. The Symptom Severity Scale was used, considered a diagnostic criterion, with a sensitivity of 90.9% and a specificity of 85.9% [
28]. It was validated by the American College of Rheumatology in 2010 [
27] and recognized by the Brazilian Society of Rheumatology in 2017. The questionnaire comprises four domains, with items referent to fatigue, non-restorative sleep, cognitive symptoms, and somatic symptoms. Scores for each domain range from 0 to 3, according to the symptom’s intensity. The total score ranges from 0 to 12; those above five are considered relevant [
27]. This questionnaire was self-applicable at the three assessed time points.
Impact of fibromyalgia on daily activities. The Fibromyalgia Impact Questionnaire (FIQ) was used, which investigates the severity of the pathology on the individual’s functional capacity and the perception of the quality of life [
1]. It was validated in 1991, translated, and adapted for the Brazilian version in 2006 [
30]. The questionnaire includes questions related to daily activities, such as cooking and going to the market, with responses ranging from “no difficulty” to “extremely difficult”. The total score ranges from 0 to 100, with higher values indicating a more significant disease impact. Scores are expressed as follows: 0 to 38 corresponds to a mild effect, 39 to 58 a moderate effect, and 59 to 100 a severe impact [
1]. This questionnaire was self-applicable at the three assessed time points.
Depressive symptoms. The Beck Depression Inventory (BDI) was used to analyze the perception of depressive symptoms [
31]. It was developed and revised in 1996 and validated in the Brazilian version in 2012 [
32]. The questionnaire includes 21 questions related to feelings of sadness, failure, dissatisfaction, pessimism, self-judgment, distorted body vision, tiredness, lack of appetite, constant concerns, difficulty in work activities, and loss of libido [
25]. Scores for each item range from 0 to 3. The total score ranges from 0 to 63, with higher values indicating the highest severity. Values between 0 and 13 show minimal symptoms, 14 to 19 medium symptoms, 20 to 28 moderate, and 29 or more indicate severe depression [
31]. This questionnaire was self-applicable at the three assessed time points.
Pain intensity at rest and after movement. The Visual Analog Pain Scale (VAS) was used to analyze the pain intensity at rest and after movement. The movement performed was guided by a call video with the assessor via WhatsApp, using three sets of 10 s of stretching at the position of shoulder flexion, with the hands splayed upwards and the fingers intertwined. The scale was shown to the participant before (at rest) and immediately after the movement to measure the pain felt at the test’s moment [
4]. Scores range from 0 to 10, where 0 corresponds to “no pain” and 10 means “the greatest pain imaginable” [
24]. This test was performed online and applied at the three assessed time points.
Flexibility. One test from the Flexitest battery [
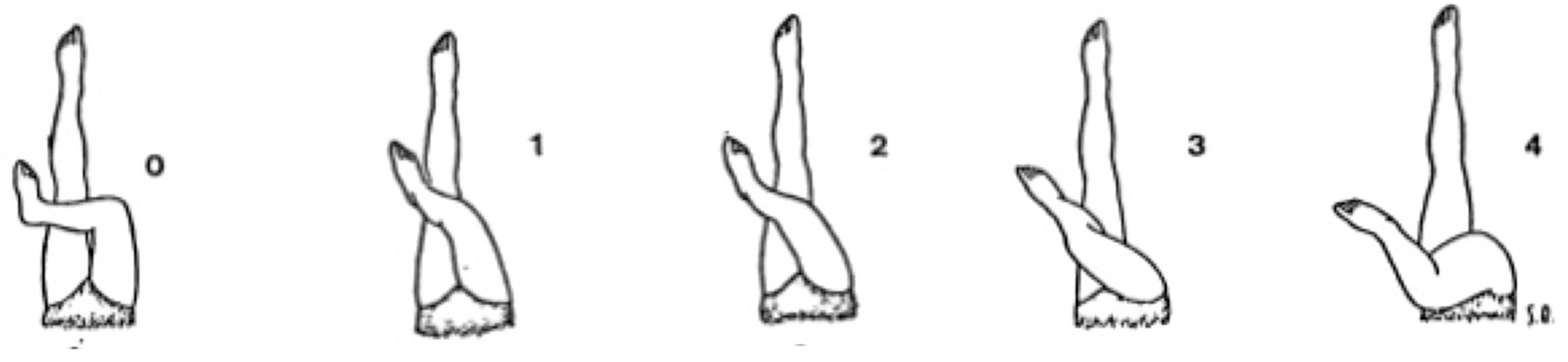
33] was adapted to evaluate flexibility in an online format. The test was active-assisted and performed by call video with the assessor via WhatsApp. The participant started in the seated position with legs extended and back supported. The target position corresponded to the unilateral hip adduction with the knee flexed and foot supported on the ground, crossing the lower limb on the opposite leg extended on the ground, with contralateral upper limb assistance. This movement aimed the unilateral hip abduction stretching until the maximum range of motion. The assessor guided such position, and at the maximum angle, the participant positioned the cell phone over the head with the ipsilateral upper limb (shoulder flexion up ≈ 180°) to register the position image at the three assessed time points. The range of motion was scored by an evaluator visual inspection comparing it with a position map with reference values ranging from 0 to 4 [
33], as shown in
Figure 2, where higher scores indicate increased mobility.
Subjective perception of well-being. A single question was used to verify the well-being: “How much did participation in the project improve your feeling of general well-being?” The response was based on a 5-point Likert Scale, varying from “dissatisfied” to “very satisfied”. The question was self-applicable via Google Docs for both groups only post-intervention (13th week), with no need for identification.
2.6.3. Other Outcomes
Sample characterization. Body mass and height were estimated by each participant and self-reported by a questionnaire via Google Docs. The body mass index (BMI) was estimated based on: BMI = body mass/height2. In addition, participants answered questions related to the diagnosis time, familiar history of rheumatologic disease, climacteric, marital status, schooling level, and occupational leave due to fibromyalgia symptoms. In addition, they should report whether they already have received a temporary disability benefit (i.e., disease aid) through the National Institute of Social Security (INSS, Brazil).
Physical activity level. The short version of the International Physical Activity Questionnaire (IPAQ-C) was used to verify participants’ physical activity levels. It was proposed and validated by the World Health Organization in 1998, with its Brazilian version published in 2001. The questionnaire includes eight questions in different domains: work, leisure, domestic activities, transportation, and physical exercises. Data were expressed in minutes using the metabolic equivalent (1 MET: 3.5 mL/kg/min) [
34]. Therefore, results were equivalent to the time spent in the activities multiplied by the days of the week they were performed and the values divided by categories. This questionnaire was self-applicable at the baseline and post-intervention.
2.7. Statistical Analysis
Data were imported from Google Docs to Excel, and a double check was performed to ensure the quality of the information. Descriptive statistics were used by means and standard deviation (SD) or 95% confidence interval (95%CI) to report the results. Sample characterization data were compared between groups by
t-tests for independent measures, considering the assumption of normality (Shapiro–Wilk’s test) and homogeneity (Levene’s test). Generalized Estimated Equations (GEE) were applied to compare the outcomes between and within-group, with Bonferroni post hoc tests. Data were analyzed by intention to treat (ITT), in which all randomized participants were included, and per protocol (PP), in which only participants who presented an attendance ≥ 70% were included. All statistical procedures were performed in the SPSS vs. 20.0 statistical package, adopting an alpha level of 5%. In addition, the Cohen’s d effect size between groups was estimated and classified as small (0.2), moderate (0.5), and large (0.8), according to Sullivan and Feinn [
35].
3. Results
3.1. Participants
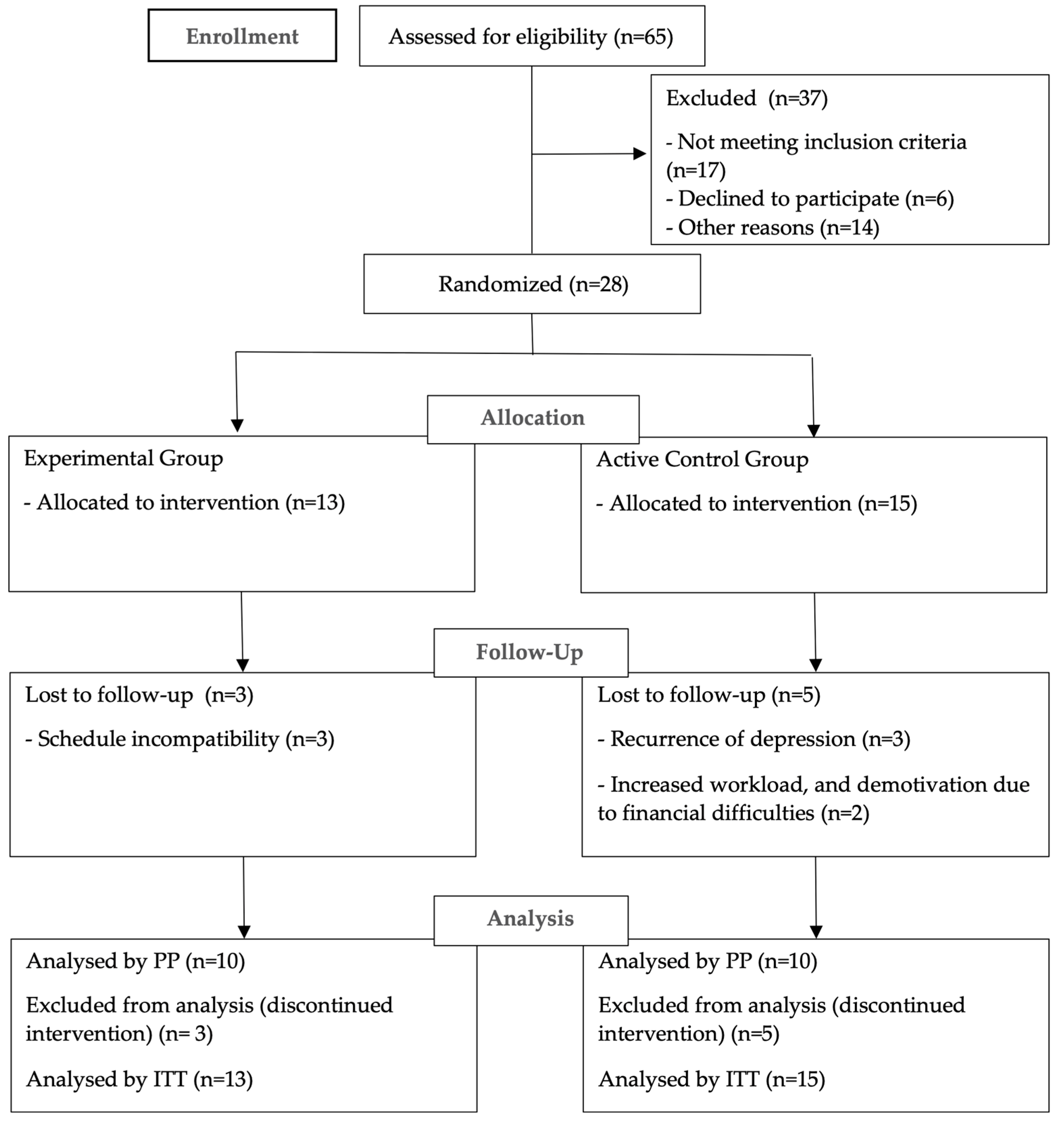
Out of 65 telephone contacts by active and voluntary recruitment, 32 women were eligible, and 33 were not included for the following reasons: another associated rheumatic disease (n = 9), regular practice of some physical exercise beyond active travel (n = 8), lack of interest (n = 6), lack of time (n = 2), and telephone call refusal (n = 8), as shown in the flowchart (
Figure 3). In addition, four women dropped out of the study after signing the consent form and before the baseline data collection. Therefore, 28 participants were randomized and included in the ITT analysis. Of these, 8 dropped out during the intervention (3 from the experimental group and 5 from the active control group), resulting in 20 participants who completed all stages of the study. Therefore, 20 participants were included in the PP analysis: 10 in the experimental group (who reached the minimal necessary attendance, i.e., 70%) and 10 in the active control group.
Regarding the sample losses of volunteers who did not reach the minimum expected frequency, we observed that many of them were associated with the pandemic scenario. Although the intervention took place remotely, the participants with loss of continuity reported discouragement, sadness, worries, unemployment, or excessive work, with a high stress level regarding information about COVID-19. Additionally, most participants had an adverse reaction to the vaccine against COVID-19, especially from the British manufacturer Oxford-AstraZeneca, reporting severe fatigue, a considerable increase in pain, fever, and headache, resulting in prolonged rest.
Table 1 presents the sample characterization at baseline. The participants of both groups presented similar mean age, estimated height and body mass, BMI, and diagnosis time. Still, the volunteers’ physical activity levels, assessed pre- and post-intervention, are reported by category, with the absolute frequency corresponding to the participants who completed the study, as shown in
Table 2.
3.2. Outcomes
The results corresponding to the study variables, analyzed by protocol and intention to treat, are shown in
Table 3. Both analyses (i.e., PP and ITT) demonstrated post-intervention improvements in the widespread pain index, sleep quality, symptom severity, and pain intensity at rest and after movement for both groups, with no difference between them. In addition, both analyses showed a significant reduction in the widespread pain index and symptom severity at week 6 compared to the baseline for both groups, with no difference between them.
Interaction between moment and group factors was only observed in the impact of fibromyalgia on daily activities. Both analyses (i.e., PP and ITT) demonstrated a post-intervention improvement in this outcome; however, a different pattern was observed between groups. In both analyses, the post hoc test indicated a significant reduction for the experimental group in the post-intervention compared to baseline and week 6. On the other hand, for the control group, both analyses showed a significant reduction in these values from baseline to weeks 6 and 13, with values maintained from week 6 to post-intervention. Additionally, the ITT analysis showed that the experimental group had lower values than the active control group at week 13, with no differences between the groups in the PP analysis.
Depressive symptoms improved in the post-intervention period in both groups by the PP analysis, with no difference between them, while no effect was observed in any of the factors for depressive symptoms in the ITT analysis. In contrast, the flexibility improved in the post-intervention period in both groups by the ITT analysis, with no difference between them, while the PP analysis showed no effect on any of the factors.
Regarding the effect size between groups, the impact of fibromyalgia on daily activities resulted in a large effect size in the ITT analysis (0.85; 95% CI from 0.08 to 1.63) and a moderate effect size in the PP analysis (0.58; 95% CI from −0.32 to 1.47) at post-intervention time point. In addition, a moderate effect size was observed in both analyzes for symptom severity at post-intervention (PP: 0.53; 95% CI from −0.36 to 1.42; ITT: 0.50; 95% CI from −0.25 to 1.25) and pain intensity at rest (at week 6 (PP: 0.67; 95% CI from −0.31 to 1.64; ITT: 0.64; 95% CI from −0.12 to 1.40).
Moreover, the subjective perception of well-being, reported by participants only post-intervention (13th week), resulted in responses between “satisfied” and “very satisfied” for both groups. In the experimental group, nine participants answered they were “very satisfied,” and one participant was “satisfied”, while in the active control group (n = 10), six participants were “very satisfied,” and four participants “satisfied”.
4. Discussion
The main findings of the present study were the improvement in the primary outcomes (i.e., widespread pain index and sleep quality) after 12 weeks of a telehealth stretching exercise program for individuals with fibromyalgia, regardless of the online supervision. Furthermore, both groups with and without online supervision observed significant reductions in the symptom severity, the impact of fibromyalgia on daily activities, depression symptoms (only in the PP analysis), flexibility (only in the ITT analysis), and pain at rest and after movement. All outcomes presented similar adaptations between groups after 6 and 12 weeks of training, except for the impact of fibromyalgia on daily activities. This outcome revealed a more significant effect for the experimental group compared to the active control group 12 weeks post-intervention in the ITT analysis. Participants’ adherence to the treatment program varied according to the allocation group. The experimental group met at least 70% of attendance with the possibility of recovering classes in case of adversity. The active control group had adherence verified through the biweekly reports of the participants, in which they reported not maintaining constancy in the execution of activities, with low follow-up of the suggested periodicity; however, they had the freedom to recover activities when necessary. Regardless of the presence of supervision, both groups reported a subjective perception of well-being as very satisfied or satisfied after participating in 12 weeks of a telehealth stretching program; however, better satisfaction was observed in the experimental group.
The present results agree with previous studies that have also investigated the effects of stretching exercise programs on pain, sleep disorders, depression symptoms, and quality of life of individuals with fibromyalgia [
16,
24,
25,
33]. However, they were not applied via an online format, evidencing the innovation of this research. Concerning pain levels, in the present study, significant reductions were observed in both the Widespread Pain Index and Visual Analog Pain Scale (at rest and after movement) in both experimental and control groups. These findings corroborate previous studies investigating pain levels in experimental exercise programs for fibromyalgia treatment [
10,
13,
16,
24,
36,
37]. Among them, Assumpção et al. [
16] observed a significant reduction in body pain and improvement in functionality after 12 weeks of in-person intervention only for the stretching exercises group compared to the resistance exercises group. In addition, the systematic review by Bidonde et al. [
10] included experimental studies involving stretching exercises as an intervention. From these, the authors reported only four research works with a low risk of bias which affirmed a reduction in pain levels in the fibromyalgia population. The present study was a randomized clinical trial, including interventions based on standardized muscle stretching, with prescription parameters according to the main exercise guidelines recommendations. Our findings demonstrate the effectiveness of the stretching exercises standardized protocol concerning the pain index for individuals with fibromyalgia, regardless of the presence of online supervision.
Regarding sleep, the present study’s findings corroborate those of the research by Goméz-Hernández et al. [
24], who performed 12 weeks of face-to-face intervention of a moderate-intensity aerobic program associated with stretching exercises in women with fibromyalgia compared to a control group that performed only aerobic exercises. Significant improvements were observed just in the sleep quality for the experimental group, assessed by the same questionnaire (Pittsburgh Sleep Quality Index) of the present study. Martins et al. [
38] conducted a study with an experimental group for individuals with fibromyalgia, including stretching, health education, cognitive-behavioral therapies, and ergonomics adjustments, compared to a control group. They observed that sleep improved in the intervention group, in addition to lower pain levels, according to our findings. Such results demonstrate the essential connection between pain chronicity with worse sleep conditions in this population, reinforcing the role of exercise as a treatment. Although it is still unclear how a stretching program interferes with improving sleep quality, it is known that the muscle relaxation produced by the technique reduces cognitive arousal, generating a positive impact on the circadian rhythm also reducing daytime sleepiness Goméz-Hernández et al. [
24].
About the impact of fibromyalgia on daily activities, Valencia et al. [
39] compared the effects of two 12-week experimental muscle stretching programs performed in person, one group including active exercises and the other with active-assisted exercises. When comparing groups and moments, they observed a significant improvement in the Fibromyalgia Impact Questionnaire score for both groups, with higher scores for the group that performed the active exercises. On the other hand, Assumpção et al. [
16] found a reduction in the Fibromyalgia Impact Questionnaire scores after 12 weeks of in-person intervention for the three investigated groups, i.e., stretching exercises, resistance exercises, and control. Although both groups actively performed stretching exercises in our study, the most expressive improvements were observed in the group with remote supervision after 12 weeks of intervention in the ITT analysis, with a moderate effect size between groups (PP: d = 0.58; ITT: d = 0.85). This difference may be a consequence of the lower attendance in the active control group compared to the group with remote supervision. In addition, another crucial factor to be highlighted is the insurance of the correct execution of movements for the supervised group. Although the active control group had received the same familiarization, had full access to the protocol, and the exercises presented a low risk of injury, during the weekly practice, the participants who performed the protocol without supervision did not have access to movement correction in real-time.
Relative to the depressive symptoms, Andrade et al. [
25] observed positive results after 12 weeks of an in-person exercise program compared to a control group, including resistance, aerobics, and stretching exercises on the depression levels (37.5 %) and the impact of fibromyalgia on quality of life (29.4%). In this study, a significant difference in the BDI score was observed only for the experimental group when comparing the baseline (week 0), middle (week 6), and post-intervention (week 13). These findings are in line with the present study, which also revealed an improvement in the BDI scores in the PP analysis, with a significant reduction after six weeks of intervention, maintaining these reduced levels until the end of period in both experimental and active control groups. It indicates that regardless of the in-person versus online format or the presence of supervision, exercise effectively reduces depressive symptoms in individuals with fibromyalgia. Such findings are reinforced by the review by Ibáñez-Vera et al. [
13], who demonstrated that stretching exercise programs reduced anxiety, depressive symptoms, and mood changes in this population.
For flexibility, Almeida and Santos [
40] compared women with and without fibromyalgia in a cross-sectional study design also using the Flexitest index. In contrast to our online evaluation, the authors conducted an in-person assessment and did not find significant differences between the groups. Notwithstanding, in the present study, this outcome presented positive results for both groups in the ITT analysis, which may indicate that Flexitest was able to show that the program was effective in developing the trained physical capacity during the 12 weeks of both programs.
Oliveira et al. [
41] analyzed, in their cross-sectional study, the level of physical activity in women with fibromyalgia through the same instrument used in the present study, the IPAQ questionnaire. The authors observed that most participants remained in the “irregularly active A-B” category. However, they inferred that low-intensity activities could moderate the perception of quality of life and social interaction. In the present study, there was a change in physical activity levels post-intervention in the experimental group, with changes in the absolute frequency in categories from less to more time spent in physical activity, starting from “irregularly active B” to “very active.” These results indicate that a supervised telehealth stretching program, performed with regularity and standardization, can positively interfere with increased general physical activity in women with fibromyalgia, including time spent on domestic and work tasks.
It is necessary to highlight the originality of the present study because we cannot consider separately each outcome related to fibromyalgia since they are manifested in an association. Therefore, it is necessary to interpret all these outcomes together. It should also be noted that currently the studies that have been trying to understand the effect of exercise on fibromyalgia symptoms include flexibility interventions [
16,
24,
25]. Review studies [
9,
10,
11] also investigated exercise models that benefit the clinical condition and symptoms of fibromyalgia and reinforced the low methodological quality of the studies which employed stretching exercise programs as intervention. In addition, Kim et al. [
12], in their systematic review, reported that eligible studies did not address the basic principles of flexibility training recommended by the American College of Sports Medicine, a fact that may have compromised the post-intervention results. Therefore, the present study’s main strengths are the study design and the intervention structure, based on the American College of Sports Medicine guidelines for stretching exercises [
16,
24,
26]. Moreover, the present study analyzes outcomes that represent the effect of online intervention in various domains of fibromyalgia, filling a gap in the literature. Likewise, stretching exercises show a low risk of injury with high practicality [
36,
37]. Thus, the study ensured the safety of the participants in the face of the pandemic, promoting the maintenance of functionality in times of social isolation and improving the main symptoms related to the disease.
This study is not free of limitations such as the high sample drop-out, most of them due to reasons related to the current pandemic scenario. Although the intervention occurred remotely, participants who dropped out reported discouragement, sadness, worries, unemployment, or excessive work, with a high stress level regarding information about COVID-19. Moreover, most participants had an adverse reaction to the vaccine against COVID-19, especially the British Oxford-AstraZeneca vaccine. In such cases, they reported severe fatigue, increased pain, fever, and headache, resulting, in most cases, in prolonged rest and, consequently, the need for remote session recovery in the experimental group. In addition, the functional assessment carried out using the adapted Flexitest (online format) may have limited the analysis of this outcome since it required a good positioning of the cell phone camera so that the screen capture taken by the evaluator obtained better accuracy of the participant’s positioning.



 and
and 



{kind=link}
{kind=link}
{kind=link}